
Abstract
Cancer survivors experience high levels of distress, associated with a host of negative psychological states, including anxiety, depression, and fear of recurrence, which often lead to sleep problems and reduction in quality of life (QOL) and well-being. As a neuropeptide hormone associated with affiliation, calmness, and well-being, oxytocin may be a useful biological measure of changes in health outcomes in cancer survivors. In this exploratory study, which comprised a subset of participants from a larger study, we evaluated (a) the feasibility and reliability of salivary oxytocin (sOT) levels in cancer survivors and (b) the effects of 2 sleep-focused mind–body interventions, mind–body bridging (MBB) and mindfulness meditation (MM), compared with a sleep hygiene education (SHE) control, on changes in sOT levels in 30 cancer survivors with self-reported sleep disturbance. Interventions were conducted in 3 sessions, once per week for 3 weeks. Saliva samples were collected at baseline, postintervention (~1 week after the last session), and at the 2-month follow-up. In this cancer survivor group, we found that intra-individual sOT levels were fairly stable across the 3 time points, of about 3 months’ duration, and mean baseline sOT levels did not differ between females and males and were not correlated with age. Correlations between baseline sOT and self-report measures were weak; however, several of these relationships were in the predicted direction, in which sOT levels were negatively associated with sleep problems and depression and positively associated with cancer-related QOL and well-being. Regarding intervention effects on sOT, baseline-subtracted sOT levels were significantly larger at postintervention in the MBB group as compared with those in SHE. In this sample of cancer survivors assessed for sOT, at postintervention, greater reductions in sleep problems were noted for MBB and MM compared with that of SHE, and increases in mindfulness and self-compassion were observed in the MBB group compared with those in SHE. The findings in this exploratory study suggest that sOT may be a reliable biological measure over time that may provide insight into the effects of mind–body interventions on health outcomes in cancer survivors.
Introduction
Cancer survivors experience high levels of distress, whether after receiving a cancer diagnosis or during or following major cancer treatment, such as radiation, chemotherapy, and surgery. In many cancer survivors, posttreatment distress can be accompanied by a host of negative psychological states, including depression, despair, anxiety, posttraumatic stress symptoms, and fear of cancer recurrence, as well as sleep disturbance.1-3 Sleep disturbance is a significant health problem in general, and is particularly so in cancer survivors, because of the role it may play in contributing to cancer occurrence and progression. 4 Developing effective treatments to improve sleep might also help reduce distress and associated emotional states and generally improve the lives of cancer survivors. Since many cancer survivors are interested in nonpharmacological interventions to help deal with sleep problems and co-occurring conditions, 5 it is important to assess how effective these nonpharmacological interventions are in improving the lives of cancer survivors. Besides the use of validated self-reported outcome measures, biological measures are increasingly used to evaluate the efficacy of these interventions and to elucidate potential mechanisms whereby these interventions might improve health outcomes in cancer survivors. 6 Understanding physiological mechanisms involved in improving health, quality of life (QOL), and well-being in cancer survivors is especially important, since biomarkers used to evaluate the efficacy of psychosocial interventions may themselves be implicated in cancer disease processes. For example, while the stress hormone cortisol, a glucocorticoid, has provided some insight into the impact of psychosocial interventions in ameliorating stress in cancer survivors, 7 glucocorticoids are increasingly studied to understand their influences in cancer occurrence and progression. 8 Since stress hormones exert anti-inflammatory effects, and impaired immune function is involved in tumor formation potentially leading to metastases, 9 targeting stress hormones might lead to beneficial outcomes in cancer prognosis. Additionally, it would be helpful to identify other biological measures that might provide mechanistic evidence of improved well-being and QOL in cancer survivors following psychosocial interventions, as well as the biological measures having a more direct relevance to, and involvement in, cancer. One candidate biomarker receiving much attention in relation to improved psychosocial states is the hormone oxytocin (OT), which may be particularly pertinent to study in cancer survivors, given their high levels of distress, negative affect, and other psychological health conditions, as well as sleep disturbance. Furthermore, OT may be involved in the regulation of cancer cells and may also be implicated in influencing sleep patterns. In view of the potential role of OT in cancer and sleep, and the lack of studies examining peripheral, endogenous OT in cancer survivors, the aims of this study were to investigate the suitability and applicability of using salivary OT (sOT) to determine (a) the impact of mind–body interventions targeting sleep on sOT release, (b) the feasibility and reliability of measuring sOT in a clinical study, and (c) associations between sOT and psychosocial variables. Overall, these aims served to evaluate the reliability and suitability of sOT as a biological indicator of positive health outcomes following psychosocial interventions in cancer survivors.
Oxytocin is a neuropeptide hormone produced in the hypothalamus, whose release activates a variety of brain regions leading to multiple physiological and behavioral effects. Oxytocin has been implicated in birth (labor), lactation, maternal behavior, parental care, social bonding, affiliation, and well-being.10-12 In recent human studies, OT has been shown to be associated with social bonding,13-16 trust,17-20 altruism and generosity, 21 parochial altruism, 22 cooperation, 23 empathy,24,25 and well-being. 26 These findings have been established in studies measuring endogenous (circulating) as well as exogenously administered intranasal OT. 27 The various functions attributed to OT have led to increased interest in understanding the role of OT as a mediator of prosocial behaviors, with implications for promoting health and well-being in humans.
Although OT was originally recognized for its physiological functions, specifically its role in reproduction, and notably parturition and lactation, it has also been identified in other peripheral tissues such as heart, kidney, pancreas, and thymus, where it mediates its effects via OT receptors located in these organs. 28 More recently, OT receptors were identified in neoplastic tissues, 29 in which OT might play a regulatory role in tumor growth, since in vitro studies demonstrated that OT inhibited the proliferation of breast, endometrial, glial and neural, and bone neoplastic cell lines, and an in vivo study showed that OT inhibited breast tumor growth in mice that were injected with a mammary tumor and treated with subcutaneous pulsatile administration of OT (reviewed in Cassoni et al 30 ). In contrast, OT can also stimulate tumor growth, as identified in other human choriocarcinoma cell lines, or endothelial-derived sarcomatous cell lines from Kaposi’s sacrcoma; this stimulatory effect has been also noted in normal nonneoplastic endothelial cells in vitro (see Cassoni et al 30 ). Further studies are necessary to explicate the regulatory processes of OT in cancer cells to further understand potential clinical effects of OT in cancer.
Despite some understanding of the role of OT in cancer cells, there is virtually no information available about circulating (plasma) or salivary OT in cancer patients at any stage of cancer diagnosis, or in cancer survivors. As such, very little is known regarding relationships between OT and clinical variables of cancer or prognosis. Obtaining this information is crucial if OT levels in cancer survivors could provide some understanding of whether a cancer patient or survivor has a potentially worsened or improved prognosis. Knowing what constitutes “healthy” OT levels in cancer survivors could additionally provide important information for inferences about a cancer survivor’s prognosis. Since OT has shown to be involved in the regulation of prosocial behaviors and can moderate relationships between psychosocial variables,31,32 characterizing fluctuations in OT based on changes in these other variables might provide an understanding of potential mechanisms whereby OT might exert its effects to improve cancer survivors’ psychological states. Furthermore, if OT could be positively regulated by psychosocial or mind–body interventions, which would elicit increased well-being and decreased stress and anxiety, this finding might provide some rationale for developing interventions to enhance these psychosocial states, specifically in terms of enhancing their well-being and QOL, which might have implications for improving the prognosis of cancer survivors.
The involvement of psychosocial factors in cancer occurrence and progression is an active area of interest. 8 Psychosocial factors can interact with tumor cells via systemic and molecular communication involving the neuroendocrine system. 33 One psychosocial factor known to be implicated in cancer is social support, which might be a significant predictor of cancer progression. 34 Social support is positively correlated with endogenous OT levels, 14 and OT can enhance the effects of social support to improve health outcomes, related to stress, 35 immune function, 31 and sleep. 32 Thus, it is possible that OT could also mediate the relationship between social support and cancer prognosis and might also impact sleep performance.
The role of OT in sleep has not been extensively evaluated in humans, and one study on the topic indicated that OT levels are not altered by sleep or stage of sleep. 36 However, OT might indirectly influence sleep patterns by its anxiolytic effects, and its ability to facilitate reduced stress responses, mediated through its effects on the hypothalamic–pituitary–adrenal (HPA) axis.37,38 In rodents, OT in the brain can regulate the HPA axis by inhibiting both basal and stress-induced adrenocorticotropin hormone (ACTH), and consequently glucocorticoid (corticosterone) release, as well as the ACTH hypothalamic releasing hormone, corticotropin releasing hormone (CRH).39,40 Among the many significant functions of the hypothalamus is its involvement in sleep–wake activities 38 ; both the HPA axis and CRH influence sleep patterns in animals and humans.39,40 Since OT is produced in the paraventricular nucleus (PVN) of the hypothalamus, which is involved in regulating sleep and arousal, OT may indirectly influence sleep–wake behavior through its actions on the HPA axis and CRH. 38 Alternatively, OT may be more directly implicated in sleep as shown in rodents, in which central (brain) OT administration led to wakefulness, while blocking OT release with an OT receptor antagonist resulted in reductions in non–rapid eye movement and pre–rapid eye movement sleep, suggesting an hypnotic effect of OT. 41 Lancel et al 41 postulated a dual mechanism of physiological action of central oxytocin on sleep: under basal conditions, endogenous oxytocin may stimulate physiological sleep, whereas under conditions of stress, related to increased levels of brain oxytocin, OT may contribute to behavioral arousal and/or impaired sleep quality. Following this thread, OT may exert similar effects on sleep in humans, especially those exhibiting chronic stress and sleep disturbance. Given that OT may influence sleep and other behavioral variables depending on its concentration, OT might account for differences in health outcomes, including sleep. For example, in low-income minority women living with HIV, perceived stress was associated with better immune status, and friendships with improved sleep, in those with high, but not low, OT levels.31,32
So how might OT elicit these beneficial effects? Given OT’s role in strengthening affiliations and promoting social interactions, endogenous OT has been hypothesized to promote relaxation and reduce feelings of vulnerability, and to engender feelings of increased safety and well-being as well as its ability to confer a sense of connectedness. 42 Endogenous OT can also act as a buffer against stressful situations, an “antistress system,” to inhibit negative psychological states, including stressful, anxious, or fearful behaviors and feelings. 37 As indicated earlier, OT is hypothesized to exert these anxiolytic effects by reducing autonomic nervous system reactivity via the HPA axis and cardiovascular stress system to lower heart rate and return blood pressure to normal levels.37,43 These stress- and anxiety-reducing features of OT make it a promising hormone to examine in clinical populations such as cancer survivors, who are particularly prone to high levels of stress.
It would be helpful to identify therapeutic interventions that target the oxytocinergic system to assist in reducing negative psychological states and improving psychosocial factors to foster longer-term health benefits. 11 Therapies especially incorporating strong affiliative and tactile components could harness the beneficial effects of OT, as indicated above. Indeed, gentle or warm touch and massage have been shown to instill feelings of relaxation, calmness, well-being, and connectedness, and reduce stress and anxiety, 37 and may be associated with increases in endogenous OT levels.37,44-48 Thus, touch therapies, acting in part by triggering OT release, may help reduce distress, by inducing feelings of calmness, relaxation, and well-being in clinical populations, including cancer survivors.
Another group of healing modalities effective in reducing stress and negative psychological states are mind–body interventions (MBIs) such as mindfulness-based stress reduction (MBSR) 49 and mindfulness-based cognitive therapy (MBCT),50,51 as well as a more recent addition, mind–body bridging (MBB). 52 MBIs have produced benefits in several clinical and healthy populations, including cancer survivors, and MBIs have been shown to be associated with declines in stress, depression, sleep disturbance, and increases in well-being and QOL.53-57 The effects of MBIs in treating sleep disturbance in cancer survivors is particularly relevant, since many survivors experience poor sleep, which is associated with stress, anxiety, depression, fatigue, 1 and fear of cancer recurrence. 2 Thus, MBIs targeting stress and co-occurring conditions and reducing mental health problems can help improve sleep, as has been documented in cancer survivors in a number of studies.5,58-61 Given the positive influences of MBIs on health outcomes, these improvements may also facilitate OT release, with positive health outcomes, as indicated previously. Thus, MBIs improving psychological states and influencing OT release could have potentially long-term benefits in cancer survivors.
In this exploratory and feasibility study, which analyzed a subset of participants from the main study, 61 we evaluated the effects of 2 sleep-focused mind–body therapies (MBB and MM) on sOT levels in cancer survivors with self-reported sleep disturbance. The data in the present study are drawn from the larger main study investigating the effects of mind–body therapies on sleep disturbance and co-occurring symptoms in cancer survivors. Results of the main study indicated that the mind–body therapies were associated with reduced sleep disturbance and depression, as well as increased well-being, mindfulness, and self-compassion. 61 We hypothesized that these mind–body therapies would be associated with increases in sOT levels to a greater extent than would the sleep hygiene control, concomitant with improved sleep and co-occurring symptoms.
Methods
Participants
Details of the methodological aspects of this study have been presented in the main study 61 and are provided here briefly. Participants were a subset of the main study, comprising 30 cancer survivors, and including 21 females and 9 males, 29 to 74 years old, recruited primarily from various cancer hospitals and oncologists in private practice and a nonprofit cancer support center.
Inclusion Criteria
To be eligible, participants had completed active cancer treatment (surgery, chemotherapy, or radiation) at least 3 months prior to the start of the first intervention session. Cancer survivors were included if they exhibited self-reported sleep disturbance, as measured by a validated sleep questionnaire (Medical Outcomes Study Sleep Scale [MOS-SS]), 62 with a score of 35 or greater on a composite summary subscale, the Sleep Problems Index II subscale (SPI-II). Individuals were excluded if they were not in remission or had metastatic disease, as was determined by their oncologist. They were also excluded if they displayed any serious mental health issues and had been previously exposed to MBB, MM, MBSR, or MCBT. The University of Utah Institutional Review Board approved the study protocol.
Study Design
In this prospective randomized-controlled study, we investigated the effects of sleep-focused mind–body interventions, MBB and MM, compared with a sleep hygiene education control (SHE), on sOT levels, in this subset of cancer survivor participants from the main study, 61 who had provided saliva samples for sOT evaluation. We additionally assessed this subset sample for sleep disturbance, and other validated self-report questionnaires, including perceived stress, depression, cancer-related QOL, well-being, mindfulness, and self-compassion, to determine if the results obtained in this subset were consistent with those obtained in the main study, as well as to examine potential associations between sOT levels and sleep, and psychological states.
Study Procedures
Cancer survivors completed a screening questionnaire about their sleep patterns, demographics, cancer history (type of cancer and treatment), medical history, and medications/supplements used. If they were provisionally eligible, the study team contacted their health care provider (with the participant’s signed consent) to verify that they were mentally competent and their cancer treatment status did not preclude participation in the study. Participants agreed to participate in the study by signing an informed consent form.
Following enrollment, participants were randomly assigned to one of the mind–body interventions or sleep education control. Each intervention comprised 3 sessions, conducted over 3 consecutive weeks and lasting approximately 2 hours each session. Saliva samples were collected at pre-intervention (baseline; Pre), postintervention (1 week after the third and final session, Post), and follow-up (2 months posttreatment), and the self-report measures were collected at the same time points.
Interventions
Sleep Hygiene Education (Control)
The instructor advised participants about using sleep hygiene approaches to deal with their cancer-related sleep issues. Each week, various sleep topics were discussed, including (a) possible causes of sleep disturbance, such as some medications, distress, anxiety, depression, or pain; (b) worries, concerns, and questions about sleep disturbance; (c) tips for getting a better night’s sleep, such as diet, exercise, supportive care; (d) preparing for sleep; (e) tips on behaviors that could negatively influence sleep quality; and (f) side-effects of sleep medications. After the various topics were presented, the group discussed their sleep issues related to their cancer experiences. Participants were encouraged to practice SHE recommendations on a daily basis. SHE was conducted by a licensed clinical social worker with experience in working with cancer survivors.
Mindfulness Meditation Program
Mindfulness meditation was an adaptation of Mindfulness-Based Stress Reduction (MBSR), 49 which teaches awareness and mindfulness skills, including basic meditation practice and yoga. MBSR provides individuals with experiential tools and mindfulness techniques that help them observe their thoughts, emotions, and physical sensations and become more aware of the present moment to deal with stressful events in their lives. MBSR has been shown to reduce stress, sleep disturbance, and other behavioral problems and has been tested in both healthy subjects and those with clinical illnesses, including cancer survivors (for a meta-analysis review, see Grossman et al 63 ). MBSR for sleep disturbance employs a 6-week-long format,64,65 which is twice as long as the MM program implemented in the present study. While the 3-week MM program in the present study was not intended to cover all the elements included in the standard MBSR program, the specific goal of MM was to focus on and teach mindfulness meditation (eg, sitting, walking, and body scan). The MM course included fundamental mindfulness meditation skills (breath awareness, awareness of thoughts and emotions), body scans, walking meditation, and forgiveness meditation. After learning basic techniques, later sessions focused on ways in which participants implemented and integrated mindfulness into their daily lives. Participants also used a writing exercise to express a cancer-related concern that was stressful, with a focus on including emotional content and expressing themselves as fully as possible. The writing exercise was included in MM to help participants become more aware of their thoughts, feelings, and emotions through their writings. Previous research indicates that expressive writing may help cancer survivors reduce their distress and fear of cancer recurrence, and in doing so, improve their psychological and physical health, including sleep disturbance related to cancer. 66 Handouts for the course included MBSR CDs for mindfulness meditation, a copy of the book, Full Catastrophe Living, 49 and a printout of “The practice of mindfulness” taken from the book, and stress reduction tips. MM was conducted by a licensed clinical social worker certified in MBSR.
Mind–Body Bridging Program
Mind–body bridging is a mind–body intervention useful for a wide range of mental and physical health problems. 52 MBB teaches mindfulness and awareness skills to help individuals recognize and become aware of potentially dysfunctional mental and bodily states, as indicated by ruminative thoughts and decreases in awareness, and body tension, which could lead to potentially negative health outcomes. MBB provides experiential exercises in which individuals are taught to pay attention to sights, sounds, and sensations to calm their minds and relax their bodies. They are also taught “mapping” exercises, which may help reveal specific types of thought patterns, known as “requirements,” which are expectations about how people and the world should be at a particular moment. Examples of requirements are, “I should cope with my cancer more effectively” and “I should not have any cancer symptoms.” Requirements can elicit negative feelings and emotions, which may contribute to distress, fear, anxiety, and worry, in the context of the cancer experience. Over time, requirements that are unmet may contribute to a dysfunctional mind–body state, through perpetuation of negative psychological states and associated body tension. Conversely, using awareness practices and defusing requirements may help individuals expand their awareness and foster a more balanced, harmonious mind–body state, to more effectively deal with life’s challenges, such as cancer. MBB also addresses what might underpin resistances to clarity by proposing a construct termed the “Identity System” or “I-System” in MBB teaching language. When the I-System gets activated (usually triggered by requirements) it generates a mind–body state that enhances self-centeredness and negative mental states, which can impede healthy functioning. Identifying when the I-System becomes activated may assist individuals in addressing and working to defuse their requirements, leading to a more harmonious outlook on life, and a better health status. MBB techniques are easy to learn and benefits may accrue rapidly. MBB was conducted by a licensed clinical social worker with MBB certification.
Because MBB provides dynamic instructions to help individuals develop greater awareness of their mental states and bodily sensations, some people may be tempted to think that MBB may be similar to biofeedback. However, biofeedback generally includes primarily electronic sensing devices to provide feedback information about various physiological signals, including brainwaves, muscle tone, heart rate, and pain, to assist in improving many different health and stress conditions, such as chronic pain, cardiac arrhythmias, hypertension, and anxiety. 67 Since biofeedback may be combined with interventions such cognitive behavioral therapy, relaxation therapy, guided imagery, and psychological education, 68 mind–body interventions such as MBB may be used in conjunction with biofeedback therapy to potentially enhance its efficacy.
Adherence to Programs
Participants in all groups were asked to practice the techniques they had learned and read the information provided on a daily basis. There was no time length specified for any of the groups to engage in home practice; nor was home practice standardized such that groups did not receive equal amounts of home practice. The practices that each group was encouraged to use at home are as follows: The SHE group was asked to review sleep topics that were provided to them in the form of handouts (indicated previously) and to implement what they had learned during the SHE sessions both prior to and at bedtime. The MM group was encouraged to practice formal meditation techniques (such as the body scan and sitting and walking meditation) several times per week using the CDs to guide their meditation practice. Participants were also asked to practice moment-to-moment breath awareness throughout the day (eg, while at a stop light, while on hold on the phone, when waiting in line, or during similar idle times). They were also encouraged, but not expected, to read pertinent sections of the 2 books included in the course. The MBB group was asked to review the MBB concepts they had learned and keep referring to the handout they had received and practice the experiential exercises (listening and paying attention to sounds, feelings, sensations, etc) and mind–body mapping exercises during the day and in the evening before bedtime. Participants in each of the groups were not required to journal what they did, nor were they required to document how much time they spent on the various activities. In lieu of a journal, during sessions 2 and 3, participants in each group were asked to share what they had done each week to help improve their sleep and in their daily lives.
Outcome Measures
Salivary Oxytocin
Saliva collection
Participants were instructed to collect saliva prior to bed time (approximately10
Salivary OT assay
The sOT enzyme-immunoabsorbance (EIA) method used to assay salivary OT in the present study was identical to that reported previously. 46 Prior to conducting the OT assay, an extraction stage was included. Since there is some controversy about the accuracy of OT measurement in saliva due to concerns about the validity of OT assays of saliva samples, sample extraction is a recommended minimally necessary procedure for measuring both plasma and salivary OT.71,72 Extraction gets rid of other molecules that could potentially interfere with OT measurement, and it additionally concentrates the sample (which is generally low) to ensure that OT concentrations are greater than the assay sensitivity level and remain in a more measurable assay range.69,72 Another problem with not conducting an extraction procedure is that unextracted OT concentrations are more than 2 orders of magnitude higher than extracted OT, in radioimmunoassays.46,69 While extraction removes other molecules, the accuracy of OT measurement could be affected by OT degradation products, as well as nonspecific reactants that are immunoreactive and could contribute to final OT measurements; this applies to plasma OT as well as salivary and urinary OT, and as such, it is imperative to conduct appropriate validations for all types of samples. 72 Some researchers even believe that saliva might not contain bioavailable OT. 73 Thus, caution is recommended since not enough research has been conducted to fully and satisfactorily characterize OT measurement in human body fluids, especially saliva, which is of great necessity in establishing the true function of OT found in peripheral tissues. 72
Salivary OT levels were measured using the OT EIA (Enzo Life Sciences, Farmingdale, NY), in which the endogenous OT hormone competes for the OT antibody binding sites with added OT linked to alkaline phosphatase. After the overnight incubation at 41°C, the excess reagents were washed away and the bound OT phosphatase was incubated with substrate. After 1 hour, this enzyme reaction (which generates a yellow color) was stopped and the optical density (OD) was read on a Sunrise plate reader (Tecan, Research Triangle Park, NC) at 405 nm. The intensity of the color is inversely proportional to the concentration of OT in the sample. The hormone content (pg/mL) was determined by plotting the OD of each sample against a standard curve. After correcting for concentration produced by extraction, the lower limit of sensitivity was 1.5 pg/mL. The intra- and interassay variations for this assay were 4.8% and 8%, respectively, determined using a set control sample with known OT concentration on each plate and in each run. Enzo Life Sciences reports cross-reactivity for similar mammalian neuropeptides in sera at less than 0.001%.
Self-Report Measures
Sleep
Sleep was measured by the MOS-SS 62 , a validated 12-item scale evaluating sleep patterns over the past week and incorporating 6 subscales: (a) sleep disturbance, (b) sleep adequacy, (c) daytime somnolence, (d) snoring, (e) waking up short of breath with a headache, and (f) quantity of sleep. Two additional subscales evaluate composite sleep problems, namely, Sleep Problems Indexes I and II (SPI-I and SPI-II). SPI-II is a composite score reflecting sleep disturbance, sleep adequacy, and somnolence, which was used as both the eligibility inclusion measure and primary outcome for the self-reported measures. Internal consistency for the current sample based on Cronbach’s α coefficient was .69.
Stress
The Perceived Stress Scale (PSS)74,75 measures the extent to which individuals perceive their lives to be unpredictable, uncontrollable, or overloaded. We used the 10-item version, which has maximum reliability. Internal consistency for the current sample based on Cronbach’s α coefficient was .93.
Depression
The Center for Center for Epidemiological Studies–Depression Scale (CES-D) 76 comprises 20 items and is one of the most common screening tests for the presence of depressive symptoms. Internal consistency for the current sample based on Cronbach’s α coefficient was .93.
Quality of life
The Functional Assessment of Cancer Therapy–General (FACT-G) 77 is a 27-item cancer-related QOL measure, which is divided into 4 primary QOL domains: Physical Well-Being, Social/Family Well-Being, Emotional Well-Being, and Functional Well-Being. It is appropriate for use with patients with any form of cancer, and it has been used to evaluate cancer-related QOL in many studies.78-82 Internal consistency for the current sample based on Cronbach’s α coefficient was .92.
Well-being
The World Health Organization Well-Being Index (WBI) 83 is a 5-item index covering positive and negative aspects of emotional functioning. Internal consistency for the current sample based on Cronbach’s α coefficient was .90.
Mindfulness
The Five-Facet Mindfulness Questionnaire (FFMQ) 84 includes 39 items and assesses 5 distinct, interpretable facets of mindfulness: (a) observing, (b) describing, (c) acting with awareness, (d) nonjudging of inner experience, and (e) nonreactivity to inner experience. We evaluated the effects of the interventions on mindfulness using the total mindfulness score. Internal consistency for the current sample based on Cronbach’s α coefficient was .93.
Self-compassion
The Self-Compassion Scale (SCS) 85 is a 26-item used to measure self-compassion, an emotionally positive attitude thought to protect against the negative consequences of self-judgment, isolation, and rumination. The total self-compassion score was computed and used as the raw data. Internal consistency for the current sample based on Cronbach’s α coefficient was .96.
Participants completed these self-reported outcome measures at approximately the same 3 collection time points (Pre, Post, and Follow-up) as the saliva samples.
Statistical Analysis
All data analyses were conducted with SPSS software, Version 18.0 (IBM, Chicago, IL).
Baseline sOT levels were initially evaluated to determine if there were any differences in sOT as an effect of sex, using a t test. We also evaluated whether baseline sOT levels varied as a function of (a) age and (b) baseline self-reported outcome measures, including sleep problems index, depression, perceived stress, well-being, FACT-G, mindfulness, and self-compassion, using correlation analysis (Spearman’s ρ). We additionally determined intra-individual reliability of sOT levels over the course of the study (Pre, Post, and Follow-up) using correlation analysis (Spearman’s ρ).
Salivary Oxytocin
The analysis evaluated the effects of the mind–body programs (MM, MBB) compared with that of SHE, on sOT levels at postintervention (comprising Post and Follow-up). The sOT data were not normally distributed and consequently were log-transformed (logOT) prior to analysis. We used a mixed effects model analysis of variance (ANOVA) to estimate intervention effects as the change in sOT at postintervention (subtracted from baseline) for each mind–body intervention versus SHE. We additionally evaluated sOT change from baseline within each of the mind–body interventions and SHE independently. The mixed effects ANOVA specified a factorial design with Treatment and Period as fixed effects, and an unrestricted covariance matrix. The maximum likelihood estimates from the mixed model are “intent-to-treat,” retaining all observations with no imputation of missing values. In the present study, randomization produced significantly different baseline (Pre) distributions across groups (see Results). With smaller samples and baseline imbalance, some degree of regression artifact is inevitable when evaluating change. To minimize this impact, we also conducted comparable analysis of covariance (ANCOVA) analyses, adjusting for baseline observations. The estimated adjusted effect magnitudes were broadly similar to those from the change analyses, with only the MBB sample showing an increase in the adjusted mean log(sOT) from baseline.
Sleep and Other Self-Report Outcome Measures
The analyses determined the effects of the mind–body programs (MM, MBB) compared with that of SHE at postassessment and follow-up, for sleep (MOS-SS: SPI-II), perceived stress (PSS), depression (CES-D), well-being (WBI), QOL (FACT-G), mindfulness (FFMQ), and self-compassion (SCS), in the subset of cancer survivors from the main study, 61 who provided saliva samples for sOT evaluation. Statistical analyses were mixed effects model ANOVAs, and intervention effects were estimated as each outcome measure’s change subtracted from baseline for each mind–body intervention versus SHE. Additional analysis examined change in outcome measure within each mind–body intervention and SHE, independently. The mixed effects ANOVAs used a factorial design with Treatment and Period as fixed effects, and an unrestricted covariance matrix. The maximum likelihood estimates from the mixed model are “intent-to-treat,” retaining all observations with no imputation of missing values.
Results
Demographics and Clinical Characteristics
Table 1 presents age, the number of subjects identified by sex, and clinical characteristics in this subset of cancer survivors evaluated for sOT. Groups were fairly well balanced and did not differ substantially in age and sex, although there were some differences in clinical characteristics, such as fewer breast cancer survivors in the MBB group (n = 2) than in either the SHE (n = 5) or MM (n = 7) group.
Baseline Demographics and Clinical Characteristics for Participants Sampled for sOT in Each Intervention Group.

Abbreviations: sOT, salivary oxytocin; SHE, sleep hygiene education; MBB, mind–body bridging; MM, mindfulness meditation; CNS, central nervous system.
Standard deviation in parentheses.
Type of cancer, including ovarian, endometrial, testicular, prostate, lung, melanoma, ependymona, leukemia, kidney, lymphomas (non-Hodgkin’s, CNS), skin carcinoma, brain, thyroid, peritoneal.
Baseline sOT Levels in Cancer Survivors
Mean sOT levels at baseline (Pre) in females (mean, 5.52; SD, 3.89, n = 21) were higher than those in males (4.37; 2.46, n = 9), but did not differ statistically (t test: t = .82, P = .42). Consequently, for the sOT analyses we pooled female and male sOT raw data.
Relationship Between Baseline sOT Levels and Age
The correlation between baseline sOT levels and age (29-74 years old) was not statistically significant (r = −.13; P = .485).
Relationship Between Baseline sOT Levels and Baseline Self-Reported Outcome Measures
Table 2 provides correlations between baseline sOT levels and baseline self-report measures. Salivary OT was not significantly correlated with any self-report measure. However, correlations between sOT and several of the self-report measures were in the predicted direction: a negative association of sOT with sleep and depression, and a positive association of sOT with QOL and well-being.
Relationships at Baseline Between Salivary Oxytocin Levels and Self-Reported Outcome Measures.
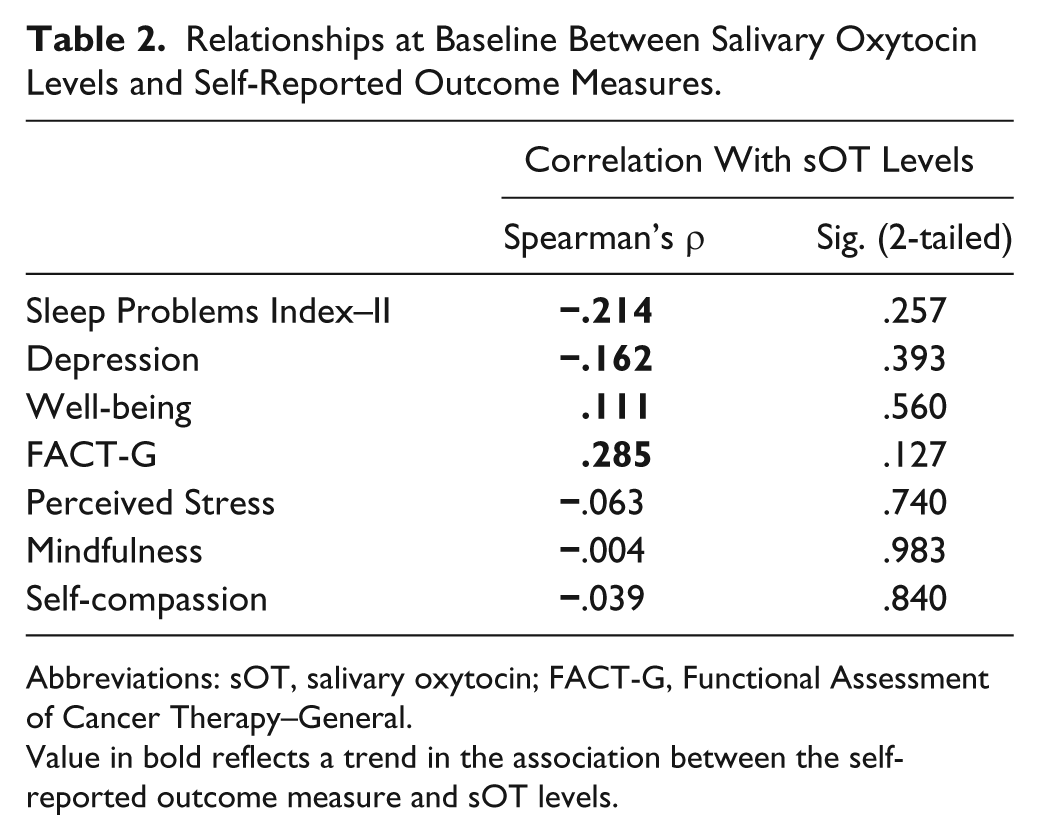
Abbreviations: sOT, salivary oxytocin; FACT-G, Functional Assessment of Cancer Therapy–General.
Value in bold reflects a trend in the association between the self-reported outcome measure and sOT levels.
Reliability of OT Measures
Salivary OT levels across the 3 assessments periods (Pre, Post, and Follow-up) were significantly correlated between Pre and Post (r = .61; P = .001) and Post versus Follow-up (r = .68; P = .001), while Pre versus Follow-up were moderately associated (r = .36; P = .092).
Intervention Effects on sOT
Table 3 displays raw mean sOT levels for each intervention across the 3 time points. At Pre (baseline), sOT levels varied significantly among the 3 treatment groups (one-way ANOVA: F = 7.05, P = .003), with higher sOT levels in the SHE group compared with those in MM and MBB. For this reason, we analyzed change from baseline sOT levels at postintervention (Post and Follow-up) to determine whether sOT levels differed in each mind–body intervention compared with that in SHE. Figure 1 presents change from baseline log-transformed sOT levels at Post and Follow-up for each of the 3 interventions and shows that sOT levels were significantly greater at postintervention in MBB compared with those in SHE (t = 2.05, P = .049), but they did not differ between SHE and MM (t = .53, P = .60). Cohen’s (d) effect size for the comparison between MBB and SHE was .82. (Cohen’s d was calculated by subtracting the change from baseline for Post and Follow-up sOT levels of MBB and SHE, divided by their pooled standard deviations.) This large effect size for Cohen’s d should be considered with caution, since it is based on sOT levels decreasing in SHE at Post and Follow-up, and sOT levels increasing in MBB at these time points. Thus, this finding should be further evaluated and replicated in a larger study designed to evaluate changes in sOT in cancer survivors.
Raw Means (and SDs) of Salivary Oxytocin Levels and the Self-Reported Outcome Measures Evaluated in This Study Across the 3 Interventions, at Baseline (Pre), Postintervention (Post), and Follow-up.
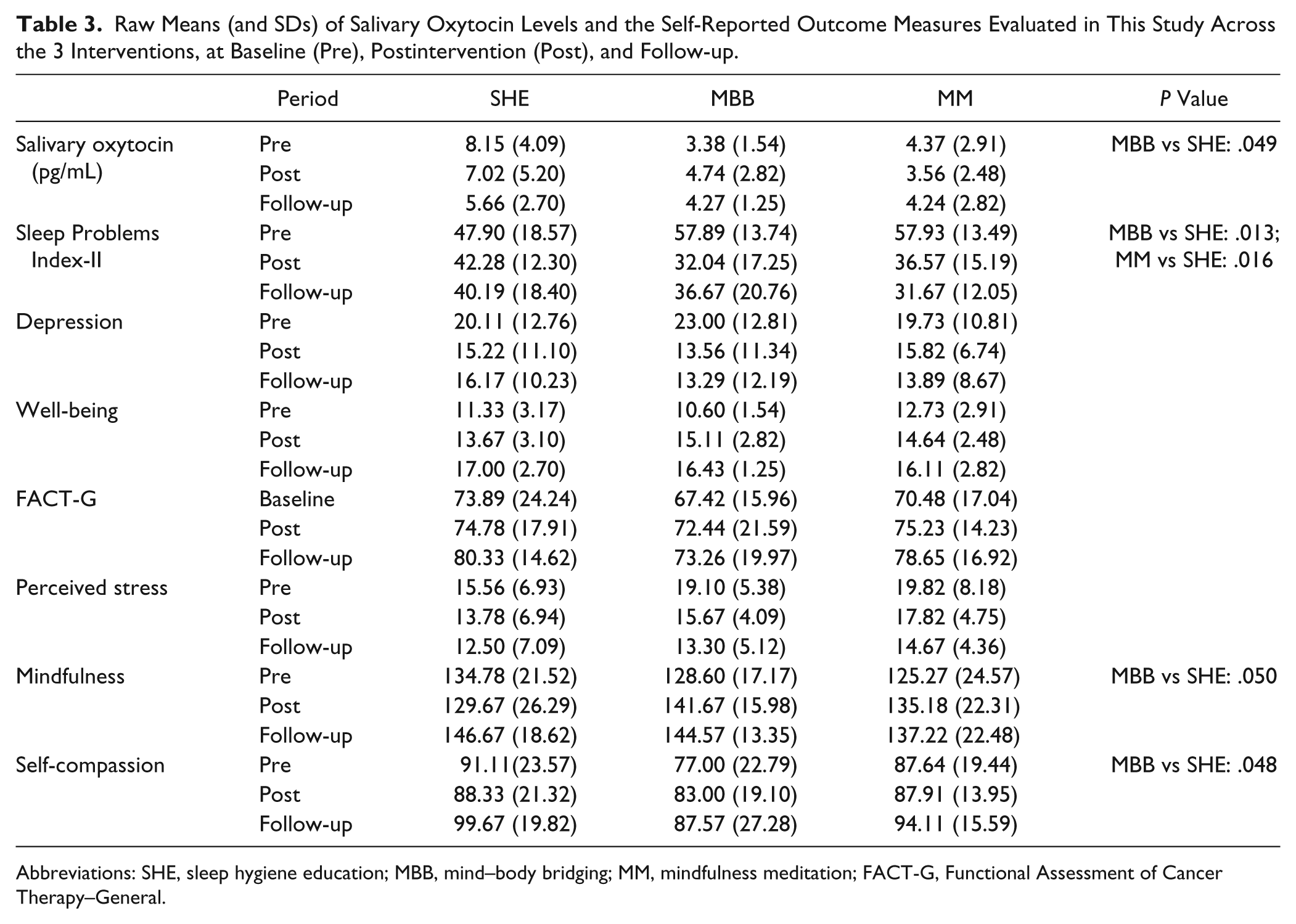
Abbreviations: SHE, sleep hygiene education; MBB, mind–body bridging; MM, mindfulness meditation; FACT-G, Functional Assessment of Cancer Therapy–General.

Comparisons among interventions (SHE, MBB, and MM) of mean (with SEM) change from baseline sOT levels at postintervention (Post) and 2 months later (Follow-up).
As seen in Figure 1, for within-group comparisons, sOT levels increased from baseline only in the MBB group (ie, changes from baseline sOT levels are positive) at postintervention (comprising Post and Follow-up), although these increases were not significant (t = 1.46, P = .156). In the other interventions, sOT levels in SHE showed a nonsignificant decline at postintervention (ie, change from baseline sOT levels was negative), while sOT levels in MM did not change significantly (SHE: t = 1.46, P = .158; MM: t = .85, P = .405).
Intervention Effects on Self-Reported Outcome Measures
For the subset of cancer survivors from the main study who provided saliva samples for sOT evaluation, we assessed the effects of the interventions on the various self-report measures. Table 3 presents raw mean scores for sleep (MOS-SS), depression (CES-D), quality of life (FACT-G), well-being (WBI), perceived stress (PSS), mindfulness (FFMQ), and self-compassion (SCS), for each intervention at Pre, Post, and Follow-up. Statistical analyses for each of the self-reported outcome measures evaluated in the present study are presented below.
For the sleep measure, the analysis revealed that SPI-II change scores at Post and Follow-up were significantly lower in MBB (t = 2.63, P = .013) and MM (t = 2.56, P = .016) compared with those in SHE, indicating greater improvements in sleep in the mind–body interventions than in the control group. Within-group analyses indicated that SPI-II scores were lower at Post and Follow-up compared with those at Pre, in MBB (t = 5.40, P < .001) and MM (t = 5.53, P < .001), but not in SHE (t = 1.49, P = .146), suggesting that sleep improved to a greater extent in the MM and MBB groups, but not in SHE.
For the other self-reported outcome measures, the statistical analyses revealed that changes from baseline scores at Post and Follow-up in MBB were greater compared with those in SHE, for mindfulness (FFMQ; t = 2.02, P = .050) and self-compassion (SCS; t = 2.07, P = .048).
Based on the CESD scale, self-reported depression decreased in MBB more so than SHE, but the difference between the 2 groups (t = 1.88, P = .072) did not reach significance. As indicated in Table 3, CESD scores were fairly high at baseline and above the cutoff of 16, indicative of being at risk for clinical depression. 76 Specifically, the raw data indicate that in each of the 3 groups approximately two thirds (SHE, 6/9 = 67%; MBB, 6/10 = 60%; MM, 8/11 = 73%) of participants were above the cutoff at baseline.
Statistical analyses of the other outcomes measures, including perceived stress, FACT-G, and well-being, did not differ for the 2 mind–body therapies compared with that of SHE at Post and Follow-up.
Discussion
In this exploratory study of a subset analysis of cancer survivors with self-reported sleep disturbance investigated previously in the main study, 61 we evaluated the feasibility and acceptability of measuring sOT, as well as the influences of sleep-focused mind–body interventions, MBB and MM, on sOT levels. We also investigated sOT as a potential biological marker of improved QOL and well-being in cancer survivors. We found that within-individual sOT reliability was high for comparisons between baseline and Post, and Post and Follow-up, and moderate between baseline and Follow-up. Furthermore, baseline sOT levels did not differ between females and males and were not correlated with age. While correlations between sOT and self-report measures were weak, several of the associations were in the predicted direction, namely, sOT was negatively associated with sleep and depression and positively associated with QOL and well-being. Baseline subtracted sOT levels at Post and Follow-up in MBB participants were significantly greater than those in the SHE control. In these cancer survivors who provided saliva samples for sOT measurement, sleep problems change scores decreased at Post and Follow-up in MBB and MM compared with those in SHE, while significant increases in mindfulness and self-compassion at Post and Follow-up were observed in the MBB group compared with those in the SHE group, indicating that in this subset group, results were similar to that of the main study. 61 The findings in this exploratory study suggest that sOT could be a reliable biological measure over time, and thus may be useful in future studies examining the effects of mind–body interventions on health outcomes in cancer survivors. However, a more strongly powered study is required to conclusively determine whether mind–body interventions may influence changes in sOT levels in cancer survivors.
In the present study, we observed that within-individual sOT levels in cancer survivors were fairly consistent across the 3 months of data collection (from baseline to the 2-month follow-up assessment), indicating reliability of sOT levels over time. While there are no other studies conducted on salivary OT to compare with the current study, plasma OT concentrations are highly stable within individuals when sampled over a 6-month period. 86 This intra-individual reliability of both plasma OT and sOT levels may be important when assessing possible associations between the endogenous OT system and various health-related states, including well-being and QOL. This type of assessment would necessarily require more frequent sampling periods for OT measurement, hence the benefits of sampling OT from saliva.
At baseline, while sOT and self-report measures were weakly correlated in a number of self-report measures, the correlations went in the predicted direction: sOT was positively associated with well-being and QOL and negatively associated with sleep disturbance and depression. Other studies have similarly failed to identify compelling links between biological measures and psychological outcome measures (see Carlson et al 87 ). This lack of correlation between physiological and psychological measures suggests that more effort is needed in designing studies that can capture the complexities and potential variability in both types of measures. One approach is concurrent and repeated collection time points and identifying appropriate self-report measures that are indicative of state effects.
To our knowledge, the present study is the first to examine the influence of mind–body interventions on sOT levels in cancer survivors. Previous studies examining the potential role of endogenous OT in health and well-being and its associations with positive health states are few, and they have been confined to tactile interventions such as gentle or warm touch46,88 and massage therapy.37,44,45,47,48 Thus, while more work is necessary to fill the gaps in the area of mind–body interventions and their relationships with OT, results of these studies could provide an important understanding of potential OT mechanisms that are mediated by mind–body interventions in improving cancer survivors’ health outcomes, including sleep.
There appears to be a lack of studies investigating salivary or plasma OT levels in cancer patients at different stages of cancer and treatment, or in cancer survivors, and as related to cancer prognosis. In this regard, the relationship between OT and cancer could be an important research avenue, since understanding the role that OT plays in cancer progression and survivorship might provide important information promoting the incorporation of OT as a screening tool to obtain a more comprehensive understanding of a cancer patient or survivor’s health status. Furthermore, OT could serve as a potentially important biomarker in assessing various aspects of a cancer patient’s QOL and well-being to help better understand how OT might enhance cancer prognosis.
As is the case in many endocrine studies in which substantial variability in hormone levels is often observed, large variations in sOT levels were also evident in this study, in which certain participants exhibited consistently higher sOT levels. In addition, large differences in sOT levels were seen at baseline, in which mean sOT levels were significantly higher in SHE compared to those in MBB and MM. While we could not ascertain what accounted for such divergent sOT levels, one factor may have been the different cancer diagnoses and treatments in this population, although our study excluded individuals with a current cancer diagnosis or having received treatment such as radiation, surgery, or chemotherapy within the past 3 months. It is also possible that differences in baseline sOT levels could be related to participants exhibiting different psychological states, for example, SHE comprising individuals with higher levels of perceived stress or depression than the other interventions. While there was a lack of significant correlations at baseline between sOT and the self-report measures across all individuals, the small size of each intervention group precluded identifying meaningful relationships between sOT levels and psychological variables within each group. As a further alternative, since OT is strongly implicated in prosocial behavior, sOT levels might have been influenced by participants’ living environment: whether they have a spouse or partner, reside with another person or live alone, and the type of social support provided to these cancer survivors. In a future study, these factors would need to be assessed to examine the influence of a person’s social environment on sOT levels.
Recent studies have demonstrated that OT may moderate the relationship between psychosocial indices and health outcomes. 32 Similarly, it would be interesting to determine if sOT in the current study could moderate the relationship between intervention effects on sleep and psychosocial states such as perceived stress and depression. Unfortunately, sample sizes within interventions were too small to conduct this type of analysis.
One of the limitations of this study was that only one saliva sample was collected at each time point. As has been generally suggested for measuring salivary hormones, it would be more advantageous to collect 2 to 3 saliva samples over at least 2 consecutive days, to increase intra-individual reliability of sOT measures, as has been suggested for cortisol. 89 Also, it is important to ensure that collection of saliva samples and self-report measures are collected as close to each other as possible. Another concern is the issue of recall for the self-report measures. For example, participants collected saliva samples in the evening before going to bed, and the sleep questionnaire ascertained sleep performance over the previous week. A better strategy would have been to collect saliva samples around the same time that a sleep diary was completed for the previous night’s sleep. Thus, having 2 to 3 saliva samples and concomitant sleep diary entries at each time point would have made it possible to collect sufficiently rich and informative data on complex relationships between this biomarker and other relevant variables.
Other limitations included that each group was not provided with an explicit task of documenting how long they practiced their respective intervention’s techniques, nor was the amount of practice among the 3 groups standardized for them to engage in approximately equal amounts of home practice. One limitation concerning saliva collection was that we did not measure participant adherence to the saliva collection protocol.
Assays evaluating salivary OT levels have been questioned for their reliability,71,72 since it has been shown that sOT assays correlate weakly with EIA-based estimates of OT in unextracted plasma, with low shared variance between salivary and plasma measures (between 17% and 35%).13,47,69 For this reason, we included an extraction technique, which has demonstrated a better validation profile. 69 The case for measuring salivary OT is compelling given some of the advantages of collecting saliva samples. Under certain circumstances, sOT may be the only possible measure that can be obtained, for example, when participants do not wish to have their blood drawn, or when the ability to collect blood is impractical, such as in the home. In addition, setting up and collecting blood draws in group intervention studies can be a laborious endeavor. The strengths and weaknesses of the sOT sampling method are not different than for other commonly measured and validated biomarkers such as salivary cortisol. 69 In support of salivary OT as a potentially valid physiological measure, intranasal OT studies have demonstrated an association between increases in sOT and behavioral and neural changes. 90 More research is necessary to further validate sOT and characterize sOT levels and patterns of release.
We acknowledge that the finding of significant differences between MBB and SHE in change from baseline sOT levels at Post and Follow-up should be considered preliminary and may be due in part to initial baseline differences among the groups, in which SHE started out with higher sOT levels than either those in MBB or MM. Small sample sizes are particularly susceptible to baseline imbalance. Thus, we cannot conclusively state that the differences in sOT levels between the 2 groups were due to intervention effects. Future studies examining the effects of mind–body interventions on sOT levels should include larger sample sizes to more strongly power the study for these analyses. A larger sample size would also reduce the likelihood of baseline imbalance of sOT levels among groups.
In conclusion, while this exploratory study has a number of limitations, it suggests that sOT may be a reliable biological measure over time and that it may be useful in evaluating the effects of mind–body interventions in cancer survivors. Finally, one of the goals of this study was to determine an effect size mediated by mind–body interventions for designing a more definitive randomized controlled trial, to better understand the role of OT in facilitating health and well-being in cancer survivors.
Footnotes
Acknowledgements
The authors would like to thank Cheryl Walker and Chihiro Christmas at UNC for processing the saliva samples and conducting the assays. We would also like to thank Richard Landward, LCSW, for developing and refining a brief Mind–Body Bridging program based on an earlier study, and the clinicians who served as the instructors for the intervention programs investigated in the study: Richard Landward, LCSW (Mind-Body Bridging), Peggy Hunter, LCSW (Mindfulness Meditation), and Katie Porter, LCSW (Sleep Hygiene Education). The authors would also like to thank Dr Saundra Buys for initial consultation about the present study. We are grateful to Dr Kathleen Light for providing consultation on OT measures and reviewing this manuscript. Last, the authors would like to express deep appreciation for the effort and time devoted by the cancer survivors who participated in the study.
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of Mind and Life Institute or National Institutes of Health, the funding agencies. Mind and Life Institute and National Institutes of Health had no role in the conduct of the study, collection, management, analysis and interpretation of the data and preparation, review or approval of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study reported was supported by Mind and Life Institute Varela Award (2009-01-009) to DLL and the National Institutes of Health (NIH) Award R21 AT002209 to YN.