
Abstract
Background. Fatigue is a distressing and pervasive problem for people with cancer. In recent years, acupuncture has gained increasing attention among researchers as an alternative management strategy for cancer-related fatigue (CRF). This review aimed to evaluate the effectiveness of acupuncture for CRF. Methods. Five databases (Medline, CINAHL, Scopus, the Cochrane Library, and CAJ Full-text Database) were searched up to May 2013. Randomized controlled trials (RCTs) of acupuncture for the treatment of CRF were considered for inclusion. Results. Seven RCTs were included for meta-analysis, involving a total of 689 subjects. Three studies compared acupuncture with sham acupuncture for CRF with follow-up at 10 weeks; the standardized mean difference (SMD) for general CRF change values was −0.82 (95% confidence interval [CI] = −1.90 to 0.26). When acupuncture plus education intervention was compared with usual care, there was a statistically significant difference for the change score of general CRF (SMD = −2.12; 95% CI = −3.21 to −1.03). The SMD for general CRF change scores between acupuncture with no treatment or wait-list control was −1.46 (95% CI = −3.56 to 0.63). Finally, the SMD for general CRF change scores between acupuncture with acupressure or self-acupuncture was −1.12 (95% CI = −3.03 to 0.78). Three trials reported data for general quality of life and functioning status, reporting enough data for statistical pooling but showing no statistically significant difference (Z score = 1.15, P = .25, SMD = 0.99, 95% CI = −0.70 to 2.68 and Z score = 1.13, P = .26, SMD = 1.38, 95% CI = −1.02 to 3.79, respectively). The I2 statistics of all statistically pooled data were higher than 50%, indicating heterogeneity between the trials. Conclusions. There were 4 sets of comparison for the effectiveness of acupuncture for CRF; statistical pooling of the reduction in CRF from baseline to follow-up showed in favor of acupuncture. However, 3 sets of comparison for the pooled estimates of effect sizes had no statistical significance. Although one set of comparison (acupuncture plus education interventions vs usual care) had statistically significant differences, it is unclear whether this pooled positive outcome is attributable to the effects of acupuncture or to the education intervention. In addition, the duration of follow-up in these included trials was up to 10 weeks, and some RCTs had methodological flaws. Further rigorously designed RCTs adhering to acceptable standards of trial methodology are required to determine the effectiveness of acupuncture and its long-term effects on CRF.
Keywords
Introduction
With the advancement of medical technology and treatment of cancer, the number of cancer survivors is increasing steadily. Nearly 25 million people live with cancer worldwide. 1 Cancer-related fatigue (CRF) represents a major public health concern. 2 Prevalence estimates of individuals who experience CRF have varied across studies from 25% to 100% depending on the type and stage of cancer and treatment types. 3 The multiple and varied effects of fatigue do not dissipate once cancer treatment has been completed. 4 It is now increasingly recognized that many individuals who are disease free continue to experience fatigue for months or even years following treatment completion.4,5
Fatigue in people with cancer is one of the most common and disabling symptoms of their condition, and is notably associated with mortality. 6 Studies have shown that CRF affects multiple aspects of individuals’ lives, such as performing activities of daily living, decreasing functional status, and limiting overall quality of life.7,8 In addition, CRF is associated with decreased survival and interferes with employment, family life, social relationships, and sex life.9-11
There are limited nonpharmacologic treatment approaches for the management of CRF. However, there is growing evidence of the impact of complementary and integrative medicine on CRF. 12 Among various complementary and integrative medicine interventions, acupuncture has gained increasing attention as a tool for managing CFR. Vickers et al 13 published the first empirical study to examine the effectiveness of acupuncture for CRF. Because of their promising findings, several randomized controlled trials (RCTs) have been published reporting the efficacy of acupuncture in alleviating CRF. A recent review by Finnegan-John et al 12 comprehensively examined a range of complementary and alternative medicine interventions for CRF, while Posadzki et al 14 focused on evaluating acupuncture for CRF. However, neither of these narrative reviews quantitatively clarified the effectiveness of acupuncture for the management of CRF.
Aims
Because of growing interest in the use of acupuncture for CRF, this meta-analytic review aimed to quantitatively evaluate the effectiveness of acupuncture for the management of CRF based on available studies to date, to explore the effectiveness of different types of acupuncture interventions, and to identify implications for future research.
Methods
Data Sources and Searches
Systematic searches of 5 databases were conducted in Medline (database start date to May 2013), CINAHL (database start date to May 2013), Scopus (database start date to May 2013), the Cochrane Library (database start date to May 2013), and CAJ Full-text Database (database start date to May 2013). Articles published in English and Chinese were included. RCTs of acupuncture for the treatment of CRF were considered for inclusion. The search terms included were “acupuncture,” “acupuncture therapy,” “fatigue,” “cancer-fatigue,” “cancer,” “carcinoma,” “tumour or tumor,” and “malignance.” The process of study selection consisted of 2 steps: 2 researchers independently screened the titles and abstracts of the studies (YCZ, TZL), and all potentially relevant studies meeting the predefined inclusion criteria were selected for inclusion in the review. Disagreements were resolved by a third review author (JF-J).
Study Population
In the planning stage, this review set out to focus on cancer survivors: those individuals who completed postprimary treatment. During the searching stage, it became clear that the number of studies on acupuncture for cancer survivors is limited. Therefore, our inclusion criteria were expanded to include cancer patients undergoing treatment.
Interventions and Outcome Measures
Acupuncture was defined as “a process involving needles that were required to be inserted in the skin (without an injection) at classical meridian points.”
15
Sham acupuncture was defined as
any intervention designed to make patients believe they are receiving acupuncture by either puncturing a location near the acupoint with tingling only but not De Qi (arrival of energy), or stimulated acupuncture technique using a toothpick or other needle-like object in the needle guidetube.
16
Studies of acupuncture that did not involve needle insertion, such as laser acupuncture or electro-acupuncture without needles, were excluded. The primary outcome was cancer-related fatigue measured by a validated scale. The secondary outcomes were quality of life and functional well-being.
Data Extraction and Assessment of Risk of Bias
Data were extracted by 2 authors (YCZ, TZL). Disagreements concerning data extraction were resolved by discussion. The methodological quality of all the included studies was assessed by 2 authors independently (YCX, TZL). The risk of bias of methodological quality was assessed using the Cochrane Assessment Tool, which consists of 7 domains. 17
Data Synthesis
The data were analyzed using the Cochrane Collaboration’s Review Manager (RevMan 5.1). 17 For continuous variables (eg, CRF reduction, functioning, or quality-of-life improvement), mean difference (MD) was calculated when outcomes were measured using the same scale, and the standardized mean difference (SMD) was used when different scales were used among different trials, with corresponding 95% confidence intervals (CI). 18 If data of standard deviations (SDs) were missing for statistical pooling of effect size calculation, missing SDs were replaced by calculating the trial data using standard error of the mean or 95% CI. 18
Clinical heterogeneity was determined by discussion among the review authors and clinically heterogeneous trials were not combined statistically. Statistical heterogeneity was calculated by using the χ2 and I2 statistics to determine whether to use the random-effects model or fixed-effects model for meta-analysis. 18 A χ2 of P value greater than .1 and an I2 value of less than 50% were considered to indicate statistical homogeneity. 18 The random-effects model was used to combine clinically homogeneous but statistically heterogeneous clinical trials, whereas clinically and statistically homogeneous trials were combined using the fixed-effects model.
Results
A total of 8 RCTs were identified, but 1 study was an unpublished thesis and was therefore excluded. The selection of studies is shown in Figure 1. The characteristics of included trials19-25 are summarized in Table 1. Three trials19-22 used a small sample size (12-30 patients). Two studies23,24 used a pragmatic RCT design and 1 study 22 adopted an open-label design. Duration of interventions ranged from 2 to 8 weeks. Outcome measures all used validated scales.

PRISMA flow diagram of study selection.
Characteristics of Included Trials on Acupuncture for Cancer-Related Fatigue.

Abbreviations: AP, acupressure; AT, acupuncture; BFI, Brief Fatigue Inventory; CES-D, Center for Epidemiological Studies–Depression Scale; HADS, Hospital Anxiety and Depression Scale; FACIT-F, Functional Assessment of Chronic Illness Therapy–Fatigue Subscale; FACT-B, Functional Assessment of Cancer Treatment–Breast; FACT-COG, Functional Assessment of Cancer Treatment–Cognitive Function; FACT-G, Functional Assessment of Cancer Treatment–General; MFI, Multidimensional Fatigue Inventory; RCT, randomized controlled trial; TCM, traditional Chinese medicine; UC, usual care; W-BQ 12, Well-Being Questionnaire.
Each included trial was evaluated in terms of its risk of bias (Figure 2). Three trials22-24 had a high risk of bias and 4 trials19-21,25 had a relatively low risk of bias. Major sources of risk of bias related to allocation concealment, blinding study subjects or research personnel, and blinding outcome assessment. Assessment of risk-of-bias by individual trials is presented in Figure 3. One trial 19 had a high drop-out rate in the sham control group (27.27%) but failed to address this incomplete outcome with intention-to-treat analysis. Four trials22-25 lacked a sham control group, which would help distinguish between benefits that could be ascribed to personal attention and group interaction as opposed to the specific effects of acupuncture. Three trials22-24 failed to blind participants in relation to intervention delivery and were therefore open to bias with false-positive results. The treatment arm in 1 trial 22 was a combination of acupuncture and education interventions, and it was impossible to parse out whether it was the acupuncture or educational components causing the effects.
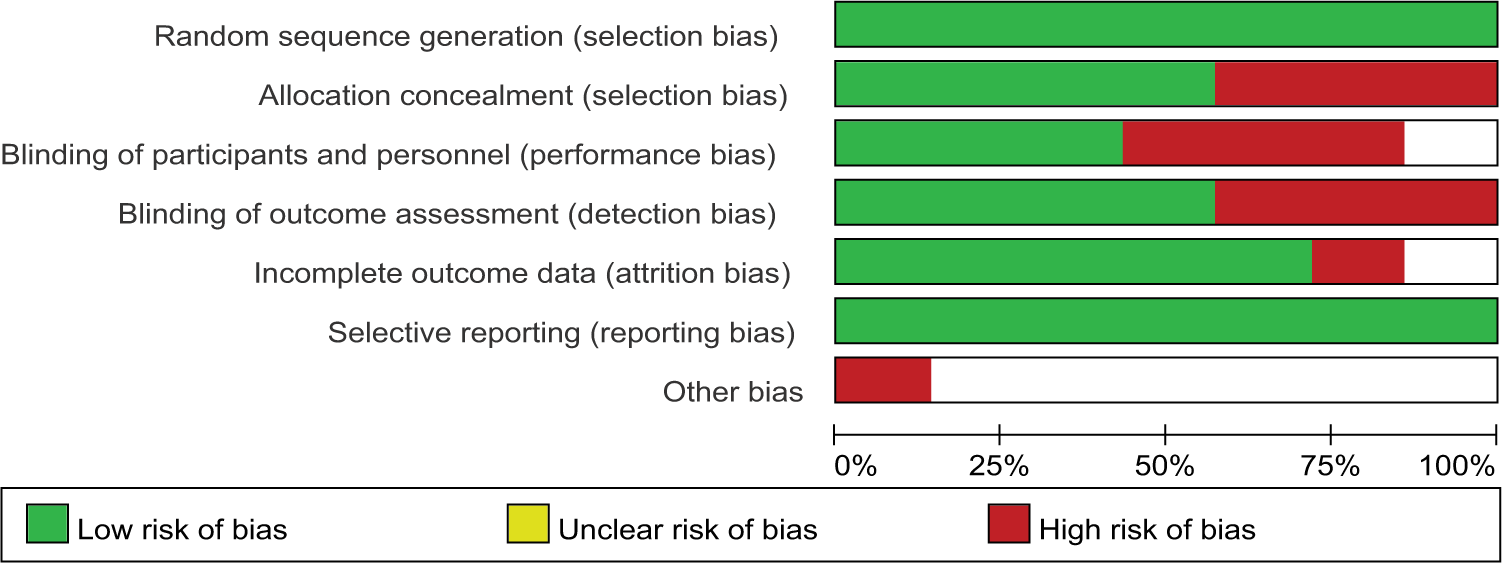
Overall risk of bias assessment using the Cochrane tool.

Risk of bias assessment by individual trials.
Seven RCTs were included for meta-analysis, involving 689 subjects. Through 6 sets of statistical pooling, all change scores were assessed with a follow-up to 10 weeks. Three studies19-21 compared acupuncture with sham acupuncture for CRF. The SMD for general CRF change values was −0.82 (95% CI = −1.90 to 0.26; Z score = 1.49, P = .14; Figure 4).

General cancer-related fatigue change score (acupuncture vs sham acupuncture) up to 10-week follow-up.
Two studies compared the effects of acupuncture plus an intervention with usual care: Johnston et al 22 integrated education with acupuncture as the treatment and Molassiotis et al 23 adopted acupuncture with usual care as the treatment. Data from a meta-analysis of these 2 studies showed that, overall, acupuncture plus an intervention had statistically significant effects in reducing CRF compared with usual care. The SMD was −2.12 (95% CI = −3.21 to −1.03; Z score = 3.81, P = .0001; Figure 5).

General cancer-related fatigue change scores (acupuncture plus an intervention vs usual care) up to 10-week follow-up
Two other trials21,24 compared acupuncture with wait-list control or no treatment. The SMD for general CRF change scores between acupuncture with no treatment or wait-list control was −1.46 (95% CI = −3.56 to 0.63; Z score = 1.37, P = .17; Figure 6), indicating no statistically significant effects of acupuncture for CRF.

General cancer-related fatigue change scores (acupuncture vs no treatment or wait-list control) up to 10-week follow-up.
Two studies24,25 compared the effects of acupuncture with other active treatment (acupressure or self-acupuncture). In a 2007 study, Molassiotis et al 25 compared the effects of acupuncture with those of acupressure, while in a more recent study, 24 the same authors conducted a comparison of acupuncture with self-acupuncture. Data from meta-analysis of these 2 trials showed no statistically significant effects in reducing CRF compared with other active treatments. The SMD was −1.12 (95% CI: −3.03 to 0.78; Z score = 1.15, P = .25; Figure 7).

General cancer-related fatigue change scores (acupuncture vs other treatment) up to 10-week follow-up.
For general quality of life and functioning status, 3 trials19-21 reported enough data for statistical pooling, and showed no statistically significant difference between acupuncture and sham acupuncture (SMD = 0.99, 95% CI = −0.70 to 2.68; Z score = 1.15, P = .25 and SMD = 1.38, 95% CI = −1.02 to 3.79; Z score = 1.13, P = .26, respectively; Figures 8 and 9). The I2 statistics of statistical pooling were all higher than 50%, indicating heterogeneity between the trials.

General quality-of-life change scores up to 10-week follow-up.

Depressive/negative well-being change scores up to 10-week follow-up.
Only 1 study reported safety issues related to acupuncture treatment: These included spot bleeding, bruising, feeling discomfort, and nausea. 25 In the study by Deng et al, 20 11 adverse events were reported, but the authors claimed that these adverse events were proven to be unrelated to acupuncture. Therefore, acupuncture seems to be relatively safe for CRF.
Discussion
To measure the effectiveness of acupuncture for CRF, 4 sets of comparisons were used as follows: acupuncture versus sham acupuncture, acupuncture plus an intervention versus usual care, acupuncture versus no treatment or wait-list control, and acupuncture versus other active treatment.
Only 1 comparison (acupuncture plus usual care or education intervention vs usual care) showed a statistically significant difference (Z score = 3.81, P = .0001). All other comparisons failed to show significant differences between acupuncture and sham acupuncture, or no treatment/wait-list control, or other active treatment, although forest plots from Figures 4, 6, and 7 indicate in favor of acupuncture. With regard to general quality of life, some improvements were demonstrated but without statistically significant differences. Similarly, there was some reduction in depressive symptoms but further trials are required to test its statistical significance.
This meta-analysis showed no statistically significant difference between acupuncture and sham acupuncture for CRF. This finding was consistent with a study by Azad and John, 26 which identified 25 randomized, sham-controlled studies in which acupuncture-point stimulation was used to treat a diverse range of symptoms of cancer. More than half (56%, n = 14) of these studies reported no statistically significant difference between acupuncture and sham acupuncture. 26 Consequently, the effects of acupuncture for CRF and other cancer-related symptoms may be attributed to nonspecific factors such as patient expectations and patient–practitioner interaction. The effectiveness of acupuncture for individuals with chronic low back pain was attributed to nonspecific effects by a meta-analysis of 13 RCTs. 15 In addition, there are well-established psychosocial predictors relating to the effects of acupuncture for pain. Bishop and Lewith 27 indicated that patients’ beliefs about acupuncture and factors related to therapeutic relationships, in particular patients’ perceptions of that relationship, are significant predictors of treatment outcomes. To address this issue, there is a need for larger trials, using rigorous methodology, to assess the specific effects of acupuncture.
In this meta-analysis, no study was found which examined the use of different acupuncture techniques for the management of CRF. Among 7 trials, 2 studies adopted traditional Chinese medicine styles, while the others used Western acupuncture techniques. Trials comparing different acupuncture techniques are warranted, as the traditional Chinese medicine style of acupuncture and Western acupuncture techniques may be based on totally different treatment protocols, in terms of commonly used acupuncture points, total of number of needle points, duration of needle retention, treatment frequency, and total number of sessions per treatment intervention.
Acupuncture is considered to be a safe technique, and evidence from this meta-analysis has demonstrated that there are no reported serious adverse events. A cumulative review estimated the risk of a serious adverse event related to acupuncture to be in the order of 0.05 per 10 000 treatments. 28 Zhang et al 29 conducted a systematic review of acupuncture-related adverse events, and they concluded that improper techniques of acupuncture were the main source of incidences of adverse events. One trial in this meta-analysis included a self-acupuncture arm, although the authors claimed these participants were trained by experienced acupuncturists. There is no guarantee that every participant could master the skills required to administer acupuncture, such as depth of needling and manipulation of needles in a proper way. Hence, further trials incorporating self-acupuncture as an intervention arm should be used cautiously.
A careful examination of the included studies reveals some methodological flaws in the trials. Three trials failed to blind research subjects, intervention delivery, and outcome assessors, introducing a high risk of bias into these trials. Despite the difficulties of blinding of research subjects and intervention delivery, studies should blind the outcome assessors to minimize potential methodological bias. Three trials included insufficient sample sizes, which meant there was a potential risk of overestimating positive outcomes. Four trials lacked a sham acupuncture group, which in turn meant that it was impossible to definitively attribute improved CRF in the acupuncture group solely to acupuncture itself. 26 Therefore, the reliability of the evidence presented here is clearly limited.
Additionally, there were some limitations to be considered when interpreting the results of this meta-analysis. Only 7 trials were included in the meta-analysis, and most of these had a high risk of bias in methodological quality. There is a need for high-quality clinical trials to test the effectiveness of acupuncture for CRF. This meta-analysis also found significant heterogeneity among combined trials, which still attributes to the methodological weakness of the included studies. Another limitation was that some trials neglected to report baseline data, which precluded us from performing further statistical pooling (eg, follow-up CRF score comparisons). In this respect, future trials of acupuncture for CRF would benefit from reporting outcomes in a standard way.
Conclusion
There were 4 sets of comparison for measuring the effectiveness of acupuncture for CRF; using statistical pooling, the findings for reduction in CRF from baseline to follow-up were in favor of acupuncture. However, 3 sets of comparison for the pooled estimates of effect size had no statistical significance. Although 1 set of comparison (acupuncture plus education interventions versus usual care) showed a statistically significant difference, it was unclear whether this pooled positive outcome was attributable to the effects of acupuncture or the education intervention. In addition, the duration of follow-up in the included trials was up to 10 weeks, and some RCTs had methodological flaws. Thus, further rigorously designed RCTs adhering to acceptable standards of trial methodology are required to determine the effectiveness of acupuncture and its long-term effects on CRF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.