
Abstract
The impact of living with metastatic breast cancer (MBC) is considerable and psychosocial support can be beneficial. Mindfulness-based stress reduction (MBSR) can help self-management of anxiety, depression, quality of life (QoL), and fatigue and has been evaluated in early-stage breast cancer but not MBC. This study investigated the acceptability and feasibility of providing MBSR for women with MBC and of introducing MBSR into a National Health Service (NHS) setting. A mixed methods convergent design was used. Eligible women with MBC, an Eastern Cooperative Oncology Group (ECOG) score of 0 to 2, stable disease, and life expectancy of at least 6 months were invited to attend (by their oncologist) an 8-week MBSR course. Qualitative interviews with patients, a focus group, and interview with NHS staff were held to explore acceptability and feasibility of MBSR. Questionnaires at baseline, during (weeks 4, 8), and after (weeks 16, 24) the course measured fatigue, anxiety and depression, mindfulness, disease-specific QoL, and generic preference based QoL. Of 100 women approached, 20 joined the study. One woman dropped out prior to the intervention due to illness progression. Nineteen women took part in 3 MBSR courses. Recruitment to 2 of the 3 courses was slow. Commitment to 8 weeks was a reason for non-participation, and proved challenging to participants during the course. Participants found the course acceptable and reported many cumulative and ongoing benefits. These included feeling less reactive to emotional distress and more accepting of the disruption to life that occurs with living with MBC. There was high attendance, completion of course sessions, adherence to home practice, excellent follow-up rates, and high questionnaire return rates. MBSR was acceptable to MBC patients, who perceived benefits such as improved anxiety and QoL; but the MBSR course requires a considerable time commitment. There is scope to tailor the intervention so that it is less intensive.
Keywords
Introduction
Breast cancer remains the most commonly diagnosed cancer in women in the United Kingdom (49 564 new cases in 2010) and is the second most common cause of death from cancer in women (11 633 deaths in 2010). 1 It is estimated that 5% to 10% of breast cancer patients will have metastatic breast cancer (MBC) at the time of their initial diagnosis, while 20% are likely to develop MBC later.2,3 Although increased treatment options have improved survival, patients with MBC remain incurable at present. Women with visceral metastases have a shorter life expectancy. Median survival for women with skeletal metastases has increased to 24 to 36 months, and women with a more indolent disease may live for many years (10-15 in some cases). 3
The prognosis of MBC has improved largely due to advances in more effective and better-tolerated therapies, 4 but this has also resulted in more complex survivorship problems for these patients with a high need for psychological support. 5 The impact of living with MBC is considerable with many patients experiencing cancer-related fatigue (CRF) and psychological symptoms such as anxiety and depression, 6 and CRF is also strongly associated with anxiety and depression. 7 CRF is common among most cancer patients and occurs because of the cancer diagnosis and the cancer treatments. Many MBC patients may have physical and psychological comorbidities that can amplify fatigue and complicate management of their cancer.8,9
Psychological interventions such as cognitive behavioral therapy or psychotherapy can improve psychosocial outcomes such as mood and quality of life (QoL),10,11 although there is little evidence that this is sustained or that they specifically address the fundamental cause of ongoing distress.12,13 Other psychological interventions include mindfulness meditation, which has its origins in Buddhist philosophy and has increasingly been adapted (mindfulness-based stress reduction [MBSR]) 14 for use in secular settings to manage psychological and physical problems. Mindfulness involves paying attention to experiences on purpose, without judging and without seeking to change.14,15 Regular practice is thought to cultivate a state of acceptance,16,17 improve emotional regulation strategies, and improve QoL, reducing intrusive thoughts, anxiety, and depression,18-20 making it strongly pertinent for breast cancer patients. Mindfulness interventions in cancer patients have been systematically reviewed with suggestions that MBSR is effective in improving a variety of symptoms such as stress, depression, anxiety, QoL, fatigue, and sleep disturbances.21-26 Two meta-analyses of MBSR in breast cancer patients have been performed, and despite the low number of eligible studies, they identified small to moderate effects for MBSR compared with usual care in decreasing depression and anxiety.24,27
Studies evaluating MBSR in breast cancer patients have focused on early-stage breast cancer (0-III), with only 3 studies including MBC patients in a mixed sample of types and stages of cancers,28-30 and none have exclusively investigated the acceptability and feasibility of delivering MBSR in a MBC population. As MBSR had not been investigated in MBC and in accordance with the Medical Research Council’s recommendation for the investigation of complex interventions, a strategic phased research development process and feasibility study is essential. 31 Feasibility studies are used to estimate important parameters that are needed to design a larger study.32,33 For the purposes of this study, we had 6 feasibility objectives that we needed to evaluate to design a larger definitive study:
To assess the appropriateness of our outcome measures
To assess the variance of key quantitative outcomes to pilot effect sizes and inform the design and sample size calculations of a Phase III randomized controlled trial (RCT)
To assess recruitment, adherence rates, and follow-up rates
To explore participants’ views on the acceptability of the MBSR course
To explore NHS staffs’ views on the acceptability of the MBSR program as a self-management option
To explore NHS staffs’ views on the major barriers and enablers to implementing a definitive RCT of MBSR for MBC patients
There is mounting evidence that MBSR can help people self-manage a broad range of symptoms. If it were found that it was both acceptable and feasible to deliver MBSR to MBC patients, and a future trial showed MBSR for MBC to be effective and cost-effective, then it would be tenable to introduce this approach into the National Health Service (NHS), meeting recommendations to provide psychosocial support for women with MBC.2,34 In order to answer the research questions, we used a mixed methods approach to data collection and analysis, and in this article, we report on the quantitative results and qualitative findings relating to the feasibility and acceptability of the program to patients and to NHS staff and of study processes. All in-depth qualitative findings relating to the impact of MBSR on MBC patients will be reported in full elsewhere. The full protocol of the study is reported elsewhere. 35
Methods
Design
A mixed methods convergent design was used, with qualitative and quantitative data given equal priority with sequential data collection and concurrent data analysis. 36 Qualitative and quantitative methods of data collection and analysis were used, as both were necessary to answer the different questions asked by the feasibility and acceptability outcomes. Both types of data can help obtain a more comprehensive account of the data by overcoming the weaknesses of one method with the strengths of another. 37 The experiences and acceptability of the MBSR intervention to MBC patients was explored in patient interviews. The feasibility of holding an 8-week MBSR intervention in the NHS was explored in an oncologist interview and a focus group discussion with breast care/research nurses. Other feasibility outcomes included recruitment issues, such as availability of eligible patients, identification of patients, recruitment rates, and willingness of patients to be recruited. The acceptability of randomization in a possible future trial was also explored with participants. Retention and adherence rates, the relevance, and the variance in outcome measures for subsequent sample size calculations were also assessed. Retention and dropout were assessed by tracking attendance and program completion (at least 6 of the 8 sessions). A key aspect of mixed methods designs is the integration of quantitative and qualitative approaches at some stage of the design. In this study, the qualitative and quantitative data were collected and analyzed independently as distinct strands to the research. The findings were then merged during the interpretation or discussion stage to inform one another and to support or refute the research questions. 38
Ethical approval was from the Isle of Wight, Portsmouth & South East Hampshire LREC (21/7/2010 REC reference number: 10/H0501/18). CCT Trial registration: ISRCTN41578109.
Participants
Patients were recruited from 3 local oncology units over 10 months (January to October 2011). We estimated that 80 women would need to be invited to create 3 MBSR courses of 7 to 10 patients per course based on MBC prevalence and previous research. 39 Oncology consultants identified eligible women who had MBC for at least 2 months, with stable disease and life expectancy of at least 6 months. Study inclusion required an Eastern Cooperative Oncology Group (ECOG) Performance Score of 0 to 2, excluding bed bound and frail patients. 40 Study information was given to the patient by the oncologist or the research nurse, and interested patients returned them to the research team. Once consultant approval was offered and patients opted into hearing more about the study, a further assessment interview with the MBSR instructor informed participants of the intervention and assessed their understanding of and suitability for the course. This is best practice and ensures that the course is safe and appropriate for each individual. Eligible and consenting patients then joined the next MBSR scheduled course. The 3 MBSR courses were held consecutively in 2011 allowing time between for recruitment for the next course. All participants received exactly the same MBSR intervention in each of the 3 courses.
The Intervention: Mindfulness-Based Stress Reduction
The MBSR programme 14 was taught by the author CH who has over 10 years training and experience of teaching mindfulness and MBSR to breast cancer survivors. The program aims to cultivate mindfulness, which is defined as bringing one’s complete attention to the present moment-to-moment experience in a nonjudgmental or accepting way.14,41,42 The intention is that, through mindfulness, the course can help people become more aware of their automatic reactions to situations in life so that they can then choose to respond more effectively. This may also help with symptoms such as mood state, for example, the emotions of depression, anxiety and anger, and fatigue. 39 Learning to bring full attention and awareness to their senses and activity of mind in the present moment can help them experience less distress. The practices of the body scan, sitting and lying meditation, gentle yoga stretching, mindful walking, and loving-kindness meditation were taught in class to cultivate mindfulness. There were also discussions about the home practice and the application of mindfulness to daily life. It was decided to retain the original 8-week Kabat Zinn course structure despite the disease burden of the patients as only patients who were well enough to join the course were eligible. We also needed to explore MBC patient experience of the Kabat Zinn MBSR program in its original format, before considering any abbreviations or major adaptions. However, as many of the participants were in active treatment we decided to reduce the duration of the class session lengths slightly to accommodate the needs of the participants. The changes were done in consultation with clinicians and CH, ensuring that the core materials and essence of the MBSR course could still be covered within the slightly reduced time. The class sessions were reduced to 2 hours in length (instead of 2½ hours) except the first and last, which were 2½ hours. The day of mindfulness in week 6 was 4½ hours (instead of 6-7 hours), and the mindfulness home practice using CDs of the above-mentioned mindfulness practices was 30 min/day (instead of 45 min/day).
Qualitative Data
Qualitative Data Collection
In-depth semistructured interviews
Patients who were eligible and who had consented to join the study were contacted to arrange a face-to-face interview to take place 1 or 2 weeks before joining an MBSR course. The interviews commenced with a “grand tour” question 43 to elicit contextual insights about individual cancer journeys and QoL issues. Tailored questions then explored topics to elicit insights as to previous meditation experience and expectations from joining the course. The same set of individuals were then contacted 4 months after the end of the MBSR course (at week 24) to take part in a second round of interviews to explore the acceptability of the MBSR course and study processes and to gather in-depth perceptions and experiences of the impact of MBSR. One oncologist was invited and consented to a face-to-face interview, which took place after all MBSR courses had occurred. The interview elicited insights into recruitment issues, study processes, and perceptions on the acceptability and feasibility of delivering MBSR to MBC patients in the NHS.
Focus group
Breast care/research nurses from the 3 recruiting oncology clinics were invited to attend a focus group 1 month after the end of the MBSR intervention. The group discussion explored feasibility and the acceptability of MBSR for MBC patients and of MBSR within the NHS. Unanticipated topics that arose during group discussion were also explored allowing increased understanding of the core issues to emerge.
The interviews and focus group lasted between 1 and 2 hours; they were recorded, transcribed verbatim in readiness for analysis, and anonymized.
Qualitative Data Analysis
A thematic analysis was conducted.44,45 Repeated reading of transcripts and listening of recordings assisted familiarization with the data and identification of initial codes. The initial codes were then defined and used to guide analysis of the full data set. Using constant comparison, a technique derived from grounded theory,46,47 transcripts were compared within and between each other aiding the iterative search for themes that were then reviewed, defined, and named. Analysis also paid attention to the key discursive repertoires the women employed in their narrative accounts. 48 The integrity of the analysis was tested through a secondary analysis of a sample of transcripts. Deviant or negative case analysis 49 was used to help avoid premature theory formation and incomplete representation of data and an audit trail of study procedures and reflexive practice to maintain transparency.50,51 The themes relating to the acceptability and feasibility of the study are described below with verbatim quotes chosen to illustrate key insights. (In-depth qualitative findings on the impact of MBSR on the lives of the women living with MBC will be reported in full elsewhere.)
Quantitative Data
Quantitative Data Collection
Each participant was asked to complete a number of questionnaires. Four of the questionnaires were administered at 5 time points (baseline prior to participation, during the MBSR course at weeks 4 and 8, and at follow-up at weeks 16 and 24) and 1 questionnaire at 2 time points (baseline and 24 weeks follow-up).
Questionnaires administered at 5 time points
The Brief Fatigue Inventory (BFI), 52 the Hospital Anxiety and Depression Scale (HADS), 53 the EuroQol Quality of Life-5 Dimensions (EQ5D), 54 and the Toronto Mindfulness Scale (TMS) 55 were administered at baseline prior to participation, during the MBSR course at weeks 4 and 8, and at follow-up at weeks 16 and 24.
Questionnaire administered at 2 time points
The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire C-30 (EORTC QLQ C30) 56 was administered at baseline and at week 24.
Outcome Measures
Cancer-related fatigue
CRF was the primary outcome measure and was assessed using the BFI. The BFI consists of 9 items and is widely used, well validated, reliable, and effective for measuring CRF. There are 3 fatigue severity items and 6 concerning the interference of fatigue with QoL over the last week. The global BFI score is the arithmetic mean of all 9 items (range = 0-10). CRF was defined as global BFI score of >3.57,58
Anxiety and depression
These parameters was measured using the HADS. The HADS is a standard and well-validated measure of mood disorder.59-61 A HADS score between 8 and 10 is borderline, and a score of >11 categorizes more definitive anxiety or depression. 62 A drop of 3 points represents a clinically meaningful improvement in both depression and anxiety. 63
Disease-specific quality of life
Disease-specific QoL was measured using the EORTC QLQ C30, which is the standard internationally accepted instrument for measuring QoL in patients with cancer. It is composed of 5 functional scales (physical, social, role, cognitive, emotional), 3 symptom scales (fatigue, pain, nausea/vomiting), a global health status, and 6 single items (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties). All the scales and single-item measures range in score from 0 to 100. A high score for a functional scale and the global health scale represents a high/healthy level of functioning and global health but a high score for a symptom scale item represents a high level of symptomatology. Clinically meaningful medium differences were assessed based on guidelines for subscales of the EORTC QLQ C30. 56 Effects are considered as medium size for differences of 10 to 15 for QoL and differences of 13 to 24 for insomnia.
Generic preference-based QoL
This factor was measured using the EQ5D a validated, standardized non-disease-specific instrument for describing and valuing health states consisting of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 3 levels: no problems, some problems, and extreme problems.
Mindfulness
This parameter was measured using the TMS. The TMS includes 2 factors, curiosity and decentering. Lau et al provide typical values of the 2 factors in the TMS scales, curiosity and decentering. TMS scores should increase with increasing mindfulness meditation experience, and decentering scores predict improvements in clinical outcome. Feasibility studies do not usually require a power calculation but the sample size should be adequate to estimate critical parameters such as recruitment rates.32,33 For this feasibility study, we hoped to recruit 30 subjects, as this would enable us to estimate effects and calculate a sample size for a future larger study. A sample of 30 would have an 80% power to detect clinically meaningful changes of 4 or 5 units for the TMS subscales and would provide evidence of a relationship between TMS and BFI if such a relationship had a correlation of at least .35.
Questionnaire data were imputed into SPSS software (version 19). Individual item missing data was imputed by using the average of available data and scaling up within each questionnaire. When whole questionnaires were missed at weeks 4 and 8, data were imputed by using previous values carried forward.
Quantitative Data Analysis
All analyses were carried out using SPSS. Data from the BFI, HADS, and TMS were intended to be analyzed using an age-adjusted repeated measures analysis of variance model taking into account the 5 observations at the 5 time periods for each patient. However, the small sample size achieved did not justify this. These variables and the EORTC QLQ-C30 variables were analyzed using paired sample t-tests comparing within-patient differences between baseline and week 24.
A series of correlation analyses was carried out on changes in outcomes from baseline to week 24. Correlations between the TMS and the BFI and HADS were computed to assess whether changes in mindfulness were associated with changes in fatigue, anxiety, or depression. Correlations were also investigated to test whether hours of formal mindfulness practice done both in the classroom and at home (30 min/day as minimum amount set in protocol) were associated with improved outcomes, HADS, TMS, and BFI.
A full economic analysis would not be appropriate at this feasibility stage due to the small sample size. The main cost “drivers” linked to MBSR were estimated, such as the cost of MBSR itself and the cost of providing the intervention to individual patients. The responsiveness of EQ-5D and the appropriateness of the QALY approach was explored (the QALY or, quality-adjusted life year, is a measure of disease burden, including both the quality and quantity of life lived). The potential QALY gain from the intervention using the area under the curve approach was also estimated.
Results
Sample Characteristics
Sociodemographic details of the 19 MBSR course participants are listed in Table 1. All the participants were on a range of treatments, such as chemotherapies, endocrine, biological, and bone therapies. Any change in treatment regime was recorded and reported back to the research team by the research nurses. None had their treatments changed during the study. Five research nurses took part in the focus group.
Sociodemographic Characteristics and Attendance of Participants.
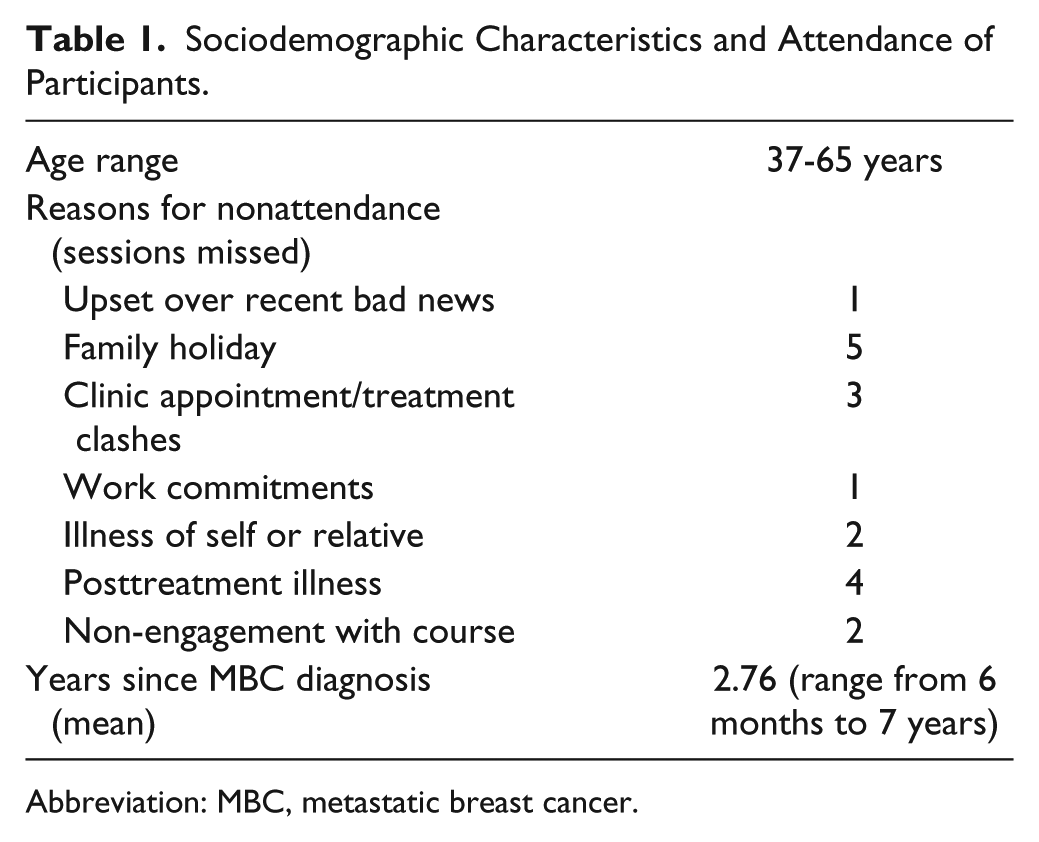
Abbreviation: MBC, metastatic breast cancer.
Recruitment
One hundred women were approached to join the study. Twenty women (20%) agreed to join the study and were recruited (the flow of participants through the study is shown in Figure 1), with 19 completing (1 dropped out after baseline measures and before joining an MBSR course due to illness progression). Eighty (80%) women did not join the study. Of these 27 (33.75%) declined to participate for unspecified reasons; 19 (23.75%) were excluded because they were too ill to participate; 13 (16.25%) felt it was too much commitment; 12 (15%) had travel problems; and for 9 (11.25%) women the sessions clashed with treatment or sessions were held at a time when they anticipated side effects from treatment.
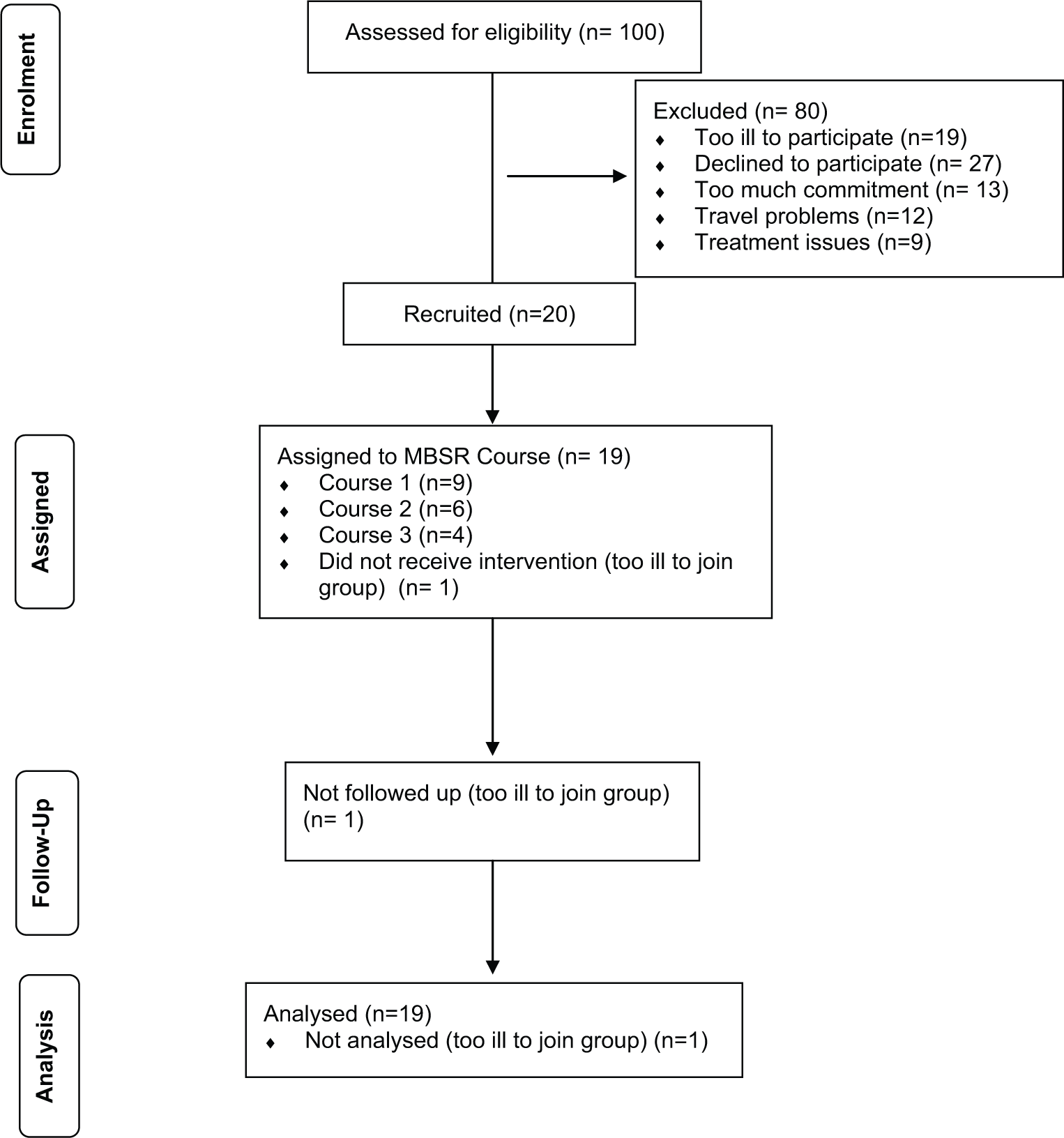
Flow of participants through study
Retention and Adherence
Mean attendance was 8 out of 9 sessions (range = 6-9), suggesting that participants were motivated to continue participating. Reasons for nonattendance are listed in Table 1. Duration of formal mindfulness practice was estimated by adding classroom and participant recorded home practice39,64 and was 27.40 min/day and was over the whole 8 weeks of the program. This shows good adherence to practice compared with 33 min/day in women treated for stages 0 to III breast cancer and 32 minutes with a mixed cancer population. 39
Qualitative Findings
The qualitative findings presented in this section only relate to the feasibility and acceptability of the MBSR study processes for patients and the acceptability of MBSR in the NHS. Full qualitative findings of the impact of MBSR on MBC patients’ lives will be reported in-depth elsewhere as there is limited space to do so in this article. Three main themes emerged from the second round of patient interviews, the oncologist interview, and the focus group. All quotes are anonymized and are presented to support and illustrate the themes. Quotes from the MBSR course participants include, in brackets, the age of the participant and the time since MBC diagnosis (e.g. age 37; 4 years). Quotes from the different focus group participants are represented by “F1, F2, F3, F4, and F5” to show that different participants are speaking. Quotes from the oncologist interview are represented by “(Onc Int).”
Theme 1: Barriers to Participation and Recruitment Challenges
We did not interview women who declined participation in the study; however, reasons for non-participation were recorded by the nurses (see Results/Recruitment section). The oncologist interview and focus group captured challenges faced during recruitment and these concurred with reasons for non-participation and can help explain the low recruitment rates for course 2 (6 participants) and particularly course 3 (4 participants).
Many patients declined participation, as they reported not feeling well enough to take part; others were not approached or deemed not eligible because their disease was considered too unstable: I—didn’t want to—offer it to patients who I felt wouldn’t physically be able to cope with it; I didn’t want to offer it to patients who I felt were at risk of suddenly deteriorating during the course—you know—the week before it starts, the disease has suddenly progressed and they need chemo and obviously—their medical care had to come first. (Onc Int)
Even for patients who were well enough to join the study, the MBSR course schedule was perceived as being too structured and prescriptive making recruitment challenging: The fact that there was a group setting, there were certain pre-set dates, patients had to travel, obviously, the geographical location was difficult for some people and—I think—you know—the day of the week also impacted on some patients as well because it didn’t fit with the days they were receiving treatment or hospital visits. (Onc Int)
The nurse led focus group discussion concurred with this perception and described how the 8-week commitment to the course was also seen as problematic and was a reason for non-participation and a barrier to recruitment:
And the length, as well . . . the time commitments—8 weeks and a whole Saturday—that was another big concern, that’s a big commitment to make as a . . .
. . . a metastatic patient . . .
Yes—yes, absolutely—you know—2 months of your life where you absolutely have to go to something. . . . I think they were very worried that—if they couldn’t commit to the 8 weeks, there was no point doing it at all.
Discussion within the focus group also led to insights into possible reasons for non-participation for patients who declined to participate for unspecified reasons (see Results/Recruitment section).
. . . the older ladies that we deal with were a bit—a bit more resistant to feeling that they had any stresses or strains in their life and—whether they did or not—they wouldn’t admit it to us. And a couple of ladies just sort of laughed—oh, I’m not that type of person . . .
. . . and when they are well—really seem—feel like they are coping, they don’t want to do it because they are working and they just want to get on with their life, but when they are ill . . .
They are too ill . . .
: Yeah—they are normally too ill or they are declining quickly and so it was really difficult to get them at the—at the right time . . .
Theme 2: Acceptability/Benefits “an Additional Band of Inner Strength”
Sixteen of the 19 participants found the MBSR course to be acceptable, reporting “cumulative and on-going” (Age 60; 1 year) benefits, with others describing the course as a “useful tool for dealing with feelings” adding that it is “ far more; the scope is far more wide-ranging” (Age 42; 3 years ), and others reporting that the course surpassed their expectations: I thoroughly enjoyed it, I have to say, it’s—it surprised me in a number of ways and I think—I can’t remember all the things I said to you right at the beginning, about what I was hoping to get from it all . . . it wasn’t what I thought it was going to be in some ways, but what actually turned out to be was much, much better than I thought it might be. (Age 37;4 years)
Many talked in detail about the techniques that they were taught and how they have adopted them into their ongoing practice and the benefits that they have experienced. The benefits described included helping become less reactive to the emotional distress and more accepting of the disruption to their lives that was a part of living with MBC: There’s quite a lot of power in just sitting with those fears and emotions, that was one of the big key things that came through; sort of the acceptance of where things are and being with it and being with each other in where we are and—and that was absolutely fine. (Age 47; 2 years)
Some discussed day-to-day benefits such as improved sleep or improved ability to manage weight control with mindful eating. Others perceived that they had experienced more profound benefits as they described developing a “shifting perspective,” which resulted in a changed relationship with themselves, with others, and with their illness: It re-established the proper balance of—of, you know, myself in my own life. I think it developed an additional band of inner strength . . . to say, yes, this time is me, this is mine; what I’m doing now—is for my own benefit and I feel I will benefit, and has continued, you know, with every time I use it. (Age 60; 1 year)
Participant feedback to the research nurses expressed many of these positive experiences described here and was reflected in the focus group and oncologist discussions. The discussions also focused on the current lack of support services available for MBC patients, with a consensus that MBSR was an acceptable intervention for MBC patients and could be acceptable and feasible to introduce into the NHS, particularly if concerns relating to time commitment, travel, and cost barriers and clinic and treatment clashes were resolved.
We need to have this type of thing . . . it is a particularly poor area for services; most things are primary breast cancer or nonspecific, so if you are metastatic, you could also go, but I certainly think our patients would be up for it—I think commitment and for people to be able to get there and—or for somebody to take them was one of the biggest barriers, the idea of having to get somewhere else is just too much for some people.
The oncologist and focus group participants had suggestions for ways that the intervention could be incorporated and adapted, and these suggestions were consistent with the interview participants’ ideas for the course:
I certainly think our patients would be up for it . . . a shorter course and a lot of our patients do a lot of things online, so I think if there were some techniques that they could pick up from that or—as perhaps as a short evening class, I think that would—you would have a higher take-up of people wanting to take part . . . or I think a lot of patients would find it really, really useful if they could come and do it—you know—you have your doctor’s appointment and then you’ve got a 2 or 3 hour wait, potentially, before you have any treatment.
Theme 3: Acceptability/Challenges “Like Having a Full-Time Job!”
Three of the participants did not find the course acceptable or experience any benefits. The reasons described included dislike of the group format, the commitment of 8 weeks and home practice, and difficulties with the techniques; for example, the following participant described her experiences with the body scan.
I don’t want to be dwelling on it and I found when I was doing the exercises and all—you know—concentration and that—although it was to help me . . . it kept reminding me that I wasn’t very well and I didn’t like that. (Age 64; 2 years)
All the participants struggled with certain aspects of the program, and one of these aspects was the amount of home practice that participants were expected to achieve.
I mean someone joked one week that it was like having a full-time job and we kind of—you know—we all kind of nodded. I really struggled with that, it was really hard, for me, with work and 3 children. You know—you must lie down for an hour. To try and get an hour’s peace in this house is impossible; my oldest goes to bed at 10 o’clock at night and my youngest is up at 7, I just don’t have an hour without noise in this house. (Age 40; 4 years)
Although the average home practice time was 27.40 min/day, some individuals, particularly those who were not working or did not have children, were able to spend more time on their home practice than others. The full-day retreat was another contentious aspect of the course a few of the participants enjoyed the experience describing it as “a powerful” and “extraordinary” day. Others expressed ambivalence or negative perceptions about the day: I thought the day was a bit too much. I didn’t feel—from my point of view—that the day really added anything that the other sessions hadn’t and didn’t give me. I just thought it was a bit too long, I really wanted to go home. I just didn’t really want to be there any longer. . . . I did find it tiring actually . . . oh and the silent eating—I could never get on with the eating. (Age 63; 1 year)
Most of the participants commented either in their interview or to the nurses that the course was overly long, making it difficult to commit to 8 weeks, some were working and/or had children, had family commitments or holidays, or the course sessions clashed with treatment and clinic times. When participants questioned reported positive opinions about study processes such as the possibility of randomization for future studies. The questionnaire burden was considered acceptable; however, most of the participants described difficulties with understanding the Toronto Mindfulness Scale: I thought I don’t know if I’m answering this right because it was a bit—I think—that stumped me a little bit. . . . Number one, you see, I find—“I experience myself separate from my changing”—see, I thought I’m not quite sure what that means. So I don’t actually know what I put on my questionnaire now, I don’t know if I put unsure how to answer—or I just thought—what does that actually mean? (Age 48; 6 months)
Quantitative Results
Nineteen patients participated in the study. Of 423 questionnaires sent out 409 were analyzed. Of the 14 not included in the analysis, 9 did not get returned (one participant did not return the TMS at week 4 and all 4 of the questionnaires at week 8 because of temporary disengagement with the course. Another participant did not complete all 4 questionnaires at week 8 because of health issues). Five were discounted as one participant completed all 5 baseline questionnaires but did not join a MBSR course and withdrew from the study due to illness progression.
The mean scores and standard deviations for the primary variable, BFI, and for the other main variables, HADS Depression, HADS Anxiety, TMS Curiosity, and TMS Decentering, at baseline weeks 4 and 8 during treatment, and at weeks 16 and 24, are shown in Table 2. The mean scores over the study period are illustrated in Figure 2.
Mean Scores and Standard Deviations for BFI, HADS Depression, HADS Anxiety, TMS Curiosity, and TMS Decentering at Baseline (Week 0) and at Weeks 4, 8, 16, and 24.
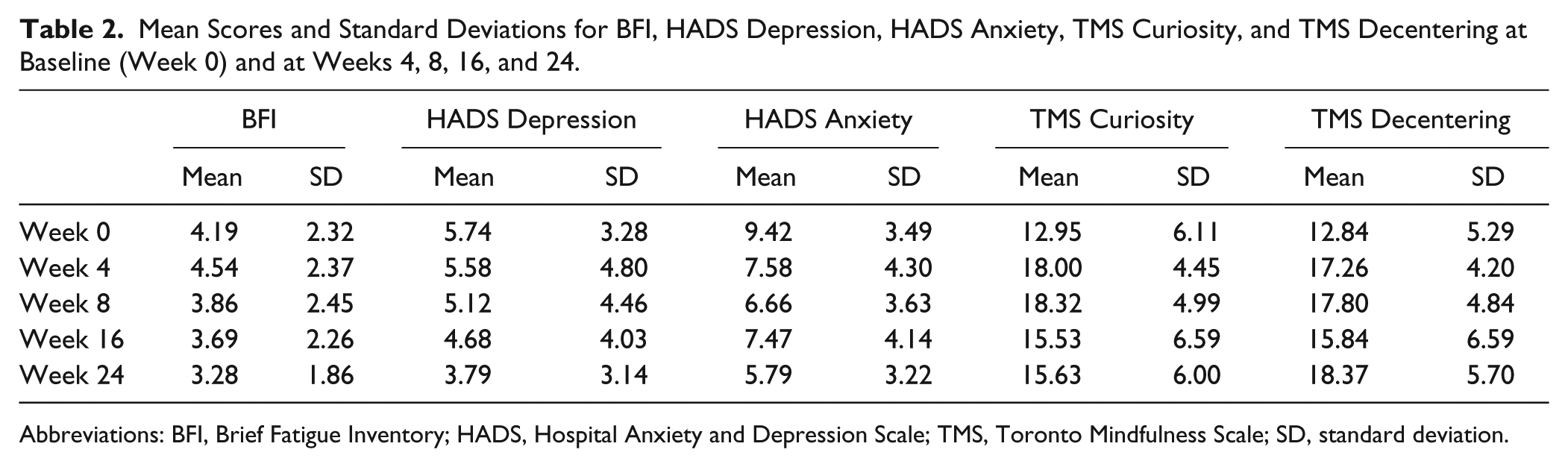
Abbreviations: BFI, Brief Fatigue Inventory; HADS, Hospital Anxiety and Depression Scale; TMS, Toronto Mindfulness Scale; SD, standard deviation.
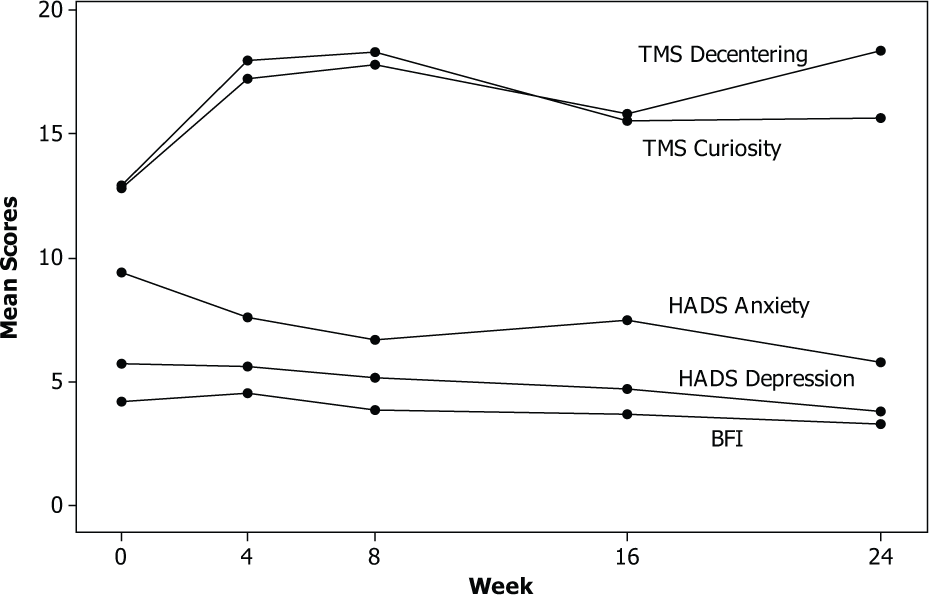
Mean scores for BFI, HADS Depression, HADS Anxiety, TMS Curiosity, and TMS Decentering over the 24 weeks of the study period.
Table 3 shows the within-patient changes in these variables from baseline (week 0) to week 24 (4 months after the end of treatment). The mean change in BFI was 0.91 units (P = .062). The reduction in BFI in this small sample of individuals with severe terminal illness indicated a small but almost significant downward trend (see Table 2 and Figure 2). The HADS Depression showed a clinically nonsignificant reduction from baseline to week 24 of 1.95 points (P = .044). HADS Anxiety showed a reduction from baseline to week 24 of 3.63 points (P < .001), representing a change that is both statistically significant and clinically meaningful, with a substantial linear downward trend. TMS Curiosity scores showed an increase in means scores from baseline to week 24 of 2.68 points (P = .087), while TMS Decentering scores showed a significant increase from baseline to week 24 of 5.53 points (P = .002). Table 3 also shows the changes from baseline to week 24 for the EORTC QLQ C30 variables. There were significantly beneficial changes between week 0 and week 24 in the EORTC QLQ C30 global health scale, physical functioning, cognitive functioning, and insomnia.
Mean Changes in Scores for BFI, HADS Depression, HADS Anxiety, TMS Curiosity, TMS Decentering, and the EORTC QLQ C30 Variables From Baseline (Week 0) to Follow-Up (Week 24) (Paired t-Tests).
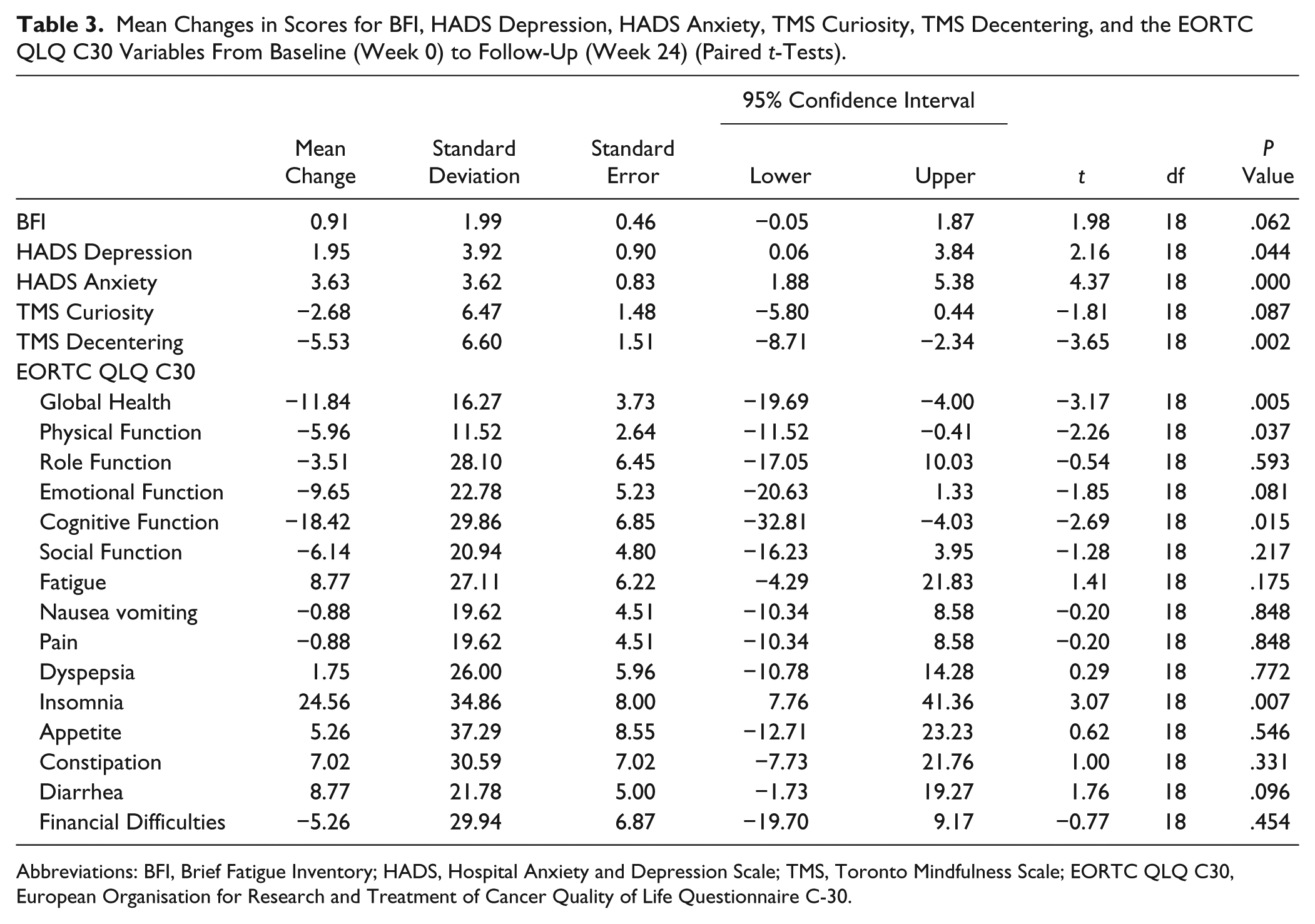
Abbreviations: BFI, Brief Fatigue Inventory; HADS, Hospital Anxiety and Depression Scale; TMS, Toronto Mindfulness Scale; EORTC QLQ C30, European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire C-30.
Correlation analysis in this small sample did not show any significant relationships between the TMS and the BFI and HADS (Table 4) and so did not indicate that changes in mindfulness were associated with changes in fatigue, anxiety, or depression. No correlation was found between formal mindfulness practice including home practice and the other outcomes (Table 5).
Correlations Between Changes in HADS, BFI, and TMS (2-Sided P Values).
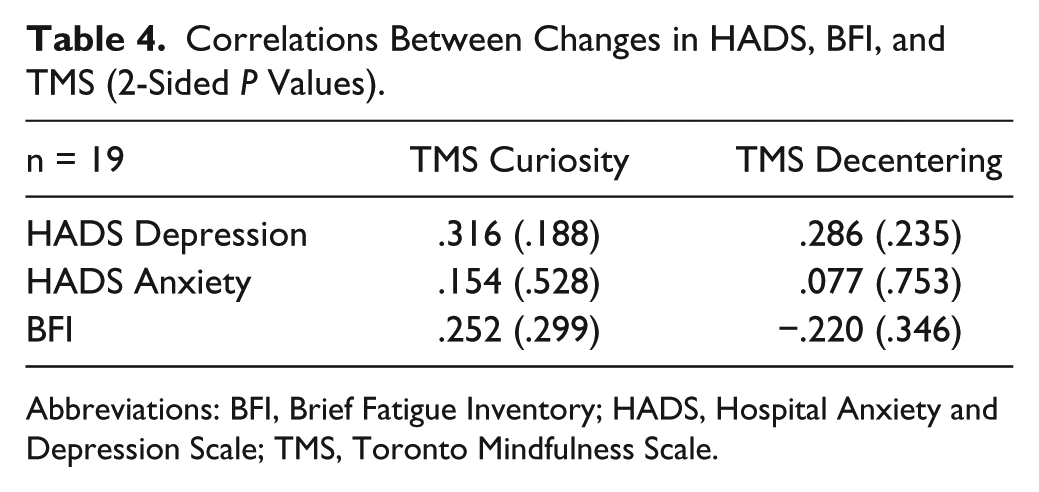
Abbreviations: BFI, Brief Fatigue Inventory; HADS, Hospital Anxiety and Depression Scale; TMS, Toronto Mindfulness Scale.
Correlations Between Changes in HADS, BFI, and TMS and Average Number of Hours of Mindfulness Practice (AveHP) (2-Sided P Values).
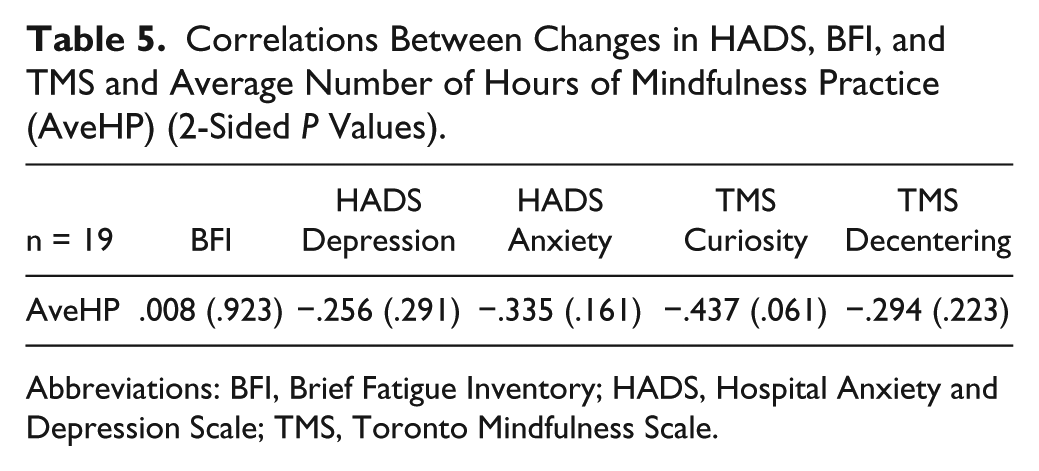
Abbreviations: BFI, Brief Fatigue Inventory; HADS, Hospital Anxiety and Depression Scale; TMS, Toronto Mindfulness Scale.
The EORTC QLQ C30 showed greater variability before and after the intervention, compared to the EQ-5D score, in function scales and Global Health score. The mean EQ-5D value at baseline was 0.74 and 0.72 at the end of the follow-up period, indicating a small deterioration in QoL. This in terms of utility score translates to a difference from baseline of −0.022. However, as the sample size is small the presence of 1 patient reporting a very low score (outlier) has contributed largely to this result. The mean score of the rest of the patients at the end of the follow-up period is 0.76 when this outlier is taken out of the estimate, and the result shows an improvement for the rest of the group of 0.04, indicating that the intervention may show different results if severity is taken into account. QALYs for individual patients have been calculated using linear interpolation between the baseline and 4-month utility values. Using the area under the curve technique, the mean QALY number generated this period from baseline to 4-month follow-up was 0.23 (standard deviation = 0.073). Translating this to 1 year equivalent the QALY value generated is 0.7. However, without having a control group the incremental QALY gain from the intervention cannot be calculated.
The cost of providing the intervention is £16109.76 for all patients (Table 6). The largest costs were the cost of the instructor and the course accommodation. The larger fixed cost indicates that the number of participants in the course is an important factor estimating per patient cost. In this case the total cost translates to a mean per patient cost of £805.5 to provide the intervention. Finally, given the cost of the intervention (£16109.8) and the NICE threshold (£20 000), the intervention should deliver at least an incremental QALY gain of 0.27 during the 4-month period to be considered cost-effective.
Costing of MBSR Course.
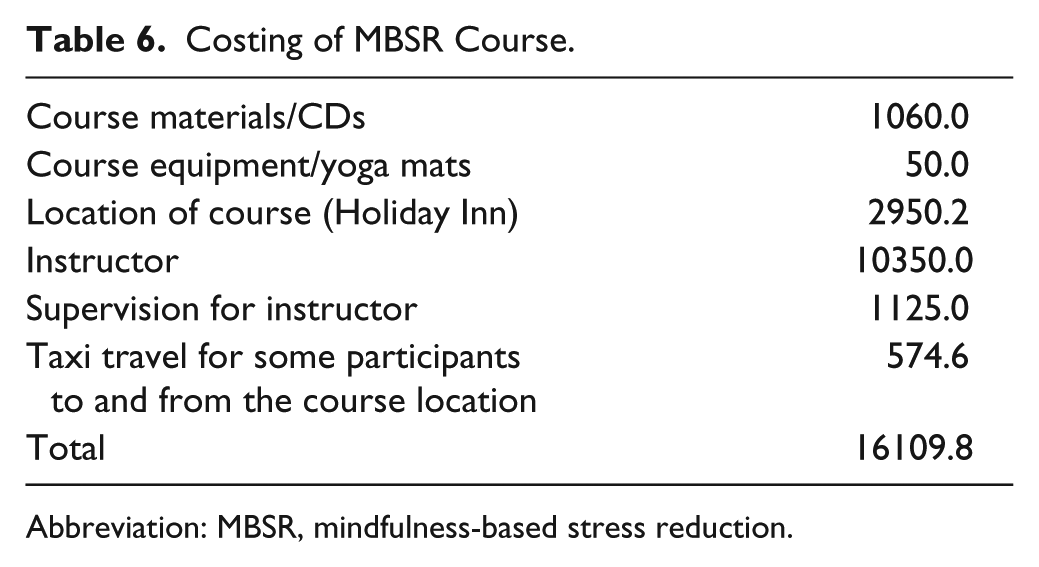
Abbreviation: MBSR, mindfulness-based stress reduction.
Discussion
MBSR has not previously been evaluated in MBC due to the nature of the disease and the specific needs of MBC patients. This is the first mixed methods study to evaluate the acceptability and feasibility of delivering MBSR to a group of patients within an NHS setting, who are nearing the end of life with a diagnosis of MBC. We intend to use this feasibility and pilot data to develop a more definitive pragmatic study evaluating the effects of MBSR on fatigue, anxiety, and depression in patients with MBC. Although there is an increasing conceptualization of MBC as a chronic illness, the current provision of psychosocial care for those living with MBC is still lacking.2,34 A recent report 34 found that women still experience a reduced QoL and report their experience of care to be poor. Palliative care services provide intensive support at the end of life, which is only a short phase of a much longer illness trajectory. 65 Palliative care services are clearly not meeting the needs of this population, and consideration of novel ways of working and developing integrated models of care with primary care and oncology services may address patients’ unmet needs.5,34 Evidence suggests that MBSR24,27 has the potential to meet some of these needs by improving psychological health in breast cancer patients.23,26 Integrating MBSR in the treatment of breast cancer can help beyond treating the physical symptoms to reduce patients’ anxiety and help them adjust to a life-threatening illness and existential distress. 66
In our original protocol, we hypothesized that an improvement in mindfulness would improve anxiety and depression, which in turn would improve their CRF. 35 This study does demonstrate an improvement in QoL and better management of participants’ distress and fatigue, thus improving their survivorship, but not through the mechanism of increased mindfulness that we originally hypothesized. Recruitment to the study was challenging because of the nature of the illness, but overall the results of the study suggest that MBSR can be effectively delivered to relatively stable patients with MBC. Among those who consented, there was a willingness to continue with full participation evidenced by the high attendance and completion of the course sessions, remarkable adherence to home practice, and high follow-up rates with just 1 dropout. This suggests that the intervention was acceptable to those who participated and this was supported by the qualitative data. The measures were acceptable to participants with a high questionnaire return rate and questionnaire completion was similar across all the measures.
There is some qualitative data reporting cancer patients’ experiences of MBSR,65,67-69 and these studies either focus on a mixed cancer type population 65 or focus on a mixed stage of breast cancer population. 68 This current study, however, focusses exclusively on MBC patients who have unique concerns due to the advanced stage of their disease. Our qualitative findings are consistent with other studies, which consistently report the overall acceptability of the MBSR program. We also report participants’ difficulties with the program and particular techniques, with a minority of our sample expressing little or no benefit from attending the course. Only one other study has qualitatively reported negative effects or lack of effect associated with MBSR 67 and our findings concur, suggesting that MBSR is not acceptable to all in its current form. In this article, we are limited because of space, to reporting the qualitative findings that are relevant to study feasibility and acceptability. The rich and detailed clinical qualitative findings will be reported elsewhere.
The sample size was lower than we hoped, but even with this size of sample some clinically important quantitative improvements in outcome measures were observed, which were significant and include anxiety measured with HADS, and this will allow us to estimate sample sizes for future, more definitive studies depending on their exact design. The improvements we were able to measure with EORTC QLQ C-30 encompassed clinically meaningful improvements for cognitive functioning, moderate improvements for QoL and insomnia, and small improvements for physical functioning. 56 Many of the participants reported improvement in anxiety, impacting positively on their ability to sleep (anxiety was often experienced more at night), with improved QoL. For example, participants reported that they were more accepting and more able to cope with their life and relationships. While improvements in fatigue and depression were noted, these were not statistically significant in this small sample.
TMS appeared to be a poor measure of mindfulness for this study; several participants reported that it was a difficult measure to understand. TMS measures the capacity to generate mindfulness in a single meditation session, but it does not measure mindfulness in everyday life. 55 In spite of these constraints and although there was a lack of correlation between the TMS and the other outcomes, there was a small increase in the curiosity subscale and a significant increase in the decentering subscale in the TMS, suggesting that individuals did gain essential mindfulness skills in decentering. This should correlate with increased participant mindfulness, but did not, possibly because of the small sample size. Consequently, we could not correlate any improvement in anxiety, fatigue, or depression with an increase in mindfulness but this may be a consequence of the unsuitability of the TMS as a measure of mindfulness. The HADS, BFI, and EORTC QLQ C30 all seemed to be appropriate and acceptable measures. The EQ-5D was not able to identify the improvement detected by the disease-specific QoL measure EORTC QLQ C30. The lack of sensitivity of the EQ-5D when used in cancer populations has been noted elsewhere. 70 Our small sample size and the presence of an outlier made the EQ-5D difficult to interpret in this population but it will almost certainly be a valuable outcome in a larger study.
There were challenges associated with delivering the MBSR program to this group of patients. Recruiting to this type of intervention from NHS oncology clinics was difficult. Some patients declined to participate for unspecified reasons. The focus group provided some insight into this, suggesting that the MBSR course could be presented to patients as an intervention with taught skills that can be useful even if one is not experiencing symptoms of distress and that can be accommodated into a busy working schedule. The issue of commitment to the course was highlighted during recruitment when many eligible women declined participation because of the level of commitment required and especially when class times clashed with other family commitments, treatment, or clinic times. Notwithstanding, those who participated (with the exception of one participant who could not join a course due to illness progression) completed the course and attendance was excellent. This suggests those participants who did enter the study were committed and motivated; it may be that the high attendance was in part due to being in a research study. 71 Indeed, this was reflected in the qualitative interviews where participants reported difficulties in attendance, particularly with the 1-day retreat, but wanted to attend having made the commitment. Participants also reported that home practice was difficult to fit into daily schedules especially if they were unwell, had children, and/or worked. In spite of this the mean time spent doing home practice was only slightly less than the amount specified in the protocol (27.4 min/day vs 30 min/day) and does indicate a strong motivation to comply with the program and that participants perceived benefits from doing their home practice.
Our findings lead us to question whether some adaptation of the classic 8-week MBSR course might be beneficial and increase the acceptability of MBSR for women with MBC, especially if it is to be delivered within the NHS. The MBSR program traditionally consists of 8 sessions plus 1-day retreat in week 6; however, a review of class contact hours and effect sizes for psychological distress did not find a significant association between effect sizes and class contact hours. 72 This suggests that adapting the traditional program to include shorter class times may be worthwhile. 18 We are currently investigating the possibility of adapting and/or abbreviating the MBSR program in a qualitative study using focus groups with breast cancer patients. Difficulties in recruiting cancer patients to studies have been noted previously, 73 and in future studies, a better more accessible explanation of MBSR could improve recruitment. We also found that there was no association between mindfulness practice and improvements in the BFI and HADS. This may in part be due to the small sample size in this study as these associations have been noted elsewhere. Other studies have found that increased mindfulness practice leads to increased participant mindfulness, which in turn leads to symptom reduction and improved well-being.39,64,74 Many studies suggest specific requirements for home practice but the relationship between optimal duration of home practice and outcomes is inconsistent,72,75,76 with many studies showing clinical benefit using reduced daily home practice of 15 to 20 min/day.77-79
Our results extend findings from early-stage breast cancer (0-III) studies24,27,39,80,81 and indicate that MBSR can improve anxiety in patients with advanced stage breast cancer. Mindfulness may mediate this reduction in anxiety by improving the emotional regulation strategies employed by people with physical illness as they ruminate less on the past and the future and are less likely to avoid difficult feelings and situations.18,82 Improvements in the TMS decentering scores have been shown to predict clinical improvements in stress, distress, 55 and depression. 83 Although our findings showed an improvement in TMS decentering scores, depression did not significantly improve in this study contrary to other MBSR and breast cancer studies.39,80 This is probably because the level of depression in our study participants was not particularly high at baseline perhaps because 47% of the participants were taking some form antidepressant. However, our finding that MBSR improves the QoL and sleep in breast cancer patients is consistent with other studies22,84 in early breast cancer. Because of considerable uncertainty surrounding these results due to the small sample size, the quantitative results of this feasibility should be interpreted with great caution. A logical approach to outcome measures in a future full RCT would be to include both disease-specific and generic QoL measures. We could consider using the EORTC-8D 85 measure to assess responsiveness of both measures in patients with cancer, deriving QALYs as a health economic measure from the disease-specific QoL measure.
The mixed methods design is strength of the study. Using both qualitative and quantitative methods of data collection and analysis has allowed us to answer the different questions posed by the feasibility and acceptability objectives. Utilizing both types of data and merging the data during the interpretation phase has enabled us to gain a more comprehensive account of the data. For example, we could quantitatively monitor participants’ attendance and completion of the course and adherence to home practice while the qualitative data allowed us to understand and interpret this data in more depth.
The study has limitations. Although appropriate for a feasibility pilot, the small sample size and the lack of educational and ethnic diversity of our participants (mostly white English middle class and with higher or further education) does not permit us to generalize these results to the population of women with MBC. The absence of a control group raises the question as whether the effects are really attributable to the practice of MBSR rather than nonspecific ingredients such as recruitment to a study, the role of the instructor, and group dynamics; further studies must address this issue. The participants in this study were a highly motivated group and their commitment to the course may have been in part due to being part of a research study. The third MBSR course only had 4 participants, and this could be a problem as most MBSR sessions are conducted with larger groups. However, none of the 4 participants indicated a problem with being part of a small group.
In conclusion, this feasibility study provided encouraging evidence that MBSR is acceptable to those participants willing to commit to the program. MBSR can be delivered to patients with MBC although an adapted shortened MBSR course may improve recruitment and adherence. The pilot element of the study provides preliminary evidence for sample size calculation for anxiety and QoL with the effect sizes, depending on the study design and the form of control group used in subsequent studies. Given the paucity of nonphar-macologic interventions available to this group of women, this study is an important step in filling an unmet need and providing an important enabling avenue for self-care and ongoing survivorship. These results suggest that further work evaluating MBSR in a more cost-effective and accessible format is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received financial support from National Institute for Health Research, Research for Patient Benefit grant award no: PB-PG-0408-16155. It funded Dr Caroline Eyles; Dr Leydon and Professor Lewith received a small allocation from the grant for time spent working on the grant as Principal Investigators.