
Abstract
Keywords
Introduction
Colorectal cancer (CRC) is one of common malignancies of the digestive system. 1 It is reported that CRC is the third leading cause of cancer mortality in China, which is associated with the improvements or changes in lifestyle, nutrition, and environment during several decades.2,3 In China, the morbidity and mortality of CRC were 23.03/100 000 and 11.11/100 000, respectively, in 2011. NCCN (National Comprehensive Cancer Network) guidelines recommend FOLFOX regimen, which consists of oxaliplatin (L-OHP), 5-fluorouracil (5-FU), and leucovorin (LV), as the standard first-line chemotherapeutic drugs for CRC; however, it still has some short- and long-term side effects or adverse reactions (ADRs) according to many clinical reports. 4 Recently, evidence in the literature indicates that traditional Chinese medicine (TCM) might be a considerably promising complementary and alternative therapy for patients with CRC.5,6 In the theory of TCM, CRC belongs to the category of “abdominal mass,” and its basic pathogenesis is closely correlated to the deficiency in origin and excess in superficiality. 7 Furthermore, the recent trials validated that TCM could produce encouraging results in CRC with notable objective responses, considerable curative effects, meaningful survival advantage, and so on.8,9 Chinese herbal injection (CHIs) are a new form of TCM preparation, which are prepared by extracting and purifying the effective and active compounds from herbs (or decoction pieces) via modern scientific techniques and methods.10,11 The anticancer CHIs are mainly used for adjuvant radiotherapy and chemotherapy against tumors by reducing toxicity, enhancing efficiency, ameliorating symptoms, and improving the performance status in clinical use.12-14 Recently, there is also increasing interest in CHIs combined with conventional anticancer therapies, and multiple studies have recognized that the combination of CHIs and chemotherapy or radiotherapy can provide supportive care for cancer patients effectively owing to its unique advantages of reducing ADRs and improving survival time.15,16
Compared with the double-arm meta-analysis, network meta-analysis (NMA) can synthesize multiple correlation factors, and direct or indirect comparisons simultaneously by summarizing different interventions for the same disease.17,18 Moreover, NMA can provide evidence for identifying optimal therapies based on the rankings of different outcomes. 19 Given the widespread and long-term use of CHIs combined with chemotherapy in China, it is warranted to explore the comparative effectiveness and safety between different CHIs plus FOLFOX against CRC. To address this issue, this NMA is conducted to provide references points regarding the clinical incorporation of CHIs as adjuvant chemotherapy for CRC.
Materials and Methods
The procedure of the current NMA includes sections on literature search, inclusion criteria, data extraction, quality assessment, and statistical analysis, in accordance with Cochrane criteria and PRISMA Checklist (Supplementary Table 1, available online).
Selection Criteria
All strictly randomized trials comparing CHIs plus FOLFOX to FOLFOX alone for treating CRC were considered as eligible for this NMA. The selection criteria of the NMA were determined through discussion and investigation by 5 researchers (DZ, JW, SL, XD, KW). Three investigators (DZ, JW, SL) independently perused the titles and abstracts of the identified RCTs, excluding irrelevant clinical trials. Only RCTs meeting the following conditions were enrolled in the present NMA:
Study design: RCTs that concerned CHIs combined with the FOLFOX regimen for patients with CRC, irrespective of the publication language. Additionally, other study types were excluded, such as reviews, duplicate publications, pharmacological experiments, case reports, editorials, and letters.
Patient: The included participants were diagnosed with CRC, and without limitations on gender, race, or nationality.
Intervention/comparison: The CHIs group was treated by CHIs plus the FOLFOX regimen; and patients with CRC in the FOLFOX group solely received the FOLFOX regimen.
Outcome: The primary outcomes of the NMA were the clinical effectiveness rate and the performance status, and the secondary outcomes were ADRs (such as leukopenia, nausea, and vomiting). The clinical effectiveness rate was defined as complete response or partial response. 20
The improvement of performance status was considered to be an increase in the Karnofsky performance score (KPS) of more than 10 points after completed treatment. More details about the product information of CHIs are listed in Supplementary Table 2, available online.
Search Strategy
RCTs concerning the different CHIs were retrieved through the following databases up to July 2016: PubMed, Embase, the Cochrane Library, the China National Knowledge Infrastructure Database (CNKI), the Wan-Fang Database, the Chinese Scientific Journals Full-text Database (VIP), and the Chinese Biomedical Literature Database (SinoMed). There was no limitation on publication year, language, and blinding methods. The search terms were divided into 3 categories: CRC, CHIs, and RCTs. The search strategy used a combination of subject words and free-text words. In the Chinese databases, search terms about CRC were “Colorectal neoplasms, Colorectal cancer, Colonic neoplasms, Colon cancer, Rectal neoplasms, Rectal cancer, Rectal tumor, Anus neoplasms, Anus cancer,” with a full-text search for “random”; in English databases, the search words in the CRC category were “Colorectal Neoplasm, Colorectal Tumor*, Colorectal Carcinoma*, Colorectal Cancer*, Colonic Neoplasm*, Rectal Neoplasm*, Sigmoid Neoplasm*, and Anus Neoplasm*”. The specific Chinese and English search terms for each CHI and specific retrieval strategies are shown in Supplemental Material, available online. The reference lists of the searched articles were also reviewed to identify the potential enrolled RCTs.
Data Extraction and Quality Assessment
The corresponding data of included RCTs were extracted using Microsoft Excel (Microsoft Corp, Redmond, WA):
Publication data: title, authors’ names, publication date, and literature sources
Patients’ characteristics: the number, age, sex, KPS before treatment, tumor types, and tumor stages
Intervention: the drug, dose, and duration
Outcomes: reported data of clinical effectiveness rate and performance status
According to the Cochrane risk of bias tool (Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0),21,22 two investigators (DZ, SL) independently examined the quality of all included trials. Discrepancies were resolved either by consensus or through adjudication by a third investigator (JW). The quality evaluation items of each trial included selection bias (random sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assessment), attrition bias (incomplete outcome data), reporting bias (selective reporting), and other bias. These items were scored as low, high, or unclear risk of bias.
Statistical Analysis
The clinical effectiveness rate and the improvement of performance status were displayed as odds ratio (OR) with 95% confidence intervals (CIs). In view of the heterogeneity between trials, the Bayesian hierarchical random-effects model was first fitted for multiple comparisons of different treatment options for CRC.23,24 On the one hand, all calculations and graphs were conducted by Stata 12.0 software (Stata Corporation, College Station, TX). The relationship of the different treatments was presented as a network graph; meanwhile, a comparison-adjusted funnel plot was utilized to test for the potential publication bias.25,26 Moreover, we adopted surface under the cumulative ranking probabilities (SUCRA) values to rank the examined treatments, and the SUCRA values ranged from 0 to 1. A higher SUCRA value corresponds to a higher ranking for CRC compared with other treatments.27,28 On the other hand, based on the theory of likelihood function and some prior assumptions, Markov chain Monte Carlo (MCMC) simulation was calculated by the Bayesian inference with WinBUGS 1.4.3 software (MRC Biostatistics Unit, Cambridge, United Kingdom) to investigate the posterior distributions of the interrogated nodes.29-31 Because there was no head-to-head trial in the NMA, the consistency assumption was not established. 32 Furthermore, cluster analysis was conducted for choosing the optimal CHIs considering both clinical effectiveness rate and improvement in performance status treatments simultaneously.
Results
Literature and Assessment of Quality
A total of 820 articles were retrieved via the searching strategy of the literature databases (see Materials and Methods). After screening the titles and abstracts to remove the irrelevant articles and reading the full texts to remove articles that did not meet the inclusion criteria, ultimately, a total of 60 RCTs that evaluated CHIs combined with the FOLFOX regimen for treating CRC were identified. In addition, this NMA incorporated 14 types of CHIs, namely, Compound matrine, Aidi, Shenqifuzheng, Kangai, Javanica oil emulsion, Shenmai, Kanglaite, Lentinan, Huachansu, Xiaoaiping, Delisheng, Astragalus injections, Shenfu, and Astragalus polysaccharides injections. All trials were published in Chinese, and the flow diagram is presented in Figure 1.

Flow chart of the search for eligible studies.
Overall, 4849 patients with CRC from 60 RCTs were involved in the present NMA; among them, 2466 patients were allocated to CHIs-FOLFOX, and 2383 patients received FOLFOX alone.33-92 All of the included RCTs reported the information of patient population sizes and ages, while 57, 23, and 29 trials described the patients’ ages, tumor staging of CRC, and KPS before treatment, respectively. There was no major difference in patient characteristics between different treatment arms. The basic characteristics of the individual trials are listed in Table 1, and Figure 2 shows the network graph of different interventions for the outcomes.
The Basic Characteristics of the Included RCTs.
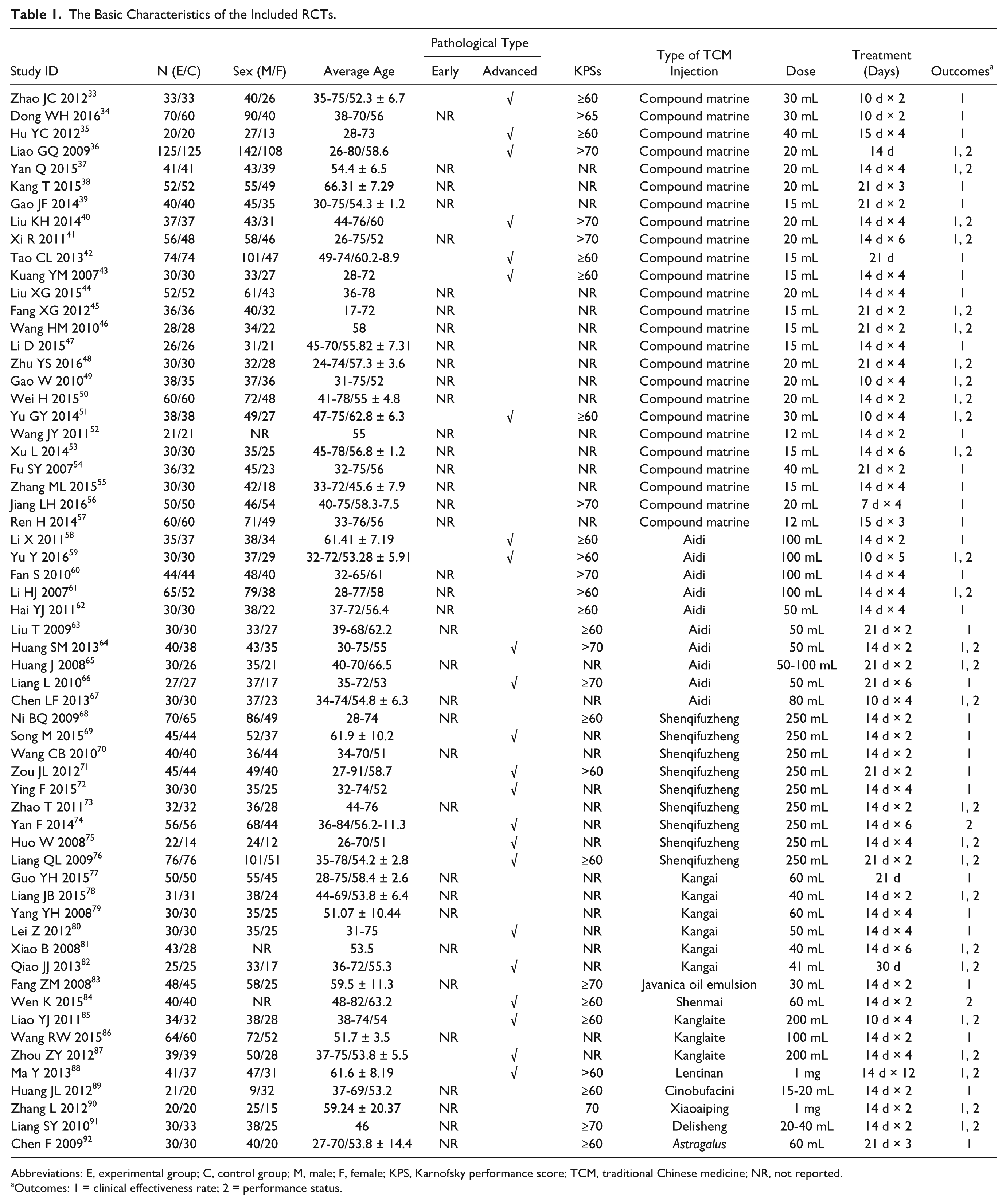
Abbreviations: E, experimental group; C, control group; M, male; F, female; KPS, Karnofsky performance score; TCM, traditional Chinese medicine; NR, not reported.
Outcomes: 1 = clinical effectiveness rate; 2 = performance status.

Network graphs of outcomes: (A) the clinical effectiveness rate; (B) performance status; (C) leukopenia; (D) nausea and vomiting.
We critically appraised the methodological quality of the included RCTs in accordance with the Cochrane risk of bias tool. In random sequence generation, although all trials mentioned randomization, a total of 14 RCTs provided the details of randomized grouping method; therefore, these trials were rated as low risk, namely, 12 RCTs used a random number table; 1 RCT applied an envelope method for randomization, and 1 RCT used stratified random sampling to generate random sequences. Only 1 RCT referred to the method of blinding, evaluated as low risk in performance bias and detection bias. Regarding allocation concealment, 1 RCT used sealed opaque envelopes. Follow-up information for 6 RCTs was available, and 3 RCTs described losses to follow-up. In terms of selective reporting, none of included RCTs explicitly showed reporting bias. Other bias sources were not identified. In general, the methodological quality of included RCTs was not high. A summary of the risk of bias for each included RCT is shown in Figure 3.

Risk of bias graph.
Outcomes
The Clinical Effectiveness Rate
The data on the clinical effectiveness rate were available for 50 RCTs involving 11 types of CHIs. According to the results of NMA illustrated in Table 2, the results showed that there was a benefit of Delisheng + FOLFOX, Kanglaite + FOLFOX, Shenqifuzheng + FOLFOX, and Aidi + FOLFOX over FOLFOX regimen alone in terms of the clinical effectiveness rate. These results were statistically significant; ORs and 95% CIs were 4.23 (1.20, 11.73), 1.99 (1.10, 3.31), 1.82 (1.13, 2.78), and 1.55 (1.01, 2.30), respectively. No statistically significant differences were observed among CHIs groups for clinical effectiveness rate.
Results (OR, 95% CI) of Network Meta-Analysis for the Clinical Effective Rate (Upper Right Quarter) and the Improvement of Performance Status (Lower Left Quarter).

Abbreviations: OR, odds ratio; CI, confidence interval; AD, Aidi injection; AI, Astragalus injection; AP, Astragalus polysaccharides injection; CM, Compound matrine injection; DLS, Delisheng injection; FOLFOX, FOLFOX regimen; JI, Javanica oil emulsion injection; HCS, Huachansu injection; KA, Kangai injection; KLT, Kanglaite injection; LI, Lentinan injection; SF, Shenfu injection; SM, Shenmai injection; SQFZ, Shenqifuzheng injection; XAP, Xiaoaiping injection.
Performance Status
In total, 37 RCTs with 9 CHIs contributed to the analysis of performance status. Indirect comparisons demonstrated that receiving Delisheng + FOLFOX, Xiaoaiping + FOLFOX, Lentinan + FOLFOX, Kangai + FOLFOX, Shenqifuzheng + FOLFOX, and Aidi + FOLFOX were associated with a substantial improvement in performance status versus receiving the FOLFOX regimen alone; these between-group differences were statistically significant, with ORs and 95% CIs of 6.14 (1.12, 20.08), 3.47 (1.10, 8.55), 2.72 (1.12, 5.69), 3.13 (1.37, 6.27), 2.58 (1.77, 3.62), and 3.80 (2.48, 5.64), respectively (Table 2). Nevertheless, the differences across different CHIs were not statistically significant.
ADRs
The specific NMA results of ADRs are presented in Table 3. A total of 45 RCTs provided sufficient information for estimating leukopenia: Compound matrine + FOLFOX, Aidi + FOLFOX, Shenqifuzheng + FOLFOX, Kangai + FOLFOX were associated with a substantially relieving leukopenia than receiving the FOLFOX regimen alone; these between-group differences were statistically significant, with ORs and 95% CIs of 3.35 (2.37, 4.76), 0.29 (0.19, 0.43), 0.45 (0.28, 0.74), 0.30 (0.18, 0.51), respectively. Among CHIs groups, Compound matrine + FOLFOX (OR = 3.98, 95% CI = 1.26-12.4), Aidi + FOLFOX (OR = 4.09, 95% CI = 1.28-13.04), Kangai + FOLFOX (OR = 3.95, 95% CI = 1.18-13.24) might relate to better effects in relieving leukopenia than Javanica oil emulsion + FOLFOX group. Similarly, Compound matrine + FOLFOX (OR = 4.42, 95% CI = 2.1-9.061), Aidi + FOLFOX (OR = 4.55, 95% CI = 2.11-9.70), Shenqifuzheng + FOLFOX (OR = 2.92, 95% CI = 1.28-6.44), Kangai + FOLFOX (OR = 4.39, 95% CI = 1.89-10.02) might relate to the better effects of relieving leucopenia than Kanglaite + FOLFOX group.
Results (OR, 95% CI) of Network Meta-Analysis for Leucopenia (Upper Right Quarter) and Nausea and Vomiting (Lower Left Quarter).

Abbreviations: OR, odds ratio; CI, confidence interval; AD, Aidi injection; AI, Astragalus injection; AP, Astragalus polysaccharides injection; CM, Compound matrine injection; DLS, Delisheng injection; FOLFOX, FOLFOX regimen; JI, Javanica oil emulsion injection; HCS, Huachansu injection; KA, Kangai injection; KLT, Kanglaite injection; LI, Lentinan injection; SF, Shenfu injection; SM, Shenmai injection; SQFZ, Shenqifuzheng injection; XAP, Xiaoaiping injection.
A total of 45 RCTs presented data about nausea and vomiting: Compound matrine + FOLFOX, Aidi + FOLFOX, Kangai + FOLFOX were associated with a substantially relieving nausea and vomiting over the FOLFOX regimen; these between-group differences were statistically significant, with ORs and 95% CIs of 2.74 (1.53, 4.95), 0.40 (0.22, 0.72), 0.40 (0.22, 0.72), respectively.
SUCRA Values of CHIs Groups for Outcomes
As illustrated in Figure 4, according to the calculated probabilities, Delisheng (83.49%), Xiaoaiping (81.94%), and Compound matrine (69.25%) yielded higher probabilities of improving clinical effectiveness rate among CHIs groups (Figure 4A), and Aidi (76.57%), Xiaoaiping (75.6%), and Lentinan (58.03%) seemed to be the optimal choices for improving performance status (Figure 4B). With regard to ADRs, Huachansu (85.3%), Aidi (77.29%), and Compound matrine (75.75%) possessed higher probability of relieving leukopenia (Figure 4C), and Shenfu (71%), Kangai (69.37%), and Shenmai (63.57%) possessed higher probability of nausea and vomiting across different CHIs groups (Figure 4D). The SUCRA values of each CHIs group for outcomes are listed in Table 4.

Rank of the cumulative probabilities for outcomes: (A) the clinical effectiveness rate; (B) performance status; (C) leukopenia; (D) nausea and vomiting.
SUCRA Values of Different Groups for Outcomes.
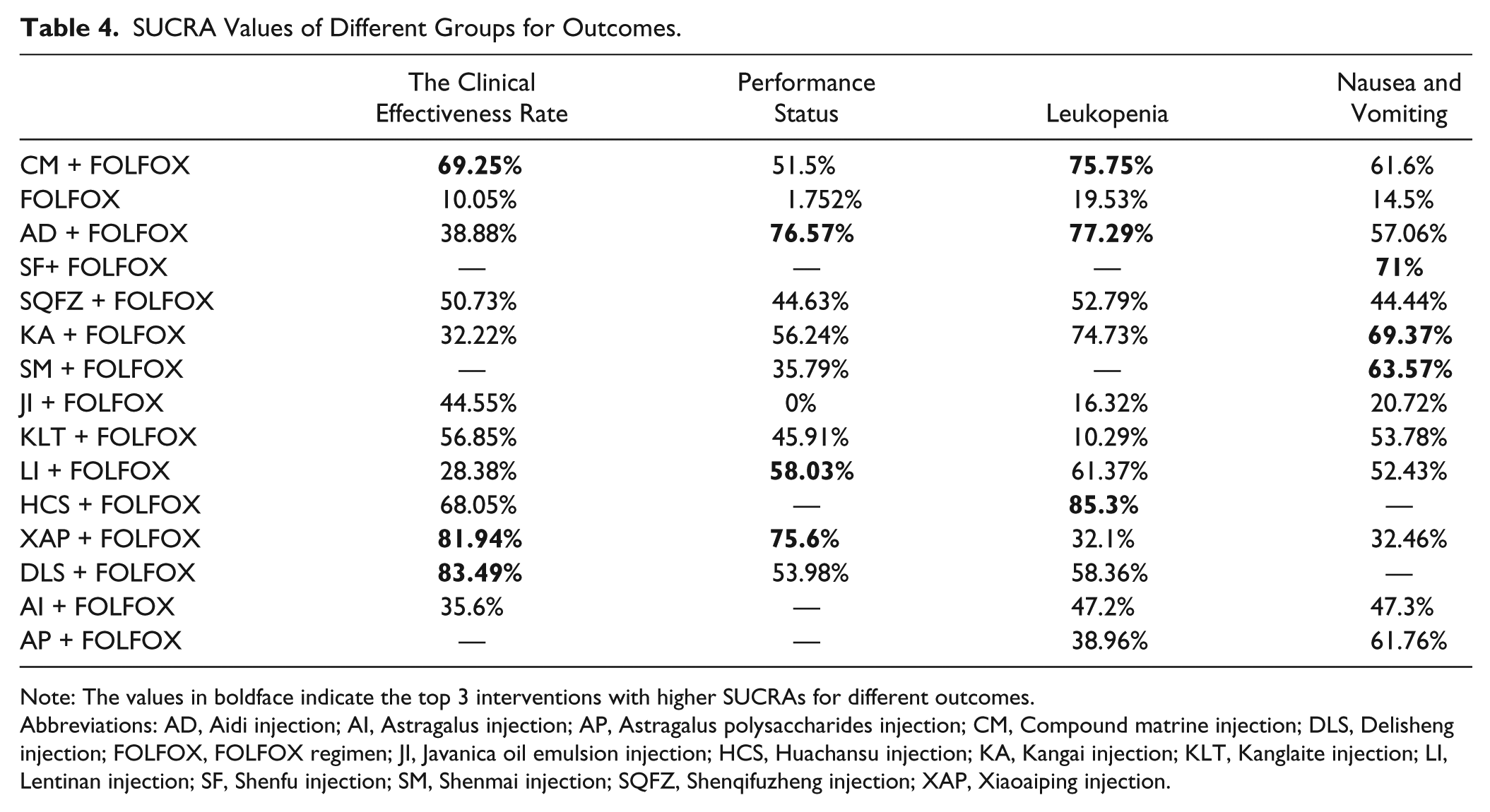
Note: The values in boldface indicate the top 3 interventions with higher SUCRAs for different outcomes.
Abbreviations: AD, Aidi injection; AI, Astragalus injection; AP, Astragalus polysaccharides injection; CM, Compound matrine injection; DLS, Delisheng injection; FOLFOX, FOLFOX regimen; JI, Javanica oil emulsion injection; HCS, Huachansu injection; KA, Kangai injection; KLT, Kanglaite injection; LI, Lentinan injection; SF, Shenfu injection; SM, Shenmai injection; SQFZ, Shenqifuzheng injection; XAP, Xiaoaiping injection.
Cluster Analysis
First, a cluster analysis was performed for 8 types of CHIs that reported the clinical effectiveness rate and performance status simultaneously. The plot is based on SUCRA values of CHI groups; each color represents a group of treatment groups that belong to the same cluster, and treatment groups that are located in the upper right corner were superior to other CHIs for both the clinical effectiveness rate and performance status. The results of the cluster analysis demonstrated that Xiaoaiping, Delisheng, and Compound matrine had better therapeutic effects. Aidi, Lentinan, and Kangai were associated with a significant improvement in performance status. In contrast, the FOLFOX regimen alone had the worst comprehensive rank of the examined regimens (Figure 5E). Second, a cluster analysis was conducted for 11 types of CHIs in terms of ADRs (Figure 5F). Kangai, Compound matrine, and Aidi injection might be the tolerable options for relieving ADRs. Taken together, the analysis results indicated that Compound matrine injection was the most beneficial option for treatment of CRC in combination with the FOLFOX regimen to balance efficacy and safety.

Cluster analysis plots: (E) the clinical effectiveness rate (x-axis) and performance status (y-axis); (F) leukopenia (x-axis) and nausea and vomiting (y-axis).
Publication Bias and Sensitivity Analysis
Publication bias and small-sample effects of included RCTs were measured by funnel plots (Figure 6), Begg’s test, and Egger’s test. For the clinical effectiveness rate, since the results of Begg’s (z = 0.67, P = .520 > .05) and Egger’s tests (t = 3.51, P = .001 < .05) were inconsistent, we first cut the included RCTs in unsymmetrical parts after the initial funnel plot. Using the symmetric remaining part to estimate center value of the funnel plot, and then along the center sides made up the sheared and missing part. Ultimately, based on the funnel plot after patched estimate of the actual value of the combined effect, the number of RCTs increased, suggesting that there was an absence of RCTs without qualitative change in the result. Thus, the included RCTs in the present NMA had a certain publication bias.

Funnel plots of outcomes: (A) the clinical effectiveness rate; (B) performance status; (C) leukopenia; (D) nausea and vomiting.
Moreover, sensitivity analysis was conducted by excluding each trial individually from the present study; the corresponding results of current study were relatively robust.
Subgroup Analysis
For the outcome of the clinical effectiveness rate, subgroup analysis was stratified by the pathological type and KPSs to detect potential sources of heterogeneity (Table 5). Regarding patients with different pathological types, those with NR (OR = 1.33, 95% CI = 1.24-1.43, P < 0.001, I2 = 38.4) and advanced (OR = 1.35, 95% CI = 1.22-1.51, P < 0.001, I2 = 20.5) had similar trends after receiving CHIs combined TACE. Additionally, among patients with different KPS, there also were no significant differences across the different KPS subgroups.
The Results of Subgroup Analysis for the Clinical Effectiveness Rate.
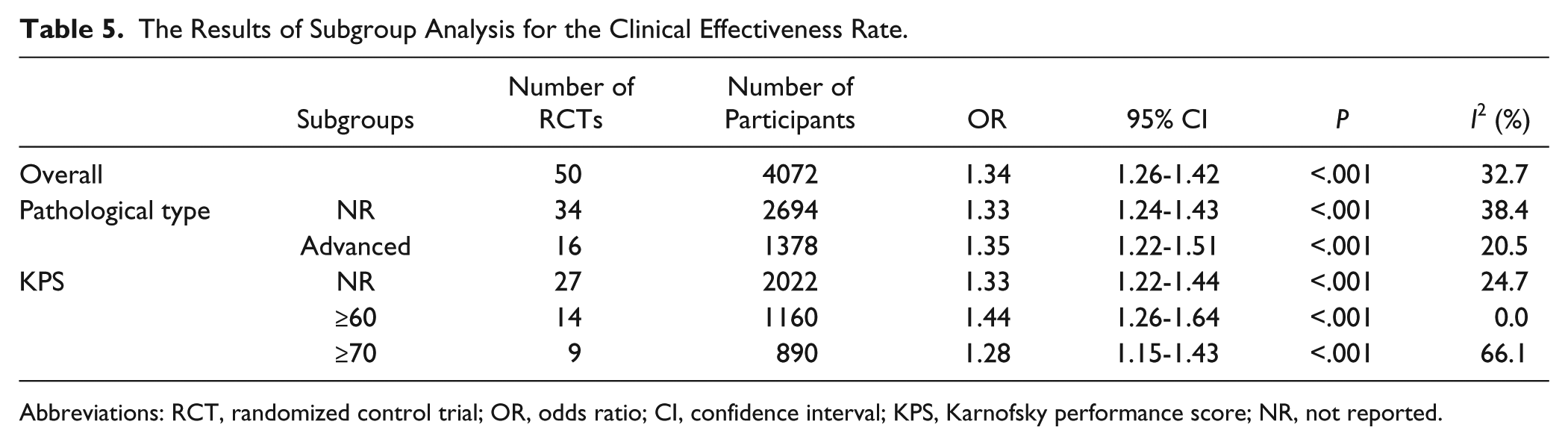
Abbreviations: RCT, randomized control trial; OR, odds ratio; CI, confidence interval; KPS, Karnofsky performance score; NR, not reported.
Discussion
For the comparative efficacy and safety of different CHIs combined with CRC against CRC, we adopted the approach of NMA for analyzing the overwhelming evidence in published RCTs. In summary, the results of the present NMA indicated that the FOLFOX regimen combined with Delisheng, Kanglaite, Shenqifuzheng, or Aidi injections could improve clinical effects compared with the FOLFOX regimen alone and that the FOLFOX regimen combined with Delisheng, Xiaoaiping, Lentinan, Kangai, Shenqifuzheng, or Aidi injections could improve performance status. In terms of ADRs, Compound matrine, Aidi, Shenqifuzheng, and Kangai injection could relieve leukopenia better than receiving the FOLFOX regimen alone. And Compound matrine, Aidi, and Kangai injection could relieve nausea and vomiting over the FOLFOX regimen. Statistically significant differences were observed between these groups. Furthermore, according to the results of cluster analysis, Compound matrine injection combined with the FOLFOX regimen against CRC might be the most favorable option in consideration of both effectiveness and safety.
It has been over 3 decades since Compound matrine injection was approved for treating cancer by the State Food and Drug Administration of China. Compound matrine injection contains anticancer components from Rhizoma Heterosmilacis Japonicae and Sophora flavescens, and it possesses the functions of blood-cooling and toxin-relieving, heat-clearing and damp-inhibiting, stagnation-eliminating, and pain-relieving in TCM theory, which might be correlative to the therapeutic principle and method of tumors in TCM theory.5,93 On the one hand, the relevant pharmacological research has indicated that its primary components, matrine and oxymatrine, can effectively reduce tumor growth of tumor. 94 For example, matrine may achieve the therapeutic benefits on CRC via inhibition of HMGB1 signaling through downregulation of IL-6, TNF-α, and HMGB1. 95 Additionally, oxymatrine could stimulate lncRNA MALAT1 to enhanced migration and invasion of cells for CRC patients. 96 And oxymatrine is associated with inhibition of TGF-β1/Smad signaling pathway activation and reducing P38-dependent increased expression of PAI-1 to alleviate CRC. 97 On the other hand, it is reported that a Sophora flavescens–containing formula could elicit anti-inflammatory and anti-oxidative stress response in vitro in a cell line and in vivo in colitis mouse model that may contribute to the overall anticolon cancer effects. 98 And it has been reported in a meta-analysis that Compound matrine injection could relieve cancer-related pain. 99 Also, our results confirm the efficacy and safety of Compound matrine injection combined with the FOLFOX regimen against CRC compared with other types of CHIs by network meta-analysis. Nevertheless, there is lack of research to validate the anticancer mechanism for Compound matrine injection against CRC. Overall, it is warranted to elucidate and confirm the efficacy of Compound matrine injection against CRC using pharmacological, bioinformatics, and genomic approaches, and clinical trials in the future.
Currently, TCM has been applied in multifaceted approaches and plays an indispensable role in the prevention and treatment of cancer owing to its unique treatment concepts, theory, methods, and basic and clinical research.5,100 Compared to TCM decoctions, CHIs has the advantages of higher bioavailability and faster absorption. 101 The antitumor effectiveness of CHIs, such as Javanica oil emulsion, Huachansu, and Delisheng, mainly involved shrinking the tumor along with amelioration of symptoms, thereby improving the performance status.102-105 The Delisheng injection, which is mainly composed of Venenum Bufonis, Cantharis, Ginseng, and Astragalus, has been applied in the treatment of tumors for more than 10 years. Its composition not only reflects the TCM therapeutic principle of strengthening the body’s resistance and eliminating evil but also integrates the principles of curing the disease, protecting the body, and improving immunity.106,107 Correlative studies have reported that the anticancer functions of Aidi injection covering heat-clearing and detoxifying effects. It can be employed in multitargeted therapy to promote the apoptosis of tumor cells and strengthen the body’s resistance to eliminate pathogenic factors.108-110 Moreover, validated modern pharmacological research findings have shown that the Kangai injection can improve immune function and inhibit tumor growth and angiogenesis due to its active components, namely, Astragalus saponins, ginsenoside, and matrine.111,112 The Kanglaite injection might influence the secretion of inflammatory cytokines to prevent the occurrence and development of cancer cachexia and induce the apoptosis of cancer cells, reducing the multidrug resistance of tumor cells caused by chemotherapeutics.113-115 In addition, the main ingredients of Compound matrine injection were matrine and oxymatrine, and they could exhibit a variety of pharmacological activities, including anti-allergic, anti-viral, anti-fibrotic, and anti-inflammatory effects.116-118 Clinical observation has confirmed that the Xiaoaiping injection reduces toxicity and enhances treatment efficacy and can be combined with cytotoxic chemotherapeutic drugs.119-121
The common intervention evaluated in our study was the FOLFOX regimen; this restriction is to avoid potential interference caused by the different chemotherapeutic drugs in clinics. In addition, although a relevant network meta-analysis has been published, our study had several strengths. 122 This study comprehensively retrieved the 21 types of CHIs widely used in clinical treatment and formulated strict inclusion criteria. Furthermore, our study not only analyzed the clinical effect and improvement of performance status for the included 12 types of CHIs but also conducted a cluster analysis of the SUCRA values to identify which TCM injection was most effective in combination with the FOLFOX regimen for the treatment of CRC.
Nevertheless, the present NMA also had several limitations. The included RCTs were performed in patients of Asian descent and there were only several included trials describing the information of CRC patients with metastatic disease; therefore, it is unclear whether the conclusions of our study was applied to other populations or patients with metastatic disease. The reliability of our study was limited by the sample size, methodological quality, and other factors of the included trials, especially for some types of CHIs. For Lentinan, Xiaoxaiping, and Delishen injection, in fact, only one clinical trial was enrolled in present study; therefore, further clinical or pharmacological research on the effects of different CHIs is necessary to support our findings. Furthermore, the survival time or survival rate were regarded as important in judging therapeutic effect of patients with cancer; however, most of the included trials in our study did not report the survival time or survival rate. Therefore, we suggest that the clinical trials of patients with cancer should focus on more meaningful endpoints. Third, no direct head-to-head comparison was conducted between different CHIs. Although CHIs are in clinical application with the adjuvant FOLFOX regimen for treating CRC in China, CHIs are not used as common drugs of conventional cancer treatment in some countries. Additionally, the majority of RCTs included in the study exhibited a relatively high risk of bias, largely in inadequate allocation concealment and blinding. The methodological quality of included RCTs was closely associated to the credibility of evaluation results in a systematic review. For this reason, we suggest that the clinical trials should pay attention to improving the methodological quality in order to support and promote rational use of CHIs. Although the placebo controls would add greatly to the credibility of the findings, there is lack of placebo-controlled trials or direct head-to-head comparisons between different CHIs to provide high-quality evidence-based medical research and verify our findings. Despite the above limitations, our network meta-analysis provides a complete evaluation of the clinical effect and improvement in performance status of different CHIs for CRC patients.
Conclusion
In general, our NMA provides strong evidence supporting different CHIs for CRC patients. Among different types of CHIs, the combination of Compound matrine injection and FOLFOX regimen was associated with more preferable and beneficial options compared with other CHIs groups. Nevertheless, future RCTs that are better designed and large, randomized, controlled, head-to-head trials are needed to confirm these conclusions, particularly in other ethnic groups.
Supplemental Material
Supplementary_part_1 – Supplemental material for Network Meta-Analysis of Chinese Herbal Injections Plus the FOLFOX Regimen for the Treatment of Colorectal Cancer in China
Supplemental material, Supplementary_part_1 for Network Meta-Analysis of Chinese Herbal Injections Plus the FOLFOX Regimen for the Treatment of Colorectal Cancer in China by Dan Zhang, Jiarui Wu, Xiaojiao Duan, Kaihuan Wang, Mengwei Ni, Shuyu Liu, Xiaomeng Zhang, Bing Zhang and Yi Zhao in Integrative Cancer Therapies
Supplemental Material
Supplementary_part_2_EDITS – Supplemental material for Network Meta-Analysis of Chinese Herbal Injections Plus the FOLFOX Regimen for the Treatment of Colorectal Cancer in China
Supplemental material, Supplementary_part_2_EDITS for Network Meta-Analysis of Chinese Herbal Injections Plus the FOLFOX Regimen for the Treatment of Colorectal Cancer in China by Dan Zhang, Jiarui Wu, Xiaojiao Duan, Kaihuan Wang, Mengwei Ni, Shuyu Liu, Xiaomeng Zhang, Bing Zhang and Yi Zhao in Integrative Cancer Therapies
Supplemental Material
Supplementary_part_3_EDITS – Supplemental material for Network Meta-Analysis of Chinese Herbal Injections Plus the FOLFOX Regimen for the Treatment of Colorectal Cancer in China
Supplemental material, Supplementary_part_3_EDITS for Network Meta-Analysis of Chinese Herbal Injections Plus the FOLFOX Regimen for the Treatment of Colorectal Cancer in China by Dan Zhang, Jiarui Wu, Xiaojiao Duan, Kaihuan Wang, Mengwei Ni, Shuyu Liu, Xiaomeng Zhang, Bing Zhang and Yi Zhao in Integrative Cancer Therapies
Supplemental Material
Supplementary_part_4 – Supplemental material for Network Meta-Analysis of Chinese Herbal Injections Plus the FOLFOX Regimen for the Treatment of Colorectal Cancer in China
Supplemental material, Supplementary_part_4 for Network Meta-Analysis of Chinese Herbal Injections Plus the FOLFOX Regimen for the Treatment of Colorectal Cancer in China by Dan Zhang, Jiarui Wu, Xiaojiao Duan, Kaihuan Wang, Mengwei Ni, Shuyu Liu, Xiaomeng Zhang, Bing Zhang and Yi Zhao in Integrative Cancer Therapies
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current research was supported by the National Nature Science Foundation of China (No. 81473547; No. 81673829).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.