
Abstract
Introduction. Many breast cancer patients and survivors experience pain and emotional stress related to their disease, its diagnostic procedures, or treatment. Hypnosis has long been used for the treatment of such symptoms. The aim of this review was to systematically assess the effectiveness of hypnosis in women with breast cancer, breast cancer survivors, and in women undergoing diagnostic breast biopsy. Methods. PubMed, Scopus, the Cochrane Library, PsycINFO, and CAMBASE were screened through February 2014 for randomized controlled trials (RCTs) of hypnosis in women with breast cancer or undergoing diagnostic breast biopsy. RCTs on postmenopausal women without a history of breast cancer were also eligible. Primary outcomes were pain, distress, fatigue, nausea/vomiting, and hot flashes. Safety was defined as secondary outcome measure. Risk of bias was assessed by 2 reviewers independently using the Cochrane Risk of Bias Tool. Results. Thirteen RCTs with 1357 patients were included. In women undergoing diagnostic breast biopsy (3 RCTs), hypnosis positively influenced pain and distress; 1 RCT on breast cancer surgery found effects of hypnosis on pain, distress, fatigue, and nausea. For women undergoing radiotherapy (3 RCTs), hypnosis combined with cognitive–behavioral therapy improved distress and fatigue. In 3 RCTs on women with and without a history of breast cancer experiencing hot flashes, hypnosis improved hot flashes and distress. Three RCTs on women with metastatic breast cancer found effects on pain and distress. Conclusions. This systematic review found sparse but promising evidence for the effectiveness of hypnosis in breast cancer care. While more research is needed to underpin these results, hypnosis can be considered as an ancillary intervention in the management of breast cancer–related symptoms.
Introduction
With more than 1.6 million new cases in 2012, breast cancer is the most frequent cancer in women worldwide. Twenty-five percent of all female cancer cases were diagnosed with breast cancer. 1 Due to improved diagnosis and treatment, there is a continuous increase in survival rates. 2 However, invasive diagnostic procedures and anticancer treatment are often associated with serious side effects. Breast biopsy, lumpectomy, and mastectomy often induce psychological distress, pain, and, mainly due to anesthesia, nausea and vomiting.3-7 Chemotherapeutic and radiotherapeutic breast cancer treatment are strongly associated with psychological distress, fatigue, and, in the case of chemotherapy, nausea and vomiting.8-10 Substantial psychological distress is present in 1 out of every 3 breast cancer patients.10-12 These symptoms often persist for years after completion of treatment.11,12 Moreover, many breast cancer survivors experience hot flashes as a result of chemotherapeutic and/or antihormonal treatment. 13 Besides personal grief, some of these symptoms can prolong hospital stay and thereby increase costs of medical care. 14 Management of symptoms related to breast cancer, its diagnostic procedures, and treatment is therefore gaining increased importance.
Hypnosis includes the use of suggestions for alterations in perception, sensation, emotion, thought, or behavior. 15 The suggestions used in hypnosis can be direct or permissive. 16 Hypnosis has long been utilized in medical settings for the control of pain and distress. 17 Suggestions for control of pain and its related distress mostly ask patients to transform the perception of pain and to disentangle the somatic sensation of pain from its emotional components. 17 Accordingly, it has been found that hypnosis can reduce both clinical and experimental pain. 18 It has also been suggested that hypnosis might be useful in reducing chemotherapy-related side effects such as anticipatory nausea and vomiting by reducing conditioning effects and treatment-related distress. 19 A mediator that has been shown to play a role in the effects of hypnosis on breast cancer–related issues 20 are response expectancies, that is, expectancies for the occurrence of nonvolitional responses, such as pain, nausea, or anxiety. Hypnotic response expectancies are related to the belief that one is capable of experiencing a suggested effect. 21
The aim of this review was to systematically assess the effectiveness of hypnosis in women with breast cancer, breast cancer survivors, and in women undergoing diagnostic breast biopsy.
Methods
PRISMA guidelines for systematic reviews and meta-analyses 22 and the recommendations of the Cochrane Collaboration 23 were followed.
Literature Search
PubMed/Medline, the Cochrane Library, Scopus, CAMBASE, and PsycINFO were searched from their inception until February 25, 2014, without language restrictions. The complete search strategy for Medline was as follows: (breast[MeSH Terms] OR “breast neoplasms”[MeSH Terms] OR “breast cancer” [Title/Abstract] OR breast[Title/Abstract]) AND (hypnosis [MeSH Terms] OR hypnosis[Title/Abstract] OR hypnotherapy[Title/Abstract]). The search strategy was adapted for each database as necessary. Additionally, reference lists of identified original and review articles were searched manually. Abstracts of identified records were screened, and the full articles of potentially eligible studies were read in full by 2 authors to determine whether they met the eligibility criteria.
Eligibility Criteria
To be eligible, studies had to meet the following criteria:
Types of studies. Randomized controlled trials (RCTs) were eligible. Studies were eligible only if they were published as a full article.
Types of participants. Studies of adult (older than 18 years) women with breast cancer, breast cancer survivors, and women who were undergoing diagnostic breast biopsy were eligible. Given that effects of therapeutic interventions for hot flashes are comparable in women with and without a history of breast cancer, it was post hoc decided to also include studies on postmenopausal women with hot flashes without prior breast cancer.
Types of interventions. Studies that compared hypnosis to standard care, attention control, or any active intervention were eligible. Studies in which hypnosis was combined with other psychological interventions were also eligible but were analyzed separately. Both studies with live administration and taped administration of hypnosis were eligible.
Types of outcomes. Studies were eligible if they assessed pain, distress, fatigue, nausea/vomiting, or hot flashes. Safety was defined as secondary outcome measure.
Data Extraction
Two reviewers independently extracted data on characteristics of the study (eg, trial design, randomization, blinding), characteristics of the patient population (eg, type of diagnostic/therapeutic procedure, sample size, age), characteristics of the intervention and control (eg, type of hypnosis, type of control intervention), outcome measures, and results.
Due to the broad inclusion criteria that were expected to result in a heterogeneous sample of RCTs, a meta-analysis was neither planned nor conducted.
Risk of Bias in Individual Studies
Risk of bias was assessed by 2 reviewers independently. The criteria recommended in the Cochrane Risk of Bias Tool were used. 23 This tool assesses risk of bias on the following domains: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other bias (rated as low risk, high risk, or unclear). Discrepancies were rechecked with a third reviewer and consensus achieved by discussion.
Results
Literature Search
Three hundred and thirty-three records were retrieved in literature search, and 16 full-text articles were assessed for eligibility25-40 (Figure 1). Two articles were excluded because they included women undergoing elective breast surgery.25,26 Another article was excluded because it was not randomized. 27 Thirteen RCTs with a total of 1357 patients were included in the review.28-40
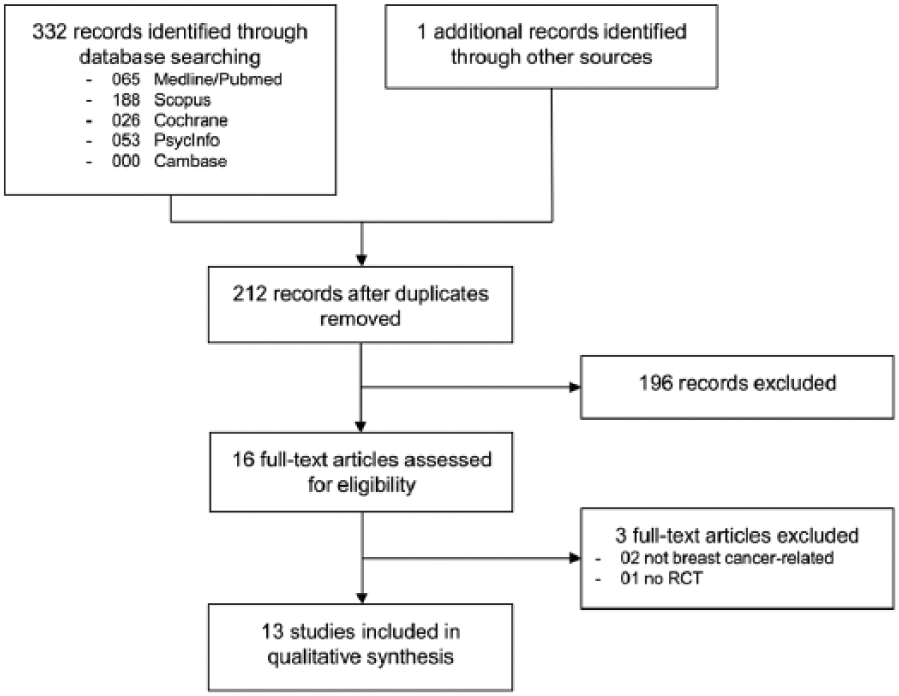
Flowchart of the results of the literature search.
Study Characteristics
Characteristics of the sample, interventions, outcome measures, and results are shown in Table 1.
Characteristics of the Included Studies.
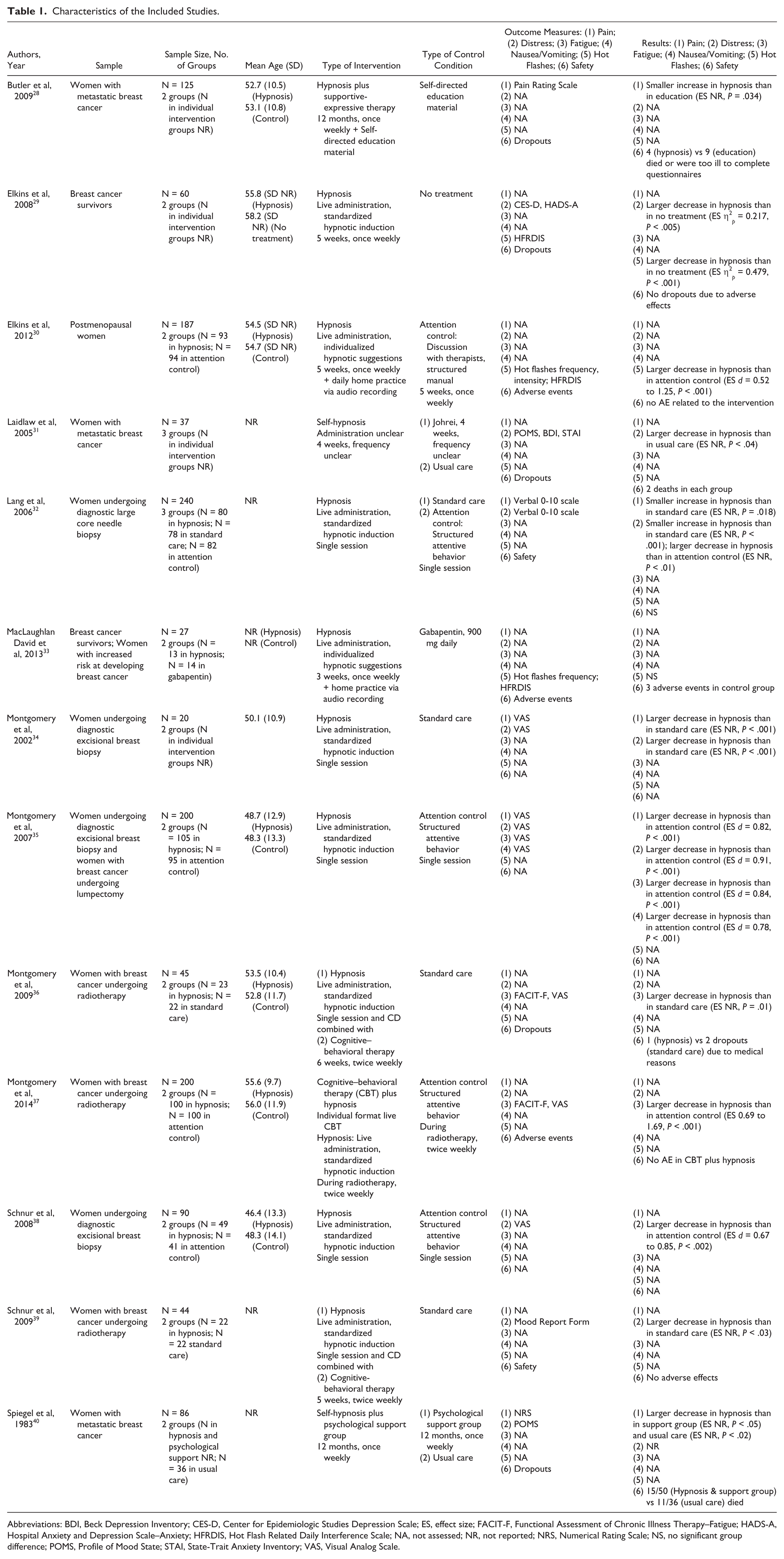
Abbreviations: BDI, Beck Depression Inventory; CES-D, Center for Epidemiologic Studies Depression Scale; ES, effect size; FACIT-F, Functional Assessment of Chronic Illness Therapy–Fatigue; HADS-A, Hospital Anxiety and Depression Scale–Anxiety; HFRDIS, Hot Flash Related Daily Interference Scale; NA, not assessed; NR, not reported; NRS, Numerical Rating Scale; NS, no significant group difference; POMS, Profile of Mood State; STAI, State-Trait Anxiety Inventory; VAS, Visual Analog Scale.
Setting and Participant Characteristics
All included RCTs except one 31 were conducted in the United States. Patients were recruited from large medical centers or community oncologists. Four studies included women who were referred to diagnostic image-guided large core needle biopsy 32 or excisional biopsy.34,35,38 One of those studies also included women with breast cancer who underwent lumpectomy. 35 Three studies included patients undergoing breast cancer radiotherapy36,37,39; 2 studies included women with metastatic breast cancer28,40; 2 studies included breast cancer survivors experiencing hot flashes29,33; and 1 study included women without a history of breast cancer who experienced hot flashes. 30 Patients’ mean age ranged from 46.4 to 58.2 years.
Intervention Characteristics
All studies used live administered standardized hypnotic procedures. Suggestions mainly addressed relaxation, imagery, and symptom control. All interventions also included guidance for self-hypnosis. One study provided the full script used for intervention as appendix. 32 Seven studies used single intervention sessions.32-39 Six of those studies reported length of the intervention.34-39 Median intervention length was 15 minutes (range = 10-15 minutes). Three studies also included cognitive–behavioral therapy sessions.36,37,39 The 3 studies on women experiencing hot flashes used multiple sessions.29,30,33 Over a period of 3 to 5 (median = 5) weeks, 1 weekly 50 to 60 (median = 50)-minute session was offered. Two studies on metastatic breast cancer combined hypnosis or self-hypnosis with support groups. Over a period of 12 months, 1 weekly 90-minute session of hypnosis and group support was offered.28,40 The third study on metastatic breast cancer used self-hypnosis over a period of 4 weeks. 31 Hypnosis was administered by clinical psychologists,28,29,34,36,38 counsellors, 40 students, 32 or physicians.28,32,40
Ten studies had 1 control arm28-30,33-39 and 3 studies had 2 control arms.31,32,40 Six studies compared hypnosis to standard care or no treatment.29,32,34,36,39,40 Five studies compared hypnosis to a standardized attention control condition.30,32,34,37 For attention control, empathic attentive behaviors without specific interventions were used. Attention control was matched for time length in all 5 studies. One study each compared hypnosis combined with support groups to self-directed education 28 or support groups alone. 40 One study compared self-hypnosis to Johrei, a Japanese visualization technique 31 ; and 1 study compared hypnosis to Gabapentin. 33
Outcome Measures
Pain was assessed in 5 studies, using a verbal rating scale, 32 a numerical rating scale, 40 a visual analog scale,34,36 or the pain rating scale. 28 Eight studies assessed distress, using a verbal rating scale, 32 visual analog scale,34,35,38 the Mood Report Form, 39 the Center for Epidemiologic Studies Depression Scale, 29 the Hospital Anxiety and Depression Scale, 29 the Profile of Moods States,31,40 the Beck Depression Inventory, 31 or the State-Trait Anxiety Inventory. 31 Two studies assessed fatigue using the Functional Assessment of Chronic Illness Therapy–Fatigue and daily visual analog scales36,37; 1 study used a visual analog scale to study nausea 35 ; and 3 studies studied hot flashes using the Hot Flash Related Daily Interference Scale,29,30,33 diaries,30,33 and/or objective measures (a skin conductance monitoring system). 30 Adverse events were reported by 5 studies.30,32,33,37,39 Four further studies reported health reasons for dropouts.28,29,31,40
Risk of Bias in Individual Studies
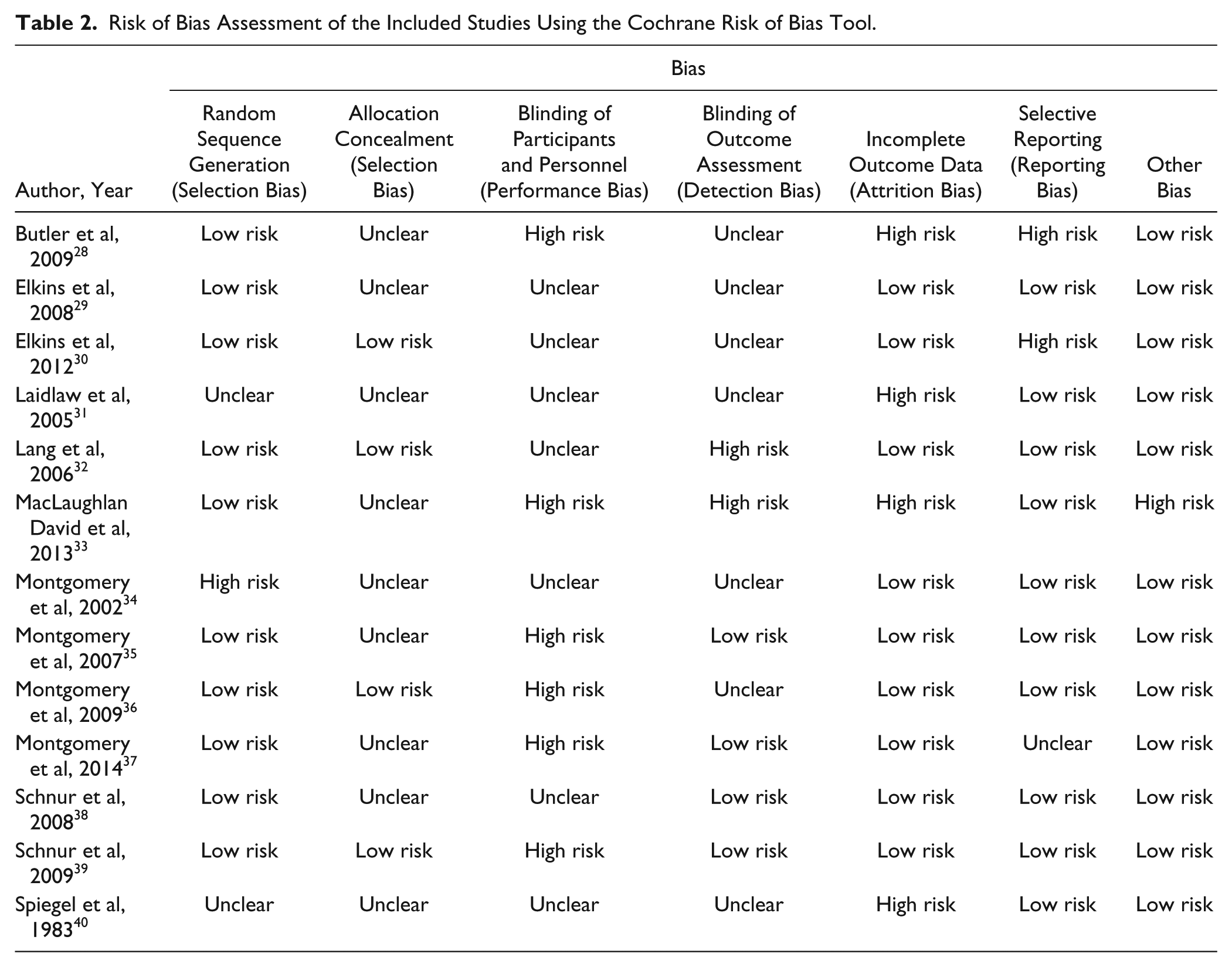
Overall, most included studies had low risk of bias. Randomization was adequate in all but 3 studies in which group allocation was based on day of surgery 34 or unclear.31,40 Only 3 studies reported adequate allocation concealment32,36,39 (Table 2). No study reported blinding of patients or care providers, but 4 studies reported adequate blinding of outcome assessors.34,38,39 Risk of attention bias was low in all studies but those on metastatic breast cancer that reported high rates of health-related dropouts.28,31,40
Risk of Bias Assessment of the Included Studies Using the Cochrane Risk of Bias Tool.
Outcomes
Women Undergoing Diagnostic Breast Biopsy
Four RCTs reported reduced pre-, 38 peri-, 32 or postoperative34,35 pain intensity and psychological distress after preoperative hypnosis compared to attention control. Decreased postoperative pain and psychological distress compared to standard care was reported in 1 RCT. 36 One study reported safety data. 32 This study reported 3 adverse events in the hypnosis group (all hematomas) compared to 7 adverse events in the standard care group and 11 adverse events in the attention control groups. Differences in proportions were insignificant.
Women With Breast Cancer Undergoing Breast Cancer Surgery
An RCT assessed the effects of preoperative hypnosis on postoperative pain, distress, fatigue, nausea, and vomiting. 36 Hypnosis induced a significantly greater reduction on all variables compared to attention control.
Women With Breast Cancer Undergoing Radiotherapy
One RCT reported significant effects of hypnosis combined with cognitive–behavioral therapy on psychological distress 39 ; and 2 RCTs on fatigue34,37 associated with radiotherapy. One RCT reported that no serious adverse events occurred 39 ; another RCT reported that no adverse events related to hypnosis combined with cognitive–behavioral therapy occurred. 38
Women With and Without a History of Breast Cancer Experiencing Hot Flashes
Two RCTs assessed psychological distress and hot flashes in breast cancer survivors.29,33 Compared to no treatment, depression, anxiety, and hot flashes significantly decreased after hypnosis. 29 Compared to Gabapentin, no group differences were found regarding number and severity of hot flashes, and hot flash–related interference. 31 While adverse events were not reported in total in 1 RCT, no patients in either group dropped out of the study due to adverse events (27). In the other RCT, no patient reported hypnosis-related adverse events while 2 patients dropped out due to side effects in the Gabapentin group. 33 A third RCT assessed hot flashes in postmenopausal women without a history of breast cancer. Compared to attention control, hypnosis reduced subjectively and objectively measured hot flash frequency, hot flash severity, and hot flash–related interference. 30 Twenty-five minor adverse events were reported but none of them was associated with the interventions. 30
Women With Metastatic Breast Cancer
Two RCTs reported significant effects on pain in women with metastatic breast cancer.28,40 While both RCTs combined hypnosis with supportive group therapy, in one of them this intervention was more effective than supportive group therapy alone. 40 A third RCT reported effects of hypnosis compared to no treatment on distress. 31 All 3 studies reported health-related dropouts. The number of dropouts due to death or illness was comparable between groups in one study, 31 higher in the hypnosis group in one study, 40 and lower in the third study. 28
Discussion
This systematic review found evidence for reduced pain and distress associated with diagnostic breast biopsy and for reduced pain, distress, fatigue, and nausea associated with breast cancer surgery after preoperative hypnosis compared to attention control; for effects of hypnosis combined with cognitive–behavioral therapy on radiotherapy-associated distress and fatigue in women with breast cancer; for effects on hot flashes in women with and without a history of breast cancer experiencing hot flashes; and for effects of hypnosis—either alone or combined with supportive group therapy—on pain and distress in women with metastatic breast cancer. No studies on effects in women with breast cancer during chemotherapy could be located. The available safety data suggest no differences in adverse events between intervention and control groups. However, future RCTs should ensure more rigorous reporting of safety data.
Agreements With Prior Systematic Reviews
This is the first systematic review on hypnosis for symptoms related to breast cancer, its diagnostic procedures, or treatment. The results of this review are partly in line with previous reviews on hypnosis in related patient samples.41-43 A qualitative review on hypnotic analgesia in adults included 2 studies on breast biopsy or cancer surgery and found effects on pain and distress. 43 A meta-analysis on hypnosis for surgery patients concluded that hypnosis can decrease negative affect and pain. 41 A more recent meta-analysis on hypnosis in various medical procedures found large effects on distress. 42 A systematic review on hypnosis for the management of chemotherapy-related side effects has concluded, mainly based on pediatric patients, that hypnosis can reduce chemotherapy-related nausea and vomiting. 44 This finding has not yet been replicated in women with breast cancer. No reviews on the effects of hypnosis during radiotherapy, in women with metastatic cancer, or cancer survivors could be located.
External and Internal Validity
All included studies were conducted in US medical centers. Patients were mainly Caucasians, but members of ethnic minorities were also included in all studies. Four studies included patients undergoing diagnostic surgery; however, only one study also included patients undergoing therapeutic surgery. Two studies included patients undergoing radiotherapy, 2 studies included breast cancer survivors, and 3 studies included women with metastatic breast cancer. Given that effects of therapeutic interventions for hot flashes are comparable in women with and without a history of breast cancer, 45 it was post hoc decided to also include studies on postmenopausal women with hot flashes without prior breast cancer.
The results of this review are applicable to a considerable number of women with metastatic breast cancer, women experiencing hot flashes, and women undergoing diagnostic breast biopsy or radiotherapy in clinical practice although the limited number of available studies precludes definite conclusions on applicability. External validity is limited for patients undergoing therapeutic breast cancer surgery and for breast cancer survivors.
Overall, most included studies had low risk of bias. However, allocation concealment was unclear in 7 studies,28,29,31,34,35,38,40 and randomization was inadequate or unclear in 3 studies.31,34,40 Blinding of outcome assessors was adequate in 4 studies. Blinding patients or care providers in hypnosis studies might not be possible at all. Therefore, internal validity of the results might be judged acceptable.
Strengths and Weaknesses
This is the first available systematic review on hypnosis for symptoms related to breast cancer and its diagnostic or therapeutic procedures. Patients undergoing a wide range of different diagnostic or therapeutic procedures as well as women with metastatic breast cancer and breast cancer survivors were included. Overall risk of bias was mainly low. Hypnosis interventions and control conditions were comparable at least for studies on patients undergoing breast biopsy and radiotherapy, thus reducing heterogeneity of analyses.
The primary limitation of this review is the small total number of eligible RCTs. Especially the results for patients undergoing breast cancer surgery and breast cancer survivors rely on single studies and should be regarded as very preliminary. Hypnosis was combined with cognitive–behavioral therapy in both trials in patients undergoing radiotherapy. Therefore, the specific effects of hypnosis and cognitive–behavioral therapy in this patient population could not be assessed. While hypnosis did not seem to be associated with severe adverse events, more rigorous reporting of safety data is needed in future studies. Hypnosis was compared to no treatment or attention control in most trials. While the results suggest efficacy of hypnotic interventions, head-to head comparisons with other effective psychosocial interventions are still rare.
Implications for Further Research
The included trials give important hints for effects of hypnosis in breast cancer patients in a variety of settings. However, as only very few and heterogeneous RCTs were available, more research is needed. These studies should ensure rigorous methodology and reporting, mainly adequate randomization, allocation concealment, intention-to-treat analysis, and blinding of at least outcome assessors. 46 Especially the effectiveness of hypnosis for breast cancer patients undergoing chemotherapy has not been investigated yet. It would further be interesting to investigate whether hypnosis combined with cognitive–behavioral therapy really is superior to hypnosis alone in patients undergoing radiotherapy, as the authors of those studies suppose.36,38,39 Furthermore, replications of positive RCTs are needed to consolidate the evidence for effects of hypnosis in women undergoing diagnostic breast biopsy, breast cancer surgery, in women with metastatic breast cancer, and breast cancer survivors. Since the findings on effects of hypnosis on hot flashes are based on 2 RCTs in breast cancer survivors29,33 and 1 RCT in women without a history of breast cancer, 30 a large-scale RCT on hot flashes in breast cancer survivors is needed to underpin the positive findings.
Conclusions
While more research is needed to underpin these results, hypnosis can be considered as an ancillary intervention in the management of breast cancer–related symptoms, namely, for women undergoing diagnostic breast biopsy or breast cancer surgery, women with metastatic breast cancer, breast cancer survivors, and postmenopausal women with and without a history of breast cancer experiencing hot flashes. Furthermore, hypnosis combined with cognitive–behavioral therapy could be considered in women undergoing breast cancer radiotherapy.
Footnotes
Authors’ Note
The funding agency did not have any influence on the design or conduct of the review; the collection, management, analysis, or interpretation of the data; or in the preparation, review, or approval of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Rut- and Klaus-Bahlsen Foundation.