
Abstract
Physical inactivity is a major concern in cancer patients despite the established preventative and therapeutic effects of regular physical exercise for this patient group. Sport not only plays an important role in supporting the development and maintenance of a physically active lifestyle but also is increasingly used as a health promotion activity in various populations. Nevertheless, the potential of sport as an effective strategy in the prevention and management of cancer has gained little attention. Based on the scant evidence to date, participation of cancer patients in supervised, well-tailored sport programs appears to be safe and feasible and is associated with an array of physical and psychological benefits. We propose that sport participation may serve as an alternative strategy in the prevention of cancer and sport medicine in the management of cancer. As with the traditional exercise modes, benefits derived from sport participation will be dependent on the sport undertaken and the physical/physiological, motor, and cognitive demands required. To this end, further work is required to develop a solid evidence base in this field so that targeted sport participation can be recommended for cancer patients.
Introduction
Cancer is a worldwide problem and imposes a tremendous disease burden. In 2018, the expected number of new cancer cases globally was 18.1 million. 1 For most cancer patients, the disease and related treatments will have a severe adverse effect on physical, mental, and social health with the most common symptoms being fatigue,2,3 pain,4,5 nausea,6,7 reduced functional capacity,8,9 depression,10,11 anxiety,3,12 and social disconnectedness.13,14 In addition, cancer patients are also more vulnerable to other chronic comorbidities such as cardiovascular disease, diabetes, osteoporosis, and sarcopenia.15-17 Therefore, strategies that can reduce the risk of cancer and mitigate a wide range of health sequelae related to the disease and its treatments are of clinical importance.
Regular physical exercise is associated with a reduced risk of many types of cancers18,19 and cancer recurrence 20 as well as attenuated treatment-related symptoms in cancer patients.15,21,22 However, physical inactivity or an insufficient level of physical activity, irrespective of a cancer diagnosis, remains a major concern. According to data recently published, 23 worldwide 27.5% of adults in 2016 (rising from 23.3% in 2010) did not meet the World Health Organization recommendations on minimum physical activity for health, that is, at least 150 minutes of moderate-intensity, or 75 minutes of vigorous-intensity physical activity per week, or equivalent combinations. With regard to cancer patients in developed countries, the prevalence of a sedentary lifestyle is much higher. The National Cancer Institute recently reported 24 that 34.8% of adult cancer patients engaged in no physical activity in 2016. In addition, an estimated 88% of prostate cancer patients in Australia do not meet the recommended physical activity level, of which 47.5% are totally inactive 25 ; while in Canada, only 21% of cancer patients were considered active in 2005, 26 with similar results also reported in the 2009-2010 National Health Survey round. 27
Sport participation is commonly advocated by policy makers to facilitate the development and maintenance of an active lifestyle in the general public. As suggested by Khan and colleagues, 28 sport contributes to a healthier nation through improved physical activity level of the population. Individuals who play sports are more likely to meet the recommended physical activity level for health than those who are not active in sport. 29 Sport, through varied forms of interactive (such as partnered-based and group-based activity) and match/contest play, may have the potential to increase participation rate and maintain exercise continuance in various populations.30,31
In recent years, a range of sports as a health promotion activity has been examined in the noncancer populations. A period of participation in organized sport activities were reported to result in a broad spectrum of cardiometabolic and musculoskeletal benefits in both the apparently healthy population and patients with common chronic diseases such as diabetes, hypertension, and osteoporosis.32,33 In addition, sport participation is often associated with a wide array of psychological benefits including enhanced self-esteem and self-efficacy and a general feeling of well-being. 34 However, the potential of sport as an effective intervention in the management of cancer has gained little attention. This may be partially related to a prevailing dogma that vigorous exercise, which would include a wide range of sport activities, may increase the risk of immunosuppression thereby compromising the immune system against tumor cells. However, a recent review by Campbell and Turner 35 dispelled such a misconception and concluded that acute vigorous exercise may actually enhance immunological health.
To date, there is no definitive evidence that would preclude sport participation in cancer patients. On the contrary, a recent review by Ruiz-Casado et al 36 synthesizing numerous preclinical and human mechanistic studies concluded that an active lifestyle (and this could be achieved through exercise and sport) through multiple biological mechanisms (such as vascular normalization, myokine secretion, etc) may potentially exert an antitumorigenic effect. In addition, emerging clinical trials37,38 have showed preliminary efficacy of prescribed sport activities (such as soccer, triathlon, wall climbing, and dragon boat racing) in patients with common types of cancers (predominantly prostate and breast cancers) on a variety of supportive care outcomes. Therefore, we propose that participating in structured sport programs may serve as an alternative strategy to conventional clinic-based and community-based physical exercise programs and could be implemented more widely in the prevention and management of cancer. In this review, we discuss the positive association between sport participation and the risk of cancer and cancer-specific and overall mortality, present studies reporting sport activities in the management of cancer, provide initial recommendations on sport participation for cancer patients, and finally discuss future opportunities for research in this emerging field of oncology.
In order to facilitate discussion on this topic, in this article sport is defined as an activity requiring physical effort and skills with predetermined rules and objectives, which typically requires multifaceted physical and physiological demands depending on various factors such as movement components and forms of play.39,40 Evidence regarding sport participation for cancer management in this review was obtained through a systematic literature search. Briefly, electronic searching was undertaken in PubMed, Web of Science, SPORTDiscus, PsycINFO, and Google Scholar databases using keywords for population (cancer OR tumor OR malignancy) AND keywords for intervention (sport OR individual sports OR team sports OR specific sport disciplines based on the current list of Summer and Winter Olympics), with databases searched up until May 2019. In addition, the reference lists of relevant primary and secondary studies (review articles, commentaries, and editorials) were also checked to identify potential eligible studies. Due to the limited evidence on sports for cancer management, studies on exercise programs primarily composed of sport-related activities (including sport skills practice and targeted physical training preparation for a specific sport such as triathlon) in cancer patients were also included in this review.
Sport, Cancer Risk, and Cancer Mortality
It is well established that sport participation reduces the risk of all-cause mortality and improves life expectancy in various populations.41-44 In the cancer context, individuals repeatedly exposed to sports (including the general public, amateur/collegiate athletes, and professional/elite athletes) also have decreased risk of cancer and cancer-related death, although disparity exists in their training levels and physical condition. An early observational study 45 suggested that regular sport participation led to a lower rate of cancer incidence in middle-aged and older men. In a similar fashion, life-time sport-active adult women have a reduced incidence of breast cancer (>50% reduction) compared with age-matched nonactive women with stronger protective effects observed in those with earlier sport engagement and higher activity level. 46 In amateur/collegiate athletes with higher training volume and intensity, a lower rate of cancer risk has also been observed. An early large-scale survey 47 in 5398 female former collegiate athletes and nonathletes indicated that long-term participation in organized sport activities was associated with a reduced risk of not only breast cancer but also gynecologic cancers; while a 15-year follow-up 48 of these subjects also indicated that previous college sports experience conferred a life-time prophylactic effect against breast cancer. Recently, a retrospective study 49 in French athletes demonstrated that the longer life expectancy in elite athletes of numerous sports was primarily attributed to the lower risk of cancer.
Regarding cancer mortality, several cohort studies50-52 and a meta-analysis 53 have demonstrated that, in comparison with the general population, elite professional athletes and Olympians (mostly men) have fewer cancer-specific deaths. As reported in the meta-analysis, 53 the pooled standard mortality ratio for cancer was 0.60 (95% confidence interval = 0.38-0.94) in professional or Olympic-level athletes. Therefore, encouraging evidence suggests that engagement in sports may be conducive in reducing cancer incidence and cancer-specific and overall mortality in adult men and women with varied sport training backgrounds, which may be attributable to a healthier lifestyle including less smoking and more physical activity in sport active people. 50
Sport and Cancer Management
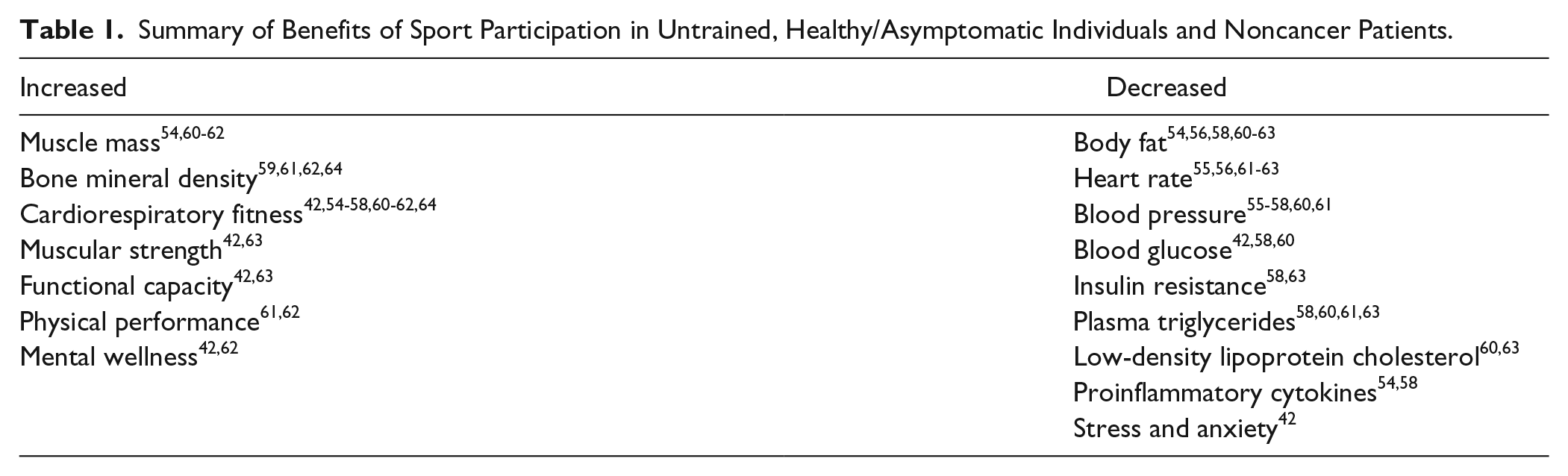
Work to date indicates that sport participation as a health promotion activity has a broad spectrum of physical and psychological benefits in not only healthy/asymptomatic individuals but also clinical populations with common cardiometabolic comorbidities including hypertension, diabetes, and obesity regardless of age, sex, and socioeconomic background. A summary of beneficial effects resulting from a period of participation in individual and team-based sport activities including golf, 42 rugby,54,55 soccer,56-60 basketball, 61 handball, 62 and floorball63,64 in untrained, healthy/asymptomatic individuals and noncancer patients is presented in Table 1. Likewise, a small but growing number of studies65-79 have shown that regular participation in individual and team-based sports (including triathlon, wall climbing, dragon boat racing, and soccer) is also effective as an exercise therapy for persons previously diagnosed with cancer (mostly breast and prostate cancer) in alleviating disease-related and treatment-related adverse effects on physical, physiological, and psychological function (Tables 2 and 3).
Summary of Benefits of Sport Participation in Untrained, Healthy/Asymptomatic Individuals and Noncancer Patients.
Physical and Physiological Benefits of Sport Participation in Cancer Patients.

Abbreviations: ↑, increase; ↓, decrease; A peak, peak mitral annular velocity during late diastole; BCa, breast cancer; BMD, bone mineral density; CON, control group; COMP, comparison group; Ea, the time to onset of early diastolic velocity of the mitral annulus; F, female; GCa, gynecologic cancer; HR, heart rate; INT, intervention group; IVRT, isovolumic relaxation time; LBM, lean body mass; min, minute; NR, not reported; NRCT, nonrandomized controlled trial; OS, observational study; PCa, prostate cancer; R, right; RCT, randomized controlled trial; RM, repetition maximum; SAT, single-arm trial; VO2max, maximum oxygen uptake.
Statistically significant from baseline.
Statistically significant from control/comparison group.
Same trial with different intervention duration and outcomes reported.
Psychological Benefits of Sport Participation in Cancer Patients.

Abbreviations: ↑, increase; ↓, decrease; BCa, breast cancer; COMP, comparison group; CON, control group; INT, interventional group; NRCT, nonrandomized controlled trial; PCa, prostate cancer; POS, prospective observational study; pRCT, pragmatic randomized controlled trial; QoL, quality of life; ROS, retrospective observational study; SAT, single-arm trial.
Statistically significant from control/comparison group.
Statistically significant from baseline.
Same trial with different data collection and outcomes reported.
Physical and Physiological Benefits
Positive adaptations in physical performance, functional ability, cardiovascular fitness, and body composition have been observed in cancer patients following short-term to long-term participation in structured soccer and dragon boat (team paddling in a heavy, dragon-shaped boat) programs with some of the changes more notable than those engaging in other fitness activities (Table 2). For example, a short-term (8-week) program of dragon boating resulted in significant improvement in muscular strength and aerobic capacity in adult cancer patients. 71 In middle-aged and older breast cancer (BCa) patients, 75 cardiac diastolic function substantially improved following long-term (48 months) participation in dragon boating compared with healthy women undertaking predominantly traditional cardiorespiratory activities including running, cycling, and swimming. In addition, BCa patients engaged in a twice-weekly dragon boat program for over 6 months had lower lymphedema incidence than a comparison group undertaking other forms of aerobic exercise including Pilates, yoga, tai-chi, jogging, and walking. 77 A randomized controlled trial (RCT) demonstrated that recreational soccer training up to 32 weeks in duration induced marked improvement in lean body mass, 73 bone mineral density, 76 and lower limb muscle strength and function 76 in men with locally advanced or metastatic prostate cancer (PCa) undergoing androgen deprivation therapy. In a subsequent 5-year follow-up, 78 the beneficial effects on the skeleton were maintained through regular participation in self-organized recreational soccer games with significant improvement observed in femoral neck bone mineral density compared with those undergoing resistance training, aerobic exercise, and yoga.
Beyond soccer and dragon boat racing, other sports including triathlon and wall climbing (adapted indoor rock climbing), albeit less examined in cancer patients, have also shown initial efficacy in improving physical functioning (Table 2). For instance, a 14-week program culminating with participation in a sprint distant triathlon (800-m swimming, 20-km cycling, and 5-km running), which comprised twice-weekly team triathlon training and 3 to 7 hours per week home-based exercise, significantly increased maximal oxygen uptake in BCa patients. 80 In addition, in undertaking an 8-week wall climbing program (including various specific skills practice and climbing strategy drills) in gynecologic cancer patients, significant improvement was observed in aerobic capacity, muscular strength, agility, dynamic balance, and flexibility. 81
The improvements observed in cancer patients are possibly related to the physical and physiological demands of the respective sport activity. Soccer is a lower limb–driven intermittent locomotor activity with various vigorous, high-impact movements, 82 which predominantly results in adaptations in cardiorespiratory and lower body musculoskeletal systems. Dragon boat racing, like most paddle sports (such as canoeing and rowing), is a non–weight-bearing, upper limb–driven endurance activity, which predominantly may result in changes in the cardiovascular system and upper body muscle endurance. 83 Triathlon is a multisport endurance event consisting of 3 continuous and sequentially performed races including swimming, road cycling, and distance running. 84 Wall climbing, which is adapted from an outdoor sport—rock climbing, primarily requires muscular strength/power, aerobic endurance, flexibility, and balance in climbers. 85
Psychological and Social Benefits
In addition to physical and physiological endpoints, participation in sports are accompanied by psychological and social benefits in cancer patients with the most frequently reported positive findings being enhanced psychological well-being and quality of life (QoL; Table 3). For instance, various dimensions of psychological well-being (such as emotional, social, and spiritual well-being) in adult BCa patients were enhanced through participating in dragon boat racing.65,66,72 In addition, health-related QoL was also improved in BCa patients67,69,72,80 and other unspecified adult cancer patients 71 after a period of dragon boating or triathlon training; and the improvement in BCa patients was comparable with age-matched healthy women. 67 A recent retrospective study 77 indicated that BCa patients who participated in a short-term low-frequency dragon boat program had better QoL compared with a group undertaking commonly used therapies (such as compression therapy and lymphatic drainage) and aerobic exercise including Pilates, yoga, tai-chi, jogging, and walking. Regaining of social support and personal control was also observed in middle-aged BCa patients following long periods (19 months to 8 years) of engagement in dragon boat programs.68,70 Moreover, both observational 67 and intervention-based 71 studies indicate that adult cancer patients (mainly BCa) within a team format developed strong cohesiveness after a period of dragon boating, which was at a higher level compared with those undertaking other group-based activity (eg, walking) 71 and comparable with those in female sport teams, 67 and was crucial to exercise initiation and maintenance. 86 Last, it has been reported that participation in small-sided soccer games by men with PCa is accompanied by improved mental health. 79
Aside from the studies dedicated to a specific sport program mentioned above, cross-sectional studies87,88 also indicate that participation in a range of sports (such as golf, swimming, hockey, tennis, etc) after a cancer diagnosis is associated with improved psychosocial outcomes in patients. The mechanisms underlying the improvements in psychosocial functioning in cancer patients participating in sports are possibly related to the social/interactive, supportive, and enjoyable/challenging environment featured in sports and in particular team sports.34,89,90 In team-based sports, participants are required to work closely toward a common goal, which tends to generate greater bonding among team peers compared with undertaking other exercise modalities. In addition, there is also evidence that cancer patients consider peer support and shared experience with co-participants as motivational factors in their sport participation.86,91,92
Safety and Feasibility
In undertaking sport activities, the cancer patient’s safety needs to be ensured. With regard to exercise in general, the Exercise and Sports Science Australia (ESSA) position stand 93 and the American College of Sports Medicine (ACSM) roundtable statement on exercise for cancer patients 22 concluded that exercise training is well tolerated during and after cancer treatment and is safe in patients of common cancers. In addition, numerous systematic reviews and meta-analyses94-105 published within the past decade further support this conclusion, adding that resistance-based and aerobic-based exercises, irrespective of mode, intensity, duration, frequency, and supervision, are safe in common adult and pediatric cancer patients at different stages or having received different therapies, with either no adverse events or only minor exercise-related injuries (such as muscle soreness, sprains, and strains) and discomforts observed.
Similar findings were also reported in patients with breast, gynecologic, and prostate cancers undertaking varied sport programs, although the incidence and frequency of adverse events or injuries were not always explicitly reported by the investigators (Table 4). For example, in nonmetastatic BCa patients following intensive treatments, no adverse events and only one case of a non-training–related injury were reported in a 4-year supervised dragon boat program 75 and a 14-week team triathlon training program, 80 respectively. Similarly, in an 8-week wall climbing program in 24 gynecologic cancer survivors, 81 only one participant suffered a leg scratch during training. Even in more advanced (≥T3n) PCa patients (including those with bone metastases) undergoing androgen deprivation therapy, the incidence of adverse events was not severe with only 5 of the 29 participants experiencing a musculoskeletal injury in a 32-week supervised trial73,76 and 2 of 11 soccer participants suffering an injury in 5 years of unsupervised soccer training. 78 Moreover, in a recent large-scale RCT in men with early-stage and advanced PCa 79 participating in 6 months of twice-weekly supervised soccer, the injury rate in the soccer players was equivalent to that in the control group receiving exercise instruction by telephone and rehabilitative therapy, with the vast majority of injuries minor including muscle strain or sprains. Although participating in soccer games appears to be associated with a risk of injury, men with PCa might instead perceive the risk a positive reinforcement of their masculinity. 106
Safety and Feasibility Outcomes of Sport Participation in Cancer Patients.

Abbreviations: ADT, androgen deprivation therapy; BCa, breast cancer; GCa, gynecologic cancer; HRmax, maximum heart rate; NR, not reported; PCa, prostate cancer.
Same trial with different intervention duration and outcomes reported.
In addition to the safety profile, the feasibility outcomes observed in various cancer patients undertaking sport-based programs also appears promising (Table 4). For instance, in the wall climbing program in women diagnosed with gynecologic cancer, on average 13.5 out of 16 sessions were attended. 81 Similarly, in the 14-week, twice-weekly team triathlon program for BCa patients, 21 out of 25 participants completed the training program and assessments. 80 Carter et al reported that adult cancer patients undertaking dragon boating on average attended more sessions than controls performing group-based walking over an 8-week period. 71 However, attendance may alter with program duration as evidenced in the soccer program by Uth and colleagues, with attendance of ~77% at 12 weeks 73 but only 46% at 32 weeks. 76 Last, in a 6-month soccer trial with early-stage and advanced PCa patients, 79 214 out of 238 eligible participants were recruited with a retention rate of 95% and attendance of 59% at 6 months.
Therefore, the preliminary evidence suggests that participation in supervised, well-tailored sport programs by cancer patients is feasible and is of low risk, and may only result in mild sport injuries that are common for people engaging in any form of physical exercise. Nevertheless, additional studies are necessary to develop this evidence base.
Opportunities and Recommendations for Sport Programs in Cancer
Classification of sports based on the principle of specificity is an essential prerequisite underpinning the effectiveness of a sport program for cancer management, as sport activities with homogeneous physical and physiological profiles will result in similar responses and adaptations for the participants. Almost all sports require a combination of coordination, strength/power, speed, and aerobic and anaerobic fitness. In accordance with the predominant characteristics involved in a particular sport and the potential physiological loads imposed by motor activity and movement demands,107-109 sport disciplines can be divided into 4 categories, that is, skill-dominant/precision sports, strength/power-dominant sports, endurance-dominant sports, and mixed sports. However, it should be noted that there are multiple ways to categorize sports. 110 Although sport activities within a category share a similar profile, variability in the demands of different energy systems and movement components may still exist across the different sports within a category due to intrinsic patient-centered characteristics, such as skill level and motivation, and extrinsic factors such as skills/competitiveness of the opponent/competitors or fellow team members and environmental factors.
Skill-dominant/precision sports. We define skill-dominant/precision sports as activities requiring a higher level of bodily coordination and skills to achieve a precise execution of movement (eg, golf, table tennis, gymnastics, diving, and archery). In general, skill-dominant sports include only a short bout of action that predominantly requires cognitive function, body control, quick reaction, and physical strength with only modest stress to the cardiorespiratory system.
Strength/power-dominant sports are activities requiring a higher level of physical strength and power output (eg, weightlifting, speed skating, shotput, sprinting, and triple jump). In general, strength/power-dominant sports include rapid forceful motion against body weight and/or an external resistance, which predominantly requires a higher rate of force development.
Endurance-dominant sports are activities requiring both cardiorespiratory and muscle endurance (eg, canoeing, road cycling, swimming, rowing, and orienteering). In general, endurance-dominant sports basically involve cyclic motion that requires sustained, repeated contraction of large muscle groups and maximum involvement of the cardiorespiratory system with comparatively lower demands on muscle strength and power.
Mixed sports. We define mixed sports as activities requiring involvement of a wide range of systems with nearly equal demands in technical skills, strength/power, speed, aerobic, and anaerobic fitness (eg, soccer, basketball, ice/field hockey, rugby, and boxing). In general, mixed sports include an assortment of repetitive dynamic movement components such as jogging, sprinting, acceleration, deceleration, stopping and cutting, jumping, and so on.
Evidence indicates that people participating in different types of sport demonstrate different physical and physiological adaptations. For example, a cross-sectional study 111 in frail older women indicated that participating in table tennis resulted in better cognitive function than nonparticipants. In addition, older golfers showed better balance control than age-match nongolfers. 112 Male and female athletes in higher resistance and impact-loading sports consisting mainly of strength/power-dominant (such as judo and karate) and mixed sports (such as soccer) show greater muscle mass and bone density compared with non–weight-bearing or low-impact sports (such as swimming and water polo) with more increases observed in athletes of longer participation and at sites of more intensive stress.113-116 In a similar fashion, sport activities with higher aerobic components (such as swimming) elicit more improvement in cardiopulmonary function. 117
Accordingly, along with the aforementioned positive changes in cancer patients undertaking various sport-based programs,71,73,75-78,80,81 we propose that sport activities with similar profiles and comparable exercise load stimulus would also result in similar beneficial effects in cancer patients. Specifically, cancer patients participating in endurance-dominant sports would predominantly improve cardiovascular fitness, and cancer patients participating in strength/power-dominant sports would predominantly gain lean mass, muscular strength, endurance, and bone density. For mixed sports, positive adaptations in circulatory and respiratory systems as well as in body composition and functional ability would be elicited. In addition, cancer patients with treatment-related cognitive deficit would benefit from undertaking skill-dominant/precision sports. However, as variability of demands in the body systems exist across sports within a category, substantial secondary adaptions would also be possible in cancer patients through regular participation.
Given the paucity of evidence with regard to sport participation for cancer management as well as the diversified characteristics across sports, specific recommendations on dosage for a particular sport in cancer patients still remains impractical. However, the general guidelines for physical exercises proposed by ACSM 22 and ESSA 93 could be considered as a basis for dosage prescription (ie, weekly 60-150 minutes of exercise at a moderate to vigorous intensity).
Additional Considerations
Several other factors should be taken into account when planning and implementing a sport program for cancer patients. First, a sport program should always be practical for cancer patients. To this end, it is vital to simplify technical skills, reduce exercise load, and avoid high-risk activity components (such as body contact) of a sport activity according to participant’s physical capacity at different phases of treatment. 118 For example, in mixed sport events (such as soccer and basketball), playing rules, field-of-play, number of players per side, and game duration can be adjusted to manage the training load and avoid risk factors. Second, a selected sport activity should appeal to potential participants. In this regard, the participant’s personal preference and previous experience in sport participation should be taken into consideration when prescribing sport programs.118-121 Third, a separate familiarization period before regular sport participation may be required for participants to learn and acquire the necessary skills related to the subsequent sport program, which should also be regarded as an indispensable part of a sport program to further ensure safety and maintain the participant’s playing interest and enjoyment as well as facilitate exercise continuance. Finally, in order to increase the participation rate of cancer patients in a sport program, the prevalence of different sport events within a region and availability of facilities should be considered. 122 For example, rugby is one of the most played and widely watched sports in Australia among men and women across all age groups, while basketball is one of the most popular sports in the United States. However, apart from referring to sport popularity and facility availability, provision of a list of sport program options for cancer patients may assist in contributing to a higher sport uptake and adherence rate. 123
Despite all these considerations, a cautious attitude should still be taken when implementing sport programs in cancer patients. Overall, for health and fitness, it is highly recommended for practitioners who are interested in conducting sport medicine programs in cancer patients to follow the general contraindications and reasons for starting and stopping exercise proposed in the ACSM roundtable statement. 22 In addition, special attention needs to be attached to patients undergoing active treatments and when implementing sport programs outdoors.
Perspectives and Future Directions
Although the benefits of physical exercise for cancer management has been well established, insufficient engagement and low adherence rate in cancer patients often compromise the beneficial effects of regular exercise training. Evidence to date indicates that in cancer patients the lack of ability and motivation, as well as the tedious and repetitive nature of exercise, are among the frequently reported barriers to regular exercise participation.124-128 Conversely, a supportive environment during exercise is a facilitator to regular engagement in physical exercise.124,128,129 Sport participation is recognized as an enjoyable experience and intrinsically involves many motivational aspects such as personal challenge, competitive climate, and goal orientation, and may facilitate exercise participation and adherence in cancer patients.
Sport participation is associated with lower risk of cancer and cancer-related death. Based on preliminary evidence, participating in sport activities is feasible and can be well tolerated by cancer patients. In addition, sport participation can play a vital role in countering a range of physical and psychological adverse effects related to the cancer and its treatments. Therefore, sport participation could be considered as an alternative strategy to frequently used fitness exercises in the prevention and management of cancer. We believe that sport participation as adjunct therapy for cancer management would especially appeal to those with previous and current experiences in sport including sports fans as well as retired professional/recreational athletes. In general, cancer patients are encouraged to participate in different types of sports according to their personal circumstance and preference.
Although there is a developing body of evidence that sport participation can enhance physical and psychosocial functioning in cancer patients, it needs to be recognized that the evidence base contains few RCTs with only a few sports investigated and is dominated by pilot studies with only small sample sizes. Therefore, at this stage, the efficacy of sport participation in cancer management should be interpreted with caution, and further work in this field is required to develop the evidence base. Robust RCTs are required to investigate the effectiveness of different sport activities in cancer patients at different stages of the cancer continuum and while receiving different treatments. In addition, sport-specific guidelines and practical strategies in planning sport programs are warranted. At present, only a handful of sports have been examined in cancer management with the majority being team-based. Therefore, comparative studies on the beneficial effects between individual, partner-based, and team-based sports are also required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.