
Abstract
Background. Health care policies and guidelines that are clear and consistent with research evidence are important for maximizing clinical outcomes. To determine whether cancer centers in Canada and the United States had policies and/or guidelines about antioxidant use, and whether policies were aligned with the evidence base, we reviewed current research evidence in the field, and we undertook a survey of the policies and guidelines on antioxidant use at cancer institutions across North America. Methods. A survey of policies and guidelines on antioxidant use and the development and communication of the policies and guidelines was conducted by contacting cancer institutions in North America. We also conducted a Website search for each institution to explore any online resources. Results. Policies and guidelines on antioxidant use were collected from 78 cancer institutions. Few cancer institutions had policies (5%) but most provided guidelines (69%). Antioxidants from diet were generally encouraged at cancer institutions, consistent with the current research evidence. In contrast, specific antioxidant supplements were generally not recommended at cancer institutions. Policies and guidelines were developed using evidence-based methods (53%), by consulting another source (35%), or through discussions/conference (26%), and communicated mainly through online resources (65%) or written handouts (42%). For cancer institutions that had no policy or guideline on antioxidants, lack of information and lack of time were the most frequently cited reasons. Conclusions. Policies and guidelines on antioxidants from diet were largely consistent with the research evidence. Policies and guidelines on antioxidant supplements during treatment were generally more restrictive than the research evidence might suggest, perhaps due to the specificity of results and the inability to generalize findings across antioxidants, adding to the complexity of their optimal and safe use. Improved communication of comprehensive research evidence to cancer institutions may aid in the development of more evidence-based policies and guidelines.
Introduction
There is growing interest in the use of antioxidants for reducing cancer risk and improving cancer treatment outcomes. Oxidation is a process whereby reactive free radicals with unpaired valence electrons formed by factors such as ultraviolet rays, carcinogens, conventional cancer treatments (chemotherapy and radiotherapy), and natural metabolic processes take electrons from other molecules, destabilize the molecules, and cause damage to DNA, proteins, and cells. 1 Antioxidants are molecules that neutralize or inhibit the formation of free radicals, thereby preventing or repairing oxidative damage to cells. 2 Excessive amounts of free radicals are thought to be one of the underlying causes of many diseases, including cancer.1,3 Recent laboratory and animal research suggests that some exogenous antioxidants can help prevent the free radical damage associated with the development of cancer as well as protect normal cells from being damaged by oxidative stress, helping lower cancer risk and reduce treatment toxicities from chemotherapy and radiotherapy.4,5
While the behavior in vitro of some antioxidants may be relatively well understood, the physiological function of antioxidants in the body and in the clinical context of disease and treatment is much more complex, and affected by many characteristics of the host, making it difficult to generalize effects both across types of antioxidants and across individuals. 6 Additionally, the group of chemicals that are included under the label of “antioxidants” are structurally quite varied, and researchers argue against lumping them together in one category, likening them to distinct drugs that should not be treated as a homogeneous group.6,7 Many are biologically active and have effects in cells that are independent of their antioxidant properties. This differentiation makes it difficult to generate overall statements or conclusions about the effects of antioxidants in general on health, as literature is available in varying degrees for different substances. 7
As a result of the controversy over the use of antioxidants for cancer prevention and treatment, and the lack of conclusive research evidence, the use of antioxidants for cancer prevention or treatment is not considered mainstream clinical practice but rather a form of complementary medicine. 8 Antioxidants are one of the most common types of complementary therapies used and discussed by cancer patients,8,9 with 64% to 81% of cancer patients and cancer survivors in the United States reporting that they use vitamin or mineral supplements compared with 50% in the general population. 10 Unfortunately, few patients are educated on which modalities are safe and effective and which may cause harm, resulting in poor communication between patients and providers around these issues.8,11-17
Surveys with cancer patients have shown that patients who use complementary therapies often report high levels of anxiety due to conflicting information on their efficacy. 18 While most patients indicate that they prefer to obtain information on complementary therapy use from their oncology physician at a conventional cancer center, 17 most patients using these therapies reportedly do not obtain information from their treating health care providers.14,17 Furthermore, most discussions on natural health products are not initiated by oncologists, 8 with 40% to 77% of complementary therapy–using patients stating they do not discuss their use with their physicians. 16 In fact, many oncologists may be unaware of the available resources and evidence on complementary therapies and lack training. 12 Therefore, having guidelines or policies that summarize the best evidence available to health care practitioners may help them better communicate knowledge on antioxidants to cancer patients.
Our objective was to evaluate policies and guidelines from cancer centers in Canada and the United States to see if they were in alignment with the research evidence on the use of antioxidants for cancer prevention and treatment. This required first assessing the general consensus in the scientific literature on these effects by surveying existing literature reviews and treatment recommendations2,6,7,19-25 and meta-analyses,26,27 which addressed the effects of antioxidant supplements (oral, intravenous, subcutaneous, etc) on cancer treatment outcomes and cancer risk, as well as relevant original research studies.
First in terms of cancer risk, key and consistent findings on antioxidants and cancer prevention centered on dietary intake: diets high in antioxidants such as fruits and vegetables with high levels of β-carotene and vitamins A, C, and E and high baseline serum levels of various antioxidants were associated with lower risk of various cancers, such as cancers of the lung, colon, breast, and stomach for both smokers and nonsmokers.4,22,28-31
In contrast, studies investigating the effects of antioxidant supplements (vs diet) on cancer risk found mixed results and remains controversial. A number of randomized chemoprevention studies in both the general population and high-risk subgroups indicated that antioxidant supplements including vitamin C, vitamin E, β-carotene, and selenium lowered the risk of various cancers such as gastric, prostate, lung, and colorectal cancers.32-36 However, several other high-profile trials found contradictory results. One of these, the ATBC trial from Finland, randomly assigned almost 30 000 male smokers to either β-carotene, vitamin E, both supplements, or placebo, unexpectedly finding increased lung cancer risk and overall mortality in the β-carotene group only. 31 A similar smaller trial found that the combination of vitamin E and β-carotene supplements for smokers and men exposed to occupational asbestos also increased lung cancer risk and mortality. 37 The most recent highly publicized chemoprevention trial aimed to reduce prostate cancer risk using either vitamin E or selenium supplements either alone or in combination, compared to placebo (the SELECT trial), but found increased risk of prostate cancer in the vitamin E arm.38,39 Further analysis of interactions with baseline levels of selenium in toenail samples showed that selenium supplementation increased the risk of prostate cancer in men who already had high baseline levels, while vitamin E supplementation increased risk for those with low baseline selenium, leading to recommendations that men avoid both at supplemental levels beyond recommended dietary allowances. 40
To add to the complexity, Meyer et al found in a randomized controlled chemoprevention trial that supplementation with vitamin C, vitamin E, β-carotene, selenium, and zinc reduced the risk of prostate cancer for men with normal baseline prostate-specific antigen but nonsignificantly increased the risk of prostate cancer for men with elevated prostate-specific antigen levels. 41 Two other prospective randomized trial studies found no effect of β-carotene supplements on cancer risk, even though one included more than 22 000 participants.42,43 Hence, the use of these supplements, particularly in doses beyond recommended dietary allowances, may be contraindicated in many circumstances.
Turning to the use of antioxidant supplements during anticancer treatments of chemotherapy and radiation therapy, this remains the most controversial area in clinical practice.2,6,7,20,24 Studies in this area are generally small and there are not many double-blind randomized controlled trials (RCTs). Despite that, some double-blind RCTs, a large number of other RCTs and uncontrolled studies, and one meta-analysis on the effects of antioxidant supplements on cancer treatment outcomes indicated that administration of a range of supplements such as glutathione, selenium, N-acetylcysteine, melatonin, amifostine, coenzyme Q10 (CoQ10), vitamin A, vitamin C, and vitamin E via various routes (eg, oral, intravenous, subcutaneous, intramuscular) in conjunction with various chemotherapy and radiotherapy regimens could decrease treatment toxicities and increase treatment tolerance, tumor response rate, quality of life, and survival for patients with various different cancers.20,23,27,44-73 For example, in a randomized double-blind placebo-controlled trial, intravenous and intramuscular injections of reduced glutathione (GSH) given to advanced gastric cancer patients being treated with cisplatin-based chemotherapy regimens significantly reduced neurotoxicity, hemotransfusion requirements, and treatment delays; response rate was 76% in the GSH-infused patients and 52% in the control patients, and median survival was 14 months in the GSH arm and 10 months in the control arm. 60 While these findings are encouraging, they cannot be generalized beyond the specific study circumstances including the study population and antioxidant(s) used, as mechanisms of action for the various substances may be different, are not always well known, and likely interact with many individual characteristics of the host.
Other studies found that antioxidant supplements given to cancer patients with or without other active agents could have both beneficial and harmful effects.74-88 For example, combination of oral α-tocopherol, an antioxidant used in clinical practice, and oral pentoxifylline, a purinergic agonist, given to lung cancer patients undergoing radiotherapy reduced radiation-induced lung toxicity and increased overall survival and progression-free survival but caused pentoxifylline-related nausea and vomiting in some patients. 84 , 85 Harmful effects typically involved the experience of side effects but did not negatively affect tumor response or survival.
Adding to the uncertainty, a number of studies indicated that antioxidant supplements during treatment were associated with adverse effects,89-96 such as mild to moderate gastrointestinal upset, nausea, and emesis, but most did not affect treatment efficacy or survival.89-91,96 However, importantly one well-publicized clinical trial found that oral α-tocopherol (vitamin E) and β-carotene supplements reduced cancer-free survival and increased all-cause mortality for head and neck cancer patients undergoing radiation therapy.92-94 Further analysis of this trial found that there was a significant adverse interaction between cigarette smoking and supplementation with α-tocopherol and β-carotene during radiation therapy for this patient group, which increased head and neck cancer recurrence, cause-specific mortality, and all-cause mortality. 95 Clinically, evidence of harm generally carries significant weight in making treatment recommendations, and hence clinicians may be prone to generalize serious negative outcomes such as this to other clinical scenarios, resulting in an overall conservative approach to using antioxidants in the treatment environment. Despite this finding cautioning against the use of vitamin E supplementation during radiation therapy for head and neck cancer patients, several other randomized controlled trials support its use for decreasing toxicities and side effects such as carboplatin-induced neuropathy, radiation-induced mucositis, and fibrosis. 24
Finally, other studies and one meta-analysis found no effect of antioxidant supplements on toxicities or treatment outcomes, either in a beneficial or harmful direction.26,97-107
Overall, because of contradictory findings and differential publicity often given in the media to studies that show harm, 24 the medical community may be receiving mixed messages on the potential value versus harm of various antioxidants that are not in alignment with the overall consensus in the scientific literature. Our study addresses the issue of what kind of advice health care providers are giving to patients regarding antioxidant use. There has been no previous research investigating policies and guidelines on antioxidant use at cancer institutions and how they were developed. In response, we explored current policies and guidelines on antioxidant use for cancer prevention, treatment, and survivorship at cancer institutions across North America to determine whether they were consistent with the prevailing research results, and provide insight into the process of guideline development.
Methods
This study involved implementation of a structured survey of formal policies and informal recommendations on antioxidant use at cancer-related institutions in North America (Canada and the United States). For the purposes of this study, policies were defined as “formal instructions prescribing patients to use or not use antioxidants during active cancer treatment or after completion of cancer treatment.” Guidelines were defined as “informal recommendations regarding antioxidant use for cancer prevention, treatment, or survivorship provided to cancer patients or the general public.” This study was approved by the Conjoint Health Research Ethics Board of the University of Calgary.
Recruitment
We approached a sample of cancer centers in North America, including all providers in Canada and a subset from the United States, that were considered most likely to address the issue of antioxidant use in cancer. Participating cancer centers were defined as institutions that provide treatment or information specific to cancer, whereas cancer institutions were defined as cancer centers and umbrella health care institutions that provide treatment or information on cancer, but are not necessarily specific to cancer. Overall, we developed a list of 40 designated cancer centers in Canada (as identified by the Canadian Organization of Medical Physicists [COMP]) 108 and 68 National Cancer Institute (NCI) cancer centers in the United States (as identified from the NCI Web site). 109 In addition, all hospitals run by the Cancer Treatment Centers of America (CTCA) were contacted. 110 Umbrella health care institutions, cancer information centers, and Canadian cancer centers not listed on the COMP Web site were also identified by word of mouth or online references on the Web sites of other identified cancer institutions. Overall, a total of 129 cancer institutions (50 in Canada, 79 in the United States) were targeted (Table 1).
Alphabetical List of Cancer Institutions in North America Identified for the Study. a

Asterisk (*) indicates cancer institution from which relevant information was obtained.
Survey
The survey included closed-ended and open-ended questions pertaining to information on current policies and guidelines on antioxidant use at the institution and how they were developed and disseminated. The survey is provided in as online Appendix A (http://ict.sagepub.com/content/by/supplemental-data). In the introductory letter or phone call, the following description was used—no other definition of antioxidants was given.
Antioxidants are molecules that inhibit the formation of free radicals or repair cells damaged by oxidative stress and can protect normal cells from being damaged by chemotherapy and radiation therapy. However, there is concern that antioxidants may also protect cancer cells and decrease treatment efficacy or cause adverse treatment interactions. Although some studies support the benefits of using antioxidants such as glutathione, amifostine, melatonin, and vitamin E during cancer treatment, there is no consensus in the literature. The objective of this study is to gather the formal and informal policies and guidelines on antioxidant use during treatment and in general at cancer centers across Canada and the United States and find out how the policies and guidelines have been developed.
If participants had questions the research assistant gave other examples of dietary antioxidants frequently investigated in the literature.
Data Collection Procedures
The primary author contacted health care workers at the identified institutions by phone, email, or in-person visitation to invite participation in the study. Health care workers included (but were not limited to) dieticians, patient educators, pharmacists, nurses, physicians, integrative oncologists, general information staff, support services staff, front desk staff, public affairs staff, and clinical trials staff. The Web site for each institution identified for the study was also searched for online resources.
Potential participants were provided with detailed information and invited to complete the study questionnaire, which was made available in English and French. Participants consented to take part in the survey by responding to the questionnaire and declined by not responding. This study involved a staged approach toward institution contact. First, where possible individuals or departments were contacted by phone. If an individual or department was unreachable by phone, then information about the study was provided by email or visitation. Two reminders were sent to nonresponders. The data collection period lasted from November 2013 to March 2014.
The researcher also conducted an online Web site search for each institution identified for inclusion in the study to identify resources and relevant research being conducted concerning the use of antioxidants. Key search terms included “Nutrition,” “Cancer information,” and “Antioxidant.”
Our target sample size was not based on a formal sample size calculation; rather, we aimed to capture as many cancer centers as possible in Canada and a subset of cancer centers in the United States that represent a range of comprehensive cancer care centers across the country.
Data Analysis
Data obtained from the survey and the online search were manually entered into Excel databases. The institution was used as the unit of analysis. Descriptive statistics consisting of means and percentages were used to describe the data.
Results
We achieved an overall response rate of 45/129 institutions (35%; Canada, 32%; United States, 37%). A “response” was defined as a health care worker at an identified institution providing one or more of the following: (a) answers to some or all of the questions on antioxidant policies and guidelines from the questionnaire; (b) written policies, guidelines, or educational materials on antioxidant use at the institution (eg, handouts); or (c) links to relevant online resources. Information obtained by online research, without help from a health care worker at the institution, was not considered a “response.” The majority of responses were from the dietetic/nutrition department (n = 23, 51%), followed by general information (n = 13, 29%), patient education (n = 6, 13%), pharmacy (n = 3, 7%), and others (n = 6, 13%). Information relevant to the study such as policies, guidelines, educational materials, and journal articles on antioxidant use for cancer prevention, treatment, and survivorship were collected (from health care provider responses and from internet searches) from a total of 78/129 institutions (60% of identified institutions), 21 in Canada and 57 in the United States. Institutions with available data included 62 cancer treatment centers, 6 cancer information centers, 4 umbrella health care institutions, and 6 cancer research institutions. Of the 78 institutions from which survey data were obtained, 38 provided information by answering questions from the questionnaire (49%), 10 provided written handouts (13%), and for 51 online resources were available on their Web sites (65%; Table 2). Of the 38 institutions that answered questions from the questionnaire, 27 did so by phone (71%), 11 by email (29%), and 1 in person (3%).
Type of Information Provided by Cancer Institutions. a

Total refers to the number of institutions from which information was obtained. Because an institution may have provided more than one type of information, numbers in individual cells may not add up to row totals.
Existing Policies/Recommendations
The current recommendations on antioxidant use for cancer prevention, treatment, and survivorship in Canada and the United States are summarized in Table 3. Of the 78 institutions from which information was obtained, 4 had policies on antioxidant use for cancer (5%), 54 had guidelines (69%), 10 had no policy or guideline (13%), and 10 provided online information on the effects of antioxidants on cancer but it could not be determined whether or not they had any policy or guideline (13%).
Number of Institutions That Recommended, Discouraged, Provided Mixed Recommendations (Recommending Some Antioxidants But Discouraging Others), or Were Neutral About Antioxidants From the Diet, Oral Supplements, or Physical Exercise for Cancer Prevention, Treatment, and Survivorship.
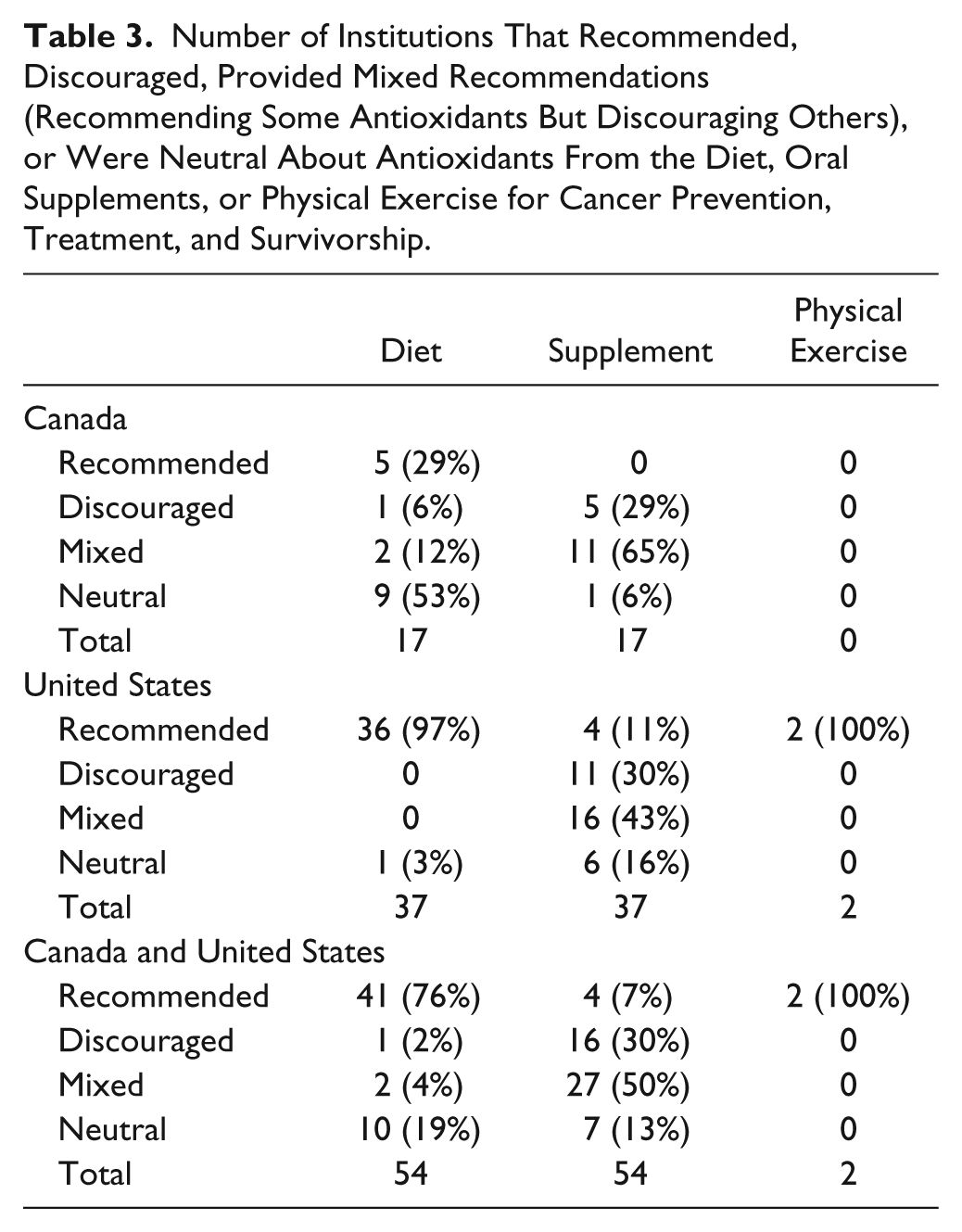
Information on antioxidant-rich diets for cancer prevention was gathered from 33 institutions. All 33 of the institutions recommended antioxidant-rich diets such as fruits and vegetables for cancer prevention (100%). Of the 23 institutions that provided information on antioxidant-rich diets during active treatment, 11 recommended the consumption of foods rich in antioxidants (48%), 1 discouraged it (4%), 2 provided mixed recommendations (eg, recommending fruits and vegetables high in antioxidant content but discouraging the consumption of green tea and phytoestrogen-rich foods; 9%), and 9 were neutral (eg, advising patients to consult their physicians; 39%). Whereas 100% of the institutions in the United States recommended consuming antioxidant-rich diets during cancer treatment, only 8% of the Canadian institutions recommended it, and most (69%) of the Canadian institutions were neutral. All 9 institutions that provided information on the consumption of antioxidant-rich foods for cancer survivors actively encouraged it (100%).
Of the 18 institutions that provided information on oral antioxidant supplement use for cancer prevention, 1 recommended it (6%), 10 discouraged it (56%), 6 were mixed (eg, stating that some supplements may increase cancer risk while others decrease risk; 33%), and 1 was neutral (6%). Of the 42 institutions that provided information on oral antioxidant supplement use during active treatment, 4 sites recommended it to increase treatment efficacy or decrease treatment side effects (10%), 9 discouraged it due to concerns about reduced treatment efficacy or adverse interactions (21%), 23 were mixed (55%), and 6 were neutral (eg, advising patients to consult their physicians; 14%). Of the 23 institutions that provided mixed recommendations on oral antioxidant supplement use during cancer treatment, 14 discouraged the use of single antioxidant supplements but allowed or encouraged the use of multivitamin supplements with small doses of various vitamins and minerals (33%), while the other 9 stated that some antioxidant supplements can be beneficial but others can be harmful and therefore patients should consult their physicians (21%). Of the 3 institutions that provided information on oral antioxidant supplement use for cancer survivors, 1 discouraged it (33%) and 2 were mixed (eg, stating that some antioxidant supplements decrease cancer recurrence but others increase cancer risk; 67%).
Two cancer centers provided information on antioxidants produced by physical exercise. Both centers recommended physical exercise to increase the production of antioxidants in the body to protect against cancer, but one of the centers suggested that too high intensity exercise may deplete the supply of antioxidants in the body and therefore recommended moderate to high intensity exercise but not exhaustive exercise.
Policy Development
A total of 34 cancer institutions provided information on how the policies or guidelines on antioxidants were developed. Of these, 18 sites used evidence-based methods such as consulting literature reviews and journal articles on the effects of antioxidants on cancer (53%), 9 used discussions or conference (26%), and 12 obtained policies or guidelines from another source such as another cancer center (35%).
Information on whether or not a specific committee was involved in the development of the policies or guidelines was provided by 16 institutions. Of these, 5/8 institutions in Canada and 7/8 institutions in the United States indicated that there was a designated committee for developing antioxidant policies or guidelines (75%). The committees were composed of dieticians or were interdisciplinary committees composed of various health care professionals such as dieticians, pharmacists, physicians, nurses, and patient educators.
Information on how the policies or guidelines were communicated to patients was available for 62 institutions. Of these, 26 provided written handouts to patients (42%), 7 used oral communication (11%), 2 gave presentations (3%), 1 used a library (2%), and 40 provided online resources such as Web pages or journal articles (65%). Written handouts were the most frequently used mode of communication at cancer institutions in Canada (87%), whereas online resources were the most frequently used mode of communication at cancer institutions in the United States (77%).
Reasons for Lack of Policies or Guidelines on Antioxidants
Reasons for lack of policies or guidelines on antioxidant use for cancer were provided by 19 institutions. Of these, 8 indicated there was lack of information (42%), 8 indicated there was not enough time or it was not a top priority (42%), 5 indicated there was too much conflicting information or opinions (26%), 2 indicated lack of interest (11%), 1 indicated it was a new cancer center and still developing policies (5%), and 5 indicated they were basic research institutions and did not interact with patients or provide clinical recommendations (26%).
Discussion
This is the first study to systematically investigate whether cancer center policies on the use of antioxidants for prevention, treatment, or survivorship exist and are consistent with the evidence base on their efficacy in cancer care.
Results indicate that the majority of cancer institutions provided guidelines on antioxidant use for cancer prevention, treatment, or survivorship, but few of them had formal policies on antioxidant use. Lack of information and lack of time were the primary reasons given by cancer institutions that lacked policies or guidelines, indicating the need for a clear and comprehensive synthesis of the current research evidence on the effects of antioxidants in cancer.
Policies and guidelines on antioxidants from food for cancer prevention, treatment, and survivorship were generally consistent with the current body of research evidence. In line with research studies that found that diets high in antioxidants were associated with reduced cancer risk,4,22,28-31 all the cancer institutions in North America recommended antioxidant-rich foods for preventing cancer and for cancer survivors.
However, policies and guidelines on antioxidant-rich diets during treatment were more variable, which was not surprising given that no clinical study to date has investigated the effects of antioxidant-rich diets on cancer treatment outcomes. This study identified that more cancer institutions in the United States reported actively encouraging the consumption of antioxidant-rich foods during treatment than in Canada (100% vs 8% among centers with relevant guidelines), suggesting that cancer centers in the United States, in general, may place more emphasis on this than Canadian cancer centers, or be more up to date with the literature in this area. However, the observed difference might have been due to a selection bias, as all cancer centers in Canada were identified for inclusion in the study whereas only US cancer centers designated by major institutions such as the NCI Comprehensive Cancer Centers and CTCA were identified for inclusion.
All information on antioxidant supplements provided by cancer institutions focused on oral supplements although a large number of studies have explored the effects of non–orally administered antioxidant supplements during cancer treatment (eg, intravenous, subcutaneous, intramuscular). For cancer prevention, the majority (56%) of cancer institutions discouraged the use of antioxidant supplements for reducing cancer risk and only a minority (6%) of institutions encouraged it. This result is not surprising given the conflicting research findings on antioxidant supplement use for cancer prevention. For cancer patients undergoing active treatment, few cancer institutions (10%) encouraged the use of antioxidant supplements during treatment and 21% discouraged all antioxidant supplement use during treatment; remaining responses were mixed or neutral. This conflicts with some research evidence showing reduced toxicities and increased efficacy of chemotherapy and radiation therapy treatments for various cancers when combined with certain antioxidant supplements.20,23,27,44-73 In addition, no cancer institution recommended antioxidant supplements for cancer survivors. Although a few research findings suggest that pentoxifylline and vitamin E supplements may be helpful for reducing radiation-induced sequelae posttreatment111,112 and selenium supplements can reduce future cancer risk in cancer survivors, 36 there is a lack of concrete and generalizable research evidence indicating the benefits of antioxidant supplement use for cancer survivors.
Part of the problem in converting clinical trial results into policy and guidelines is that research is specific to benefits of certain supplements used in patients with a particular type of disease receiving one specific combination of medications. Hence, blanket guideline statements are difficult to make, and few institutions are likely willing to incorporate the complexity of these recommendations into guidelines or policies for fear of misleading patients and inadvertently causing harm. Indeed, ignoring this issue is likely to have negative consequences since patients are motivated to use antioxidants during treatment.8-10
Two cancer institutions recommended physical exercise to increase the body’s endogenous production of antioxidants to prevent or fight cancer. Although we did not list physical activity as an antioxidant in our survey, these recommendations echo increasing evidence indicating that physical exercise is associated with reduced cancer risk and cancer mortality 113 and better psychological and physical health and quality of life during and after cancer, 114 but the evidence that the mechanism of this effect is through increasing antioxidants is not established.113,115 One cancer center did not recommend participation in very high intensity exercise, consistent with research indicating that although exercise can increase the body’s production of defensive antioxidants, too high intensity exercise may deplete the body’s supply of antioxidants and cause oxidative stress.115-117
The majority (53%) of cancer institutions used evidence-based methods such as consulting literature reviews and original research articles to develop the policies or guidelines. Some institutions used peer discussion or obtained policies or guidelines from another institution. The dietetic/nutrition department was central to policy development and dissemination. The majority of Canadian institutions communicated the policies and guidelines using written handouts, which may limit accessibility in comparison to making information available online. A clinical implication is that ongoing education of dieticians may be the most reliable method of promoting uptake and translation of relevant research findings. Furthermore, there is merit in developing unified and evidence-based online policies to improve communication of up-to-date advice to patients, researchers, other cancer institutions, and the general public.
Limitations
A limitation of the study was the low response rate, which may have been an indication of lack of policies and guidelines on antioxidants at cancer institutions. People with no information to provide may have been more likely to simply not respond to the survey. Furthermore, the majority of responses were from either the dietetic/nutrition department or general information line. More responses from other clinicians may have provided data of further importance. It is possible that we were not able to contact or were not directed to the most appropriate or knowledgeable professionals in all of the organizations we contacted. While the nutrition departments were the primary source of information, often integrative medicine specialists and oncologists are the ones with specialized knowledge about usual practices or more informal guidelines in clinical use. Hence, even for institutions that provided information, it may not always be consistent with actual practice in that institution. Perhaps increasing the incentive for participation in future studies may increase the response rate and representativeness of the data.
Recommendations for Clinical Practice
There is a need for the implementation of clear policies and guidelines on antioxidants based on an up-to-date and comprehensive body of research evidence. Policies and guidelines on antioxidant supplements in particular need to be addressed since general guidelines are not sufficient to communicate the complexities of the research evidence. Specifically, policies should highlight current research evidence, including details on specificity of what types of antioxidants may be beneficial to certain cancer populations, in combination with the respective treatment regimens recommended. This may be, in part, why institutions have been slow to respond to emerging research evidence. Indeed, many cancer centers in this study discouraged the use of all antioxidant supplements based on a few specific studies that found adverse effects of certain antioxidant supplements on specific populations. However, some research studies indicate that various antioxidant supplements can be beneficial for reducing treatment-induced toxicities and sequelae and increasing efficacy of conventional cancer treatments. Therefore, a clear summary on the effects of antioxidants for different populations and cancer treatments may reduce extrapolation from a few studies that found adverse effects.
We advocate that cancer centers should consider incorporating into mainstream clinical practice certain antioxidant supplements and carefully monitor clinical outcomes. Overall, clear guidelines summarizing the current research evidence should be made available and further clinical trials encouraged. Ideally, cancer treatment centers would have trained integrative oncology staff with expertise in antioxidant use, and each patient’s case would be discussed by a multidisciplinary team consisting of these specialists along with treating radiation and/or medical oncologists and supportive care specialists to choose the most appropriate treatment protocols, using best practice guidelines as a starting point, and balancing benefits against potential adverse effects. An emphasis should be placed on balanced dietary sources of antioxidants rather than supplements, except in extreme cases of measured deficiencies. Outcomes including long-term evaluation of toxicity, side effects, quality of life, treatment responses, and adverse effects should then be monitored carefully on an ongoing basis.
Recommendations for Future Research
More studies examining the effects of specific antioxidant supplements on cancer risk and cancer survivorship and the effects of antioxidant-rich diets on cancer treatment outcomes are needed. Inquiry into the biological mechanisms behind certain antioxidant therapies that are beneficial for some population and treatment combinations in certain individuals but not others may aid in the development of more effective antioxidant therapies for cancer. Future research can also investigate which factors affect the decisions of health care providers and patients to use or not use these therapies. A possible area of investigation in the realm of knowledge translation is discovering the type of research evidence that is needed in order for a complementary therapy to become mainstream. For the field to advance it is likely helpful to stop thinking of antioxidants as a group of chemicals with similar properties and focus more on the individual substances, since there is so much variability among them in mechanism of action and clinical effects.
Conclusion
This study compared the current policies and guidelines on antioxidant use for cancer prevention, treatment, and survivorship at cancer institutions across North America with the current body of research evidence. Current recommendations on antioxidant-rich diets and physical exercise were generally consistent with the current research evidence base. However, the current research evidence on antioxidant supplements is unclear and difficult to generalize, so perhaps it is not surprising that institutional recommendations on antioxidant supplements tend to be more conservative, using the medical principle of primum non nocere (first do no harm). Health care providers may be hesitant to recommend antioxidant therapies unless they are consistently shown to be beneficial and generalizable to different populations and treatments. More specific recommendations on specific antioxidant supplements for specific populations may help bring policies and guidelines more in line with the research evidence. Communication of comprehensive research evidence to key individuals or departments involved in the development and communication of the policies and guidelines may aid in the more rapid development and dissemination of up-to-date and evidence-based recommendations on antioxidant use at cancer institutions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.