
Abstract
This meta-analysis evaluates the clinical evidence for the addition of traditional Chinese medicines (TCMs) to 5-fluorouracil (5-FU)-based regimens for colorectal cancer (CRC) in terms of tumor response rate (TRR). Five electronic databases were searched for randomized controlled trials of 5-FU-based chemotherapy combined with TCMs compared to the same 5-FU-based regimen. Forty-five randomized controlled trials were involved in this study, and all the data were analyzed by Stata software (version 14.0). Our results suggested that the TRR of the group with TCMs combined with 5-FU-based regimens was higher than that in the group with 5-FU regimens alone (risk ratio [RR] 1.36 [1.25-1.49], I2 = 0%). Furthermore, both nonoral administration (RR 1.51 [1.29-1.76], I2 = 0%) and oral administration (RR 1.31 [1.18-1.45], I2 = 0%) of TCMs showed benefits to the CRC treatment. Further sensitivity analysis of specific plant-based TCMs found that fuling, sheshecao, banzhilian, eshu, baizhu, huangqi, yiyiren, and dangshen had significantly higher contributions to the results of the risk ratio. Therefore, TCMs may have the potential to improve the efficacy of 5-FU-based chemotherapy for CRC.
Introduction
Colorectal cancer (CRC) is the third most commonly diagnosed cancer and the third leading cause of cancer mortality worldwide. 1 Despite the advancement in clinical oncology, approximately 25% of patients present with metastases on diagnosis and almost 50% of patients with CRC will develop metastases, 2 contributing to the low survival rates reported for CRC. Chemotherapy is still the main treatment for metastatic and local late-stage CRC; however, side effects and resistance to chemotherapy have shown the limitations of current chemotherapy and led to the search for alternative treatments.
5-Fluorouracil (5-FU) is a pyrimidine analogue that incorporates into the DNA molecule to suppress thymidylate synthase. 3 This subsequently inhibits the synthesis of pyrimidine thymidine required for DNA replication so that actively dividing cancerous cells will undergo apoptosis. 3 So far, 5-FU-based chemotherapy remains the backbone of CRC treatment, and it has been demonstrated that the use of combination regimens of 5-FU with cytotoxic agents, such as 5-FU combination plus either irinotecan (FOLFIRI), oxaliplatin (FOLFOX), or capecitabine (CAPOX or XELOX), have significantly improved the survival of patients with advanced CRC. 4
Traditional Chinese medicines (TCMs), which emphasize overall coordination of the environment inside and outside the human body, have been widely used for complementary treatment of cancer patients including CRC in China. 5 Application of TCMs as an adjuvant cancer therapy has been reported to enhance the efficacy of chemotherapy and to help reduce adverse effects of anticancer drugs. 6 However, whether the TCMs combined with 5-FU-based regimens may be more effective than 5-FU-based chemotherapy alone is still uncertain.
In this article, we compared the combination of 5-FU-based chemotherapy plus TCMs with 5-FU regimens alone in terms of tumor response rate (TRR) for CRC. As a result, our results suggested that the TRR of the group with TCMs combined with 5-FU-based regimens is remarkably higher than that in the group with 5-FU regimens alone. This meta-analysis provides evidence that TCMs could have the potential to improve the efficacy of 5-FU-based chemotherapy for CRC.
Methods
We have searched PubMed, EMBASE, Cochrane CENTRAL, China Academic Journals (CNKI), and Chinese Science and Technology Journals (CQVIP) databases for relevant articles from their inceptions to July 2018. The keywords are the following: (a) Disorder: colorectal cancer and related terms; (b) Intervention: fluorouracil (5-FU), herbal medicine, traditional medicine, and related terms; and (c) Study type: randomized controlled trial and related terms. The test arm and the control arm of the randomized controlled trials that are involved in the meta-analyses were fluorouracil regimens combined with TCM intervention and fluorouracil regimen alone, respectively. According to the administration type of the TCMs, the studies were divided into 2 groups: oral administration group and non-oral (injection products) administration group. All CRC cases in each study were confirmed by histopathological examination. The screening and review were performed by 2 independent reviewers searching the literature and extracting data independently.
According to the Response Evaluation Criteria in Solid Tumors (RECIST) criteria, tumor response criteria included complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). The primary clinical outcome was TRR. CR and PR were included in data pooling as TRR. Relative risk (RR) estimates were calculated using the Stata software application (version 14.0; StataCorp, College Station, TX). Methods were based on Cochrane Handbook 5.1.0. Subgroup analyses based on heterogeneity between trials used the χ2-based Q statistic and were considered statistically significant at a P value less than .05 or I2 ≥ 50%. In the presence of heterogeneity, data were analyzed in a random-effects model; otherwise, a fixed-effects model was used. A statistical test resulting in a P value less than .05 was considered to indicate a statistically significant difference.
Studies with zero events were included to avoid overestimation of effect. When the same outcome was reported by more than 10 studies, publication bias was assessed using a Begg funnel plot.
Results
There were 4018 potential relevant citations that were located according to the search strategy. Following screening, 45 studies were included in the meta-analysis (Figure 1).7-51 All studies met the requirements of 5-FU regimen combined with TCM intervention versus 5-FU regimen alone. The TRR was provided as well. These 45 studies were classified as oral administration group (37 studies) and non-oral administration group (8 studies), which enrolled 2986 participants with 1544 participants in the experimental groups and 1442 participants in the control groups. All the clinical characteristics of the participants are summarized in Table 1, including the sample size, dosage and duration of TCM intervention, and dose and cycles of 5-FU regimen, among others.

Flow diagram of the search and selection process of randomized controlled trials of 5-FU regimens combined with TCM for CRC.
Characteristics of Randomized Controlled Trials of Traditional Chinese Medicines (TCMs) Combined With Fluorouracil-Based Regiments for Colorectal Cancer (CRC).

Abbreviations: T, treatment group; C, control group; M, male; N, number; NS, not stated; ID, intravenous drip; TRR, tumor response rate; TNM, cancer staging system (“T” for tumor, denotes the extent of the intestinal wall; “N” for lymphatic node, the amount of lymphatic node involvement; and “M” for the metastasis); KPS, Karnofsky Performance Status; ECOG, Eastern Cooperative Oncology Group Performance Status; TM, traditional medicine; 5-FU, 5-fluorouracil; LV, leucovorin; Ox, oxaliplatin; HCPT, hydroxycamptothecine; FOLFOX, Ox. + 5-FU + LV; ACRC, advanced colorectal cancer; bid, twice per day; tid, thrice per day; qd, once per day; wk, week; mth, mouth; med, median. Risk of Bias Categories: SG, sequence generation; AC, allocation concealment; BPt, blinding of participants/personnel; BOA (obj), blinding of outcome assessment (objective outcome measure, ie, TRR); IOD, incomplete outcome data; SOR, selective outcome reporting. Risk of Bias Judgements; L, low risk; U, unclear risk; H, high risk.
Methodological Assessment
All studies stated the use of randomization, so risk of bias of sequence generation (SG) was judged as “low.” Allocation concealment (AC) and blinding of participants (BPt) were only described in 2 studies (Kono T, Cao B) and these were judged “low risk,” since a placebo control had been used for the TCM. The other studies did not describe procedures for AC, so were judged “unclear risk” for AC, while BPt was “high risk” since the additional therapy of TCM was difficult to conceal. Blinding of outcome assessors (BOA) for TRR was not mentioned. Blinding of participants is difficult to achieve in cancer trials. Six studies (Qin Y, Xu Y, Wang Z, You J, Xu Y, Dai L) reported that they had participants dropping out or lost to follow-up; thus, these missing data were not treated as “intent to treat.” So these were judged as “high risk” of attrition bias. Studies that had the same numbers of participants at inception as in the outcome reports were judged as “low risk” of incomplete outcome data (IOD; Table 1).
As for the selective outcome reporting (SOR), only when the objectives and outcome measures stated in the method section were all reported in the results section, was the study judged as “low risk.” The 47 studies showed symmetry for TRR in the funnel plot, suggesting the risk of publication bias was low.
Meta-Analysis of Tumor Response
The RECIST criteria were used to evaluate TRR in 47 studies. Meta-analyses were conducted for CR and TRR. When RR ≥1 (IV model, fixed, 95% confidence interval), it favors the test group. Three groups were divided for meta-analyses: total (47 studies); non-oral group (8 studies) and oral administration group (39 studies).
Total Group
In the 47 studies (n = 3066, Table 1), the test groups showed significantly improved TRR (RR 1.38 [1.26-1.50], I2 = 0%; Figure 2).

Forest plot of meta-analysis of tumor response rate of TCM plus 5-FU-based regimens versus 5-FU-based regimens alone.
Non-Oral Group
Five different injection products (Kushen or Fufangkushen, Huachansu, Shenqifuzheng, Delisheng, Banmaosuanna vitamin B6) were tested in 8 studies (n = 795; Table 1). There were significant improvements for TRR (RR 1.51 [1.29-1.76], I2 = 0%). The TRR funnel plot was symmetric.
Oral Administration Group
In 39 studies (n = 2307), TCMs were administered orally as decoctions, capsules, or tablets. The pooled TRR showed significant improvement (RR 1.33 [1.19-1.47], I2 = 0%).
The Effects of Multi-Ingredient TCM in the Oral Administration Group
As is well known, the TCM formulae usually have different names; however, their main components are considered to have similarity. In order to identify the most comparable subgroups of studies and potential synergistic effects, we made a series of planned sensitivity analyses. Only the TCMs with significant RR results for tumor response have been reported in our analyses.
Level 1: Single TCMs
Ninety-two ingredients in the formulae have been included in this review. Among them, there are 35 ingredients that have been used in 3 or more formulae. The Chinese name in pin yin of each ingredient was used to stand for the TCMs.
According to their frequency of use in formulae, TCMs were listed as follows: Huangqi (n = 28), baizhu (n = 27), yiyiren (n = 27), fuling (n = 26), dangshen (n = 22), sheshecao (n = 20), baijiangcao (n = 12), eshu (n = 11), and banzhilian (n = 10).
Then, the RR values were calculated, which were listed in descending order in Table 2. The pooled RR values were divided into 2 groups. The RR values of the first group were equal to or greater than the RR results of the total pool. In the second group, the RR values were less than the RR results of the total pool.
Effects of Specific Orally Administered Traditional Chinese Medicines (TCMs) on Tumor Response.
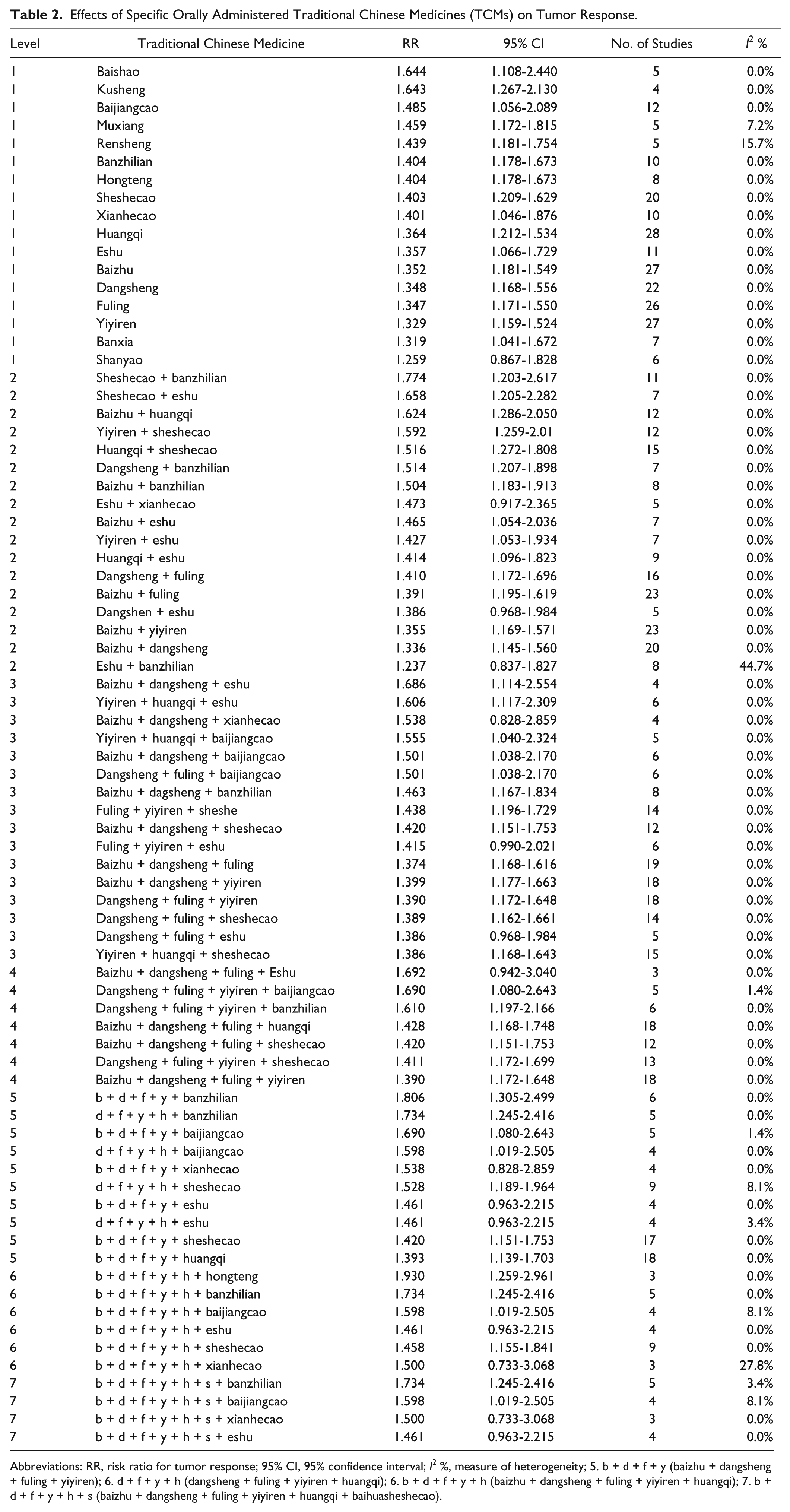
Abbreviations: RR, risk ratio for tumor response; 95% CI, 95% confidence interval; I2 %, measure of heterogeneity; 5. b + d + f + y (baizhu + dangsheng + fuling + yiyiren); 6. d + f + y + h (dangsheng + fuling + yiyiren + huangqi); 6. b + d + f + y + h (baizhu + dangsheng + fuling + yiyiren + huangqi); 7. b + d + f + y + h + s (baizhu + dangsheng + fuling + yiyiren + huangqi + baihuasheshecao).
The first group included 16 TCMs: baishao (n = 5), kusheng (n = 4), baijiangcao (n = 12), muxiang (n = 5), rensheng (n = 5), banzhilian (n = 10), hongteng (n = 8), sheshecao (n = 20), xianhecao (n = 10), huangqi (n = 28), eshu (n = 11), baizhu (n = 27), dangshen (n = 22), fuling (n = 26), yiyiren (n = 27), and banxia (n = 7). In the second group there was only one TCM, shanyao, which had a lower value than the RR of the total pool (Table 2).
Level 2: Combinations of 2 TCMs
In this level, there are 17 pairs of TCMs from group 1 or 2 above. Among them, the RR values of 16 pairs were shown to be equal to or greater than the total pool, including sheshecao + banzhilian (n = 11), sheshecao + eshu (n = 7), baizhu + huangqi (n = 12), yiyiren + sheshecao (n = 12), huangqi + sheshecao (n = 15), dangshen + banzhilian (n = 7), baizhu + banzhilian (n = 8), eshu + xianhecao (n = 5), baizhu + eshu (n = 7), yiyiren + eshu (n = 7), huangqi + eshu (n = 9), dangshen + fuling (n = 16), baizhu + fuling (n = 23), dangshen + eshu (n = 5), baizhu + yiyiren (n = 23), and baizhu + dangshen (n = 20). Only one pair was lower than the RR of the total pool (Table 2).
Level 3: Combinations of 3 TCMs
In this level, there are 16 significant pairs from level 2 that were combined with other TCMs that showed significant RRs at level 1. The RR values of all pairs in this level were greater than the total pool, as follows: baizhu + dangshen + eshu (n = 4), yiyiren +huangqi +eshu (n = 6), baizhu +dangshen + xianhecao (n = 4), yiyiren + huangqi + baijiangcao (n = 5), baizhu + dangshen + baijiangcao (n = 6), dangshen + fuling + baijiangcao (n = 6), baizhu + dangshen + banzhilian (n = 8), fuling + yiyiren +sheshe (n = 14), baizhu + dangshen + sheshecao (n = 12), fuling + yiyiren + eshu (n = 6), baizhu +dangshen + fuling (n = 19), baizhu + dangshen + yiyiren (n = 18), dangshen + fuling + yiyiren (n = 18), dangshen + fuling + sheshecao (n = 14), dangshen + fuling + eshu (n = 5), and yiyiren + huangqi + sheshecao (n = 15; Table 2).
Levels 4 to 7: Combinations of 4 to 7 TCMs
The significant combinations from levels 4 to 7 were further combined. As a result, the RR values of levels 4 to 7 were significantly higher than the total pool (Table 2).
TCMs Potential Synergistic Effects Selection
Compared with TCMs alone, 15 TCM pairs showed higher RR values and potential synergistic effects, including sheshecao + banzhilian (n = 11), sheshecao + eshu (n = 7), baizhu + huangqi (n = 12), yiyiren + sheshecao (n = 12), huangqi + sheshecao (n = 15), dangshen + banzhilian (n = 7), baizhu + banzhilian (n = 8), eshu + xianhecao (n = 5), baizhu + eshu (n = 7), yiyiren + eshu (n = 7), huangqi + eshu (n = 9), dangshen + fuling (n = 16), baizhu + fuling (n = 23), dangshen + eshu (n = 5), and baizhu + yiyiren (n = 23).
When comparing the RR values of the combinations in levels 3 to 7 with each singe TCM in level 1, however, we found that the RR value of 2 combinations in level 3 is lower than the single TCMs, as follows: dangshen +fuling + sheshecao (n = 14) and yiyiren + huangqi + sheshecao (n = 15).
Discussion
TCM, as a complementary and alternative medicine, has been recorded in the Chinese medical literature for thousands of years and gradually became a commonly used treatment for cancer in China. 52 Application of TCM as an adjuvant cancer therapy has been recognized as an important approach to enhance the efficacy of anticancer strategies or to reduce adverse effects of these treatments.53-55 5-FU is widely used in the treatment of a variety of cancer types, and 5-FU in combination with other chemotherapeutic agents has been demonstrated to improve the overall and disease-free survival of patients with resected stage III CRC.56-58 The study from Chen et al evaluated the clinical evidence for the addition of TCMs to oxaliplatin-based regimens for CRC in terms of tumor response rate and their results showed specific combinations of TCMs appeared to produce higher contributions to TRR than the TCMs individually. 59 However, the relationship between the combination of 5-FU-based chemotherapy plus TCMs with 5-FU regimens alone in the treatment for CRC is still unclear.
To evaluate the clinical evidence for the addition of TCMs to 5-FU-based regimens for CRC in terms of TRR, our study reviewed 45 studies that were classified as oral administration group (37 studies) and non-oral administration group (8 studies) and enrolled 2986 participants with 1544 participants in the experiment groups and 1442 participants in the control groups. As a result, we demonstrated that the TRR of the group with oral TCMs or injection products (Kushen or Fufangkushen, Huachansu, Shenqifuzheng, Delisheng, Banmaosuanna vitamin B6) combined with 5-FU-based regimens was remarkably higher than that in the group with 5-FU regimens alone. Furthermore, both oral administration and injection of TCMs showed benefits to the CRC treatment. Further sensitivity analysis of specific plant-based TCMs found that fuling, sheshecao, banzhilian, eshu, baizhu, huangqi, yiyiren and dangshen produced significantly higher contributions to the results of RR value.
In conclusion, our study suggests that specific combinations of TCMs with 5-FU-based chemotherapy appear to produce higher contributions to TRR than 5-FU regimens alone. Notable among these is the combinations of fuling, sheshecao, banzhilian, eshu, baizhu, huangqi, yiyiren, and dangshen. Therefore, TCMs may have the potential to improve the efficacy of 5-FU-based chemotherapy for CRC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from National Natural Science Foundation of China (Grant Nos. 81874380, 81672932, and 81730108), Zhejiang Provincial Natural Science Foundation of China for Distinguished Young Scholars (Grant No. LR18H160001), Zhejiang Province Medical Science and Technology Project (Grant No. 2017RC007), Key Project of Zhejiang Province Ministry of Science and Technology (Grant No. 2015C03055), Talent Project of Zhejiang Association for Science and Technology (Grant No. 2017YCGC002), Zhejiang Province Science and Technology Project of TCM (Grant No. 2019ZZ016), Key Project of Hangzhou Ministry of Science and Technology (Grant Nos. 20162013A07 and 20142013A63), and Zhejiang Provincial Project for the Key Discipline of Traditional Chinese Medicine (Grant No. 2017-XK-A09).