
Abstract
Background. The quality and dose of acupuncture used in a clinical trial affects the outcome, as with the quality and dose of any intervention. The dose of acupuncture treatment may be characterized by the frequency of treatment, needle type and depth, length of needle retention, point selection, and combination. The dose in trials of acupuncture has at times been described as low or inappropriate but is seldom assessed in systematic reviews of acupuncture trials. This article examines the research evaluating acupuncture for cancer-related fatigue to determine what characteristics of treatment may contribute to a quality acupuncture intervention. Methodology. English and Chinese language databases were searched from inception to December 2013 for randomized controlled trials of acupuncture for the treatment of cancer-related fatigue. Assessment of the quality of the acupuncture intervention was undertaken using the domains and items from the NICMAN framework. Results. Seven studies with a total of 690 patients were included. Four of the studies were designed as feasibility or pilot studies, and the other 3 studies were described as “effectiveness” trials. The treatment paradigm for the active intervention was based on traditional Chinese medicine in all studies, yet few of the studies were explicit as to how the active intervention was justified within a traditional Chinese medicine paradigm. Acupuncture point prescriptions were developed by a small consensus panel or based on typical points and/or “clinical experience.” No discussion of traditional Chinese medicine theory or literature review was reported in any studies. Acupuncture point location was adequately described in 4 of the 7 studies. Frequency of treatment was twice per week in 2 studies; all others were once per week. Two studies did not apply needle manipulation or stimulation, and no justification was given. Conclusion. The 7 trials reviewed meet some criteria for a quality acupuncture intervention. However, frequently elements of the intervention were not addressed, and it is possible that the dosage trialed was suboptimal. Systematic reviews of acupuncture are likely to continue to be inconclusive while comparisons are conducted of heterogeneous interventions without providing.
Background
The quality and dose of acupuncture used in a clinical trial affects the outcome, as with any intervention.1-3 The dose of acupuncture treatment is characterized by the frequency of treatment, needle type and depth, length of needle retention, point selection, and combination. These characteristics affect the effectiveness, efficacy, and cost of an acupuncture treatment. 4 Underpinning dosage are the many different traditions of acupuncture—Japanese, traditional Chinese medicine (TCM), Korean, and dry needling. The heterogeneity of acupuncture is a formidable challenge in a clinical trial setting. 5 Dose is also affected by the state of the patient, their response to treatment, and the severity of the disease. 6 There are good reporting criteria for acupuncture trials, but criteria for assessing the quality of acupuncture interventions in clinical research or the representation of real-world practice of acupuncture within study designs are lacking.4,7 The dose in trials of acupuncture has at times been described as low or inappropriate but is seldom assessed in systematic reviews of acupuncture trials. 8 This article examines the research evaluating acupuncture for cancer-related fatigue (CRF) to determine what characteristics of treatment may contribute to a quality acupuncture intervention.
Fatigue is reported by people with cancer as the most prevalent, debilitating, and unrelieved symptom of cancer and its treatment.9,10 Fatigue affects 70% to 100% of patients undergoing chemotherapy, radiotherapy, or biotherapy.11,12 It may be a presenting physical symptom of cancer alone, or it may result from the complex interplay of other factors such as the psychological distress associated with a diagnosis of cancer, the negative influences of cancer-related surgery, and the commencement of radiotherapy and/or chemotherapy.11,13 CRF generally increases during therapy but declines after treatment completion.13,14 There is a small but growing body of research examining the feasibility of acupuncture in the management of cancer fatigue and associated features.15,16 A recent meta-analysis found a significant difference between acupuncture and usual care but no significant difference between acupuncture and sham or waitlist despite a trend in favor of acupuncture. 17 These trials applied acupuncture at different stages of the cancer trajectory, and all used different acupuncture interventions with varied rationale, techniques, and dosage.
To assess the quality of the acupuncture interventions used in clinical trials, there are limited critical appraisal tools available. STRICTA provides a thorough reporting tool for acupuncture trials but does not provide an indication of the quality of the acupuncture intervention. Recent efforts have been made to understand or assess aspects of what might constitute a quality acupuncture intervention.6,18-20 Despite this early work, the best method to assess quality of acupuncture remains undecided, and no clearly reliable tool has been developed. A recent Delphi study of expert opinion in Australia identified 28 items as essential components of quality acupuncture treatment. Domains of the resulting NICMAN framework included study design, rationale of intervention, specific criteria relating to needling stimulation either manually or using electro-acupuncture, duration and frequency of treatment, and practitioner training. 7 To inform the treatment parameters for a future clinical trial of acupuncture and CRF, we used the NICMAN framework to review studies addressing CRF. The quality of the acupuncture interventions was assessed to identify optimal treatment characteristics.
Methods
The following databases were searched without language restriction from time of database inception to December 2013: Cochrane Complementary Medicine Field’s Trials Register, PubMed, MEDLINE, EMBASE, CINAHL, Dissertation Abstracts, PsychINFO, Chinese National Knowledge Infrastructure Databases (CNKI), Chinese Science and Technology Periodical Database (VIP), Chinese Biomedical Literature Database (CBM), and the Wanfang Database. Trial registries in Australia (Australia New Zealand Clinical Trials Registry), the United States (Clinical Trials.gov), and the World Health Organization (International Clinical Trials Registry Platform) were also searched. Bibliographies of relevant articles were also searched. The search strategy adopted was modified as fit for each database (a detailed search strategy is provided in the appendix).
We included all randomized controlled trials (RCTs) using manual, electric, or auricular acupuncture for the treatment of cancer fatigue. Transcutaneous electrical nerve stimulation RCTs were excluded. Comparators included sham acupuncture, no intervention, and other management options for cancer fatigue including but not limited to acupressure, psychological interventions, and pharmacological interventions. Participants were 18 years and older with clinically significant levels of cancer fatigue, regardless of gender, cancer stage and type, duration of fatigue, and modality of any treatment received. Participants were excluded if their fatigue existed prior to the diagnosis of cancer, or if the fatigue was explained by a preexisting secondary cause such as anemia, hypothyroidism, or depression.
We searched PubMed for information on biomedical functions relevant to the acupuncture points used in the clinical trials. We searched using [point or pinyin name] combined with [fatigue or cancer [MeSH] or immun* or inflammat*] and [acupuncture [MeSH term].
Data were extracted by 3 reviewers (SG, NDS, and CS). One study authored by CS was assessed by SG and NDS. Assessment of the quality of the acupuncture intervention was undertaken by 2 reviewers (SG and CS) using the domains and items from the NICMAN framework (Table 1). 7 To determine if the acupuncture intervention addressed the research question (Domain 4 of the NICMAN framework), we identified if the study sought to test or pilot an intervention, or determine its efficacy or effectiveness. The 7 criteria set out by Singal et al were used to distinguish between “efficacy” and “effectiveness”, although efficacy and effectiveness exist on a continuum and the studies might not fall neatly into one category or the other. 21
Assessment of Quality of Acupuncture Studies.

Does not apply for pragmatic or effectiveness studies.
Results
A total of 745 records were identified and 7 studies met the inclusion criteria (Figure 1). Seven studies with a total of 690 patients were thus included. All studies were RCTs of parallel design. Five trials had 2 study groups,22-26 and 2 trials had 3 study groups.27,28 Risk of bias assessment has been completed elsewhere for these trials.15-17

PRISMA flow diagram of studies.
Population, Intervention, Comparator, Outcome (Domain 1)
According to Domain 1 of the NICMAN framework, the study population, intervention, comparator, and outcome must be clearly stated and a study design appropriate to the research question outlined (see Tables 2 and 3).
Assessment of Quality of Acupuncture Studies.

Abbreviations: CRF, cancer-related fatigue; BFI, Brief Fatigue Inventory; CES-D, Center for Epidemiologic Studies Depression Scale; FACIT-F, Functional Assessment of Chronic Illness Therapy (FACIT) Measurement System–Fatigue; HADS, Hospital Anxiety and Depression Score; HRT, hormone replacement therapy; MFI, Multidimensional Fatigue Inventory.
Assessment of Quality of Acupuncture: Domains 7 to 14.
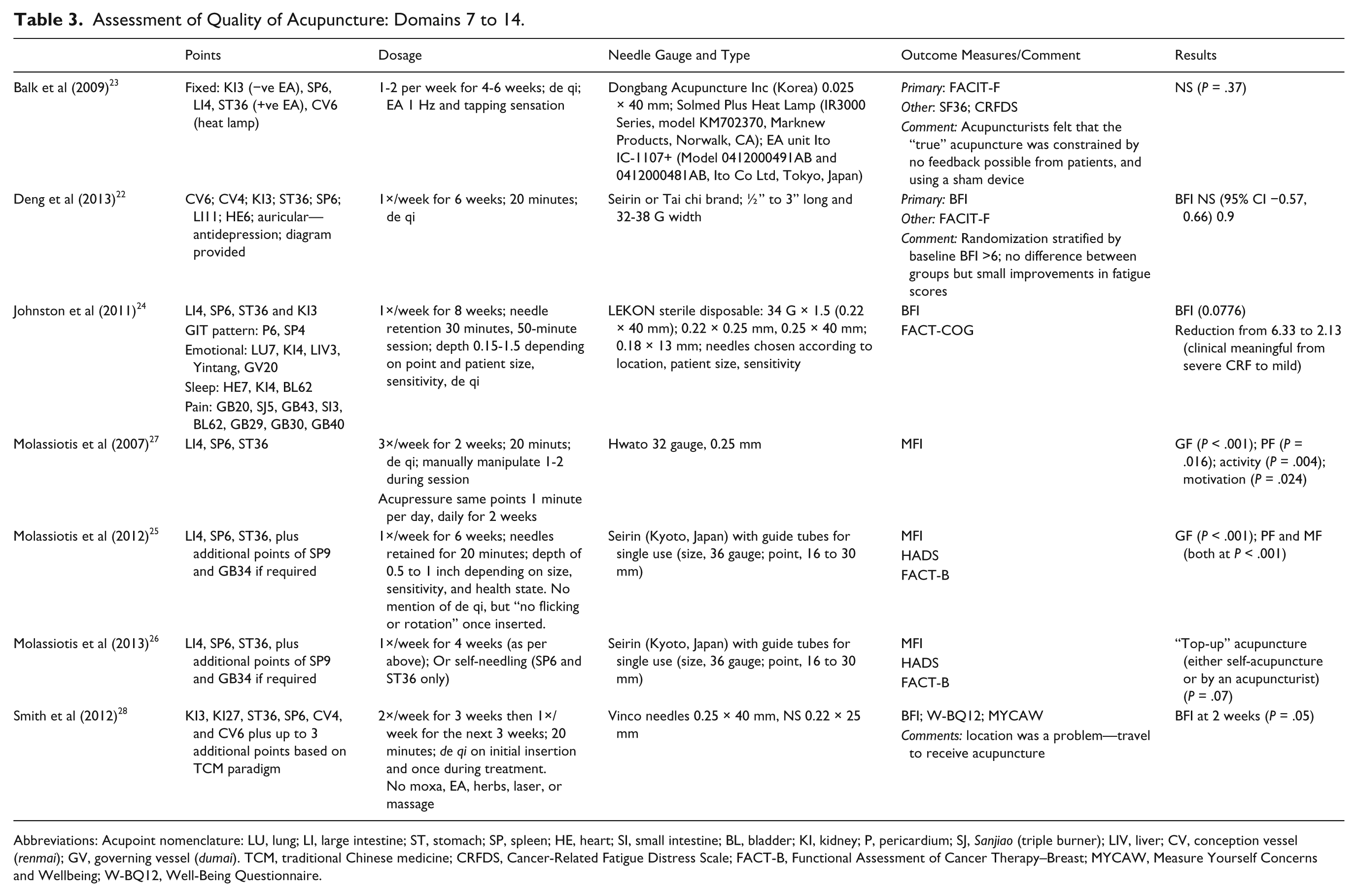
Abbreviations: Acupoint nomenclature: LU, lung; LI, large intestine; ST, stomach; SP, spleen; HE, heart; SI, small intestine; BL, bladder; KI, kidney; P, pericardium; SJ, Sanjiao (triple burner); LIV, liver; CV, conception vessel (renmai); GV, governing vessel (dumai). TCM, traditional Chinese medicine; CRFDS, Cancer-Related Fatigue Distress Scale; FACT-B, Functional Assessment of Cancer Therapy–Breast; MYCAW, Measure Yourself Concerns and Wellbeing; W-BQ12, Well-Being Questionnaire.
All patients had a diagnosis of CRF following chemotherapy and/or radiotherapy treatment. To recruit patients with persistent CRF, studies sought patients who had chemotherapy at least 1 month 24-28 or at least 60 days prior to the trial commencement date. 22 One study did not include length of time since chemotherapy or radiotherapy. 23 The type of chemotherapy was documented in all 3 Molassiotis studies and length of chemotherapy regime or radiotherapy in one study. 28
Five studies were conducted in breast cancer patients23-25,27,28 the 2 other studies included a variety of tumor types.
None of the studies recorded details of medications such as antidepressants, sleep medication, or other confounding factors such as hypothyroidism or recent surgery that may have an impact on CRF.
Several validated instruments to assess CRF were used to screen participants. Three studies used the Brief Fatigue Inventory (BFI),22,24,28 including only patients with a BFI ≤4. One study used the Functional Assessment of Cancer Therapy Treatment instrument (FACIT-F) including patients scoring below <44. 23 Molassiotis and colleagues included patients who reported high fatigue levels >5 on a visual analogue scale (VAS) of 0 to 10.25-27
The primary outcome measures used were FACIT-F, 23 BFI,22,24,28 and the Multidimensional Fatigue Inventory (MFI).25-27
Interventions were acupuncture alone, or acupuncture combined with education. Comparators were Park Sham needle on same points, Streitberger needle, usual care, sham acupressure, enhanced usual care, or waitlist. The essential components of the research questions in all studies were clearly expressed and the experimental designs aligned with the questions. All studies met the requirements of Domains 1 and 2 of the NICMAN framework.
Design of the Intervention (Domains 3-5)
The treatment paradigm for the active intervention was based on TCM in all studies. Yet in only 2 of the studies was any form of TCM diagnosis undertaken.24,28 In these two studies the TCM diagnosis was undertaken to partially individualize a fixed intervention. In none of the other studies was TCM diagnosis performed. As such it was not explicit as to how the active intervention was justified within a TCM paradigm (Domain 3 of the QoA framework). All studies defined the study population in terms of a Western medicine paradigm.
Four of the studies were designed as feasibility or pilot studies, and intended to determine an effect size and verify that the acupuncture intervention and control were designed appropriately.23,24,27,28 The 3 other studies were described as “effectiveness” trials. In one of these studies, the acupuncture intervention was fixed, sham controlled, allowed no pragmatic alterations, no concurrent interventions, and was conducted in an experimental rather than a clinical setting. 22 This study design would appear to be more appropriately defined as an “efficacy” study. The other 2 studies allowed for additional points that could be used at the discretion of the acupuncturist somewhat reflecting clinical practice, compared the intervention to usual care, and may be defined as “pragmatic” or “effectiveness” although no additional or concurrent treatment was permitted.25,26
The diagnostic process according Western medicine was appropriate in all studies, and a validated tool was used to determine the level of fatigue and criteria established to ensure the diagnosis of cancer-related fatigue was met. Domain 5 was met by all studies.
Acupuncture Intervention (Domain 6)
The development of an acupuncture point prescription for a trial should be consistent with differential diagnosis, a treatment paradigm, and/or based on a literature review or other evidence (Domain 6). Two studies22,28 based their intervention on an earlier Phase II study.29,30 The intervention arrived at by Vickers et al was the product of a consensus panel at the Memorial Sloan Kettering Cancer Centre, and were “points typically used in Chinese medicine to treat fatigue.” The other 5 studies23-27 based their acupuncture presciption on “TCM theory . . . points traditionally used for ‘energy’ over the past 2000 years and the ‘clinical experience’ of the attending acupuncturists.” No discussion of TCM theory was provided although 2 studies provided single references to 2 general acupuncture textbooks. No literature review concerning acupuncture point selection was reported in any of the studies.
Two studies permitted acupuncture points to be selected according to a differential diagnosis based on Chinese medicine. One of these studies permitted practitioners to select from 3 secondary points based on differential diagnosis from a TCM paradigm. 28 The other study provided the option for practitioners to diagnose according to TCM theory a “gastrointestinal pattern”; “emotional,” “sleep,” or “pain” pattern; and use additional points from a list provided. 24
Point Selection, Location, Needling, Depth, and Duration (Domains 7-10)
The needle brand, gauge, and length was documented adequately in all studies (Domain 7). In most studies, the exact needle gauge and length used for each acupuncture point was selected according to the location of the point being needled, the size of the patient, patient sensitivity to needles, and the general state of health of the patient.
Actual acupuncture point location was adequately provided in 4 studies by providing a figure in one study 22 and described in anatomical terms in 3 studies.23,26,27 Three studies did not provide details of actual acupuncture point location in anatomical terms or by reference to a standard acupuncture text.24-26,28
Needles were placed bilaterally in all studies24,25,28 unless the point was located on the midline. If a patient was at risk for lymphedema, the affected limb was not needled.22,23,25,26 Depth of needling insertion was appropriately referenced to guidelines such as the American Academy of Medical Acupuncture, 23 or standard texts, 28 or depth expressed in terms of a range of 0.5 to 1 inches or millimeters.
Number of Treatments (Domain 11)
CRF is a chronic condition, and the NICMAN group proposes that a chronic condition requires a minimum of 6 treatments in the intervention to be thought adequate. All studies met the NICMAN criteria with the exception of one. In the study conducted by Balk et al, 23 the frequency and duration of the intervention was “1-2× week for 4-6 weeks.” As such some subjects in this study may have received as few as 4 treatments. Two studies provided 2 or more treatments per week.27,28
Needle Manipulation (Domains 12 and 13)
Two studies met the criteria set out to adequately describe the method of needle manipulation. In one study the needles were “flicked or rotated once or twice per session” 27 ; and in the other study, the needles were manipulated on “initial insertion” and “once more during the treatment.” 28 Five studies referred to attaining “a “needle grab” sensation or “deqi.”22-24,27,28 Two studies did not describe any needle manipulation or stimulation, and no justification for this aspect of the intervention was provided.
Only one study used electro-acupuncture. 23 This study adequately described the level of stimulation and the type of machine used, but the approval status within the country where the study was conducted was not reported.
Acupuncturist: Training and Monitoring (Domain 14)
All studies used licensed and registered acupuncturists. No specific training in the acupuncture intervention and clinical condition or monitoring of the actual administration of the intervention in any of the trials was mentioned. Two studies referred to following a “strict protocol” but no further information was provided.25,26 Two studies noted that the acupuncturist was experienced in treating patients with cancer.24,27
Prevalent Acupuncture Points Used
Two points were used in all the clinical trials: Zusanli and Sanyinjiao (Table 4). Zusanli is often termed the “immune-enhancing acupoint” and is frequently used in acupuncture point combinations for diseases where there is immune system dysregulation or inflammation. 31 Electro-acupuncture at Zusanli controls systemic inflammation by the production of dopamine in the adrenal medulla, and dopamine inhibits cytokine production. 32 Animal or clinical evidence for regulating immunity and/or reducing inflammation was available for most of the acupuncture points used in the clinical trials for CRF. The causes and manifestations of CRF are multifactorial. There is some evidence that CRF is caused by a persistent inflammatory or immune response. 33 The tumor itself may be a source for pro-inflammatory cytokines while treatment may induce cytokines in response to tissue damage from radiation or chemotherapy.
Main Acupoints Used in the Studies.

Single acupoints analysis precludes the synergy of using point combinations.
Discussion
Acupuncture is a complex intervention. Acupuncture trials often reach contrary or inconclusive results.6,59,60 There are many elements that have been attributed to exerting effect within the intervention: needle sensation, manipulation, frequency, duration, and point location along with aspects of the acupuncture “ritual.”61,62 It would appear fairly self-evident that an acupuncture protocol prepared for a clinical trial is of vital importance, placing the dose of the intervention in a clear therapeutic framework and a considered rationale. 6 The 7 trials reviewed met some criteria for an adequate “dosage” of acupuncture. However, frequently elements of the intervention were not addressed and it is possible that the dosage trialed was suboptimal.
The treatment paradigm of all trials was nominally TCM, yet only 2 research designs incorporated elements of TCM diagnostic and treatment theory. No explanation was provided as to why these points were expected to have an effect, in either TCM terms or biomedical terms. One reference was made to “these points are traditionally used for ‘energy’ over the past 2000 years.” The interventions were not placed within a theoretical framework, biomedical or Chinese medicine. The treatment paradigm, TCM or medical acupuncture, influences not only the diagnostic theory but the treatment and practice. “Model validity” is considered a key component of complementary therapy RCTs, and acupuncture protocols for RCTs should clearly detail how the intervention fits within the nominated “model” or “paradigm.”
Few of the studies drew on an adequate review of the literature, or sought a consensus with a number of experts. Interventions were based on a previous study or “clinical expertise” or a single textbook. While these sources may inform an intervention, a more “optimal dose” may have been obtained through broader systematic consensus using a combination of expert survey, literature, and meetings. 63
All studies used a protocol of fixed acupuncture points, with 2 studies permitting the of use additional points. Fixed protocols have the advantage of good internal validity but poor external or model validity. 64 It is arguable if fixed protocols are best practice as far as acupuncture is concerned. 6 One way of allowing more flexibility in the acupuncture points selected is through the use of “manualization.” Treatment manualization specifically details the treatment framework and protocols, facilitates the design of protocols that reflect complex interventions, and allows treatments to be tailored to individuals to maximize therapeutic effects.65,66
Frequency of dosage was partially met in the studies. All but one of the studies provided a minimum of 6 treatments but few provided these treatments twice weekly. In an individual patient meta-analysis of data from clinical trials of acupuncture for pain, increased number of needles and more sessions appear to be associated with better outcomes when comparing acupuncture to control groups. 67 Specifically the number of treatment sessions appeared to be positively correlated to good outcomes as did the number of needles used. 67
Needle sensation was not considered in 3 of the trials reviewed here. De qi sensation has been associated with increased local blood flow to the area and deactivation and activation of different parts of the brain.68-70 The de qi response is a standard part of clinical practice in TCM. The studies that did not seek to elicit de qi did not provide a rationale for its omission. From a neurophysiological perspective, we know that the response of an organism will typically be dependent on the intensity or dose of the stimuli. 71 De qi should universally be assessed and reported in all types of clinical and experimental trials. 68
In Chinese medicine, different needle manipulation techniques are used to “tonify” or “reduce.” Different manual needle techniques have been associated with different biomarkers, different autonomic effects, and varied cerebral activation.61,71
Our review is consistent with other studies examining the dosage or adequacy of the acupuncture intervention. White and Ernst provide a checklist of data required for reporting acupuncture from which to enable reviewers to determine if the acupuncture was “possibly adequate” to “probably adequate.” 20 In their review of acupuncture trials for neck and back pain, Smith et al conclude there is insufficient information to answer important questions of validity. 7 Price and colleagues suggest adequate information be provided to enable acupuncture trials to be classified as “traditional acupuncture (TA),” “medical acupuncture (MA),” or “unclassifiable.” 6 These studies, along with our review, aim to build on the existing STRICTA framework to enable an assessment to be made about the adequacy or dosage of the acupuncture intervention.
The reporting of acupuncture research has improved in response to the STRICTA Statement. 72 However, the related issue of being able to assess the quality of acupuncture has remained problematic. Early efforts to assess quality by White and Ernst 20 stalled due to the unreliability of the method with inconsistent scores. In 2008, development of the NICMAN framework commenced, involving external views of stakeholders through a consensus method to define the inclusion of items describing quality acupuncture. Our review highlights the potential usefulness of the NICMAN framework to assess the quality of acupuncture interventions. While the NICMAN framework 7 is still undergoing continued validity and reliability testing, the framework has demonstrated usefulness in this context enabling the differentiating dimensions of acupuncture studies to be assessed. However, we recognize that until validity and reliability is established an assessment of the clinical significance of acupuncture quality remains open to subjective interpretation.
It is difficult to conclude from examining these studies which might be the most effective dosage. Furthermore, systematic reviews of acupuncture are likely to continue to be inconclusive while comparisons are conducted of heterogeneous interventions and heterogeneous cancer populations. Differentiating between traditional acupuncture and biomedical acupuncture might be a start, whether or not de qi was elicited, and understanding patient expectations. A clear acupuncture protocol will assist in determining whether the “dosage” administered was adequate. The analysis of individual trial data from pragmatic or “whole system” clinical trials may also be one method of determining efficacy. The complexity of acupuncture and true efficacy will be best understood through comparison and meta-analysis of trials that are similar in their treatment paradigm and dosage.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.