
Abstract
Background. Physical activity has been demonstrated to increase survival in breast cancer patients, but few breast cancer patients meet the general recommendations for physical activity. The aim of this pilot study was to investigate if a supervised integrated counseling and group-based exercise program could increase leisure-time activity in women with breast cancer. Methods. This pilot project, designed as a single-arm study with pre-post testing, consisted of 24 classes of combined aerobic and strength exercise training as well as classes on dietary and health behavior. A total of 48 women with breast cancer who were undergoing or had recently completed anticancer treatment completed the study. Leisure-time physical activity, grip strength, functional capacity, quality of life (QoL), and depression were assessed at baseline, after intervention, and at the 12-week follow-up after intervention. Results. The breast cancer patients increased their leisure-time physical activity (P = .004), global strength (P = .004), functional capacity (P = .001), and QoL (P = .009), and their depression score (P = .004) significantly decreased. These improvements were independent of whether the patients were in ongoing therapy or had completed their treatment. Conclusion. This integrated intervention may produce lifestyle changes in breast cancer patients and survivors using the teachable moment to increase their leisure-time physical activity and, thereby, their QoL.
Keywords
Introduction
Exercise training has been established as a feasible and safe intervention during or after neoplastic treatment in breast cancer patients. 1 Numerous studies have shown that exercise can prevent and control various treatment-related side effects, including functional limitations, physical capacity, anxiety, and sleep disturbance.2-4 In the longer term, an active lifestyle has been demonstrated to increase survival in women who maintain a moderate level of activity (30-75 minutes of brisk walking 5 days a week).5,6 Specifically, physically active breast cancer survivors have a 51% to 85% lower cancer-specific mortality and 33% to 82% lower all-cause mortality. 7 But despite this, most breast cancer patients reduce their physical activity levels during and after cancer treatment. 8 In 2010, a roundtable meeting of the American College of Sport Medicine (ACSM) published guidelines for cancer survivors, defining that the recommended amount of exercise was 150 minutes per week of aerobic exercise at moderate intensity and 2 to 3 times weekly sessions of strength training, including training of major muscle groups. 1 But only 30% to 47% of breast cancer survivors follow these exercise recommendations.9,10
The cause of reduction in physical activity levels is multifactorial, with treatment-related side effects, 11 fatigue, depression, anxiety, and weight gain being common limiting factors. 11 As a consequence, some breast cancer patients find it difficult to begin or maintain physical activity at the minimal recommended levels. A typical obstacle includes lack of directions from experts to guide patients, who are unsure of the safety and efficacy of the exercise they perform. 12 Studies using integrated approaches have been conducted to promote a healthy lifestyle in cancer patients.3,13-15 As principal findings, these studies showed that theoretical and educative interventions, together with supervised practical training sessions, significantly improved total physical activity after intervention.
In contrast, unsupervised interventions such as phone or e-mail counseling on exercise may show improvements in behavioral changes immediately after the intervention, 16 but this improvement is not maintained in the follow-up period.17,18 This suggests that close intervention and follow-up are necessary for more permanent changes in patients’ behaviors. A cancer diagnosis may be a potential “teachable moment,” where patients are particularly motivated to make lifestyle changes. 10 Given this, it is important to approach the patients with an integrated intervention (consisting of training sessions and an educative program),10,12 which can explain the benefits of being active and eating healthy, providing tools to help the patients maintain their lifestyle changes.
Taking this into account, the hypothesis of this pilot project was that a guided integrated group exercise program combined with an educational program on healthy lifestyle would increase the adherence to exercise in breast cancer patients and survivors. Therefore, the first aim of this pilot study was to examine the effects of a comprehensive and specific group exercise program on leisure-time physical activity during and 3 months after the intervention. The secondary aim was to increase functional capacity, strength, and QoL through this intervention.
Material and Methods
Design and Inclusion/Exclusion Criteria
This study was performed as a collaboration between Universidad Politécnica de Madrid (UPM) and Asociación de Cáncer de Mama de Madrid (ASCAMMA). The project was carried out at the facilities of the Physical Activity and Sport Science Institute (INEF) and was approved by the Ethical Committee of the UPM. A single arm pilot project with pre-post test was designed. 19
Women showing interest were contacted by phone or e-mail with study information. Following information, potential participants were asked to fill out an initial questionnaire. Participants had to be older than 18 years and live in the Madrid Community. Participants should have been diagnosed with stage I to IIIA breast cancer and been operated on at least 1 month before enrolment. The patients could receive neoadjuvant, adjuvant, local or systemic and endocrine treatments, but this should not have been completed more than 10 years from the date of entry. The patients were not supposed to surpass a moderate level of exercise (300 min/wk) at inclusion. Exclusion criteria included serious medical risk such as unstable cardiac condition, severe pulmonary disease, severe back pain, uncontrolled hypertension, immune or endocrine abnormality, mental illness, and anticoagulant treatments. In addition, individual evaluation for participation was performed by the oncologist or primary care provider. A total of 50 women were recruited between October 2011 and June 2012 by ASCAMMA and oncologists at participating hospitals and provided written informed consent.
Intervention
The exercise program was designed and conducted by a qualified exercise physiologist with oncological training. It consisted of a twice-weekly (Monday and Thursday) supervised training program developed in a familiar and trusted environment, which promoted socialization between participants. Participants exercised twice a week for 12 weeks (24 sessions). They wore heart rate monitors during each exercise session. The intensity was progressively increased from 65% to 85% of heart rate reserve 1 for aerobic activities and by 8 to 15 repetitions in 2 to 3 sets for the strength exercises. Completion of the intervention was defined as attendance to 80% or more of the sessions. Except 2 dropouts, who left because of treatment-related side effects and who were not included in the analyses, all participants completed more than 80% of the training sessions.
Every supervised session had the same structure and duration (60 minutes). 20 The ACSM Guidelines for Cancer Patients were followed for the session design. 1 Designed sessions consisted of a warm-up of 10 minutes walking and doing articular movements. The aerobic part consisted of 25 minutes of designed whole-body exercises (ie, aerobic and step) to increase the participant’s functional capacity. After that, 15 minutes of upper-limb strength exercises with elastic bands to improve strength and increase arm lean mass was performed, focusing on chest and dorsal exercises. The last 10 minutes included whole-body stretching to improve joint mobility and muscle flexibility. 21
The exercise program was complemented with an educational program about exercise and nutrition. One class of exercise prescription was conducted to orient the patients about exercise recommendations and how to adapt it to their personal necessities.
The nutrition program consisted of 3 theoretical and practical classes, where specific terms of nutrition and diet were explained. The first class explained the different groups of nutrients. The second class was a practical class about how to interpret food labels and relating measurements of food portions with recommendations for a healthy diet. The final session addressed the 10 best (ie, rich in antioxidants) and the 10 worst (ie, rich in animal fat) dietary components, which might prevent or promote cancer. Teachers recommended a Mediterranean diet. 22
Follow-up Period
After finishing the 12-week exercise and educational program, participants were encouraged to continue the active lifestyle, but no contact was made. In addition, they did not know that they would be evaluated 3 months after the program had finished. Participants were contacted by mail, and 32 participants returned to be evaluated.
Assessments
All clinical and patient-reported outcomes were assessed at baseline, after 12 weeks of intervention, and at the 12-week follow-up after the end of the intervention.
Demographic and Descriptive Data
Age, marital status, profession, subtype of tumor, type of resection, lymph node resection, and type of endocrine medication were recorded at baseline in an individual interview.
Adherence and Leisure-Time Exercise
Adherence was assessed based on attendance at each physical activity training session. Leisure-time physical activity was assessed by the validated Godin Leisure-Time Test questionnaire.23,24 Patients had to indicate how many times a week they had been exercising for at least 15 minutes. The performed exercises are divided according to intensity—that is, low intensity, medium intensity, and high intensity. The provided number is multiplied by 3, 5, or 9, respectively, and the results for each intensity activity are summed. In the second part, the patient must indicate how often they did activities at intensities that made them sweat rarely (1), sometimes (2), or often (3). To complete exercise level information, the participants were asked to define their quantity of physical activity as sedentary (defined as less than 30 minutes of exercise per week), low level of physical activity (defined as 30-150 min/wk), moderate level of physical activity (defined as 150-300 minutes of exercise per week), or high level of physical activity (defined as 300 minutes or more of exercise per week). These data were collected in the individual interview. Participants were instructed not to include their program classes into their assessment because these were mainly for instruction.
Physical Variables
Physical effects were monitored to control the effectiveness of the program on the physical status of the patient. Functional capacity was assessed by the 6-Minute Walking Test. This test consists of walking as fast as possible for 6 minutes, in laps of 25-m distances. At the end of the test, the total distance walked by the patient is noted. This test was performed according to the recommended American Thoracic Society ATS guidelines.25,26
Isometric strength was assessed by grip strength in the arms, legs, and back. These tests are isometrics and do not require articular movements. Global strength was assessed by the strength index, which was obtained by adding all grip strength values and dividing the result by the participants’ weight. Grip Strength Dynamometer T.K.K.5401 was used to test arm strength and T.K.K.5402 to test leg and back strength.21,27
Anthropometric Data
Weight and height were collected at baseline, at the end of the intervention, and at follow-up assessments. Arm volumetries were performed to check for possible lymphedema.
Psychological Variables
Quality of life (QoL) was assessed by Functional Assessment of Cancer Therapy–Breast (FACT-B). 28 It is a Likert test where the patients have to choose which level of a specific affirmation fits one’s present state. This level is calculated based on the FACIT.org guides to this questionnaire to a single score. Higher scores are related to better QoL.
Health perception was assessed by the SF-36 (Short Form–36 Health Survey).29,30 This test shows 36 affirmations and questions and gives the patients different options to choose the one most similar to her feelings. The SF-36 test was analyzed by norm-based score to the population mean, and a higher score is interpreted as better health perception and QoL. This test is divided into 2 separate dimensions, and the results are presented as Physical Component Summary (PCS) and Mental Component Summary (MCS).
Depression grade was assessed by the Center of Epidemiology Studies–Depression (CES-D) questionnaires. 31 CES-D is also a Likert test, where the patients have to choose which level of a specific affirmation fits one’s present state. Each choice is given a number according to the guidelines of the test, and a final score is calculated. A high score implies higher levels of depression, and a score of 16 points or more is considered to denote being depressed.
Statistical Analyses
Descriptive analysis was performed for the frequency and percentage of the demographic and descriptive characteristics. The effects of intervention on continuous outcomes were analyzed using a 1-way ANOVA with repeated measurements and post hoc planned comparisons performed with Bonferroni correction, examining all combinations of time points (overall baseline to 3-month follow-up, baseline to 12 weeks, and 12 weeks to 3-month follow-up). Between-group comparisons (in ongoing therapy or completed treatment) were performed using unpaired t tests. Effects of intervention on nonparametric outcomes were analyzed using he Friedman test, and post hoc planned comparisons were done with “a posteriori” multiple comparisons. Spearman correlation analyses were used to examine the associations between leisure-time exercise levels and functional outcomes (functional capacity and strength) and between leisure-time exercise and psychological variables (QoL, depression, and health perception) for data obtained immediately after the intervention or at follow-up. Statistical analysis was developed with SPSS v18 software. Data are presented as means ± standard deviation, and P < .05 was considered statistically significant.
Results
Demographic and Clinical Characteristics of the Study Population
From October 3, 2011, to June 29, 2012, 48 women with breast cancer completed the exercise intervention. A total of 87 women were contacted by e-mail and phone, 67 were screened, 58 were eligible, and 50 were finally enrolled (86% enrollment rate of those who were eligible). There were no differences in age, profession, marital status, physical activity level, and kind of treatments between women who were screened and those who declined screening (Figure 1).

Flow chart: CONSORT diagram for study recruitment and assessment. The dropouts are noted and explained.
Participant characteristics are shown in Table 1. Most of the participants had a partner (74%). A little more than half of the women had tumors that were estrogen receptor and progesterone receptor positive (56.8%), and almost all participants had been operated on when enrolled (96%). At inclusion, 16% (8 patients) were receiving chemotherapy and 12% (6 patients) radiotherapy. Totally, 28% (15 patients) were in ongoing treatment during the exercise intervention. None of the patients presented with lymphedema at baseline assessment. All participants presented with low physical activity levels; 32% (16 patients) defined their behavior as sedentary, 46% (23 p patients) performed a low amount of exercise, and 22% (11 patients) were physically active at the medium level. No patient performed high-intensity exercise at inclusion.
Sample Characteristics.
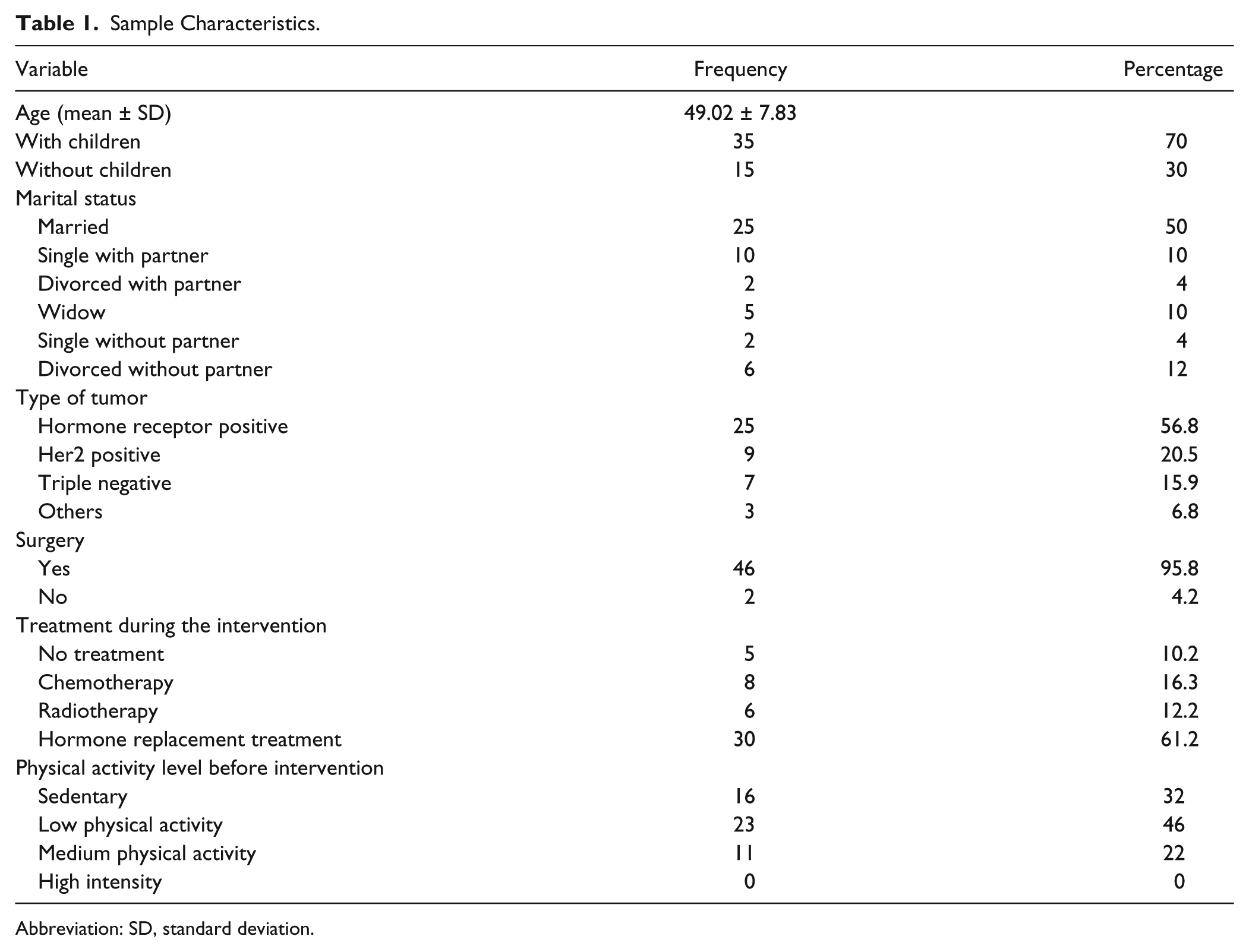
Abbreviation: SD, standard deviation.
Exercise Prescriptions and Leisure-Time Exercise Results
The adherence rate to the training sessions was on average 92%. Women under treatment had an average adherence rate of 85.5%, whereas women not in ongoing treatment had an adherence rate of 98.5%. This shows a high adherence for both groups, but as expected, the patients who had completed treatment showed better compliance.
In the first part of the leisure-time activity test (Godin 1, Table 2), a significant increase in leisure-time exercise level was observed (F2 = 6.77; P = .004, Figure 2A). This effect was mainly driven by an increase in leisure-time exercise level from the baseline assessment to after the 12-week intervention (P = .039). In the 3-month follow-up period, the patients maintained their increased leisure-time exercise level but did not increase it further (P = 1.0). Thus, over the 24 weeks, the patients maintained the effect obtained during the intervention period (P = .021).
Means and Standard Deviations (SDs) of Baseline (Pre), Postintervention (12-Week), and 3-Month Follow-up (24-Week) Measures and Statistical Significance Representing the 1-Way ANOVA and the Post hoc Bonferroni Analysis.

Functional Assessment of Cancer Therapy–Breast: higher scores represent better quality of life.
Short Form–36 Items Questionnaire: higher score represents better health perception. SF-36 is presented by norm-based score to the population mean.
Center for Epidemiologic Studies–Depression: higher score represents higher level of depression.

Changes in leisure-time exercise levels over time. A. Godin 1: variation over time in the quantity and intensity of leisure-time exercise levels. B. Godin 2: How often they sweat during exercise.a
The second part of the leisure-time activity test (Godin 2, Table 2), which evaluates how often patients perform exercise that makes them sweat, showed significant differences between assessments (F2 = 16,94; P = .0001; Figure 2B). During the exercise intervention, this score improved significantly (P = .011), and a tendency to further increase was observed in the follow-up period (P = .07). Thus, over the 24 weeks, the patients steadily increased their training intensity (P = .0001).
Subanalyses showed that there was no difference in the improvements in Godin scores between patients in ongoing treatment and patients who had completed treatment. According to the ACSM categories, the patients increased both the intensity and number of minutes of exercise per week (χ22 = 29.18; P = .001). This effect was most pronounced during the intervention period (P < .05).
Effect on Functional Parameters
In line with the increase in physical activity levels and leisure-time exercise levels, we found improvements in the functional parameters of isometric grip strength and 6-Minute Walking Test, as a measure of physical capacity (Table 2).
Global Strength Levels
Significant increases were found in the Strength Index assessments across the intervention (F2 = 6.78; P = .004). The main improvement was observed during the 12 weeks of training (P = .04), and the patients maintained their increased strength during the follow-up period (P = 1.00). Thus, over the 24 weeks, the patients significantly improved their upper and lower body strength (P = .03).
Physical Capacity
Physical capacity also increased across the intervention period (F2 = 45.95; P = .0001). Bonferroni post hoc tests showed significant improvements between all assessment points. Comparing baseline with posttreatment showed significant improvement in physical capacity (P = .0001), and the physical capacity also improved in the 12 weeks of follow-up (P = .009). Thus, over the 24 weeks, a significant increase in physical capacity was found (P = .0001).
Correlations Between Increased Leisure-Time Exercise and Functional Outcomes
A positive correlation was found between physical capacity and the Godin 1 leisure-time exercise test, showing that an increase in leisure-time exercise increases physical capacity (r2 = 0.51; P = .002). No significant correlation was found between leisure-time exercise and strength (r2 = 0.26; P = .14).
Anthropometric Assessments
No differences were found in volumetries of arms (P > .05) or body weight (P > .05) across the intervention.
Effects on Psychosocial Parameters
Functional Assessment of Cancer Therapy–Breast
In the QoL assessment, significant improvements were found in FACT-B values across the intervention (F2 = 5.471; P = .009; Table 2). No significant differences were found between baseline values and values after the training period (P = .14), nor in values at the 12-week follow-up (P = .65). But over the 24 weeks, significant increases in QoL were found by Bonferroni post hoc analysis (P = .03).
SF-36 (Short Form–36 Health Survey)
In the PCS, a significant improvement across the intervention was found (F2 = 8.13; P = .001; Table 2). Using Bonferroni post hoc analysis, no significant difference was found between baseline and postintervention. Interestingly, significant improvement was found between baseline and follow-up assessment (P = .019) and between posttreatment and follow-up results (P = .009).
In the MCS, significant improvements were also found across the intervention (F2 = 4.16; P = .025). However, Bonferroni post hoc analysis did not show significant differences between assessment points. Between baseline and postintervention, a borderline significance was found (P = .054). Our trial was not designed to be powered for evaluations in this dimension, indicating that larger sample numbers could have resulted in significant results in this dimension.
Center of Epidemiology Studies–Depression Scale
Finally, the depression test also showed significant improvements across the intervention (F2 = 6.87; P = .004; Table 2). Post hoc analysis using the Bonferroni test showed a significant improvement between baseline and postintervention (P = .009). However, no further improvement between the posttreatment and follow-up periods was observed (P = 1.000). Subanalyses showed that there was no difference in the improvements in psychosocial outcomes between patients in ongoing treatment and patients who had completed treatment.
Correlations Between Increased Leisure-Time Exercise and Psychosocial Parameters
No correlations were found between leisure-time exercise and FACT-B results, mental or physical dimensions of SF-36, or depression levels.
Discussion
The goal of this pilot study was to investigate if an integrated group-based exercise intervention could increase leisure-time exercise levels in women with breast cancer. Indeed, we found that this intervention increased leisure-time activity close to the recommended levels as given by the Godin scale values, which surpassed 24 points. 32 In fact, most participants ended up following the ACSM guidelines, and 88% of them increased their physical activity to >150 min/wk, meeting the levels thought to elicit health benefits. Maintaining a healthy lifestyle is related to increased survival in breast cancer survivors as well as decreased long-term side effects5,33; so finding appropriate and effective ways to promote a healthy lifestyle could prevent comorbidities, sparing the patients further disease and, in addition, saving public money.
Breast cancer patients decrease their activity levels, and because of both short- and long-term treatment effects, it has been difficult to break this pattern. Our results indicate that with only 12 weeks of intervention of just twice-weekly sessions, significant improvement in physical activity levels and functional outcomes can be obtained. This intervention is at an extent that is acceptable for most patients and, therefore, presents a feasible way of lifestyle intervention in breast cancer patients. Our results on the activity levels are in accordance with those in previous studies13-15 and add to these studies by proving the possibility of improving physical activity levels at the time of breast cancer treatment and not long into the survivorship. 12
A cancer diagnosis may be a potential “teachable moment,” where promotion of positive changes in various behaviors, attitudes, and beliefs are attainable. For this reason, high-quality information related to dietary and physical activity issues have to be transmitted to patients in order to approach this window of change in their lifestyle, as close as possible to cancer diagnosis. 34 When designing exercise trials for cancer patients, it is worth noting that 84% of patients would like to receive exercise counseling at some point during their cancer experience; 85% of cancer survivors preferred exercise counseling face-to-face, and 77% preferred to receive it from an exercise specialist. 35 As for the settings, it is important to note that many exercise interventions trials have been conducted mainly focusing on feasibility and improving functional and psychological parameters. 36 Much fewer studies have addressed the effect of interventions on leisure-time activity levels, in particular in the follow-up period. 37 Studies using unsupervised training may improve leisure-time activity levels initially, but these increased levels are not maintained. This pilot project is one of the first studies to show that an integrated approach with group-based training twice a week and educational classes can in fact improve leisure-time activity levels to the recommended levels, and these are also maintained into the follow-up period. Another strength is the group-based training, which promoted a social dimension and offered patients a trusted environment, where they could speak about cancer without reservations and be understood by others in a similar situation.
Along with other exercise intervention trials in breast cancer patients, we found improvement in QoL, mental functioning, and depression. Recent Cochrane reviews showed that exercise during anticancer treatment, as gathered from 56 studies, produces beneficial effects on QoL, physical functioning, role function, social functioning, and fatigue, and in addition, the positive effects of exercise interventions are more pronounced with moderate- or vigorous-intensity versus mild-intensity exercise programs in these patients. Similarly, for cancer survivors, a review of 40 studies indicated that exercise improved QoL and certain health-related QoL domains, including cancer-specific concerns (eg, breast cancer), body image/self-esteem, emotional well-being, sexuality, sleep disturbance, social functioning, anxiety, fatigue, and pain at varying follow-up periods.
Intuitively, improvements in psychological variables could act as a motivation factor for maintaining exercise levels after intervention, but future research is needed to verify that such a causal relationship exists. Breast cancer patients who participate in our study scored higher on QoL and health perception and lower on depression than before the intervention.
Moreover, in line with other exercise intervention trials in breast cancer patients, we saw increases in muscle strength and physical capacity. Global strength index increased 8% and physical capacity by 19% during our intervention compared with baseline levels. Previous studies have shown similar increases in muscle strength with combined training.38,39 Regarding the initiation of training, a 63% increase in 1-RM bench press was observed in women who started training just after finishing anticancer treatments compared with a 12% increase in women who started training 6 months after their treatment. 40 This proves that there is a large window of improvement with training during or right after anticancer treatment. With respect to physical capacity, McNeely et al 41 reported increases in the 6-minute walking test of 35 m. Our results showed an average increase of 6 m, but our patients did already walk >675 m (27 paths) at baseline, compared with 300 m (12 paths) in the McNeely study. It is important to note the positive correlation found between leisure-time exercise levels and the improvements in physical capacity, which confirm the positive effect on patients’ lives.
There are certain limitations to this study. First, the absence of a control group prevents us from relating our findings to the development in a group without interventions. The nutrition classes were not evaluated, which limited our ability to describe the effect of these classes on lifestyle changes in patients. Yet our perception was that these classes were an essential part of the process. Another specific difficulty was the lack of knowledge in Spain about the benefits of exercise in the oncological setting. In addition, it is important to note that this was a pilot study preceding a larger intervention study, so data analysis provides the basis to design an adequate intervention for breast cancer patients on a larger scale.
This project highlights the usefulness of promoting healthy lifestyle and the effectiveness of this specific program as an integrative tool to work with patients during treatments. However, because of the above-mentioned limitations, further randomized controlled trials have to be developed.
In conclusion, we found that a guided, integrated group-based exercise program, which included an educational program on healthy lifestyle, promoted such healthy lifestyles in breast cancer patients, with increased leisure-time activity 3 months after the intervention, as well as improvements of parameters related to physical capacity, muscle strength, and mental well-being. Of particular interest is that women undergoing anticancer treatment had adherence levels almost as high as women who had completed their treatment as well as improved leisure-time activity and physical and mental functioning to a similar extent. This indicates that this group is highly motivated, and with proper counseling and recommendations from health professionals, these patients can change their behavior, ensuring better survivorship.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Technical University of Madrid. Asociación de Cáncer de Mama de Madrid,. Hospital Universitario Puerta de Hierro, Majadahonda, Madrid, and Hospitales de Madrid have collaborated in sample recruitment.