
Abstract
Introduction: Tibetan medicine (TM) is a whole systems medical approach that has had growing interest in the West. However, minimal research, particularly with cancer, has been conducted. The purpose of this article is to provide an overview of TM and describe a clinical case review study to obtain preliminary evidence of TM’s safety and effect on patients treated for cancer or hematologic disorders. Methods: A retrospective case review was conducted in India and cases met the following inclusion criteria: (a) confirmed diagnosis of cancer or hematologic disorder by standard Western biomedical diagnostic tests, (b) either treated exclusively with TM or received insufficient Western treatment followed by TM and (c) were in remission or had stable disease at least 2 years after start of TM. Results: Three cases were identified, 1 solid tumor and 2 hematologic diseases: Case 1—poorly to moderately differentiated adenocarcinoma of the stomach, positive lymph nodes and mucosal infiltration, with clear scans and excellent quality of life 29 months later ; Case 2—chronic myelogenous leukemia with normalization of hematologic labs within 3 months of starting TM and stable 4 years later; and Case 3—red cell aplasia improved significantly and reversed dependence on blood transfusions with TM. None of the cases experienced demonstrable adverse effects from TM. Conclusions: This limited case review found TM to be safe and have positive effects on quality of life and disease regression and remission in patients with cancer and blood disorders. Further exploration and investigation using rigorous methods is warranted.
Introduction
Tibetan medicine has historically existed as a comprehensive public health care system and as a treatment modality of choice particularly for chronic illness throughout Tibetan regions across Asia and the Trans-Himalaya, with origins preceding the seventh century CE. As Tibetan medicine has grown throughout Asia (namely, India, Nepal, Bhutan, Mongolia, and China) and more recently entered Europe and North America, it has gained intrigue for its extensive pharmacology and variety of treatment approaches.1-3 Likewise, with Buddhist religion as a core aspect of Tibetan culture and its value of scientific tradition for establishing validity through inference and evidence, 1 Tibetan medicine demonstrates interdependent causal relations and systematic organization of the body and mind through functional modes. Tibetan medicine tracks negative mental states and emotions and their cascading effects of subtle to gross trajectories that affect the overall functional activities of the mind and body. Such deleterious effects can then be rehabilitated and treated through an integrated whole health approach. Such an approach has provided it with promising potential for collaboration with Western biomedical paradigms and methods. Interest has developed for collaborative research in several areas of chronic illnesses and testing of Tibetan pharmacology.4-16 However, such interest has yet to generate any published results of clinical studies in Western medical journals investigating Tibetan medicine’s efficacy in treating cancer patients. Our intention with this article is to provide a brief overview of Tibetan medicine and describe 3 cancer case studies as a basis to stimulate interest toward future research and collaborative efforts between Western and Tibetan medicine practitioners and researchers.
Overview of Tibetan Medicine
Tibetan medicine is a whole system medical approach that uses a multimodal, individualized patient approach. Through perceptual and investigatory diagnostic methods of Tibetan medicine, patient-oriented medication, individual-specific diet and behavioral interventions, and subtly nuanced therapeutic applications, the Tibetan medical system engages a precise conceptualization of ways to identify, recognize, and treat disease to restore health and balance through a dynamic equilibrium of 3 functional energy systems called nyespas. Its practical potency resides in 2 aspects of the system: (a) a sophisticated conceptualization of function, diagnosis, and treatment that links mind, nutrition, behavior, pharmacology, and accessory therapies in relation to disease etiology and treatment trajectories; and (b) cultivated expertise in the practices of its physicians through diagnostics and patient-specific pharmacology.
Diagnosis
Tibetan medicine employs 3 fundamental diagnostic approaches via touch, observation, and investigative questioning for the complete understanding of the etiology, pathology, and its multidimensional approach to the successful treatment of imbalances of mental and bodily functions. Pulse and urine analysis form its 2 most important diagnostic methods to produce highly specific and subtly discerned diagnoses, with pulse reading including numerous measures extending far beyond a simple pulse rate. Unlike Western medicine (also referred to as “biomedical” or “conventional medicine”), which has relied increasingly on technological diagnostics and less on physical assessment, Tibetan medicine, by contrast, uses the physician’s proper assessment of patient’s body constitution, his or her own expertise in the thorough understanding and interpretation of pulse and urine analysis, and deep observational skills to uncover the underlying causes of the illness and distress. The diagnosis combines interrogation—inquiry into the patient’s medical history, diet, behavior, mental states, social relations, and habits that help confirm the findings of the pulse and urine analysis. Additionally, assessments of the patient’s sensory organs and defects help the physician to further deepen his/her understanding of the disease pattern.
The characteristics assessed in the diagnosis correspond to the 3 systems of functional energies called nyespas that determine the balance and imbalance of the body system and etiologies of the specific patient condition. As such, diagnosis provides a means to illuminate the pathologic trajectories for a given illness and its pathways for healing, formulated in terms of these dynamic functional energetic systems, namely, rlung, mkhrispa, and badkan (pronounced loong, tripa, and baekan, respectively). rLung is connected with variant emotion, stress and tension, and neuroendocrine functions; mkhrispa with metabolic functions, blood and vascular processes, inflammation, some infections, and physiologic thermoregulation; and badkan with mucosal and membranous functions and muscular, fat, and osteopathic conditions. In general, the nyespas, when in balance, help build up and sustain all the physiological and neuropsychological functions of the body and, when in imbalanced condition, manifest different kinds of diseases and pathological conditions.
Treatment
Treatment in Tibetan medicine is individualized and uses multiple modalities, chiefly herbal and mineral-based formulas of pills, powders, decoction, and pastes in combination with advice on diet and lifestyle conditions, mental and spiritual inclinations, and social and environmental factors. In addition, accessory therapies may also be administered as 2 distinct categories: wellness or relaxation therapies and minor invasive interventions. Among many other therapies, the former includes meridian massage, hot and cold fomentation, and medicinal bath, whereas the latter includes moxabustion, venesection, and cupping or vacuum therapies. Moxabustion entails the application and burning of herbs on the skin in relation to various disease-related energy meridians. Venesection involves the application of small cutaneous punctures that “let” impure or diseased blood (ie, blood that exhibits defined characteristics of imbalances in the system that result in illness) at specific disease meridians distinct from those of moxabustion.
In Tibetan medicine, a patient population with similar cancer types may have different specific diagnoses of the underlying pathogenesis depending on their body constitution and the nyespa involved. Therefore, slightly different or additional supporting treatments may be implicated based on their specific constitution, influential factors, and diagnosis. This is similar to a patient-oriented approach of personalized or individualized medicine that is gaining popularity in conventional Western clinical settings. 17
Tibetan Medical Approach to Cancer
The indigenous nosological category in Tibetan medicine 2 that most closely aligns with that of cancer in Western medicine is dre-nay (Tib. ‘bras-nad), which comprises numerous subtypes and levels of aggressiveness in growth. Although dre-nay has different etiologies than the Western medical conception of cancer, for the comparative purposes of this article we will refer to both as “cancer.” The Tibetan medical conception of cancer has deeply rooted associations with what is known as chu-ser 1 and impure blood (T. Dawa, Personal interview, October 2, 2011). Chu-ser in Tibetan medicine, translated literally as “yellow liquid,” comprises the body’s lymph fluid, blood plasma, interstitial fluid, extra- and intracellular fluid, and cerebrospinal fluid. Although serum provides a close correlate, chu-ser comprises a wider scope of the body’s fluids. Improper movement, processing, and metabolism of chu-ser across and within all these associated fluid cavities, pathways, and functions are key elements in the development of cancer from a Tibetan medicine perspective. Likewise, improper blood development and metabolism leading to “impure blood” is also a key element in the Tibetan medical conception of cancer etiology.
The subcategories for cancer in Tibetan medicine correspond to the location of the cancer, vital body organs, and the type of functional energetic systems (nyespa) involved. Eighteen broad types of cancer are classified as sha-dre, rus-dre, and rtsa-dre as part of the outer locations of cancer. Sha-dre refers to muscles and connective tissues, whereas rus-dre refers to skeletal or bone cancer. rTsa are specific, recognized channels in the body that relate to blood vessels, lymph vessels, and nerves, but form a more subtle type that energetically crosses all 3 systems of channels and physiologic pathways. Internal dre-nay includes most of the visceral and hollow organs like lung, heart, liver, spleen, kidney, stomach, intestine, colon, and urinary bladder. For instance, one could have stomach cancer, which is rlung type, mkhrispa type, and/or badkan type. rLung forms of any cancer types or subtypes can be the most aggressive kinds of cancer in the Tibetan nosological system. In this system, breast and uterine cancer are placed as a blood type of cancer. 18 Cancer that results from any chronic injury or wound is known as tson-dre (Tib. Mtshon-’bras), or “injury-derived” cancer. Jae-dre (Tib. Bye-’bras) is likened to a tumor with varying sizes as that of a bird’s egg; it could be hard and round and multiple in its formation, much like lymphadenopathy in Western medicine.
Whereas chu-ser and impure blood described above comprise the proximal causes of cancer in Tibetan medicine, Tibetan medical cancer etiology describes several general causes for cancer development:
Subjecting the body to extreme physical and psychological pressures
Ma-zhu-wa, or chronic disruptions in gut metabolism, digestion, and absorption of food that consequently interferes with proper nutrient extraction and waste disposal processes
Abnormal proliferation of impure blood
Harmful interactions with and from the natural environment
These factors are seen to contribute to the production of abnormal blood cells or blood impurities, which gradually multiply, proliferate, coalesce, and solidify due to an associated aggravation of the rlung functional energy system, or nyespa (T. Dawa, Personal interview, October 2, 2011). It is important to note that although each cancer subtype is strongly influenced by its location, predominant nyespa, individual conditions, host constitution, and rlung aggravation, all cancer types are affected by impure blood, chu-ser, ma-zhu-wa, and all 3 of the nyespas.
Cancer Treatment
Tibetan medical treatments for cancer can be simplified into the following approach: first, breaking down or dissolving the cancer growth; then pacification of the predominant nyespa involved, cleansing necrotic tissues, and reducing inflammation; and finally, healing and rehabilitating the targeted organ in particular and the body system in general. Since blood pathologies are considered an underlying source of cancer etiology in Tibetan medicine, they are similarly treated with venesection at the points nearest to the cancer site (T. Dawa, Personal interview, October 2, 2011). Additionally, pharmacologic formulas for cancer include various compounds that bolster supporting systems of the body (J. Drolma, Project interview, May 23, 2012). The medicine is composed of herbs, precious gems, and minerals that are processed through extensive grinding, sifting, compounding, warming, cooling, and distilling processes.
Tibetan medicine sees infection as a supporting cause of cancer’s development in the body, and thus, Tibetan physicians also administer herbal anti-inflammatory medicines. 16 Because inflammation is associated with body channel (Tib. rtsa) flow in Tibetan medicine, Tibetan physicians also administer medicine that cleanses these channels. Since cancer often results in tumor growth, hot medicinal compression, medicine bath, and, most often, moxabustion are given.
Diet and lifestyle guidance are also seen as an important part of the treatment regimen for cancer. The choice of the diet and lifestyle may depend on the nature of the cancer and the nyespa involved. Timely and appropriate proportion of recommended foods are seen as crucial in boosting the immune system and general well-being of the patient through administering various combinations and amounts of the 6 tastes and 5 cosmo-physical elements. In Tibetan medicine, all food and medicine are considered to have a given degree and profile of all the 6 tastes (sweet, sour, salty, bitter, hot, and astringent) and the 5 cosmo-physical elements (earth, water, fire, wind, and space [Tib. sa, chu, me, rlung, nam mkha’]), which may be understood as that which exhibits the characteristics of solidity, adhesiveness, heat, motility, and vacuous space, respectively. Overconsumption of one or more of the tastes and/or elements leads to imbalance and illness. The proper balanced consumption of the tastes and elements leads to balance, well-being, and health.
Tibetan physicians also focus on constant reassurance and support of patient attitude and outlook, as well as the importance of social connectedness and living in a healthy environment. Healthy environment implies avoiding areas with high toxic loads and conditions of extreme heat, cold, or other environmental stress that may potentially alter the energetic balance of the body system. Adequate sleep and minimal mental stress and strain are also highly recommended for cancer patients, and physicians may refer patients to spiritual teachers and ritual specialists for specific meditations or purifying rituals believed to be beneficial.
Research on Tibetan Medicine
As research on Tibetan medicine is slowly gaining momentum, collaborative studies have been conducted in several areas of chronic illness. 18 Promising findings have been documented in a number of medical conditions including, but not limited to, multiple sclerosis,4,5,11 type 2 diabetes, 6 peripheral vascular disease,7,9 depression, 14 corneal disease, 19 arthritis,10,20 hepatitis B, 13 and hypertension. 20
In terms of cancer, specifically, very little documentation or formal research has been generated in investigating Tibetan medicine’s efficacy in treating cancer. An exhaustive search of the research literature identified only 4 references related to clinical studies in cancer. One opinion paper published in the Journal of the National Cancer Institute in 1999 described anecdotal experience and plans for a clinical trial with advanced breast cancer patients. 21 Two papers were published in India: a review of several cases studies 22 and a single case study of aplastic anemia. 23 A fourth clinical study, though not classically included in Tibetan medical treatment,2,3 evaluated quality of life effects of a 7-week Tibetan yoga program for lymphoma patients and found improvements in sleep quality associated with the intervention. 24 More recently, a few preclinical studies have observed anticancer properties of particular Tibetan herbal compounds and have illuminated potential mechanisms of action from a biomedical perspective.25-27
Safety
Controversy exists over the safety of Tibetan mineral products, namely, “precious pills” often used for cancer and as an “elixir of life,” due to known mercury content—known in Tibetan as tsothel (Tib. btso thal), or “purified mercury extract.” Tibetan medical doctors recognize unpurified mercury as highly poisonous, but create tsothel through extensive processes that “detoxifies” the mercury by binding it to other compounds (eg, sulfides, sulfites, and sulfates) prior to its use in such medications. Toxicology studies are beginning to examine this claim. 28 Pilot research compared data on 11 individuals taking purified mercury-based Tibetan medicine with others taking Tibetan medicine containing no mercury and healthy volunteers. The study showed prolonged ingestion of mercury-containing Tibetan medicine was associated with absent blood levels of mercury, moderate urinary levels (10 µg per day compared to EPA low toxicity levels of less than 20 µg/L) and normal renal and liver function tests that did not differ significantly between groups. 28 Those taking purified mercury-containing Tibetan medicine demonstrated no difference in nonspecific symptoms of mercury toxicity than controls but had more loose teeth and a higher diastolic blood pressure; both findings may have been secondary to the higher age of this group.
Case Studies
Methods
A retrospective case review was conducted. The Research and Development Department of Men-Tsee-Khang (Tibetan Medical and Astro. Institute) in Dharmasala, India initially identified cases that had a cancer-related diagnosis with a positive response to Tibetan medicine. Colleagues from the United States (Emory University and University of Virginia) then thoroughly reviewed the medical records for those that met the following inclusion criteria: (a) confirmed diagnosis of cancer or hematologic disorder by standard Western biomedical diagnostic tests (ie, pathology, laboratory, and radiology reports); (b) either treated exclusively with Tibetan medicine or received inadequate Western treatment (ie, only surgery [without other conventional treatment] followed by Tibetan medicine for stage III or IV solid tumor diagnosis; or insufficient conventional treatment for hematologic disorders [ie, stopping conventional therapies when clinically unstable and/or with active disease]), and (c) in full remission or had stable disease at least 2 years after start of Tibetan medical treatment and without receiving concurrent conventional cancer treatment. Records that were not in English were collaboratively reviewed and translated accordingly. Fifty cases were initially identified by the Tibetan research staff; however, only 3 cases met all of the inclusion criteria. Most were excluded due to inadequate Western biomedical diagnostic documentation.
Diet and Lifestyle
All 3 of the identified cases were given consistent advice regarding diet and lifestyle. They were advised to eat plenty of green leafy vegetables, fresh seasonal local fruits, and vegetable soups; to thoroughly cook or boil food; and to drink several cups of green tea each day. They were also advised to avoid meat and foods that are fatty, raw, cold (refrigerated), sweet, acidic, or leftover for long periods. Regarding lifestyle approaches, they were advised to participate in daily moderate physical exercise such as brisk walking, daily mindfulness meditation or deep breathing exercises for 15 to 30 minutes, and enjoyable hobbies and activities—all intended to alleviate stress, distress, and agitation; attain a peaceful and calm mind; and promote sleep. No documentation on accessory therapies was identified for these cases.
Case 1: Gastric Carcinoma
The first case is a 47-year-old man who, in September 2001, presented with dyspepsia, vomiting, weight loss, elevated white blood cells, high protein in his urine, and a distinct, firm stomach mass. In December 2001, the patient underwent radical distal gastrectomy surgery followed by complications resulting in a temporary tracheotomy.
Diagnosis
Pathology revealed a diagnosis of poorly to moderately differentiated adenocarcinoma of the stomach infiltrating the submucosal and muscular layers. Two out of the 8 lymph nodes tested positive for cancer. Diagnostic stage was determined to be Stage IIIA (T2, N1, M0).
Treatment
Several doctors recommended chemotherapy. Because of the extremely difficult postoperative course, the patient had refused chemotherapy and all other biomedical treatments.
He first saw a Tibetan medical doctor in February 2002, and he received a Tibetan medical diagnosis of stomach cancer (Tib. pho’bras) with badkan as the predominant nyespa and ma-zhu-wa (ie, gastric metabolic disruptions) conditions. He continued only on Tibetan medicine, taking herbal compounds and precious pills for over 20 months with no additional Tibetan medical accessory therapies. He received the following Tibetan compounds: Sangdak Dharyaken, Gawa Chudruk, Dashel Sodhuen, Gurgum Chusum, and Yukar + Khyunga. Dosage and durations of each of these medicines are described in Table 1, and the medicine compound ingredients are described in the appendix. Among the precious pills, the patient took Rinchen Tsodru Dashel and Rinchen Mangjor Chenmo, alternating these on a weekly basis. (Of note, activities of the Tibetan medicines common to all 3 patient cases are listed in the appendix.)
Name of the Tibetan Medicine Prescribed, Number of Doses, Pills per Dose, and Treatment Duration for Case 1 With Gastric Carcinoma.

Clinical Course
Abdominal computed tomography (CT) scans showed no evidence of cancer 29 months later. As of February 2004, 30 months after diagnosis, he described an excellent quality of life. In a note written and signed by the patient (found in his medical record), he stated,
I was in a very serious state surrounded by death from all sides. . . . My weight was down from 76 kg [sic] to 53 kg. Many doctors recommended chemotherapy, otherwise 3 to 6 months to live. . . . I started your [Tibetan] medicine and began improving . . . my weight is now 78 kilograms and all CT scans are clear.
Case 2: Chronic Myelogenous Leukemia
The second case is a 27-year-old man who, in May 2007, presented at the Tibetan medical branch clinic with high persistent fever, nausea, weakness, abdominal swelling with a hard mass, and emaciation. He had both an enlarged spleen and liver, and laboratory tests revealed a total white blood cell count of 149 000/µL (normal is 4500-10 000) and hemoglobin level of 10.8 g/dL (normal for men is 13.5-17.5).
Diagnosis
Six months prior to arriving at the Tibetan medical clinic, in November 2006, he had received a diagnosis of chronic myelogenous leukemia. A reverse transcriptase polymerase chain reaction assay had confirmed a “Philadelphia” chromosome (translocation of chromosomes 7 and 22). Physical exam identified splenomegaly and hepatomegaly. At the time of diagnosis, his white blood count was 125 000.
Treatment
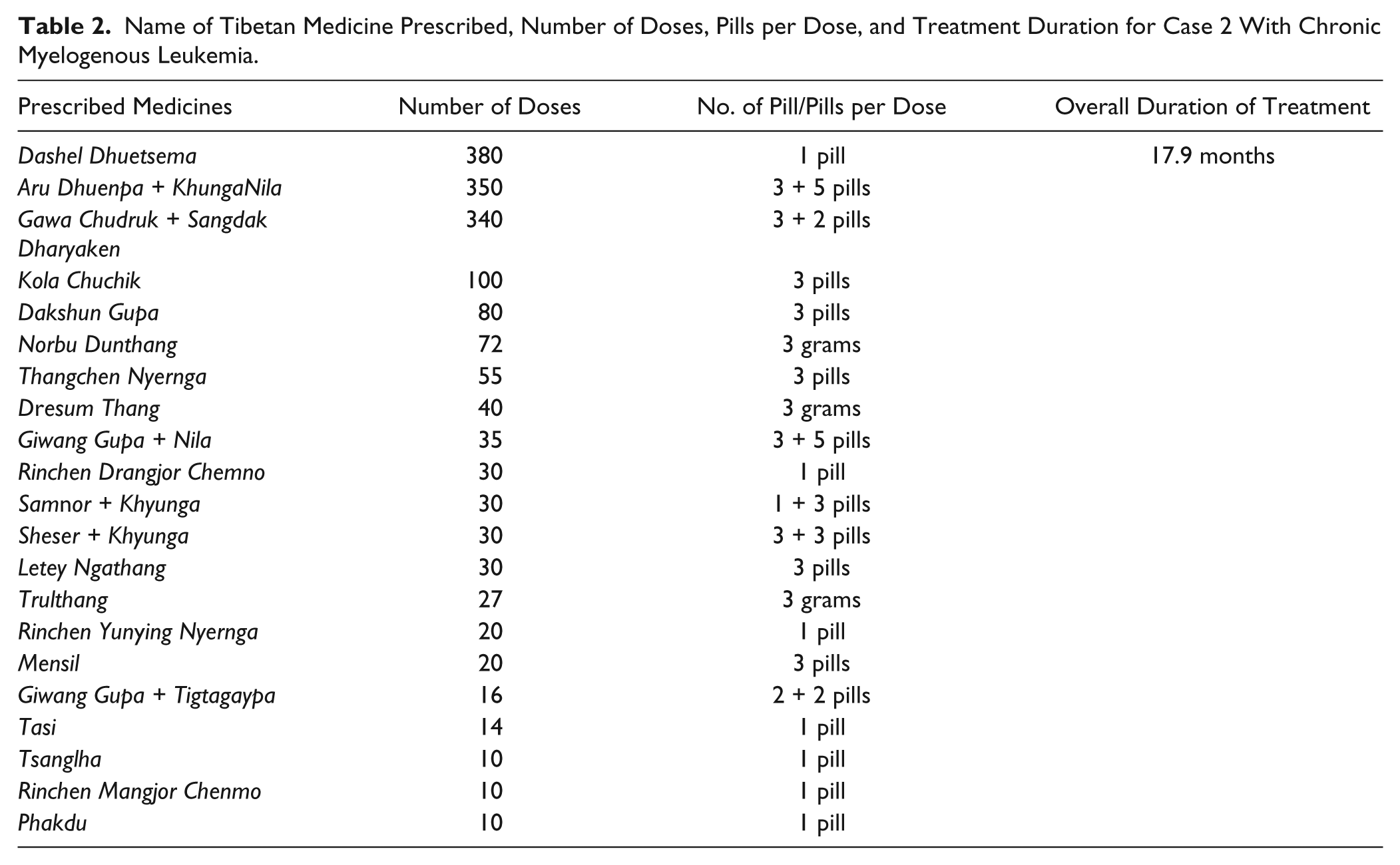
After a Tibetan medical diagnosis of mkhrispa-dominated blood cancer (Tib. khrag ‘bras), he began Tibetan medical treatments on May 29, 2007. He did not receive any Western medical treatment prior to beginning the Tibetan regimen: Dashel Duestsema + Dagshun Gupa, Gawa Chudruk + Sangdak, Aru Dhunpa + Khyunga, Giwang Gupa + Khyumngya, Mensil, Thangchen Nyernga, Dresum Thang, and Pangtzi Chunyi. Among the precious pills, he took Rinchen Drangjor Chenmo and Rinchen Mangjor Chenmo on a weekly basis. The detailed list of the prescribed Tibetan medicines with their varying number of doses and treatment durations is documented in Table 2.
Name of Tibetan Medicine Prescribed, Number of Doses, Pills per Dose, and Treatment Duration for Case 2 With Chronic Myelogenous Leukemia.
Clinical Course
Within 3 months of starting Tibetan medicine, both his white blood cell count and hemoglobin levels were in normal range. He received Tibetan medicine exclusively. Figures 1 and 2 track these laboratory values over time. In short, his white blood cell count had decreased from 149 000 to 8300, and hemoglobin went from 10.5 to 15.0 within weeks of starting the Tibetan medical treatments. Four years after he began treatment, his white blood cell counts and hemoglobin levels were still stable at 5700 and 14.4, respectively. Presently, the patient is still continuing the Tibetan medication, without any complications, and continuing to lead a healthy and productive life.

Hemoglobin levels (g/dL) for Case 2, 27-year-old male, with chronic myeloid leukemia, 4 times over 4 years with the first one taken immediately prior to the initiation of Tibetan medicine (normal values for men are 13.8-18.0 g/dL).

Total white blood cell counts (x103/µL) for Case 2, 27-year-old male, with chronic myeloid leukemia. Four time points over 4 years with the first one taken immediately prior to the initiation of Tibetan medicine (normal values are 3.6-11.0 x103/µL).
Case 3: Red Cell Aplasia
The third case, a 37-year-old man, had dangerously low hemoglobin levels requiring frequent blood transfusions.
Diagnosis
In September 1997, he was diagnosed with red cell aplasia, possibly associated with a myelodysplastic syndrome.
Clinical Course
His hemoglobin levels continued to drop necessitating more frequent (at least weekly) transfusions. In India, he was advised to have a bone marrow transplant, but a donor match could not be found. He then went to the National Institutes of Health in the United States, but was not eligible for a clinical trial. He returned to India and began cyclosporine, prescribed by a hematologist. After 6 months of taking cyclosporine, his blood sugar was at 500 mg fasting and 750 postprandial, and he became insulin-dependent. Throughout the 2-year period of receiving cyclosporine, he continued to need frequent red cell transfusions and also remained on insulin.
While in the waiting area of his hematologist, he heard about Tibetan medicine—that someone’s brother was “taking it and doing very well.” He was then inspired to try Tibetan medical treatment and started it (and immediately stopped cyclosporine) in June 2000. Two weeks later, after starting the Tibetan medicine, his hemoglobin was higher than it had been in the preceding 3 years (without a transfusion), and it was the longest period that he did not need a blood transfusion.
He continued on Tibetan medicine for the next 4.5 years, requiring no transfusions. Additionally, 16 months after starting the Tibetan medicine and stopping the cyclosporine, he was told by his biomedical physician that he no longer needed insulin and was put on oral hypoglycemic medication.
In early 2005, his hemoglobin began dropping and he began acupuncture and a new regimen of Tibetan medicine, without Western medical intervention. In May 2006, all blood counts were normal, he did not require transfusions, and he stopped all treatments.
As of September 2011, he was alive and well, and had not had any treatments (Tibetan or Western) since May 2006. After 11 years since his initial Tibetan medicinal treatment, he wrote and signed a letter addressed to the Tibetan medical clinic, saying,
This was a miracle. Just two weeks of Tibetan medicines [sic] had changed my life. . . . I did not take my usual transfusion. Life became easy. . . . As a chemical engineer, I feel when it comes to medical treatment for any ailments, the probability for Tibetan medicines [sic] working for you is same [sic] or better than allopathic. These medicines have minor to no side effects. I have not had any difficulties taking them. Many thanks.
Tibetan Medical Treatment
After a Tibetan diagnosis of “blood cancer” (Tib. Khrag ‘bras), his first regimen of Tibetan medicine (in 2000) comprised primarily of Dashel Dhuetsema, Dashel Sodhuen, Dangney, Dagshun Gupa, Kyuru-Drukpa, Yungwa Shithang, ArunChupa + Sangdak. Then in 2005, his Tibetan medical treatment included Dashel Dhuetsema, Gawa Chudruk, Sangdak Dharyaken, Sertig, Gurgum Chusum, and Gurkhyung. The precious pills he was administered included Rinchen Mangjor Chenmo and Rinchen Yunying Nyernga taken on an alternating basis each week. The total duration of his Tibetan medicine course was 19 months. Detailed documentation of his medicines and their doses is listed in Table 3.
Name of the Medicine Prescribed, Number of Doses, Pills per Dose, and Treatment Duration for Case 3 With Red Cell Aplasia.

Discussion
In this very limited case review, Tibetan medicine has appeared safe and effective for the given cases of cancer and hematologic disorders evaluated. Furthermore, the Tibetan medical treatments demonstrated positive effects on patient quality of life and cancer regression and remission, in some cases within weeks of starting treatment and lasting for years. For each of these cases, conventional biomedical treatments were recommended, yet patients opted for the Tibetan treatments because of past experiences with severe complications, side effects, and/or poor response of the Western treatments.
In Tibetan medicine, a given prescribed formula may have multiple target benefits for a given treatment approach and may take on different active roles in the treatment progression. For example, in the case of cancer, Sangdak Dharyaken is described as functioning to control the multiplication and growth of cancerous cells as well as killing and dissolving the cancerous cells of the targeted internal organ. Thus, in the simplified 3-fold approach to Tibetan medical cancer treatment described above, Sangdak Dharyaken would play an important part in the first step of breaking down or dissolving the cancer growth. However, Sangdak Dharyaken is seen to also maintain important roles in the next stages of the treatment that go beyond its role in addressing the cancer growth. Gawa Chudruk is primarily prescribed to target the final step in the treatment by rehabilitating the affected bodily constituents, targeted organs, and physiologic systems that viral, bacterial, and cancerous cells have debilitated. However, Gawa-Chudruk is also recognized to be important in the first stage of diminishing the cancer growth. Likewise, many of the medicines in each case’s therapeutic approach are recognized to address the second therapeutic step of the treatment regimen by pacifying the predominant nyespa or functional energy system involved, cleansing necrotic tissues, and reducing inflammation, but involved in the first and third steps as well. As is seen most quintessentially with the precious pills, but applies to all medicines for a given Tibetan medical treatment regimen, each medicine may have a multitude of roles and therapeutic target activities along a given treatment trajectory. A list of the common medicines to all 3 cases, along with some of the benefits, is included in Table 4.
Tibetan Medicines Common Across All 3 Cases, Names and Benefits.
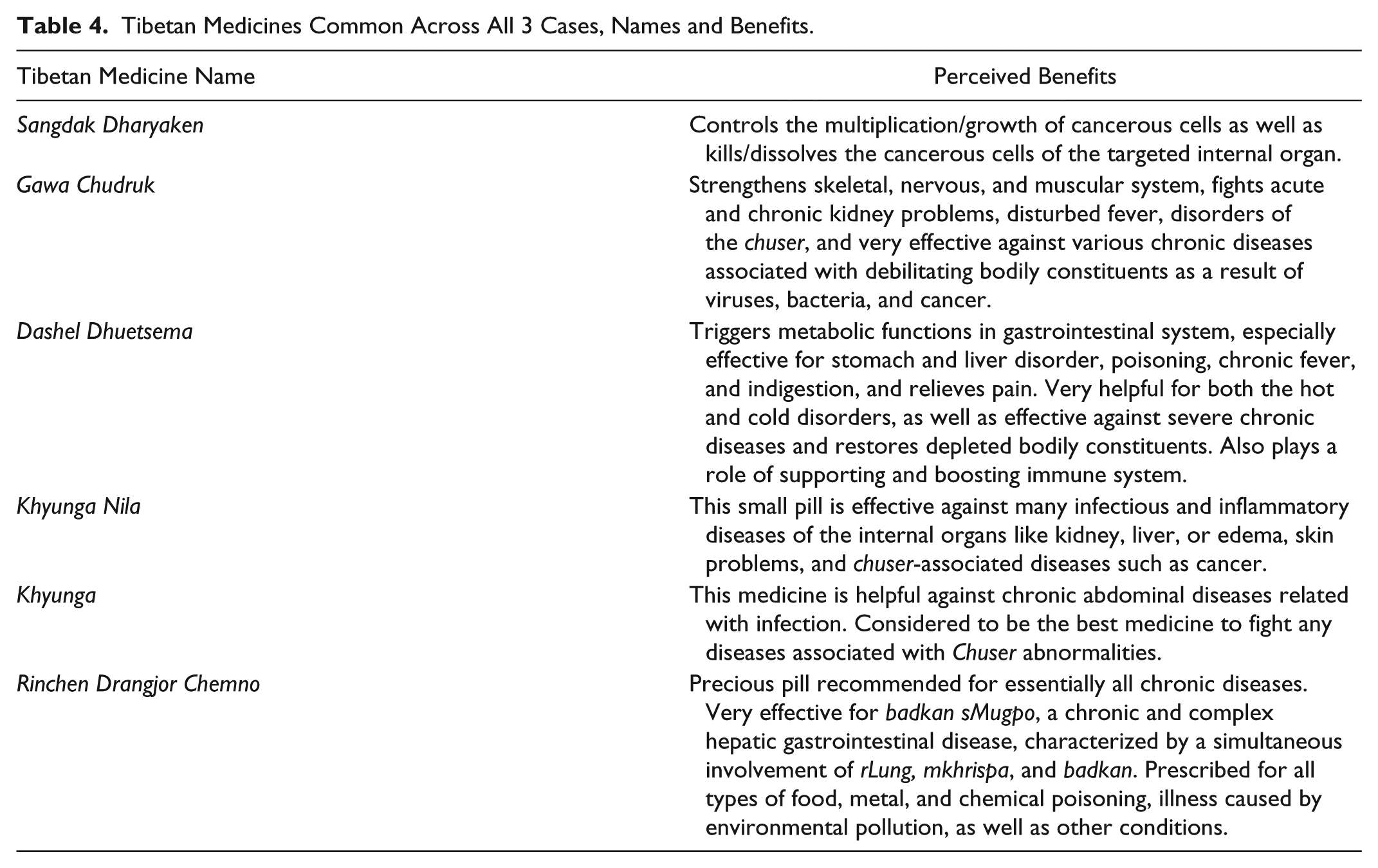
Herbal and mineral formulas are the mainstay for treating cancer patients. Despite individual differences in the regimens, common treatments for all the aforementioned patients were the following: Gawa Chudruk, Khyunga Nila, Dashel Dhuetsema, and Sangdak Dharyakan. Gawa Chudruk has the primary active ingredients of safflower petals, chebulic and beleric myrobalan, Indian gooseberry, and red sandalwood. Khyunga Nila and Khyunga are primarily composed of chebulic myrobalan, sweet flag, saw-wort, and acacia in concentrated form (as khenda syrup confection). It is to be noted that medicines like Dashel Dhuetsema, Dangney, and Dagshun Gupa have many ingredients that help bolster the immune response and hematological parameters like hemoglobin, as well as balance the body’s energy levels. The detailed list of the key ingredients and botanical names for the prescribed medicines are provided in the appendix.
This was a small retrospective case review that encountered several challenges thereby limiting the final selection of cases that met inclusion criteria. First, most of the medical records had poor documentation of the Western and Tibetan diagnoses and treatments and follow-up testing. Second, most patients received a combination of Western biomedical and Tibetan medical treatments. While this may be an ideal course of treatment for many patients, this integrative approach limits the ability for such a case review to be able to draw conclusions on the effects provided by Tibetan medicine exclusively. Nonetheless, we are encouraged by the few cases identified and believe that the findings suggest the need for further collaborative research in this area, specifically rigorous, longitudinal observational studies or clinical trials.
With growing interest in botanicals and nutritional supplements for cancer and other chronic illnesses, biomedical researchers are keen to test particular herbs or extractions for their active component(s). However, we caution against such a reductionist approach that loses sight of the synergy inherent in multimodal whole system traditions like Tibetan medicine, where the holistic and synergetic effects of the formulation become the deciding factor. We believe optimal future research will involve active collaborations between experienced Tibetan medical practitioners and biomedical researchers in order to maintain the integrity of the Tibetan medical treatments and to ensure rigor in the scientific approach.
Conclusion
Tibetan medicine is an ancient health system that uses a variety of treatments and a personalized approach in preventing and treating a wide range of illnesses, particularly chronic conditions including cancer. Very limited research on Tibetan medicine exists with minimal published clinical studies on cancer patients. Though quite limited, this case review sheds some light on the safety and promising effects of Tibetan medicine for cancer to suggest that it is an area that warrants more attention. We recommend rigorous and ethical collaborative research to bring Tibetan medicine into the emerging field of integrative oncology.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Some of the authors (Tenzin Lhundup, Tenzin Lhadon, Jamyang Dolma, Pema Dorjee, Dorjee Neshar, Rigzin Sangmo, and Tenzin Yeshi) are employed at or affiliated with Men-Tsee-Khang (Tibetan Medical and Astro. Institute) with headquarters in Dharamsala, India and branch clinics throughout India; Men-Tsee-Khang is comprised of a Tibetan Medicine hospital, pharmacy, medical school, and branch clinics.
Funding
The first author Dr. Susan Bauer-Wu, was supported by a Georgia Cancer Coalition Distinguished Scholar Award during part of this research period. Other authors received no financial support for the research.