
Abstract
Introduction
Cancer is the second leading cause of death in the United States; 1 in every 4 deaths is attributed to it. In 2018 alone, it is estimated that there will be 1 735 350 new cancer cases. 1 The toll of cancer, both physically and economically, makes it a high health priority. In fact, the rising cost of cancer care is a primary focus for patients, payers, and providers alike. Over the past 40 years, the median monthly costs of cancer drugs have risen from less than $100 in 1965 to 1969, to more than $10 000 in 2016. 2 This is partly due to the escalating costs of clinical trials. 3 The significant and sustained decline in cancer mortality over the past 2 decades, as reported by the American Cancer Society, 1 indicates that these health care expenditures and corresponding treatments are effective. However, as health care costs continue to escalate, the importance of finding innovative ways to reduce cost burden rises accordingly.
Several meta-analyses report that exercise interventions are beneficial for patients undergoing cancer treatment, in that they reduce symptom severity 4 and improve cancer-related fatigue,5-7 cardiac function, 8 muscle weakness, 9 and overall quality of life. 10 However, the focus of exercise oncology research has traditionally been on the efficacy of exercise programming. 11 With cancer mortality rates on the decline, 1 and patients living longer with the chronic and late effects of cancer treatment, economic evaluations of exercise oncology are warranted. As such, the purpose of the present study was to investigate the cost-effectiveness of an individualized exercise program starting early after cancer diagnosis. We hypothesized that individualized exercise training during cancer treatment would lessen symptom severity and improve treatment outcome, leading to a decrease in health care–related expenditure. We recently reported the effects of individualized exercise training during cancer treatment on symptom severity, 4 resulting in significant decreases in depression, fatigue, anxiety, and fear for the future, as well as corresponding improvements in quality of life. 4 In the current investigation, we report the economic evaluation of such a program.
Methods
Setting
ASCEND Innovations is an independent research group that partners with member hospitals in Dayton, Ohio. As part of their partnership agreement, they are granted access to medical data for each member hospital of the Greater Dayton Area Hospital Association (GDAHA). Researchers at ASCEND retrospectively analyzed patient records to statistically demonstrate the impact of exercise oncology during cancer treatment. Records of patients who had participated in the exercise oncology program were drawn from the GDAHA database. Because all subject data were de-identified and there was no way to link health record information back to the patient, this study was considered exempt from institutional review board review.
Subjects
This retrospective analysis involved patients who participated in an exercise oncology program at Maple Tree Cancer Alliance. All patients began participation on referral by their oncologist. They completed 12 weeks of prescribed, individualized exercise that included cardiovascular, strength training, and flexibility components. The intensity level for the cardiovascular exercise ranged from 30% to 45% of the individual’s predicted VO2max. Strength training involved a full body workout, with emphasis on all major muscle groups and employed machines, free weights, and tubing. Patients completed 3 sets of 10 repetitions for each exercise. Flexibility training involved static stretching of all major muscle groups for 15 to 20 seconds at the completion of each workout. Patients met with a trainer once a week and were given instructions on how to remain active at home.
Data Collection
This study leveraged data from GDAHA’s 360° Healthcare Database, which provides over 14 million comprehensive patient encounter observations across 25 regional hospital organizations for the time period of January 2012 to September 2017. Record search criteria aggregated encounters occurring 6 months prior and 6 months after the supportive care enrollment date for each patient. Therefore, 1 year of data were collected for each patient with enrollment occurring at the median. The latest enrollment date for patients to be included in the study was March 31, 2017. The earliest enrollment date matched was November 11, 2014.
Data Analysis
The 3 primary hospital measures leveraged for statistical comparison before and after supportive care enrollment were number of encounters, number of readmissions, and average total charges. A t test was used to compare the before-and-after observations of repeated subjects. All assumptions for the t tests were validated prior to generating results to ensure quality results (continuous dependent variable, independent observations, approximate normal distribution, and absence of outliers). Some measures such as length of stay and number of emergency room (ER) visits did not have a significant incidence rate, so only the change in values are reported. A significance level of P < .05 was used.
Results
Patient Demographics
The resulting dataset consisted of 1493 total hospital encounters for 147 unique patients; 60% of the patients had breast cancer (Figure 1). The average age of these patients was 64.6 years (Figure 2). Figure 3 presents the gender breakdown of the patients. Figure 4 presents the payer mix of the patients who participated in this study.

Types of cancers.

Age distribution of patients.

Gender distribution of patients.

Payer distribution of patients.
Most of the patient encounters were outpatient; of the 1493, only 60 (4%) were inpatient. To demonstrate the effectiveness of supportive care, we focused on 3 primary measures for each patient: number of hospital encounters, readmissions, and total charges. We also looked at length of stay and ER visits, which showed a decrease post enrollment, but did not exhibit enough cases to be statistically relevant.
Length of Stay and ER Visits
Length of stay is typically calculated based on inpatient stays, which accounted for an extremely small percentage of the encounters included in the study. Despite the low numbers, we still found a 6% decrease in the number of inpatient stays and a 19% decrease in the length of stays associated with those admissions following supportive care enrollment. Length of stay nearly decreased by a full day within the post-enrollment encounters. A similar trend was found with the number of ER visits, which decreased by 27%. These data are presented in Table 1.
Patient Encounters Before and After Supportive Care.

Patient Encounters
The 3 primary hospital measures leveraged for statistical comparison before and after supportive care enrollment were number of encounters, number of readmissions, and average total charges (Table 2). The major types of encounters appear to have been similar pre- and post-enrollment, with the most frequent type of diagnosis code for each time period being “Encounter for antineoplastic chemotherapy,” with a total of 72 encounters in the 6 months prior to supportive care and 86 in the 6 months after supportive care at Maple Tree Cancer Alliance. Visualizations of the change in measures for each patient are provided in Figures 5 to 7.
Total Charges Averaged Across All Encounters Before and After Enrollment.

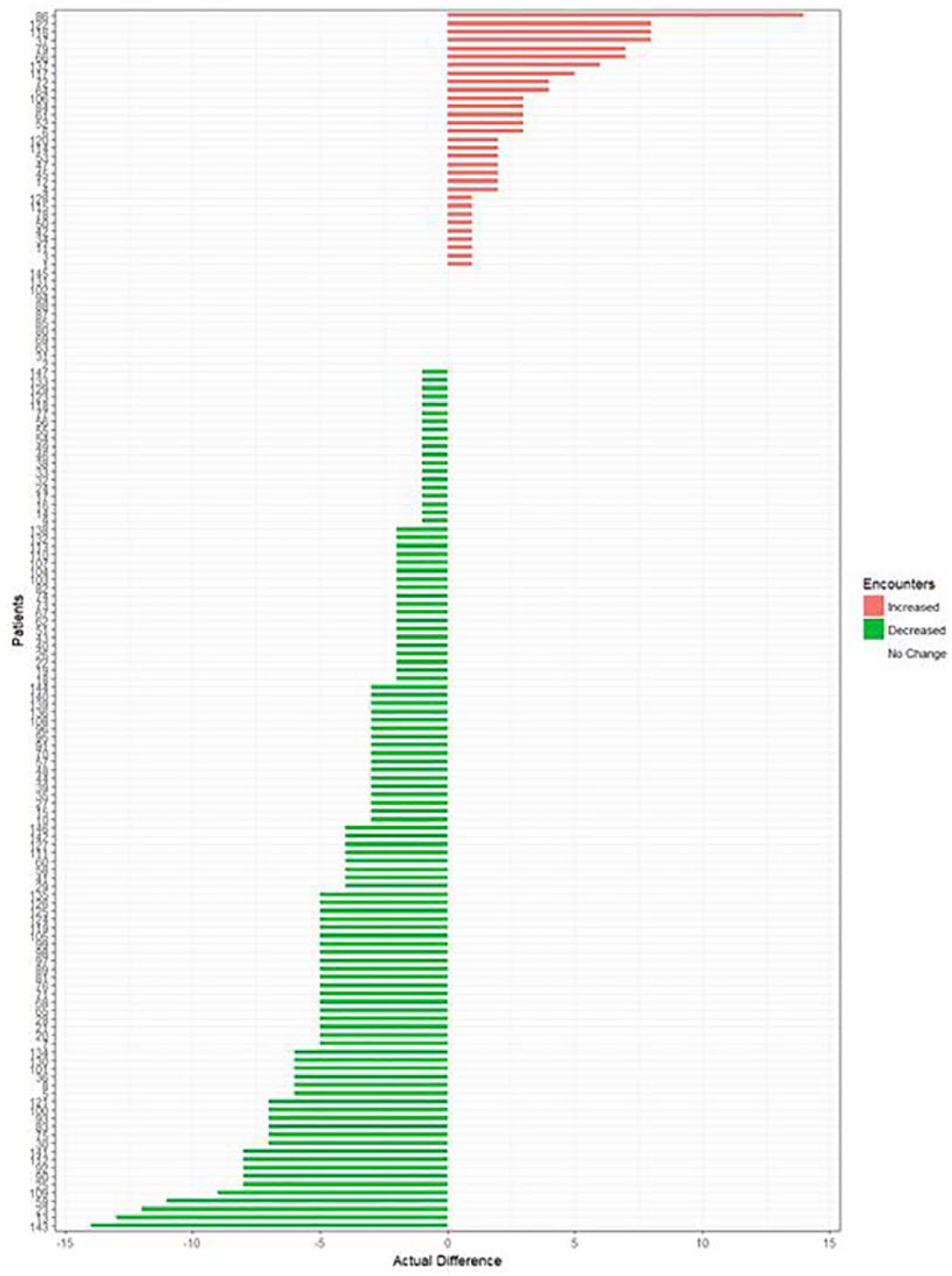
Change in number of encounters 6 months after supportive care enrollment. Actual differences in encounters following 6 months of supportive care (average change = −2.06). Increase in encounters: 31 patients; decrease in encounters: 104 patients; no change: 12 patients. Paired t test results: P < .001; encounters were significantly decreased by supportive care.

Change in number of readmissions 6 months after supportive care enrollment. Actual differences in readmissions following 6 months of supportive care (average change = −1.93). Increase in readmissions: 30 patients; decrease in readmissions: 94 patients; no change: 23 patients. Paired t test results: P < .001; readmissions were significantly decreased by supportive care. Readmission is defined as returning to the hospital within 30 days.

Change in average total charges 6 months after supportive care enrollment. Actual differences in average total charges following 6 months of supportive care (average change = −$2834). Increase in average total charges: 50 patients; decrease in average total charges: 97 patients. Paired t test results: P = .012; average total charges were significantly decreased by supportive care. Average total charges refer to the average cost per encounter over the 6-month study period.
Number of encounters reflects each time a patient had an inpatient or outpatient encounter with a GDAHA hospital. In the data prior to patient enrollment, there were 898 total encounters. Following patient enrollment, the data showed 595 total encounters; a significant (P < .001) 33% decrease. This shows that on average, each patient exhibited 2.06 fewer encounters following enrollment in supportive care (Figure 5).
A readmission for this study is defined as a patient returning to a hospital within 30 days of a previous visit, regardless of inpatient or outpatient status. This does not include rules incorporated in the CMS (Centers for Medicare and Medicaid Services) definition of a readmission. We are purely measuring the frequency with which a patient returns to the hospital. Prior to enrollment, there were 634 readmissions. Following enrollment, there were 351 readmissions; a significant (P < .001) 47% decrease. This shows that on average, each patient had approximately 2 fewer readmissions across the board (Figure 6).
Total charges were averaged across all encounters before and after enrollment (Table 2) to understand the average total charges per encounter; in this case, this is the bill received by the payer before adjustments. The average cost per encounter significantly decreased by $2834 (28%) per patient after enrollment (Figure 7; P = .012).
Discussion
The purpose of the present study was to investigate the cost-effectiveness of an individualized exercise program starting early after cancer diagnosis. The results statistically demonstrate a positive effect of exercise oncology during cancer care, in terms of overall cost per patient pre- to post-intervention. This study also noted nonsignificant reductions in length of stay and ER visits. Of importance is that the measured change in cost between periods does not appear to be due to a change in types of encounters, which suggests lack bias in the cost savings.
Numerous published research articles demonstrate improved patient outcomes as a result of exercise during cancer recovery. Moderate physical activity exercise has a profound effect on energy levels5,12 and increases overall quality of life.10,13 Exercise has also been found to promote a healthy body weight,14,15 decrease oxidative stress, 16 and boost immunity. 17 While the mechanism behind these benefits of exercise is not entirely clear, research indicates that exercise has the potential to affect many biological pathways that influence treatment outcome. Namely, its influence on the inflammatory immune response 18 leads to a reduction in cell differentiation and proliferation related to chemotherapy treatment. 19 Moreover, exercise has a positive effect on metabolic, genetic, and neuroendocrine function, 18 leading to lower levels of circulating sympathetic hormones, which are implicated in fatigue, depression, and pain.20-22
It is thought that the positive impact of exercise on biological and physiological mechanisms during cancer treatment lead to a reduction in health care costs for the patient, payer, and provider alike. The term “financial toxicity” has been used to describe the growing concern of the high cancer-related health care costs. Medical bills are now the leading cause of personal bankruptcy 23 and are implicated in medication nonadherence. 24 Health care companies have responded to this cost burden by decreasing utilization of services and increasing patient responsibility. Patients are now met with higher deductibles and co-pays. As a result, a patient with cancer is now 3 times more likely to file for bankruptcy than those without cancer. 25
There is a growing demand to reduce health care costs and implement care delivery models that are patient-centered, evidence-based, and high quality. Despite other investigations that have supported the efficacy of exercise during cancer treatment, nationally <5% of patients are ever referred to a cancer rehabilitation program. 26 A reported 88% of patients did not even receive education on the importance of exercise during treatment. 27 Public funding and lack of resources has been identified as a significant barrier to national exercise oncology programs.27,28 Other known barriers include lack of general knowledge about the need to stay physically active during and after cancer therapy, qualified personnel, 29 and available programs. 27 Research also emphasizes the need for individualized programs.29-31 Maple Tree Cancer Alliance is a national organization that employs a system of individualized exercise prescription through a unique phase system. We have previously shown a reduction in health care costs through fewer ER visits, 30-day readmits, and shorter length of hospital stay with exercise (EX) patients (n = 672) compared with sedentary (SED) controls (n = 728). 31 In this study, the exercise group had a significantly lower number of ER visits (EX = 2, SED = 14, P < .05), 30-day readmits (EX = 2, SED = 53, P < .05), as well as a shorter length of stay (EX = 0.75, SED = 3, P < .05).
The present study validates these findings by comparing our patients against themselves and showing significant cost savings. This system of exercise oncology has the potential to contribute to a national standard of care for individuals battling cancer.
Study Limitations
Due to the retrospective nature of the investigation, it is unknown if patient self-selection into the program may have influenced results, resulting in better health outcomes. Physician referral bias and small sample size may have also contributed to limitations in this investigation.
Directions for Future Research
Further studies should take into account the cost savings effects of exercise during various stages of cancer. In addition to breast cancer, other types of cancer populations should be studied. Furthermore, a larger sample size would have likely produced significant differences in terms of ER visits and length of hospital stay.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We would like to thank the Gala of Hope Foundation for their generous funding of this study.