
Abstract
Introduction
Breast cancer is one of the most frequently diagnosed cancers and the leading cause of cancer death in females worldwide, accounting for 23% (1.38 million) of the total new cancer cases and 14% (458 400) of the total cancer deaths in 2008.1-3 As in most other countries, breast cancer is by far the most common cancer in women in China and has posed a formidable potential threat to public health owing to its high morbidity and mortality.4-6 Important risk factors associated with breast cancer included estrogen receptor, progesterone receptor, growth factors, and others. 7 Despite the remarkable advances achieved in the fields of surgery, endocrine therapy, chemotherapy, radiotherapy, and targeted therapy against breast cancer over the past several decades, most cases are still suffering from the metastasis, recurrence, and adverse drug reactions (ADRs). 8
As an important part of complementary and alternative medicine, traditional Chinese medicine (TCM) has become one of the main methods for comprehensive anticancer treatment owing to its advantages in treating complications, preventing drug resistance, and so on. 9 According to TCM theory, the basic pathogenesis of breast cancer is the meridian barrier, phlegm retention, qi stagnation, and blood stasis. 10 Therefore, the therapeutic principle is to nourish liver and kidney, strengthen body resistance, and eliminate pathogen. 11 As a new formulation of TCM, Chinese herbal injections (CHIs) own the features of notable curative efficiency and high bioavailability. 12 Among the variety of CHIs, SQFZI has long been extensively used in the clinical setting. It is composed of Codonopsis pilosula (Franch) Nannf and Astragalus membranaceus (Fisch) Bunge and was approved by the State Food and Drug Administration of the People’s Republic of China (CFDA) in 1999. 13 It possesses the effects of nourishing the spleen and stomach, promoting blood circulation, and removing blood stasis. Modern research has revealed that SQFZI has the characteristics of enhancing efficacy and reducing toxicity. 14 SQFZI combined with chemotherapy is currently widely applied for treating breast cancer in China. Considering that a relevant systematic review remains lacking, we intended to investigate the efficacy and safety of SQFZI for breast cancer using meta-analysis to provide valuable evidence for clinical decision making.
Material and Methods
Inclusion and Exclusion Criteria
The inclusion and exclusion criteria were prespecified according to the PICOS (patients, intervention, comparator, outcomes, study design) criteria through discussion by the authors. Only randomized controlled trials (RCTs) meeting the following criteria were included in this meta-analysis: (1) Types of studies: RCTs focused on the effect of SQFZI combined with chemotherapy for the treatment of breast cancer. (2) Participants: all the involved participants were diagnosed as breast cancer according to the pathological, cytological, and histological features. (3) Interventions: the interventions of the control group included conventional chemotherapy agents such as cyclophosphamide, doxorubicin, epirubicin, pirarubicin, 5-fluorouracil, paclitaxel, docetaxel, methotrexate, Changchun ruisabine, gemcitabine, capecitabine, cisplatin, mitomycin, and so forth. The experimental group included studies of SQFZI combined with the same chemotherapeutic drugs as the control group. (4) Outcomes: The primary outcomes of the research included the clinical total effective rate and the performance status. According to the therapeutic effect criterion of the World Health Organization for solid tumors, 15 the clinical total effective rate was calculated by the following formula: (number of complete response patients + number of partial response patients)/total number of patients × 100%. Karnofsky performance status (KPS) was used to assess the performance status of patients. An increase of more than 10 points after treatment was deemed as significant improvement. Additionally, the incidence of immune functions changes (T lymphocyte subsets such as CD3+, CD4+, CD8+, CD4+/CD8+, NK cell, and peripheral hemogram) and ADRs (leukopenia, nausea and vomiting, hepatorenal dysfunction, and so on) were evaluated as secondary outcomes. The criterion of the ADRs met the World Health Organization criteria for common toxicity of chemotherapy drugs released in 1981. 16
Exclusion criteria were as follows: (1) Types of studies: RCTs for which full-text versions were unavailable, case reports, animal experiments, editorials, letters, and review articles; as for any publications shared overlapping information, the more recent and comprehensive article was included. (2) Interventions: The chemotherapeutic drugs, dose, and duration of treatment was incomplete or incorrect. (3) Outcomes: RCTs did not report the data of clinical total effective rate, performance status, and ADRs.
Literature Search
A systematic literature search was conducted to identify the published RCTs with SQFZI for the treatment of breast cancer. The retrieval was performed in the following databases from their inception to October 29, 2017: PubMed, the Cochrane library, Embase, China National Knowledge Infrastructure Database (CNKI), Wan-Fang Database, China Science and Technology Journal Database (VIP), and the Chinese Biomedical Literature Database (SinoMed). “Breast Neoplasm” was regarded as MeSH term. All the searching strategies were developed and adapted for each database. The search strategies of PubMed are listed as follows:
#1 Breast Neoplasm[MeSH Terms]
#2 Breast Cancer[Title/Abstract] OR Mammary Cancer[Title/Abstract] OR Breast Malignant Neoplasm[Title/Abstract] OR Breast Carcinoma[Title/Abstract] OR Breast Malignant Tumor[Title/Abstract] OR Human Mammary Carcinoma[Title/Abstract] OR Human Mammary Neoplasm[Title/Abstract]
#3 #1 OR #2
#4 Shenqi Fuzheng
#5 Randomized Controlled Trial[Publication Type]
#6 Controlled Clinical Trial[Publication Type]
#7 random*[All Fields]
#8 #5 OR #6 OR #7
#9 #3 AND #4 AND #8
Data Extraction and Quality Assessment
Two independent reviewers performed the data extraction and in case of discrepancies, a third reviewer would be consulted. The following contents were considered in data extraction: (1) baseline characteristics of included RCTs—the first author, publication date; (2) characteristics of patients—the number of patients in the experimental group and the control group, age, TNM stage; (3) details of intervention—the names, dosages, and treatment cycles of SQFZI; and (4) outcomes—the measured data about clinical total effective rate, performance status, ADRs and immune function. All literature was managed by NoteExpress (Wuhan University Library, Wuhan, China).
Methodological quality assessment of each RCT was conducted by the Cochrane risk of bias tool (Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0). 17 Disagreements were resolved by methodological experts to reach consensus. Besides, 5 domains of bias that are relevant to the quality of RCTs, namely random sequence generation (selection bias), allocation concealment (selection bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective outcome reporting (reporting bias), and other bias were considered. If any RCTs described a correct random generation, or implemented blinding or reported complete measure outcomes, this RCT belonged to “low risk.” Otherwise, trials were judged as “high risk.” The evaluation of “Unclear” meant that the literature did not provide enough information for judgments.
Statistical Analysis
This current meta-analysis pooled data from clinical trials via Review Manager 5.3 (Cochrane Collaboration, Oxford, UK). 18 Dichotomous outcomes were presented as relative risk (RR), whereas continuous variable was evaluated by mean difference, and 95% confidence intervals (95% CIs) of outcomes were calculated to indicate the range of results. The chi-square test was applied to evaluate heterogeneity among studies, and I2 was used to show the magnitude of this heterogeneity. Results of P ≥ .1 and I2 ≤ 50% suggested a lack of significant heterogeneity; the fixed-effect model was used accordingly. 19 For cases with P < .1 and I2 > 50%, we adopted a random-effect model, and subgroup analysis was presented to explore the sources of heterogeneity. 20 Meanwhile, the visual inspection of publication bias was demonstrated by funnel plot. Egger’s test and Begg’s test were also adopted, the result of P > .05 showed that there was no obvious publication bias among included studies. 21 In addition, sensitivity analysis was conducted in clinical total effective rate so as to test the stability of results, by excluding the RCT seriatim to resynthesize the data. Egger’s test, Begg’s test, and sensitivity analysis were estimated and processed using STATA 13.0 software (Stata Corporation, College Station, TX, USA). 22
Results
Literature Search and the Characteristics of Included RCTs
Our research yielded a total of 209 RCTs by a primary search of the aforementioned literature databases. After reading the titles and abstracts by 2 reviewers respectively, 63 RCTs were retrieved in full text, of which 32 were excluded due to the following reasons: not complying with the intervention of inclusion criteria (12 RCTs); not referring to the diagnostic standard or therapeutic criteria (15 RCTs); improper randomization method (3 RCTs); could not obtain the full text (2 RCTs). Ultimately, 31 related RCTs were deemed eligible in this meta-analysis. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram in Figure 1 illustrates the selection process.

Flowchart of literature search.
There were 1292 and 1251 patients in the experimental group and control group, respectively. Among included RCTs, the sample size ranged from 40 to 185. All the patients qualified were women, who received treatment once a day intravenously, and the most frequent period of treatment was 21 days in 9 trials (29%). More details form the included studies are presented in Table 1.
The Basic Characteristics of the Included Studies.

Abbreviations: E, experimental group; C, control group; CAF, cyclophosphamide+ doxorubicin+ 5-fluorouracil; CTF, cyclophosphamide+ pirarubicin+ 5-fluorouracil; CEF, cyclophosphamide+ epirubicin + 5-fluorouracil; ATC, anthracyclines; NE, navelbine+ epirubicin; CMF, cyclophosphamide + methotrexate + 5-fluorouracil; ECX, capecitabine; TA, paclitaxel + doxorubicin; TD, pirarubicin + docetaxel; TC, docetaxel + Epirubicin; NVB, navelbine; GEM, gemcitabine; DDP, cisplatin; MMC, mitomycin.
①, the clinical total effective rate; ②, the performance status; ③, adverse drug reactions (ADRs); ④ immune function.
Quality Assessment
After performing quality assessment, only 3 RCTs adopted a random number table to generate the group, 1 RCT grouped patients by the toss of a coin.28,29,37,52 Therefore, their selection bias was evaluated as “low risk.” Five RCTs grouped in congruence with the therapeutic methods or admission time, so the selection bias was remarked as “high risk.”36,42,48,54 The other 22 RCTs did not illustrate the specific method of random sequence generation, therefore their selection bias was “unclear risk.” Information on allocation concealment and blinding was not observed in the trials. Hence this study evaluated the selection bias of allocation concealment, performance bias, and detection bias as “unclear.” Moreover, none of the included RCTs assessed had incomplete data, thus the attrition bias and reporting bias were assessed as “low risk.” Additionally, none of the RCTs offered any details contributing to high risk for other bias, so this item was appraised as “unclear risk.” Graphical description about quality assessment is shown in Figure 2.
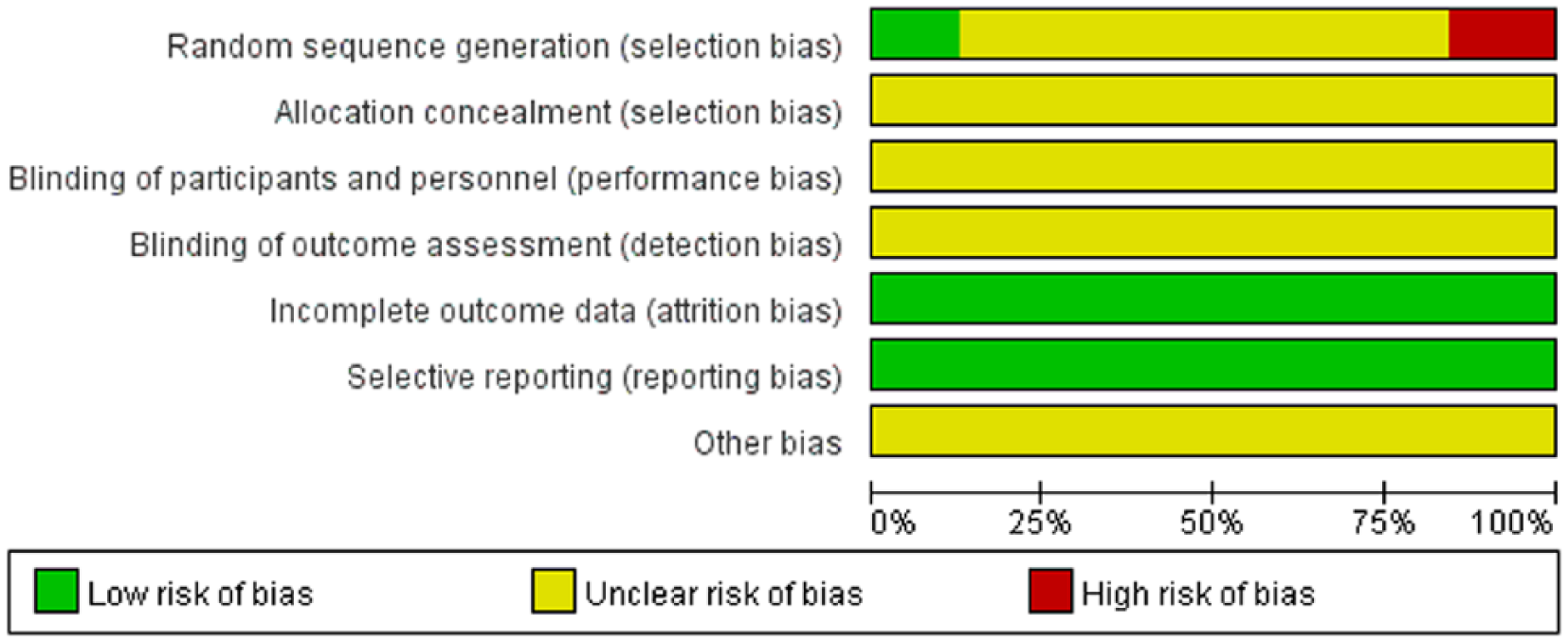
Risk of bias summary.
Outcomes
Clinical Total Effective Rate
Depending on use of anthracycline, all chemotherapy regimens were divided into anthracycline-based subgroup and other chemotherapeutic drugs subgroup. The former contained 3 main chemotherapies: cyclophosphamide + doxorubicin + 5-fluorouracil (CAF), cyclophosphamide + pirarubicin + 5-fluorouracil (CTF), or cyclophosphamide + epirubicin + 5-fluorouracil (CEF).We assessed the clinical total effective rate in 2 subgroups respectively. The results of subgroup analysis are as follows.
Anthracycline-based subgroup: 9 RCTs were available in this subgroup and displayed no heterogeneity (P = .90 > .1, I2 = 0% < 50%); a fixed-effect model was used.24,27,28,31,32,34,35,39,40 The results indicated a statistically significant difference between SQFZI group and control group; thus, in terms of clinical total effective rate, SQFZI combined with anthracycline-based chemotherapy was superior to the anthracycline-based chemotherapy alone (RR = 1.36, 95% CI 1.21-1.53, P < .00001).
Other chemotherapeutic drugs subgroup: 4 RCTs demonstrated no evidence of heterogeneity in this subgroup, so the fixed-effect model was adopted (P = .12 > .1, I2 = 48% < 50%).46,48,49,52 The results of meta-analysis presented a better impact when adding SQFZI than using other chemotherapeutic drugs alone. The difference between two groups was statistically significant (RR = 1.22, 95% CI 1.03-1.44, P = .02).
There was no obvious interstudy heterogeneity reported among the subgroups (P = .31 > .1, I2 = 4.3% < 50%), hence it is acceptable that the results derived from 2 subgroups could be amalgamated. The pooled analysis demonstrated that SQFZI group performed even better on improving clinical total effective rate than control group, which received chemotherapeutic alone. The difference between SQFZI group and control group was considered as statistically significant (RR = 1.31, 95% CI 1.19-1.44, P < .00001; Figure 3).
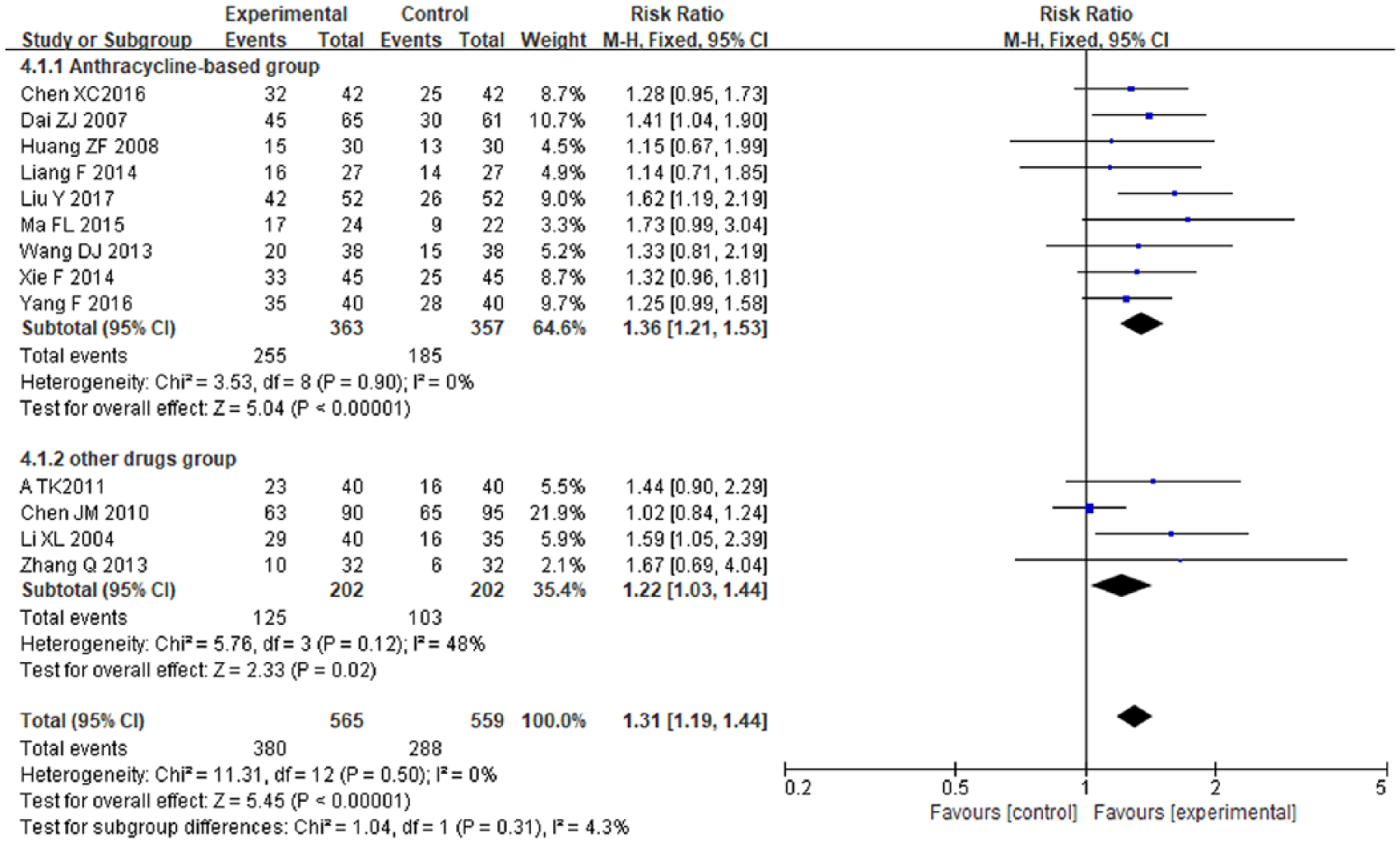
Forest plot of the clinical total effective rate.
Sensitivity Analysis and Publication Bias
For the outcome of clinical total effective rate, a sensitivity analysis was carried out to verify the stability of result. As shown in Figure 4, since the clinical total effective rate did not show a qualitative transform, the result of sensitive analysis was robust.
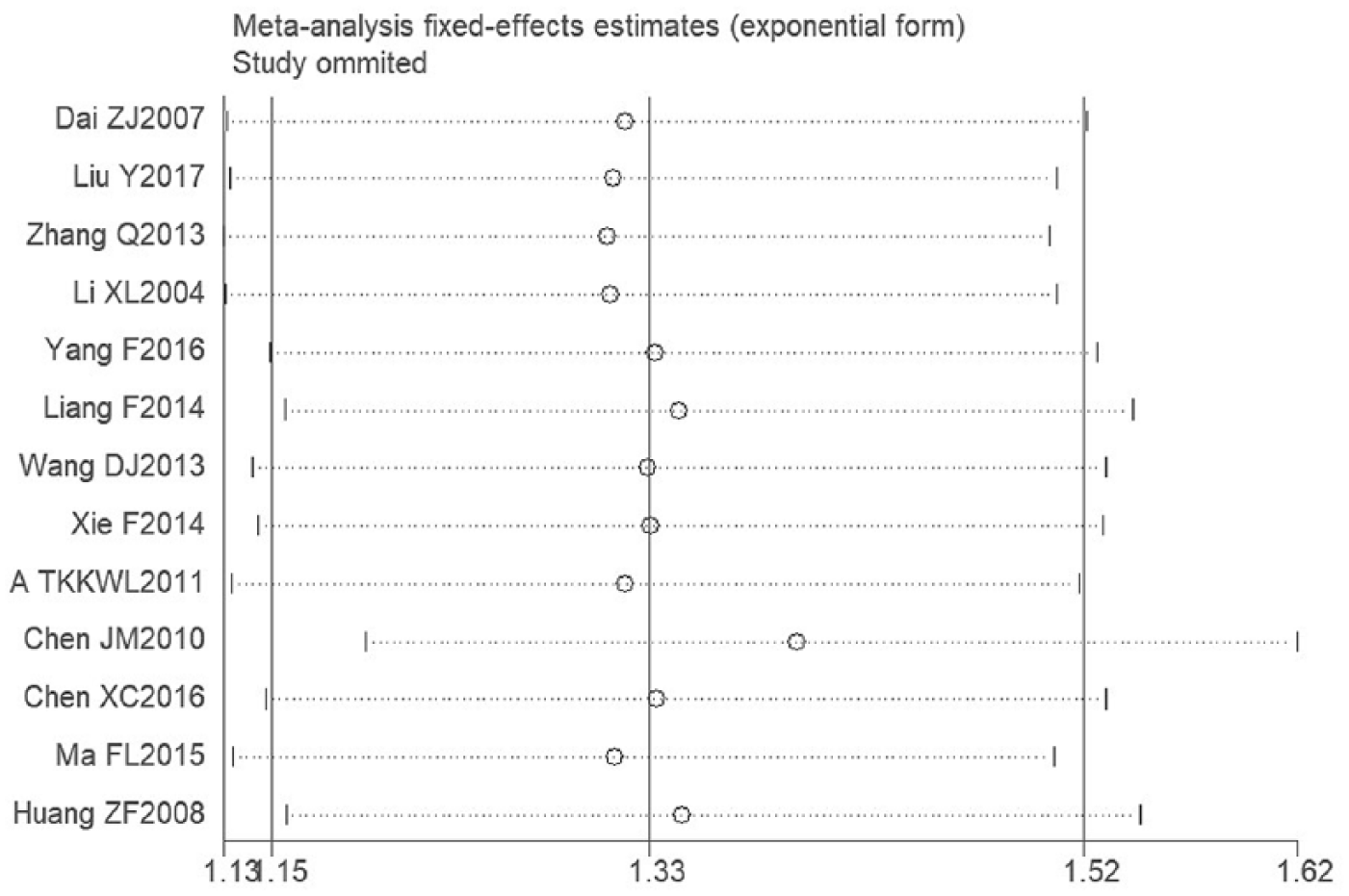
Sensitivity analysis of the clinical total effective rate.
Although the results of Egger’s test (t = 2.20, P = .05) and Begg’s test (z = .92, P = .360 >.05) indicated no significant publication bias, the funnel plot on publication bias for clinical total effective rate presented modest asymmetry (Figure 5), which suggested that there might be potential publication bias among included RCTs.

Funnel plot of the clinical total effective rate.
Performance Status
Anthracycline-based subgroup: No significant heterogeneity was detected among 10 RCTs of this subgroup (P = .24 > .1, I2 = 23% < 50%), thus we applied the fixed-effect model.23-26,30,34-36,41,42 Compared with anthracycline-based therapy alone, the SQFZI group was more effective in raising performance status (RR = 2.29, 95% CI 1.79-2.93, P < .00001); the difference between 2 groups was considered to be statistically significant.
Other chemotherapeutic drugs subgroup: There were 5 RCTs in this subgroup.44,46-48,53 After examination, no heterogeneity was found, so we adopted fixed-effects model (P = .43 > .1, I2 = 0% < 50%). It turned out that SQFZI combined with other chemotherapeutic drugs was superior to chemotherapy based on other drugs alone for improving performance status of patients. The difference between the groups was statistically significant (RR = 2.04, 95% CI 1.55-2.68, P < .00001).
No visible heterogeneity was obtained between the two subgroups (P = .55 > .1, I2 = 0% < 50%), so we merged these subgroups into one group. The result demonstrated that SQFZI group achieved better effects than the control group, which received chemotherapeutic drugs alone; the difference between the above 2 groups had statistical significance (RR = 2.18, 95% CI 1.82-2.62, P < .00001; Figure 6).
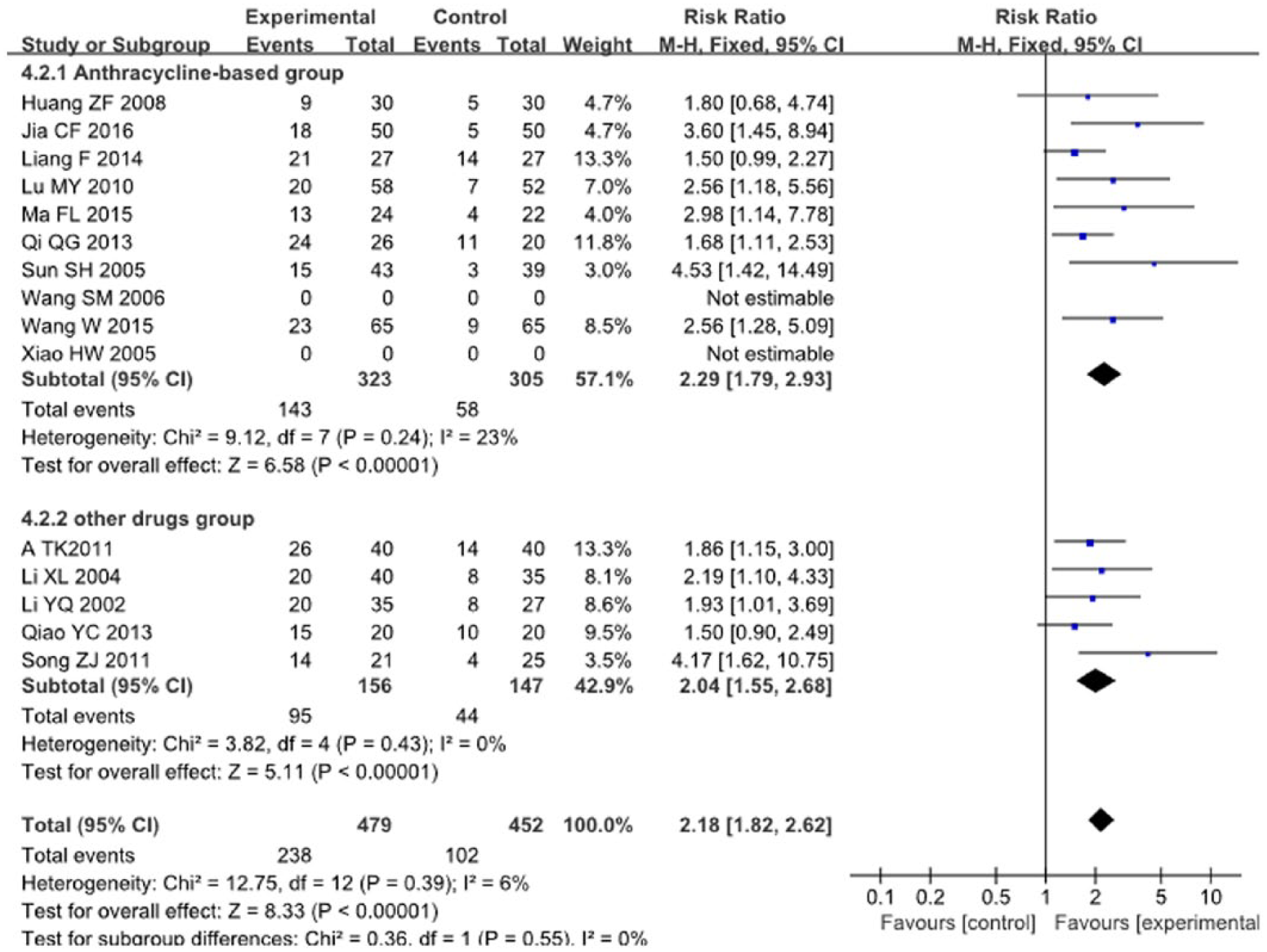
Forest plot of the performance status.
Other Outcomes
This study made a qualitative description for immune function of patients, which was considered as secondary outcome. The pooled analysis demonstrated that SQFZI group performed better in preventing the loss of peripheral T-lymphocyte subsets (CD4+, CD4+/CD8+), NK cell, leukopenia, and platelets. However, the combination of SQFZI and chemotherapy failed to achieve a better effect on CD3+, CD8+, and hemoglobin. More details regarding immune function were presented in Table 2.
Results of Other Outcomes.

Adverse Drug Reactions
In this meta-analysis, we mainly discussed three representative ADRs (leukopenia, nausea, and vomiting and hepatorenal dysfunction) and other ADRs to assess the curative effect of experimental group:
Twelve RCTs reported leukopenia.24,27,32-34,36,39,44,45,47,48,52 The overall results demonstrated that the combination of SQFZI and chemotherapy was more efficient in relieving leukopenia than the control group which only received the chemotherapy; these between-group differences were statistically significant (RR = 0.51, 95% CI 0.41-0.64, P < .00001; Figure 7a).
Eight RCTs covered data on nausea and vomiting: pooled results showed that SQFZI plus chemotherapy decreased nausea and vomiting compared with chemotherapy alone.27,32-34,38,45,48,52 There was no statistically significant between-group difference (RR = 0.51, 95% CI 0.40-0.66, P < .00001; Figure 7b).
Seven RCTs investigated hepatorenal dysfunction.24,27,28,31-33,48 The results demonstrated that the conjunctive use of SQFZI and chemotherapy can decrease the incidence of hepatorenal dysfunction observably, and no significantly statistical difference was found (RR = 0.38, 95% CI 0.25-0.59, P < .0001; Figure 7c).

The forest plot of adverse drug reactions (ADRs): (a) leukopenia, (b) nausea and vomiting, and (c) hepatorenal dysfunction.
Additionally, this meta-analysis demonstrated that the SQFZI group had better efficacy in relieving other ADRs caused by chemotherapeutic drugs, including electrocardiogram changes, alopecia, intestinal reaction, thrombocytopenia, hemoglobin reduction, myelosuppression, and fatigue (Table 3).
Results of Other Adverse Drug Reactions (ADRs).

Discussion
This meta-analysis assessed the available evidences derived from 31 RCTs to detect the efficacy and safety of SQFZI combined with chemotherapy in treating breast cancer. According to the foregoing results, SQFZI plus chemotherapy can make a nonnegligible influence versus chemotherapy alone in terms of improving clinical total effective rate and performance status. Subgroup analysis revealed that especially in improving performance status of patients, SQFZI combined with chemotherapy showed a more impressive effect. Simultaneously, this combined chemotherapy approach also enhanced immune function of breast cancer patients and relieved ADRs.
Breast cancer poses threats to the health and safety of human life. Although the treatment of this disease has been constantly improved, ADRs of patients have still increased year by year, which becomes a significant handicap to enhancing the curative effect of breast cancer. 3 In TCM theories, the occurrence of breast cancer is mostly associated with invasion of exopathogens and the deficiency of Qi-blood. 54 TCM possesses unique advantages of overall regulation and syndrome differentiation treatment as well as addressing both the symptoms and the root causes of the disease. 55 Related pharmacological studies have shown that SQFZI promotes the proliferation of macrophages in vitro, thereby improving the immunosuppression caused by chemotherapeutic drugs.56-57 Furthermore, research suggested that astragaloside could inhibit the proliferation of tumor cells in S phase and G2/M phase, suppress the expression of p21 and reduce the activity of cyclin-dependent kinase. 58 The authors concluded that astragaloside could be used as an effective adjuvant chemotherapeutic drug in cancer treatment. 59 As one of the effective components of Codonopsis pilosula, Codonopsis pilosula polysaccharides (CPP) could cause the inhibition of SMMC-7721 cells of hepatoma cells without obvious toxicity to viscera of Kunming mice. 60 To summarize, these 2 kinds of Chinese herbs synergistically nourish Qi-blood, reinforce kidney and spleen, and eliminate stagnation.
Currently, there is a lack of systematic reviews comparing SQFZI combined with chemotherapy in the treatment of breast cancer. In this regard, our meta-analysis provides relevant medical evidence in this field and has the following advantages: First, to our knowledge, the present study is the first meta-analysis which delved into the efficacy and safety of SQFZI combined with chemotherapy in treating breast cancer. Second, we conducted a comprehensive literature search to identify the published studies through the combination of MeSH terms and text words. Clearer inclusion and exclusion criteria have been introduced, and the patients were diagnosed with breast cancer by a definite diagnostic standard, with a relatively consistent baseline. Third, we carried out subgroup analysis in the light of whether anthracyclines were used or not, which demonstrated that regardless of use of anthracyclines, chemotherapy drugs combined with SQFZI had superior curative effect. Arguably, no conspicuous intergroup heterogeneity was found between 2 subgroups.
However, because of the limited data available for this population, the present meta-analysis had some limitations. First, only 5 RCTs specifically described randomization method, whereas they did not make a detailed description of random sequence connation, allocation concealment, or blinding methods. Besides, most items were assessed as unclear risk, which may have therefore affected the reliability of the results. Second, though the Egger’s test and Begg’s test manifested that there was no potential publication bias in present study, the deficiency of the funnel plot’s bottom also indicated a lack of RCTs with large sample. Third, our results might have limited generalizability because all of the included RCTs were performed in China among Chinese populations; therefore, it is unclear whether the effect may change when SQFZIs are used in populations of other ethnicities and in different geographical locations. Fourth, because of the original research limitation, we failed to evaluate the long-term effect of SQFZI. On account of the limitations mentioned above, we raise several suggestions: first, RCTs are supposed to be registered in advance and implemented according to CONSORT standard so as to ensure the transparency of trial process. 61 Meanwhile, the clinical trials should pay more attention to randomization, concealment, blinding methods, and long-term follow-up to provide high-quality evidence-based medical evidence for clinical decision making. In addition, clinicians ought to strengthen monitoring of ADRs while remaining concerned on the measurement of effectiveness. It is the responsibility of the medical staff to use SQFZI as per the instruction guidelines and monitor the occurrence of ADRs.
Conclusions
In summary, this study revealed that the combination of SQFZI and chemotherapy had a better effect on treating breast cancer. However, due to the limitations of the current meta-analysis, the strength of evidence needs to be promoted by rigorously designed, multicentered, large-sample randomized double-blind controlled trials.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Nature Science Foundation of China (No. 81473547; No. 81673829).