
Abstract
Hyperthermia is often used in combination with chemotherapy and radiotherapy for cancer treatment. Recently, immunotherapy has become a popular research area, breaking exciting new ground with concurrent immunotherapy and hyperthermia. Much evidence has demonstrated the effectiveness of multidisciplinary synergistic therapy, and the underlying mechanism has been gradually explored. In this review, we focus on the mechanism of various cancer treatments in the current literature and recent advances in hyperthermia. Additionally, we review clinical studies of hyperthermia combined with other therapies in the previous 10 years and propose future prospects for hyperthermia in multidisciplinary synergistic therapy.
Keywords
Introduction
Hyperthermia refers to the use of heat and its secondary effects produced by raising the temperature of the whole body and/or local tumor tissue to treat malignant tumors. In clinical practice, it can be used alone or in combination with other methods such as radiotherapy (RT), chemotherapy, and immunotherapy. Hyperthermia is mainly divided into 3 categories according to the manner of administration: local, regional, and whole-body hyperthermia. Local hyperthermia is defined as increasing the temperature of local tumors and is often used for skin or natural body surface tumors, such as cervical lymph node metastases and skin tumors. Regional hyperthermia is achieved by increasing the perfusion of organs or limbs with heated liquid, such as intraperitoneal hyperthermia, which is often combined with chemotherapy, and radiofrequency in deep tumors. Whole-body hyperthermia is mostly applied to treat metastatic tumors. 1 According to different heating media, it can be divided into microwave heating therapy, infrared heating therapy, magnetic heating therapy, and photothermic therapy, among others. 2 Although increasing studies are focusing on the mechanism of hyperthermia, many details still remain unclear. At present, hyperthermia is widely used in the clinic, but how to achieve a more appropriate target temperature, more accurate target location, and an optimal treatment strategy remain a great challenge.
Mechanisms of Hyperthermia Alone or in Combination With Other Therapeutic Methods
Mechanisms of Hyperthermia
Hyperthermia is a therapy that consists of heating the lesion site to treat tumors based on the differential response of tumor tissue and normal tissue to heat.3,4 Blood vessels in the tumor are different from those in normal tissues. The normal vascular system is a network of arterioles, capillaries, and veins. In contrast, tumor blood vessels assemble into a chaotic network of capillaries, most of which lack smooth muscle layer and innervation. 5 This vascular abnormality leads to a hypoxic environment inside the tumor, and a mild temperature (37°C to 42°C) can lead to local vascular dilation and increased vascular perfusion to improve oxygenation of tumors, thus mitigating inflammation and deep tissue hyperemia, moreover reducing the excitability of pain-sensing nerves to relieve pain. 3 At temperatures above 42°C, the tumor vasculature is directly damaged by increased permeability, which results in fluid and protein accumulation in the microenvironment and contributes to elevated interstitial fluid pressure, in turn leading to vessel compression and further vascular perfusion reduction. Furthermore, the mechanism responsible for the vascular injury is activated, and tumor growth and proliferation are inhibited during the heating process. 6 In addition, when the temperature exceeds 37°C, the membrane fluidity increases, thereby affecting its permeability. Changes in the cytoskeleton and membrane structure can destroy the tumor cell movement, intracellular signal transduction, and further inhibit tumor growth and metastasis. 7
Mechanisms of Hyperthermia Combined With Chemotherapy
The combination of hyperthermia and chemotherapy agents can lead to an overall enhancement of drug cytotoxicity. An artificial increase in tissue temperature can lead to higher fluidity of the bilayer of phospholipids in tumor cells, which in turn facilitates their drug permeability. 8 Moreover, the structure of the cell membrane changes, the membrane viscosity decreases, and cellular uptake of drugs rises in cancer tissue.9,10 Studies have demonstrated that hyperthermia (43°C) has a synergistic interaction with cisplatin (cPt) on cell growth inhibition, probably because it can modulate the function of the cPt transporter Ctr1, leading to increased cPt uptake with enhanced cytotoxicity.11-13 Carboplatin and oxaliplatin show only additive effects. Based on the above-mentioned mechanisms, regional chemotherapy combined with hyperthermia has been developed, such as hyperthermic intraperitoneal chemotherapy (HIPEC) or hyperthermic intravesical chemotherapy (HIVEC) of the bladder, in which heated chemotherapy agents are perfused into the abdominal cavity or bladder to exert antitumor effects by increasing their thermodynamic effects.14,15
Mechanisms of Hyperthermia Combined With Radiotherapy
Hyperthermia increases the sensitivity of tumor cells to ionizing radiation. First, it is well known that hypoxia is related to radioresistance, and improvement of the hypoxic environment of tumor tissues can lead to increased radiosensitivity of tumors. This phenomenon can be attributed to the ability of hyperthermia to reoxidize hypoxic tumor cells by increasing blood flow, so that tumor cells lose the protection of the hypoxic environment during RT. Only an appropriate temperature can improve oxygenation and vascular perfusion of tumors, resulting in radiosensitization. In contrast, a high temperature will reduce blood perfusion, damage blood vessels, and aggravate cell hypoxia, which is associated with decreased radiosensitivity. 10 Changes in protein structure caused by heat can affect multiple components of cells to varying degrees, thus suppressing DNA damage repair. 16 Hyperthermia induces heat shock protein (Hsp) 70 synthesis and thus interferes with telomere activity. Overexpression of telomerase in tumor cells can stabilize telomeres and prolong the life of cells. Therefore, hyperthermia indirectly inhibits the activity of telomerase and promotes cancer cell apoptosis. 17 The sensitivity of tumor cells to ionizing radiation is influenced by their phases of the cell cycle. G0 and S phase cells are less sensitive to RT injury but more sensitive to hyperthermia.18,19 Furthermore, RT can reduce the thermal tolerance of tumor cells and improve the curative effect of hyperthermia.
Mechanisms of Hyperthermia Combined With Immunotherapy
Studies have also revealed the role of temperature in facilitating the efficacy of immunotherapy. Accumulating evidence indicates that the immunosuppressive state of the tumor microenvironment is supported by hypoxia within tumors.20-22 Using the potential ability of heat to modulate reoxygenation of the targeted tumor site plays a fundamental role when coupled with immunotherapy. Furthermore, an elevated temperature can not only induce the immune response at the targeted tumor site, but it can also stimulate an antitumor response throughout the body.
There is a growing appreciation that mild hyperthermia has an effect on the functions of innate immune cells. Previous studies have revealed that macrophages can be activated by mild heat through Hsp-mediated enhanced expression of various signaling pathways and oxides, as well as the direct immunogenic influence of mild hyperthermia.23,24 For dendritic cells (DCs), which present antigens to adaptive immune cells, hyperthermia can enhance their proliferation, maturation, and antigen presentation.25-30 Moreover, natural killer cells are activated and show elevated cytotoxicity and recruitment to tumor sites on heating, causing increased tumor cell recognition by natural killer cells.31,32 Adaptive immune cells can also be targeted by heat. Hsp70 activates T-cells by inducing CD69, interferon-γ, and tumor necrosis factor-α, whereas Hsp90 and Hsp27 play an important role in antigen presentation among T-cells and DCs, and can serve to activate antitumor immune responses.33-36 The proliferation and activation of B-cells may be enhanced after exposure to elevated temperatures by activating the extracellular signal-regulated kinase and nuclear factor-κβ signaling pathways and inducing heat-shock transcription factor 1 expression.37-40
During an immune response, lymphocytes and leukocytes infiltrate the tissue and interact with DCs after activation of innate immune cells. Several investigations have revealed a barrier to CD8+ T-cell infiltration in tumor sites. Hyperthermia can increase the trafficking of immune cells across the tumor vascular barrier to access the tumor and immune organs.41-44 This process probably occurs through elevated integrin- and selectin-mediated adhesion, stable binding to intercellular adhesion molecule-1, as well as increased endothelial cell activation and permeability.45,46
Clinical Use of Hyperthermia
In the 18th century, doctors found that tumors began to shrink when cancer patients suffered from febrile diseases. Thereafter, research on hyperthermia for tumor treatment never stopped. In the past few decades, hyperthermia has played a benign role in the treatment of multiple cancers, such as head and neck, breast, brain, bladder, rectum, lung, skin and accessory, ovary, various types of sarcomas, and other tumors.
Hyperthermia combined with chemotherapy and RT changed the original single treatment mode and broke through its limitations, thus enhancing the therapeutic effect and becoming a ray of dawn for tumor treatments.2,47-53 For different tumors, the specific treatment methods and curative effects are also different. In this article, we review the clinical trials and case reports of hyperthermia combined with chemotherapy, RT, chemoradiotherapy, and immunotherapy over the most recent 10 years (Table 1), and we discuss and summarize the results of these existing trials to provide new ideas for clinical practice.
Published Trials of Hyperthermia Combined With Other Therapies.
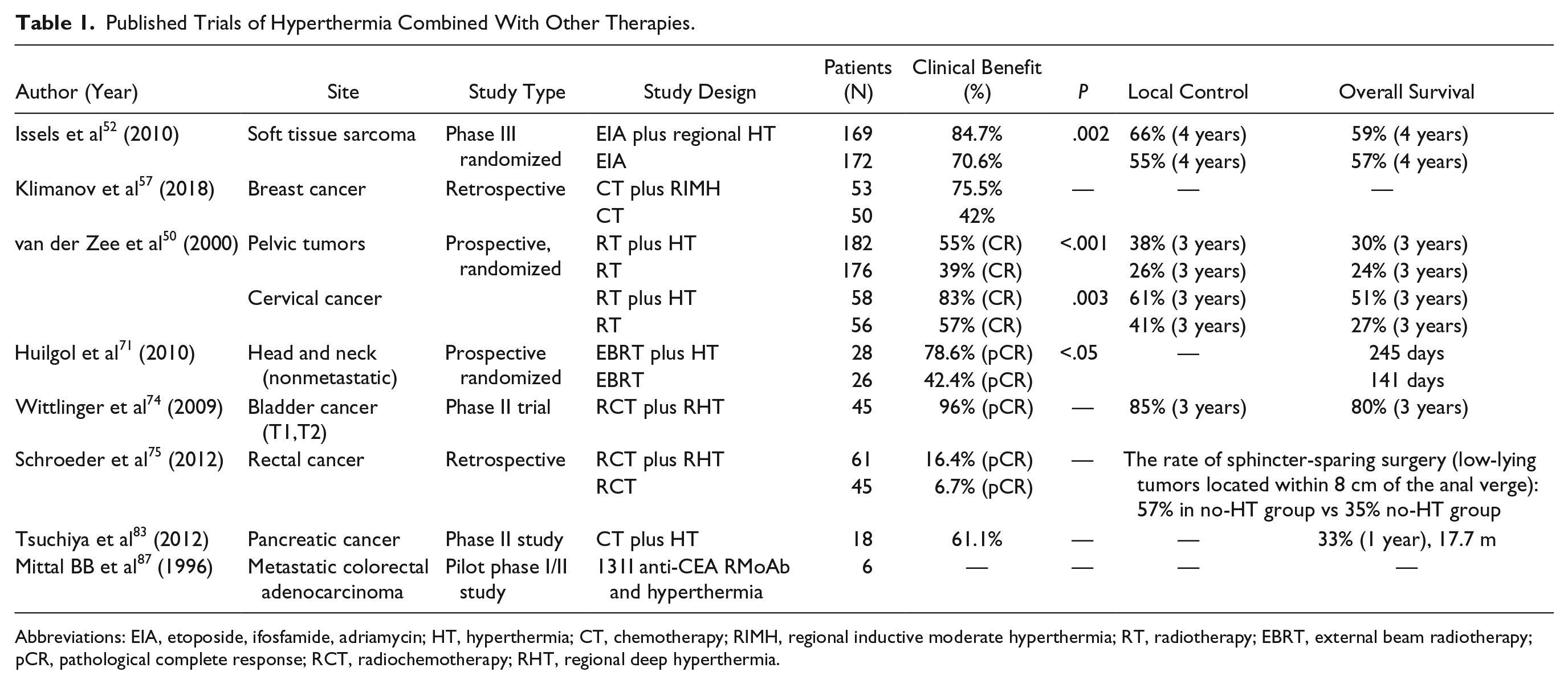
Abbreviations: EIA, etoposide, ifosfamide, adriamycin; HT, hyperthermia; CT, chemotherapy; RIMH, regional inductive moderate hyperthermia; RT, radiotherapy; EBRT, external beam radiotherapy; pCR, pathological complete response; RCT, radiochemotherapy; RHT, regional deep hyperthermia.
Hyperthermia Combined With Chemotherapy
Hyperthermia combined with chemotherapy is widely used in clinical practice and has been widely studied in soft tissue sarcoma (STS). In a retrospective study, 61 cases of high-grade STS patients were included, among whom 28 received preoperative neoadjuvant chemoradiotherapy (CRT) and 33 received neoadjuvant chemotherapy plus hyperthermia (HCT). Hyperthermia aiming at a target temperature of 42°C was usually conducted on the first and third days of chemotherapy for 60 minutes, with isocyclophosphamide applied during or immediately after local hyperthermia. There were no significant differences in tumor response between the 2 groups (P = .67), whereas for toxic reactions, postoperative wound dehiscence and complications in the CRT group were markedly higher than in the HCT group. Furthermore, there were no significant differences in overall survival (OS), local control, and freedom from distant metastases over 2 years between the 2 groups.54,55
In a more recent trial, the prospectively randomized NCT 00003052 phase III multicenter trial, 341 patients with untreated localized high-risk STS were enrolled, of whom 169 received neoadjuvant chemotherapy consisting of etoposide, ifosfamide, and adriamycin (EIA) plus regional hyperthermia, and the remainder received EIA alone. After induction therapy, the tumor response was evaluated by imaging, and the best local treatment (surgery and/or RT) was selected, followed by another 4 cycles of induction therapy. Regional hyperthermia was performed on the first and fourth days of each chemotherapy cycle at a target temperature of 42°C for 60 minutes. The relative hazard for local progression or death between patients receiving combined therapy versus EIA alone was 0.58 (95% confidence interval [CI] = 0.41-0.84; P = .003), with an absolute difference at 2 years of 15% (95% CI = 6% to 26%; 76% vs 61%). Among them, 169 patients with nonextremity tumor showed a more noteworthy benefit from regional hyperthermia. In the safety evaluation, the combined treatment group did not show an increased incidence of adverse reactions of chemotherapy. Therefore, this trial demonstrated that local hyperthermia could improve the efficacy of chemotherapy for high-risk localized STS. 52 In addition, subgroup analysis revealed a greater benefit in the patients who underwent surgical resection. 56 Despite some problems in the above-mentioned clinical trials, for example, the combined treatment group received more chemotherapy than the chemotherapy alone group; this is the first phase III clinical trial to investigate whether chemotherapy combined with hyperthermia or chemotherapy alone is more effective in patients with STS. To some extent, the results have indicated that the combination of hyperthermia and other therapies is a good therapeutic strategy, but the timing of hyperthermia combined with chemotherapy and the method of hyperthermia require further experimental study.
Regional inductive moderate hyperthermia in combination with chemotherapy can improve the therapeutic effect of breast cancer patients with multiple liver metastases. 57 The MegaTherm apparatus was set in the metastatic lesion to generate electromagnetic irradiation, with a temperature less than 40°C lasting for 30 minutes. The magnetic field generated during regional inductive moderate hyperthermia can significantly accelerate the interaction between chemical molecular oxygen and cellular metabolites, leading to remarkably enhanced oxidative stress in tumors and their microenvironments and increased apoptosis induced by hyperthermia.58,59
For advanced ovarian and colorectal cancers, extensive peritoneal metastasis is often a sign of a poor prognosis. Among these patients, peritoneal recurrence is a major problem. Owing to the high selectivity of intraperitoneal administration and the pharmacokinetic characteristics of local chemotherapy, a positive effect of HIPEC on the survival of patients with advanced ovarian and colorectal cancer has been reported with increasing frequency.60,61 HIPEC is a local treatment to clean the abdominal cavity with hyperthermic chemotherapeutic drugs, which is based on the direct cytotoxicity of heat to cancer cells and the indirect increase in the toxicity of anticancer drugs. Moreover, HIPEC must be combined with complete surgical resection of peritoneal cancers. 62 There is increasing evidence that HIPEC is beneficial for the prognosis of ovarian peritoneal metastasis. In a multicenter retrospective study, 56 cases of recurrent epithelial ovarian cancer patients who were treated with cytoreductive surgery combined with HIPEC were included. The median follow-up time was 23.1 months. The median OS and progression-free survival were 25.7 months (95% CI = 20.3-31.0) and 10.8 months (95% CI = 5.4-16.2), respectively. The 5-year OS and progression-free survival were 23% and 7%, respectively. 63 Nevertheless, the median survival rate was 11.2 months, and the 3-year survival rate was 18% in patients with recurrent ovarian cancer who received cytoreductive surgery alone. 64 For patients with advanced ovarian cancer with peritoneal metastasis, the combination therapy can be beneficial for a wider subset of patients than conventional secondary debulking surgery alone. Nonetheless, these data should be further evaluated in randomized clinical trials due to the limitations of the research program design and the small sample size.
Therefore, regional hyperthermia is often used in combination with chemotherapy, generally not alone, in patients with advanced nonoperative tumors. Regional hyperthermia is usually given on the first and last day of the chemotherapy cycle for 60 minutes at 40°C to 42°C.
Hyperthermia Combined With Radiotherapy
Hyperthermia alone or combined with RT has special significance in the treatment of locally advanced cervical cancer. Evidence has shown that hyperthermia can improve the survival and reduce toxicity in patients with locally advanced cervical cancer.65-67 In 2000, the Lancet published a Dutch Deep Hyperthermia Group trial, which was designed to treat locally advanced pelvic tumors with RT alone or combined with hyperthermia. Hyperthermia was prescribed 1 to 4 hours after RT once weekly, for a total of 5 times. Treatment was continued for 60 minutes after the tumor reached 42°C, usually up to 90 minutes. This multicenter phase III trial showed that the 3-year survival rate nearly doubled from 27% to 51% in patients with locally advanced cervical cancer after combining RT with hyperthermia. 50 Therefore, for patients with locally advanced cervical cancer, the combination of hyperthermia and RT should be considered to improve the therapeutic effect. Not only does the temperature of the hyperthermia contribute to the effectiveness of the treatment, but the timing also matters. Moreover, the time interval between the external beam RT and hyperthermia is related to the recurrence risk and OS. The 3-year recurrence rates in the short-term group (<79.2 minutes) and long-term group (>79.2 minutes) were 18% and 53% (P = .021), whereas the 5-year OS rates were 52% and 17%, respectively (P = .015). There was no significant difference in toxicity (P = 1.00) between the 2 groups. 68 Preclinical evidence indicated that the enhanced radiosensitivity of hyperthermia was remarkably reduced if the interval between RT and hyperthermia was longer than 1 to 2 hours, which may be because most DNA damage was repaired within 2 hours, resulting in a reduction of long-term-interval-heat therapeutic effects. 69
Concerning head and neck tumors, RT is the main treatment, but only 20% of patients with locally advanced recurrent head and neck tumors can be treated with surgery or re-irradiation therapy, and the disease control rate after retreatment is only 26% to 52%. Although the combination of RT and chemotherapy improved survival, toxicity was increased. 70 However, there is growing evidence indicating that heat improves the prognosis of head and neck tumors. Huilgol et al reported a phase III clinical trial in which 56 patients with locally advanced head and neck cancer were randomly admitted for RT either with (n = 28) or without (n = 26) regional hyperthermia. The complete response rate of the RT-alone group and the combination group were 42% and 79% (P < .05), respectively, and no obvious toxicity reaction was observed. 71
Radiotherapy is often combined with deep hyperthermia, mostly for head and neck tumors and other radiosensitive malignant tumors. Hyperthermia is often carried out in the interval of RT, usually 1 to 2 hours after RT, with the temperature reaching 42°C and lasting for 60 to 90 minutes. Special devices are often required to achieve deep hyperthermia. For example, the HYPERcollar applicator was invented and improved continuously to achieve deep local head and neck hyperthermia, with verified therapeutic effects in multiple studies.70,72,73
Hyperthermia Combined With Chemoradiotherapy
Hyperthermia often increases sensitivity to conventional chemoradiotherapy in some tumors that were previously less sensitive to chemoradiotherapy alone. The combination of hyperthermia and chemoradiotherapy has been widely studied in bladder and rectal cancer, among others.
In 2009, Wittlinger et al published a retrospective study of 45 patients with high-risk T1 and T2 stage bladder cancer. After transurethral resection, the patients received whole bladder and pelvic lymph node RT for 5 consecutive days a week and regional deep hyperthermia (RHT) once a week. RT was started within 60 minutes after RHT. During the whole course of RT, the lowest and highest frequencies of hyperthermia treatment were 5 and 7 times, respectively. Moreover, cPt combined with 5-fluorouracil chemotherapy was scheduled for the first and fifth weeks of treatment, and cPt was also applied to RHT. The median follow-up was 34 months (range = 12-60), and the complete response rate was 96% (43/45). The 3-year local recurrence-free survival rate was 85%, OS rate was 80%, disease-specific survival rate was 88%, metastasis-free survival rate was 89%, and bladder-preserving rate was 96% (43/45). Overall, the patients were satisfied with their quality of life. 74
Schroeder et al demonstrated that the potential use of regional hyperthermia in combination with neoadjuvant chemoradiotherapy can improve the pathological complete response (pCR) rate and selection of better surgical options for rectal cancer. Between 2007 and 2010, 106 patients with locally advanced rectum cancer received neoadjuvant chemoradiation with (n = 61) or without (n = 45) regional hyperthermia. The patients received 5 weeks of RT, 5 times per week. Regional hyperthermia was administered immediately after RT, once or twice a week, with a target temperature of 40.5°C and a duration of at least 60 minutes and no longer than 90 minutes. In addition, continuous infusion of 5-fluorouracil was administered in the first and fifth weeks of treatment. Low anterior or abdominoperineal resection with total mesorectal excision were performed 4 to 6 weeks after the end of chemoradiotherapy. The pCR rate reached 6.7% and 16.4% in the radiochemotherapy group and hyperthermia combined with radiochemotherapy group, respectively, and the pCR rate increased 22.5% in patients who received at least 4 cycles of hyperthermia treatments (P = .043). A particularly interesting finding of this study was that patients with low rectal tumors near the anal verge showed better sphincter preservation in the hyperthermia combined with radiochemotherapy group (57% vs 35%, P = .077). 75 Moreover, several studies have also demonstrated a better local control rate and survival benefit of the combination of preoperative neoadjuvant chemoradiotherapy and hyperthermia than chemoradiotherapy alone for rectal cancer patients.76,77
In clinical practice, RHT combined with radiochemotherapy has been shown to be an effective sensitizer for chemoradiotherapy, which can be applied in various types of tumors. Chemoradiotherapy is carried out according to clinical guidelines, while hyperthermia is usually performed immediately after RT, once or twice a week. Chemotherapeutic drugs are infused into the body during the hyperthermia process. In addition, the regional temperature should be monitored continuously during heating. After reaching the target temperature, hyperthermia should be carried on for at least 60 minutes and not exceed 90 minutes. Typically, the temperature achieved in 90% of tumor-related measurement points (T90) and the cumulative equivalent minutes at a reference temperature of 43°C (CEM T43) serve as effective indices.
Hyperthermia Combined With Immunotherapy
In recent years, immunotherapy has been widely praised, but its curative effect is still limited by tumor immune escape. Tumor immune escape refers to tumor cells that can avoid recognition and attack by the immune system by changing themselves or their microenvironment. The complex network of the tumor microenvironment significantly weakens the efficacy of immunotherapy, making it difficult to initiate immunotherapy in solid tumors. A crucial feature of the microenvironment that promotes tumor immune escape is the lack of tumor antigen recognition and antitumor T-cells. 78
Recent studies have shown that immunotherapy is more effective when performed in combination with other therapeutic approaches. In 2018, Kleef et al reported a 50-year-old woman with advanced triple-negative breast cancer who had postoperative axillary lymph node metastasis and even bilateral lung metastasis after standard RT. The gene analysis revealed wild-type BRCA1, with a 61% Ki-67 index, suggesting a high proliferation potential. The patient received a combination of low-dose checkpoint inhibitors, nivolumab (0.5 mg/kg) and ipilimumab (0.3 mg/kg), accompanied by local hyperthermia once a week, over 3 weeks, and high-dose interleukin-2–induced whole-body hyperthermia for 5 days. After 1 year of treatment, the total gene expression in the resected metastatic lymph node showed that immune surveillance was enhanced, with several overexpressed checkpoint genes and active cytokines (eg, interleukin-2, interferon-γ, transforming growth factor-β, etc). Overall, the patient was completely relieved, presenting with only temporary Health Organization Grades I-II diarrhea and skin rash, and the OS period was 27 months from the beginning of treatment. 79
For pancreatic cancer, owing to its anatomical location and histological characteristics, the penetration of cytotoxic drugs is restricted, causing a severe hypoxic microenvironment within the tumor and thus inhibiting the efficacy of RT and chemotherapy, leading to a poorer therapeutic effect compared with other solid tumors.80,81 Moreover, the effectiveness of immunotherapy is also greatly reduced because of the presence of a large number of immunosuppressive cells in the microenvironment of pancreatic cancers. 82 There is abundant evidence that hyperthermia can enhance the efficacy of RT and chemotherapy in pancreatic cancer.83-85 A recent study verified that anti-PD-1/PD-L1 immunotherapy combined with RT and hyperthermia can enhance the antitumor effect. 86 Nonetheless, there is no published clinical data available on pancreatic cancer based on the tripartite treatment of RT, hyperthermia, and immunotherapy, which is supported by only animal experiments and preclinical data. One explanation for the enhanced antitumor effects of tripartite-combined therapies involves the repair inhibition of RT-induced DNA damage and improvement of the hypoxic environment of tumors, leading to increased radiosensitivity. In contrast, appropriate hyperthermia can also lead to the release of tumor antigen, recruitment of immune cells, and improvement of immune function. Hence, the triple therapy of RT, hyperthermia, and immunotherapy may become a new strategy for the treatment of pancreatic tumors, but more clinical trial data are needed to confirm it. 87
Conclusions and Future Directions
At present, hyperthermia has been widely used in clinical practice, and it has achieved good efficacy in clinical trials examining a variety of malignant tumors. Moreover, many researchers have tended to explore the combination of hyperthermia and other therapies. Hyperthermia plays an antitumor role by killing cells directly, increasing drug permeability, enhancing radiosensitivity, disrupting DNA repair, releasing antigens, and activating immunity. The key parameters of hyperthermia are the temperature and heating time, and therefore, real-time multipoint temperature measurement is crucial. Currently, conventional local hyperthermia is usually carried out for 60 to 90 minutes at a target temperature of 39.5°C to 43°C, while whole-body hyperthermia often lasts for no less than 90 minutes at 39.5°C to 42°C. In addition, considering individual differences, the duration of hyperthermia should be appropriately extended at a lower temperature for patients with poor tolerance, whereas for patients with good tolerance, the duration can be appropriately shortened at a higher temperature.
A mathematical model has validated a nonlinear relationship between the concentration of extracellular Hsp and the number of dead cells, along with a rising temperature. Through the application of hyperthermia, tumor antigens are released by extracellular Hsps during the process of tumor cell necrosis to activate antitumor immunity. This induced immunity has been further demonstrated to contribute to the control of recurrence and metastasis of tumors.88,89 With the increase in temperature, the optimal antitumor immune effect can be achieved only in a narrow thermal dose range. 90 Nevertheless, it is still a great challenge to apply appropriate and sufficient heat energy to the target tumor without affecting normal tissue and accurately detect the temperature of the target position in vivo. Additionally, more data are needed to help guide the clinical practice of hyperthermia, such as how to combine it with other therapies, the sequence, and the interval between therapies, among others.
The recent publication of a large number of clinical trials on tumor immunotherapy has attracted the attention of the medical community. Previous in vivo and in vitro experiments have confirmed that hyperthermia can improve the expression of Hsp and activate nonspecific and specific immune responses in vivo. In a study conducted by Sottile et al, MMR-deficient (MMR−) and MMR-proficient (MMR+) cell lines were exposed to cPt combined or not with hyperthermia. Hyperthermia pretreatment increased cPt resistance in MMR− cells (1.42-fold), whereas enhanced cPt sensitivity and nuclear colocalization of Hsp27 and Hsp72 were observed with MLH1 and MSH2 in MMR+ cells. 91 The sensitization of hyperthermia to chemotherapy or immunotherapy may be related to the status of MMR, and further studies are needed to identify the dominant beneficiaries of hyperthermia and how to more effectively combine chemotherapy with immunotherapy.
Furthermore, hyperthermia involves a variety of heating media to meet clinical needs. At present, photothermic therapy and magnetic hyperthermia (MHT) are the frontiers of this research field. MHT refers to the use of magnetic nanoparticles exposed to a magnetic field to generate heat, thus inhibiting tumor survival through apoptosis and necrosis pathways. 92 The key of MHT is to select appropriate magnetic nanomaterials, construct a thermomagnetic-induced drug release polymerization platform, and stabilize the local heat transfer and subsequent release of therapeutic drugs. At present, research on MHT has made great progress, which includes nanomagnetic fluid interventional therapy and nanothermosensitive liposome–encapsulated chemotherapy drug–targeted chemotherapy. The former refers to the injection of magnetic nanomaterials into the center of tumors and the application of an alternating magnetic field to produce high temperature above 60°C in the local area of tumors, to achieve the purposes of the tumor treatment. The latter refers to the use of nanothermosensitive liposomes to encapsulate chemotherapeutic drugs and then use the temperature to control drug release. A phase II clinical trial is now being conducted to investigate nanothermo-therapy in glioblastoma multiforme. The challenge of magnetic nanoparticles lies in the associated biological toxicity, detection of the target and surrounding temperature, and more important, the study of the drug release and further immune activation mechanism. Photothermal therapy is a method in which materials is injected with high photothermic conversion efficiency into the human body, followed by its accumulation near tumor tissues through targeted recognition technology and the later conversion of light energy into heat energy under external light source irradiation (usually near-infrared light) to kill cancer cells.
For the different types of hyperthermia mentioned above, hyperthermia alone should be augmented with multiple synergistic strategies, such as MHT combined with phototherapy, to enhance its effect. In the field of cancer treatment, the increasing development of multidisciplinary synergistic therapies and the proposal of precision medicine challenge current treatments. We should take a new look at the development and prospects of hyperthermia in cancer therapy.
Footnotes
Author Contributions
YC and SW analyzed the previous literature regarding hyperthermia, and drafted the manuscript. LY, NZ, and MY provided a critical reading of the manuscript and revised it. YY revised the manuscript and approved the final version of publication. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.