
Abstract
Introduction. Nasopharyngeal cancer (NPC) survivors often sustain head–neck–shoulder impairments from conventional treatments, which could disturb sleep. This novel study aimed to examine the efficacy of Tai Chi (TC) Qigong in optimizing temporomandibular joint (TMJ), cervical, and shoulder joint mobility and reducing sleep problems in NPC survivors. Methods. Fifty-two NPC survivors participated in the study. The experimental group (n = 25) received 6 months of TC Qigong training (1.5 h/session; 4 sessions/wk including self-practice) while the control group (n = 27) received no training. Cervical side flexion and rotation, shoulder flexion and horizontal flexion range of motion (ROM), mouth opening capacity (interincisor distance), and sleep problems (Medical Outcomes Study Sleep Scale) were assessed at baseline, mid-intervention (3 months), immediately after TC Qigong training, and at 6-month follow-up. Results. Intention-to-treat analysis revealed improvement in cervical side flexion ROM only (P < .008) and unchanged shoulder and TMJ mobility (P > .008) after the TC Qigong training. Deterioration was observed in shoulder flexion ROM and mouth opening capacity in the no-training controls over time (P < .008). Sleep problems also decreased in the TC Qigong group (P < .008), and this effect was most profound during the follow-up period. In addition, improvement in cervical side flexion ROM was associated with a reduction in sleep problems in the experimental group after TC Qigong training (P < .05). Conclusions. The 6-month TC Qigong intervention improved neck mobility, maintained TMJ and shoulder joint mobility, and reduced sleep problems for NPC survivors. TC Qigong could be an effective nonpharmacological intervention for managing progressive trismus, chronic neck and shoulder hypomobility, and reducing sleep problems among NPC survivors.
Introduction
Nasopharyngeal carcinoma (NPC) is a malignancy of the head and neck region common in Southeast Asia, Southern China, and North Africa. The incidence rate in these regions is high (25-50 per 100 000). 1 Currently, the primary medical management for NPC is radiotherapy, while chemotherapy and surgery (eg, nasopharyngectomy) are elective treatments. 2 Although previous research has shown that these aggressive treatment methods can successfully control tumors and thus increase overall survival rates, 1 survivors generally experience many associated side effects, such as neck muscle fibrosis,3,4 trismus or restricted mouth opening,5,6 and shoulder dysfunctions. 7 The disease can also directly cause chronic symptoms, such as pain and fatigue. 8 These clinical symptoms, together with the sequelae of NPC treatments, can disrupt the sleep of NPC survivors.8,9 Sleep is a necessary physiological and behavioral activity and is essential for maintaining health and well-being. 9 Therefore, it is of paramount importance to explore effective strategies for relieving the physiological side effects and sleep problems suffered by NPC survivors.
To manage the adverse effects of NPC and the side effects of conventional cancer treatment, many survivors turn to complementary and alternative medicines such as Tai Chi (TC) and/or Qigong. 10 TC and Qigong are ancient Chinese psychosomatic exercises comprising meditation, breathing exercises and coordinated body movements. Regular practice of TC/Qigong helps develop good health and promotes self-healing. 11 Previous studies have reported that short-term Qigong training can reduce neck–shoulder pain and disability in individuals with neck pain12,13 and increase sleep duration among university students. 14 However, no studies have specifically investigated the effects of TC Qigong among NPC survivors who also suffer from head–neck–shoulder disabilities and sleep disturbance. This study aimed to (1) investigate the effects of TC Qigong training on the temporomandibular joint (TMJ), cervical and shoulder joint mobility and sleep problems of NPC survivors and (2) explore the relationship between upper body joint mobility and sleep problems if any significant changes in these outcomes were demonstrated after the TC Qigong training.
Methods
Study Design
This was a single-blinded, nonrandomized, controlled clinical trial. The outcome assessors were blinded to the group participation. The participants were instructed not to inform the assessors about their group to avoid possible bias during measurements.
Participants
Tang et al 15 reported that the sleep quality score of cancer patients improved from 13.42 ± 2.27 to 9.78 ± 3.06 after gentle exercise training, which translated into a large effect size (1.32). In a study of Qigong, the effect size for joint range of motion (ROM) flexibility tests (eg, the sit-and-reach test) was 0.68 (pre-Qigong = 9.8 ± 10.8 cm; post-Qigong = 13.0 ± 6.1 cm). 16 Therefore, assuming a medium-to-large effect size of 0.68, a power of 0.80 and an α of 0.05 (2-tailed), a minimum sample of 19 participants is needed to detect a significant within-group difference in outcome measures. Anticipating a possible dropout rate of 15%, 17 22 participants were required for the TC Qigong group and the control group.
Survivors of NPC were recruited from a medical clinic and a cancer survivors support group on a voluntary basis. The inclusion criteria were that the participants (1) had a formal diagnosis of NPC (positive Epstein–Barr virus DNA and biopsy test results), (2) received conventional hospital medical care, (3) were aged between 40 and 85 years and had an expected survival time of over 12 months, (4) were Cantonese and had lived in Hong Kong continuously for at least 7 years, and (5) had normal cognitive, visual, and hearing functions. The exclusion criteria were that they (1) were receiving active cancer treatments (eg, radiotherapy, chemotherapy, acupuncture or herbal medicine) or were engaged in postoperative rehabilitation, (2) had other chronic diseases (eg, uncontrolled diabetes mellitus, hypertension or cardiopulmonary diseases) or psychiatric disorders, (3) had TMJ disorder or significant neurological (eg, cervical myelopathy) or musculoskeletal disorders (eg, fractures and shoulder adhesive capsulitis) that could affect assessment performances, and (4) were on hypnotic medications or other medications that could affect sleepiness. The participants were first screened by a medical doctor. If the participants met the inclusion criteria, they were allocated to either the TC Qigong group or the control group according to their preference. Ethical approval was obtained from the administering institutes. The study was explained to each participant, and written informed consent was obtained. All procedures were conducted in accordance with the Declaration of Helsinki.
Intervention
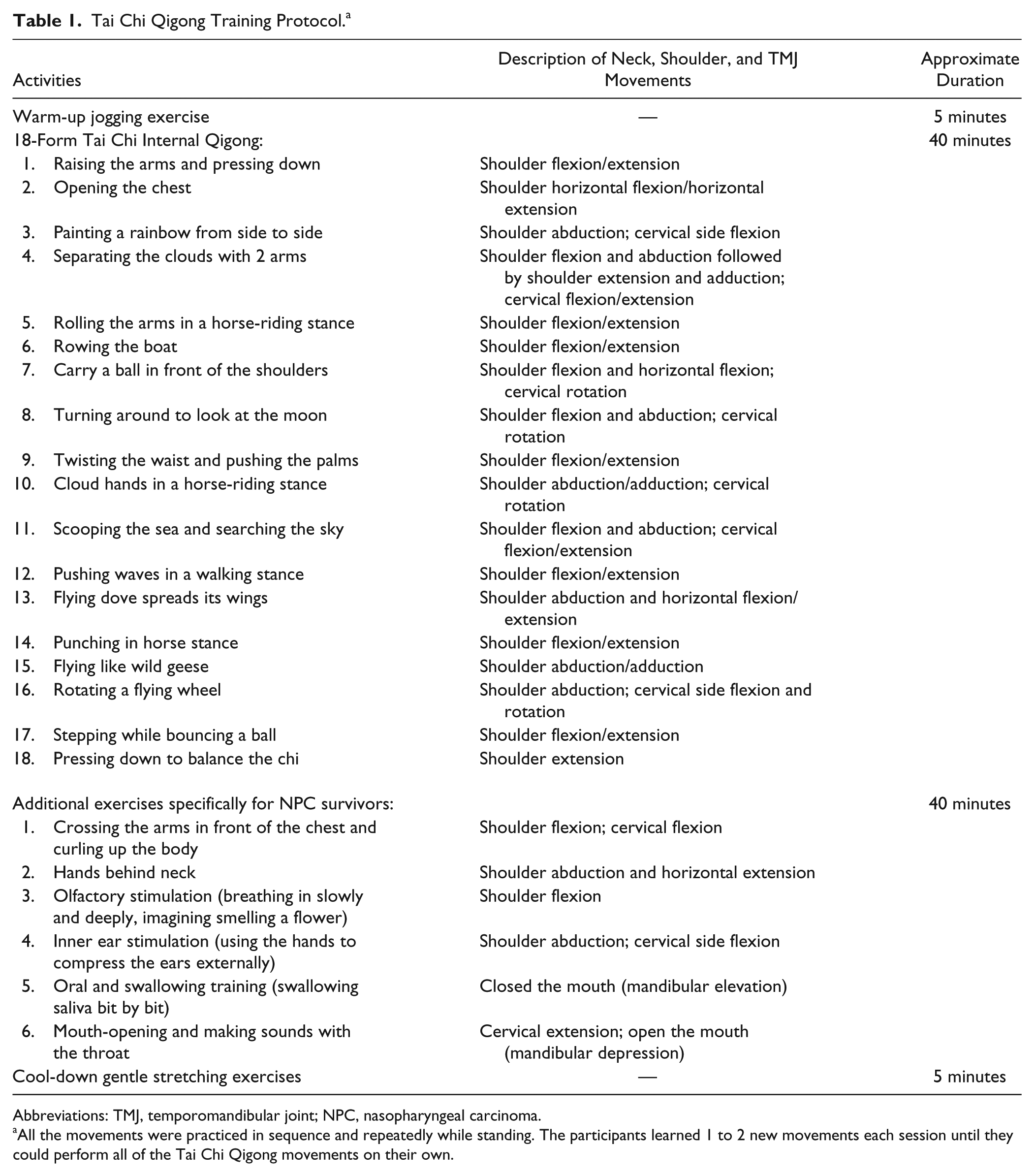
The participants in the TC Qigong group attended a weekly 1.5-hour session of TC Qigong training (concurrent conventional medical care was allowed) at the Nature Health Qigong Association for 6 consecutive months. The TC Qigong training protocol is described in Table 1. The protocol was designed by a medical doctor and a Qigong master based on the Eighteen Form Tai Chi Internal Qigong. 18 It included NPC-specific movements, such as mouth opening and inner ear stimulation exercises, in addition to the basic TC Qigong form. Like other TC/Qigong training regimes, our TC Qigong protocol emphasized deep concentration (meditation) and coordinated breathing in conjunction with slow and smooth TC movements (focused on upper limb movements). The aim of TC Qigong is to bring the body, mind, and spirit into balance. 18 All the training sessions were conducted by a certified Qigong instructor and an assistant instructor.
Tai Chi Qigong Training Protocol. a
Abbreviations: TMJ, temporomandibular joint; NPC, nasopharyngeal carcinoma.
All the movements were practiced in sequence and repeatedly while standing. The participants learned 1 to 2 new movements each session until they could perform all of the Tai Chi Qigong movements on their own.
Each participant was also given TC Qigong home exercises to supplement each training session and to increase the exercise frequency to three times per week (excluding the TC Qigong class days). The home exercises were the same as those practiced in the face-to-face TC Qigong training sessions. The participants were allowed to split the 1.5-hour practice time into 2 or 3 shorter sessions to avoid fatigue. The Qigong instructor or assistant instructor checked with the participants during each supervised lesson to ensure that they completed the home exercises. The control group did not receive any TC Qigong training during the study period, but continued to receive conventional hospital medical care as appropriate.
Outcome Measurements
The participants were assessed by a physiotherapist and a trained assistant 1 week before the TC Qigong training started (pretest), after 3 months of TC Qigong training (mid-intervention assessment), within a week of the 6-month TC Qigong training ending (posttest), and 6 months after posttest (follow-up test). The assessors were blinded to the participants’ subject groups. The participants were asked about their demographic and medical characteristics at pretest (Table 2). All the participants, regardless of their grouping, were assigned to the pre-, mid-, postintervention and follow-up assessments in random order.
Participants’ Characteristics.
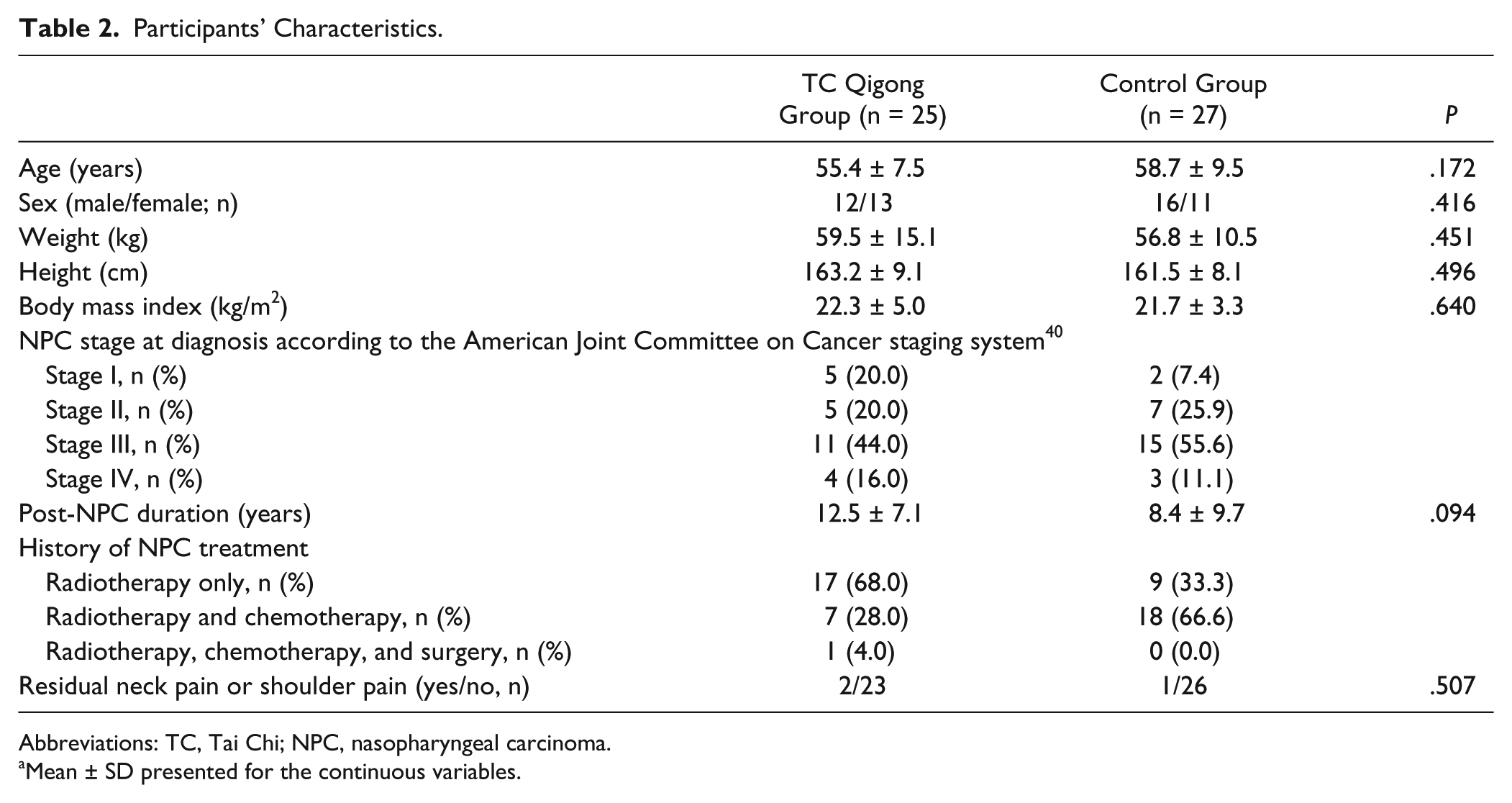
Abbreviations: TC, Tai Chi; NPC, nasopharyngeal carcinoma.
Mean ± SD presented for the continuous variables.
Cervical Spine Ranges of Motion
Active cervical spine side flexion and rotation ranges of motion were selectively measured because these movements are essential for bed mobility and daily functioning.19,20 To measure the ROM, a Myrin goniometer (Medema, Stockholm, Sweden) was attached to the forehead (when measuring cervical side flexion) or secured on top of the head (when measuring cervical rotation) of the participant by Velcro strips while the participant was in a seated position. This instrument is reported to have near perfect test–retest reliability (intraclass correlation coefficient [ICC] = 0.90-0.96), interrater reliability (ICC = 0.92-0.97), and concurrent validity (ICC = 0.93-0.96) compared with a criterion measure (3-dimensional ultrasound movement analysis device) for cervical full ROM measurements in adults. 21 During the test, the assessor helped the participant to stabilize the trunk and instructed him or her to move the head sideways (cervical side flexion) and then turn the head to one side (cervical rotation) to the limit of motion. The active bilateral cervical side flexion and rotation ranges of motion were read from the goniometer dial. 19 After 4 warm-up trials, 21 2 testing trials were conducted and the average ROM values in each movement direction were documented.
Shoulder Complex Range of Motion
Among the physiological movement directions of the shoulder complex, flexion and horizontal flexion are particularly important for the initiation of rolling and daily functions.19,20 Thus, these 2 movement directions were measured by a universal goniometer following standardized protocols to minimize compensatory or trick movements. 19 The universal goniometer was used because it is a valid tool with demonstrated good intrarater reliability (ICC = 0.84-0.91) and interrater reliability (ICC = 0.82-0.89) for shoulder hypomobility measurement. 22 Only the dominant side was assessed because no significant difference was found between the 2 sides when shoulder flexion and horizontal flexion ranges of motion were compared. 23 To measure shoulder flexion, each participant sat on a chair with a backrest. The assessor stabilized the participant’s trunk and instructed him or her to elevate the arm in the forward direction until the limit of motion. The goniometer axis was aligned with the glenohumeral joint axis (the lateral aspect of the center of the humeral head) to measure the maximum active shoulder flexion ROM without fixing the scapula. 19
To measure shoulder horizontal flexion ROM, the goniometer axis was placed on top of the acromion process. Starting from 90° shoulder abduction, the participant was instructed to slowly reach across his or her chest to the limit of motion. The assessor supported the participant’s arm in abduction, if necessary, and measured the maximum active horizontal flexion ROM using the same universal goniometer. 19 Four warm-up trials were allowed for all shoulder ROM measurements. 21 Then, the average ROM value of the 2 testing trials was documented.
Temporomandibular Joint Mobility
Mouth maximum unassisted opening capacity (mandibular depression) was assessed by measuring the distance between the incisal edges of the maxillary and mandibular central incisors using a plastic ruler marked in millimeters. 24 This method was found to have near-perfect intrarater (ICC = 0.70-0.99) and interrater reliabilities (ICC = 0.90-1.00). 24 Three trials were conducted and the average mouth-opening distance was calculated and recorded.
Sleep Problems
The Medical Outcomes Study (MOS) Sleep Scale is a 12-item self-reporting measure that assesses 6 sleep dimensions: sleep disturbance, perceived adequacy of sleep, quantity (hours of sleep each night), daytime somnolence, snoring, and shortness of breath or headache. The MOS scale is a valid and reliable instrument for assessing sleep problems in adults.25,26 The participants were asked to indicate how often they had experienced each of the sleep-related problems in the past 4 weeks on a 6-point categorical scale ranging from “all of the time” to “none of the time.” In addition, they were asked to indicate the time taken to fall asleep (ranging from “0-15 minutes” to “more than 60 minutes”) and the number of hours they slept each night. The scores were recalibrated and converted to the MOS sleep subscale scores (eg, sleep disturbance score) and the 9-item sleep problems index according to the guidelines stipulated in the MOS Sleep Scale scoring manual. 26 The sleep disturbance score and the 9-item sleep problem index were used for analysis. A higher sleep disturbance score indicated that the participants were less able to fall asleep and maintain restful sleep. A higher sleep problem index reflected worse sleep problems, including sleep disturbance, sleep inadequacy, respiratory impairment, and somnolence among the participants. 26
Statistical Analysis
The normality of the data was checked by using the Kolmogorov–Smirnov tests. Independent t tests (for continuous data) and the χ2 test (for nominal data) were used to compare the demographic and baseline characteristics of the experimental and control groups. The intention-to-treat principle was used for the primary data analysis. For participants who withdrew from the study, the last observations (data points) before dropping out were carried over to the subsequent assessments. Next, to assess the overall time-by-group interaction effects of TC Qigong training and to avoid committing a type one error due to multiple comparisons, 2-way repeated-measures multivariate analysis of covariance (MANCOVA) with a mixed design was conducted twice. The first MANCOVA analysis incorporated all the joint ROM outcomes while the second MANCOVA analysis included all of the MOS Sleep Scale–derived scores. The within-subject factor was time and the between-subject factor was group. If there were significant between-group differences at baseline in any of the outcome parameters, the baseline data for the outstanding outcome variables were entered as covariates. Effect sizes (partial η2) were reported for each outcome. By convention, partial η2 values of 0.14, 0.06, and 0.01 were considered as large, medium, and small effect sizes, respectively. 27 After the multivariate tests, further analyses were performed using 1-way repeated-measures analysis of variance (ANOVA) and then post hoc paired t tests with Bonferroni correction (to compare each outcome variable between time points within each group) as appropriate. Independent t tests were used to compare all of the outcome variables between the 2 groups.
Secondary data analysis was carried out to further explore the relationships between sleep problems and joint range of motion if any of these outcomes demonstrated a significant change after TC Qigong training. The bivariate associations between the significant MOS Sleep Scale–derived scores and the cervical/temporomandibular/shoulder joint ROM values after TC Qigong training were determined using the Pearson product–moment correlation coefficient (r). All of the statistical analyses were performed using IBM SPSS Statistics version 20.0 software (IBM, Armonk, NY). The significance level was set at .05 (2-tailed) and corrected using Bonferroni adjustment for the paired t tests (ie, the α was adjusted to .008 because of 6 paired comparisons) to maintain an overall type I error of 5%.
Results
Fifty-two survivors of NPC were deemed eligible to participate in the study. Twenty-five joined the TC Qigong training group voluntarily and the rest (n = 27) acted as controls. Over the study period, 11 participants (44.0%) in the TC Qigong group dropped out of the study for reasons that were not related to the training program (busy work schedule n = 4; illnesses n = 2; and unable to commit the time n = 5). Six participants (22.2%) in the control group dropped out for similar reasons (busy work schedule n = 1; unable to commit the time n = 1; traveled overseas n = 1; and lost to follow-up n = 3). A total of 35 participants (TC Qigong group n = 14 and control group n = 21) completed all the assessments. No significant differences in baseline characteristics or outcome measures were found between the dropouts and those who stayed in the study (P > .05). Moreover, no adverse events were reported during the TC Qigong training sessions, and the average attendance rate was approximately 90% for those who completed the TC Qigong intervention.
Comparison of Baseline Characteristics
No significant differences were identified in any of the demographic variables between the 2 groups (P > .05; Table 2). However, cervical spine bilateral side flexion and right rotation ROM, shoulder horizontal flexion ROM, and mouth-opening capacity differed between the 2 groups at baseline (P < .05; Table 3). Therefore, these outcome values were used as covariates in our primary data analysis.
Outcome measurements.
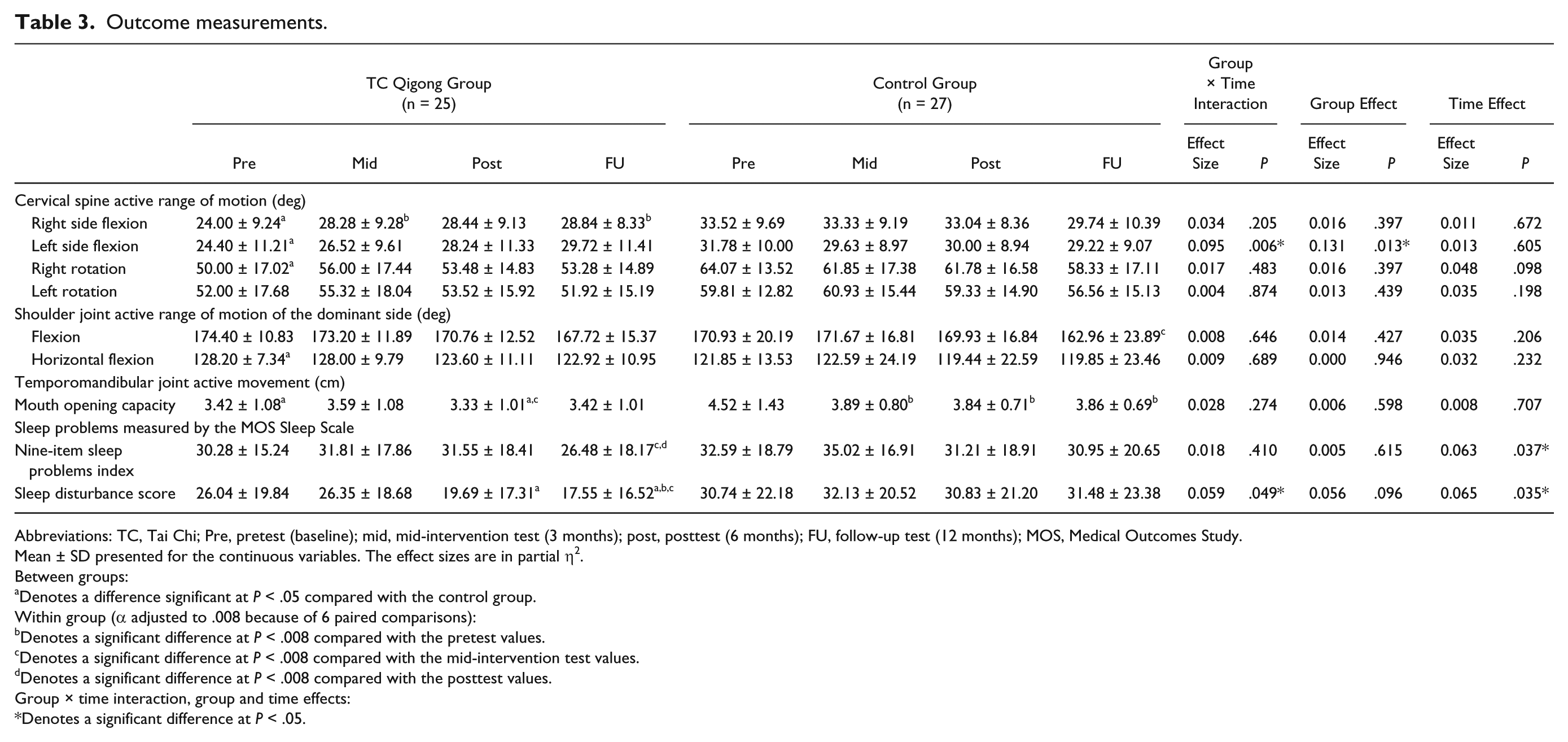
Abbreviations: TC, Tai Chi; Pre, pretest (baseline); mid, mid-intervention test (3 months); post, posttest (6 months); FU, follow-up test (12 months); MOS, Medical Outcomes Study.
Mean ± SD presented for the continuous variables. The effect sizes are in partial η2.
Between groups:
Denotes a difference significant at P < .05 compared with the control group.
Within group (α adjusted to .008 because of 6 paired comparisons):
Denotes a significant difference at P < .008 compared with the pretest values.
Denotes a significant difference at P < .008 compared with the mid-intervention test values.
Denotes a significant difference at P < .008 compared with the posttest values.
Group × time interaction, group and time effects:
Denotes a significant difference at P < .05.
Changes in Joint Mobility
Repeated measures MANCOVA revealed a significant time-by-group interaction effect (P = .006) and a significant group effect (P = .013) for the cervical left side flexion ROM outcome. The results indicated that, overall, the TC Qigong training program produced more gains in the cervical left side flexion ROM than no training. The cervical left side flexion ROM increased continuously from pretest to follow-up test in the TC Qigong group, although these improvements were not statistically significant (P > .008) for the sample size (Table 3). For cervical right side flexion, 1-way repeated-measures ANOVA showed that the ROM increased significantly at the mid-intervention (P = .001) and follow-up assessments (P = .001) compared with the baseline values. No significant change in cervical side flexion ROM was noticed in the control group over time (P > .05). Moreover, no significant time-by-group interaction, group, or time effects were detected for the cervical rotation ROM outcomes (P > .05; Table 3).
Multivariate analysis also revealed no significant time-by-group interaction, time, or group effects for the shoulder flexion and horizontal flexion ROM outcomes (P > .05). However, further analysis using paired t tests with Bonferroni correction showed that the shoulder flexion ROM decreased significantly from the mid-intervention assessment to the follow-up assessment in the no-training control group (P = .003). No significant deterioration in shoulder ROM was observed in the TC Qigong group over time (P > .05; Table 3).
Regarding mouth opening capacity, again no significant time-by-group interaction, time, or group effects were found (P > .05). Further analysis using independent t tests showed that excluding the between-group comparisons at baseline, a significant difference in mouth opening capacity at posttest only was found between the 2 groups (P = .039). Specifically, the TC Qigong–trained participants had 13.3% less mandibular depression than the untrained participants. Mouth opening capacity also decreased from mid-intervention test to posttest (P = .001) in the TC Qigong group. However, even more severe deterioration was observed in the control group. In the control group, the participants’ mouth opening capacity dropped significantly from pretest to mid-intervention test (P = .004), posttest (P = .001), and follow-up test (P = .003; Table 3). Therefore, the deterioration in mouth-opening capacity appears to have been less severe in the TC Qigong group (P = .181) than in the control group (P < .001) over time.
Changes in Sleep Problems
Multivariate analysis revealed that the time-by-group interaction effect (P = .410) and the group effect (P = .615) were not significant in the 9-item sleep problems index. However, the time effect was significant (P = .037). Post hoc paired t tests with Bonferroni correction revealed a significant decrease in the 9-item sleep problems index between the mid-intervention and follow-up tests (P = .006), and between posttest and the follow-up test (P = .007) in the TC Qigong group. No significant change in this index was observed in the control group over time (P > .05; Table 3). These results indicated that sleep problems in general decreased during the 6-month post–TC Qigong intervention period.
For the sleep disturbance score, there were significant time-by-group interaction (P = .049) and time effects (P = .035), but the group effect was not statistically significant (P = .096). The sleep disturbance score obtained at the follow-up test was significantly lower than at the pretest (P = .005) and mid-intervention test (P = .003) values for the TC Qigong participants. The sleep disturbance scores were similar across the 4 assessment time points in the control group (P > .05). The sleep disturbance scores in the TC Qigong group were 36.1% (P = .047) and 44.3% (P = .019) lower than those in the control at posttest and follow-up test, respectively (Table 3). Overall, our results indicate that at least 6 months of TC Qigong training reduced sleep disturbance, and that this effect was most profound during the post–TC Qigong training period.
Relationship Between Joint Mobility and Sleep Problems
Because only the bilateral cervical side flexion ranges of motion demonstrated significant improvement after TC Qigong training, these 2 outcomes were correlated with the 9-item sleep problems index and sleep disturbance scores at posttest and follow-up test. The results revealed that cervical right side flexion ROM was significantly associated with the sleep disturbance score at posttest (r = −0.734, P < .001) and follow-up test (r = −0.534, P = .007). The cervical left side flexion ROM was also significantly correlated with the 9-item sleep problems index at follow-up (r = −0.533, P = .007; Table 4).
Correlations Between the Cervical Side Flexion Ranges of Motion and MOS Sleep Scale–Derived Scores in the TC Qigong Group at the Posttest and Follow-up Test Periods.
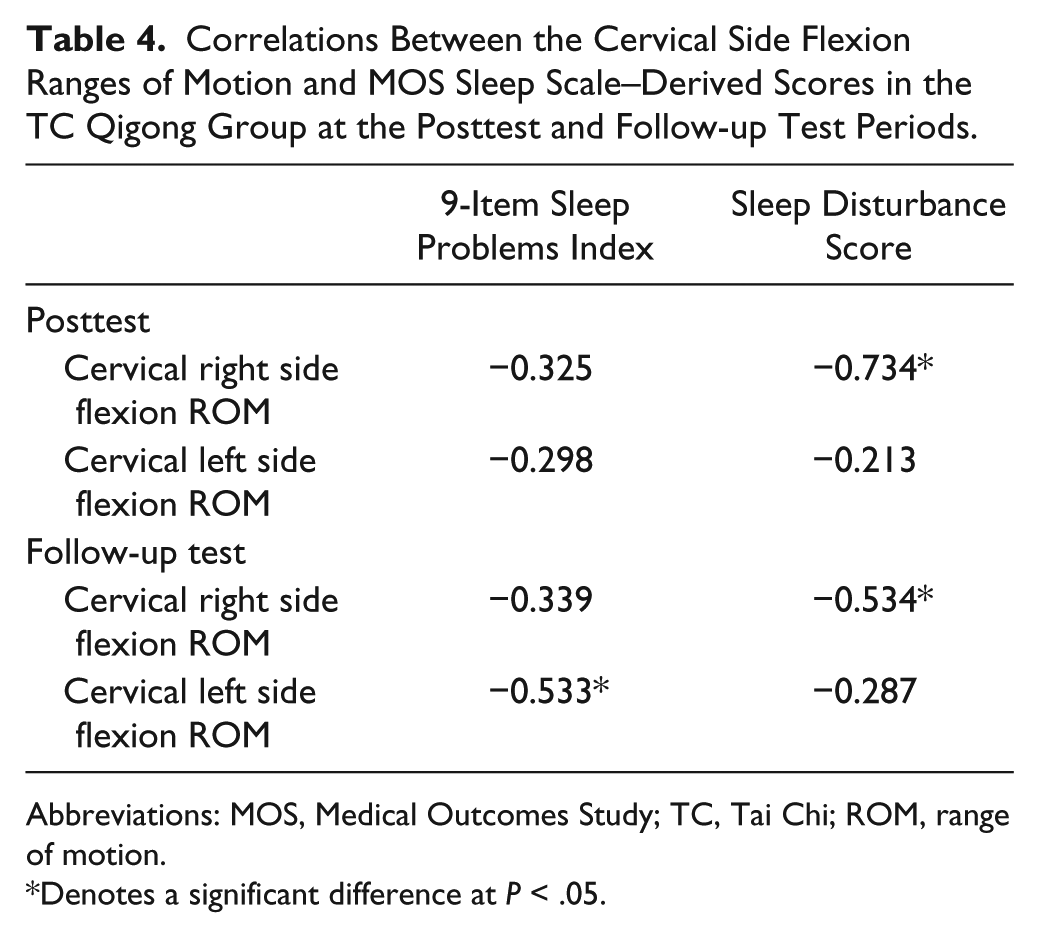
Abbreviations: MOS, Medical Outcomes Study; TC, Tai Chi; ROM, range of motion.
Denotes a significant difference at P < .05.
Discussion
This pilot study is the first to report the effects of TC Qigong training on upper body joint mobility and sleep problems for individuals living with the residual negative effects of NPC treatment. Our 6-month NPC-specific TC Qigong training program was safe, achievable and well received by the participants.
Neck muscle and soft tissue fibrosis is one of the most common radiation-induced complications among NPC survivors. It may also limit cervical ranges of motion.4,19 Indeed, the bilateral cervical side flexion ranges of motion of our NPC survivors (average 24° to 33°) were lower than those of healthy individuals (normal 45°) 19 at baseline. We observed a differential increase in cervical right side flexion ROM, starting from the 3rd month until the 12th month in the participants who undertook the TC Qigong training regime. A similar trend was also observed in the cervical left side flexion ROM, although it was not statistically significant with respect to the sample size (Table 3). This phenomenon can be explained by the fact that our TC Qigong training program included stretching postures and movements that may improve cervical side flexion mobility. For example, the “painting a rainbow from side to side” and “ear stimulation” exercises required the practitioners to slowly stretch their bilateral neck side flexors (the scalene muscles and upper trapezius) repeatedly. In addition, the amount of TC Qigong training was sufficient for improving flexibility (3-4 days per week; 1.5 hours of repeated slow stretching exercises per session) according to the American College of Sports Medicine guidelines. 28
Although neck stretching exercises were included in our TC Qigong program, no improvement in cervical rotation ROM was found in the participants after TC Qigong training (Table 3). This finding is consistent with Lansinger et al 12 who reported no improvement in cervical rotation ROM after 3 months of medical Qigong intervention in patients with chronic neck pain. However, rather than proving that TC/Qigong is ineffective, the findings in both studies are because of the fact that the participants had already achieved full cervical rotation range at baseline (Table 3). Another study showed that it was not possible to go beyond the cervical rotation physiological limit of motion (60°) 19 with further Qigong training.
Our results revealed that the shoulder range of motion in the forward flexion and horizontal flexion directions remained unchanged over time in the TC Qigong group. This finding is consistent with one of our previous studies, which showed that TC Qigong training might not be able to improve shoulder mobility in breast cancer survivors. 29 Moreover, as 24 of the 25 participants in the TC Qigong group did not undergo surgery following radiotherapy and chemotherapy, their shoulder mobility was by and large intact. 30 Accordingly, the TC Qigong training appeared to provide no additional benefit to the participants’ normal shoulder ranges of motion. Interestingly, we observed a slight deterioration in shoulder flexion ROM in the control group from the 3rd month to the 12th month within the study period. We postulated that this might be due to aging or a latent effect of radiotherapy on the muscles and soft tissues surrounding the joint.4,31 Further investigation is necessary to understand the exact causes of this phenomenon.
Trismus is a common problem in NPC survivors and is associated with reduced nutrition, speaking difficulty and compromised oral hygiene. 5 To the best of our knowledge, our study is the first to show that TC Qigong training was able to attenuate the deterioration in mouth opening capacity among NPC survivors. The participants that did not undergo TC Qigong training demonstrated a dramatic decrease in interincisor distance over the 12-month study period (Table 3). Our findings concur with those of Tang et al 6 who reported that trismus progressed quickly in NPC patients if no rehabilitation was received. They found that therapeutic exercises (TMJ active ROM exercises) prevented the progression of trismus in NPC patients after radiotherapy. 6 Our TC Qigong program included TMJ active ROM exercises that were similar to the rehabilitation regime used by Tang et al. 6 As expected, we found that trismus progressed much more slowly in the TC Qigong group than in the control group (Table 3).
The exact mechanisms of the therapeutic effect of TC Qigong training in alleviating trismus are not fully understood. Possible mechanisms include (1) ROM exercises increase TMJ mobility and improve the flexibility and elasticity of the connective tissues surrounding the joint 6 and (2) TC Qigong training improves blood circulation and decreases the local inflammatory response.6,32,33 Certainly, further research is needed to confirm these hypotheses.
We observed that sleep problems, such as sleep disturbance, sleep duration inadequacy, respiratory impairment and somnolence, decreased 6 months after the NPC survivors stopped TC Qigong training. In particular, sleep disturbance started to decrease after 6 months of the TC Qigong training and continued to decrease during the no-training follow-up period. The TC Qigong–trained participants experienced less sleep disturbance than the controls at posttest and follow-up test (Table 3). Our findings are consistent with a previous study that showed that short-term Qigong training enhanced sleep duration. 14 However, as the Qigong training period in the previous study was very short (1 month), changes were not found in sleep disturbance, sleep quality, sleep latency, and habitual sleep efficiency before and after the Qigong training. 14 Our results demonstrate that at least 6 months of TC Qigong training is needed to reduce sleep problems. Moreover, the participants’ sleep problems continued to decrease after the termination of TC Qigong training because some of the participants continued to practice TC Qigong at home after the assigned training period. Although this may have confounded the follow-up test results and is an apparent limitation of the study, this finding suggests that longer term TC Qigong training may further benefit NPC survivors in terms of quality and quantity of sleep.
Sleep experts have proposed several mechanisms to explain the sleep-promoting effects of exercise, which may apply in TC Qigong training. First, exercise-induced body temperature elevation can activate both heat loss and the associated sleep mechanisms. 34 Second, sleep duration increases as a function of increased energy expenditure during exercise.35,36 Third, exercise increases electroencephalographic delta power and thus overall sleep quality. 37 Finally, we found that TC Qigong, a type of mind–body exercise, was able to improve the cervical side flexion ranges of motion, which have been associated with reduced sleep problems (Table 4). This is the first study to demonstrate this link in relation to NPC survivors. It may be that the improved cervical side flexion range enables NPC survivors to achieve better head and neck inclination in side lying posture, especially when the pillow is too thick or thin. 38 Further kinematic and kinetic measurements are required to substantiate this hypothesis.
A major limitation of this study is that the group allocation was not randomized. Therefore, subject self-selection bias may be present. For example, the participants who chose to participate in the TC Qigong program may have been more motivated or physically capable. As a result, the observed changes in the outcome parameters may be attributable to the physical or psychological characteristics of the participants rather that the direct effects of the intervention itself. 27 In addition, due to ethical reasons, both groups of participants can continue to receive hospital care that may not be identical during the study period. This may confound the results of the study. Another limitation of this study is the high total attrition rate, especially in the TC Qigong group. Intention-to-treat analysis (last observation carried forward) was used, which may explain the nonsignificant changes in some of the outcomes over time. Further studies may consider adopting a randomized, controlled, crossover design with an adequate washout period. 27 Moreover, as aggressive cancer treatments have numerous adverse effects of different severities, further research is needed to determine the clinical efficacy of TC Qigong training in alleviating other side effects, such as different degrees of xerostomia, joint and eating and speech dysfunctions, thereby improving the quality of life of NPC survivors. 39
Conclusions
This 6-month TC Qigong intervention aimed to maintain or improve temporomandibular, cervical, and shoulder joint mobility and reduce sleep problems among NPC survivors experiencing the residual side effects of conventional cancer treatment. Our study produced some promising results. The beneficial effects of TC Qigong lasted for 6 months after the cessation of training. Clinicians may therefore wish to suggest TC Qigong as a therapeutic exercise for this particular group of clients.
Footnotes
Acknowledgements
The authors are grateful to the Mutual Aid Association for their kind assistance in recruiting the participants and the Nature Health Qigong Association for providing TC Qigong training for the participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Seed Fund for Basic Research for New Staff from the University of Hong Kong (201308159012) and an Internal Research Grant from the Hong Kong Institute of Education (RG57/2012-2013R).