
Abstract
Purpose. Radiation-induced oral mucositis is an acute morbidity seen in patients undergoing treatment for head and neck cancers. In this study, we evaluated the efficacy of turmeric in preventing radiation-induced mucositis. Methods. This was a single-blinded, randomized, controlled clinical trial and was conducted with head and neck cancer patients requiring 70 Gy of radiation or chemoradiotherapy (daily radiotherapy plus carboplatin once a week). Eligible patients (n = 80) were randomly assigned to receive either turmeric gargle (n = 40) or povidone-iodine ([n = 40] active comparator condition) during chemo/radiotherapy during the period of treatment. Oral mucositis was assessed using the RTOG (Radiation Therapy Oncology Group) grading system before the start, during, and at the end of the treatment by an investigator unaware of the treatment. The primary endpoint of this study was the incidence of mucositis every week during the 7-week period. The secondary endpoint was the effect of turmeric gargle on the incidence of treatment breaks, loss of scheduled treatment days, and decrease in body weight at the end of the treatment. Results. This study clearly suggests that when compared with the cohorts using povidone-iodine gargle, the group using turmeric as a mouthwash had delayed and reduced the levels of radiation-induced oral mucositis and was statistically significant at all time points (P < 0.001 to P < 0.0001). Additionally, the cohorts using turmeric had decreased intolerable mucositis (P < 0.001) and lesser incidence of treatment breaks in the first half of the treatment schedule before 4 weeks (P < 0.01) and reduced change in body weight (P < 0.001). Conclusions. Gargling with turmeric by head and neck cancer patients undergoing radiation therapy provided significant benefit by delaying and reducing the severity of mucositis. Turmeric is readily available, relatively inexpensive, and highly accepted making it useful in cancer treatment.
Introduction
Oral mucositis, an inflammatory response of the oral–pharyngeal mucosa in response to systemic chemotherapy or from radiotherapy for the head and neck carcinoma is extremely painful and increases morbidity of the patient. 1 Depending on the severity, oral mucositis is grouped as tolerable mucositis (grade 1 and 2 mucositis) and intolerable mucositis (grade 3 or higher). 2 In radiation treatment for the head and neck cancers, tolerable mucositis develops in all patients and is easy to manage.1,3 However, intolerable mucositis needs additional medical care for effective pain management and may also lead to use of gastrostomy tube or intravenous line for nutritional supplementation.1,3 At times intolerable mucositis also contributes to dose reduction, dose delay, and even termination of the planned radiation therapy, all of which may consequentially complicate the treatment of the underlying malignancy and cure. 1 Additionally, treatment aimed at ameliorating the complications of mucositis also increases the hospitalization time and the treatment cost.1,4
The currently available therapies consisting of dental care, use of anti-inflammatory agents, application of topical antiseptics, and antimicrobial agents are essentially palliative, and there is no widely accepted prophylactic or effective treatment for intolerable mucositis. 5 The use of biologicals like the recombinant human KGF-1 (palifermin) although efficacious is very expensive and unaffordable to most patients. 5 Herbal drugs offer an alternative to the synthetic compounds and are considered either nontoxic or less toxic than their synthetic counterparts. Natural products with free radical scavenging, antioxidant, antimicrobial, anti-inflammatory, wound healing, radioprotective, and immunostimulatory properties could be of possible use in the prevention of radiation mucositis and previous studies have shown that honey,2,6 Isatis indigotica, 7 Leptospermum scoparium, 8 Glycyrrhiza glabra, 9 and Kunzea ericoides, 8 possess beneficial effects.
The rhizome of Curcuma longa Linn, commonly known as turmeric and belonging to the ginger family, Zingaberaceae is an important spice and a medicinal agent in the various traditional and folk systems of medicine in India, and through different routes of administration, including topically, orally, and by inhalation.10-13 Turmeric finds mention in the various pharmacopeias as an antiseptic, analgesic, anti-inflammatory, and wound healing agent, and scientific studies have validated these ethnomedicinal properties. 11
Studies indicate that curcuminoids, which include mainly curcumin (diferuloyl methane), demethoxycurcumin, and bisdemethoxycurcmin, are the active components and that these phytochemicals like turmeric also possess antioxidant, anti-inflammatory, antimicrobial, anti-carcinogenic, antimutagenic, immunomodulatory, and wound healing effects.10-12 Scientific studies have also shown that turmeric/curcumin is effective against various pro-inflammatory diseases and to mediate the beneficial effects by modulating pro-inflammatory cytokines, apoptotic proteins, nuclear factor-κB (NF-κB), cyclooxygenase-2, 5-LOX, STAT3, C-reactive protein, and prostaglandin E(2).12,13
Turmeric/curcumin has been extensively investigated for its pharmacological effects on the oral and dental ailments and diseases. Experimental studies have shown that they prevent chemical-induced oral carcinogenesis in experimental animals14-18 and to induce apoptosis and inhibit cell proliferation of neoplastic cells of head and neck origin.19-23 Studies have also shown that they are effective in preventing the side effects of anticancer drugs24-27 and ionizing radiation.28-31 Turmeric is a frontline wound healing agent in the various traditional systems of medicine and experiments have also shown that turmeric/curcumin were effective in healing wound in different conditions,32-35 including that of wounds created in mice previously exposed to γ-radiation.36-39
With respect to clinical studies, turmeric is shown to be effective as a mouthwash and to possess antiplaque, anti-inflammatory, and antimicrobial properties. 40 Additionally, studies have also shown that the alcoholic extracts of turmeric, turmeric oil, and turmeric oleoresin decreased the number of micronucleated cells both in exfoliated oral mucosal cells and in circulating lymphocytes in patients suffering from oral submucous fibrosis 41 Recently, Chainani-Wu et al 42 have also observed that curcumin was effective in reducing the symptoms and signs of oral lichen planus in humans. With this background of turmeric being effective in various inflammatory conditions and a need for a nontoxic agent to prevent radiation-induced mucositis, the present investigation was performed to assess whether turmeric was effective in reducing the severity of radiation-induced mucositis in patients undergoing radiation therapy for head and neck cancers
Patients and Methods
Patient Population
The subjects were histopathologically confirmed patients of head and neck cancer (according to TNM classification) scheduled to receive radiotherapy or chemoradiotherapy. Patients with recurrence of cancer in the oral cavity were eligible. Exclusion criteria included patients younger than 18 years, patients who were pregnant, patients who had oral surgery within the previous 6 weeks, received chemotherapy or radiation treatment previously to the head and neck region, patients using high doses of nonsteroidal anti-inflammatory drugs, patients with poor oral hygiene and xerostomia, and patients with comorbid conditions (poorly controlled diabetes mellitus, hypertension, schizophrenia, bipolar disorders, severe depression). The study was approved by the hospital ethical committee in accordance with the percepts established by the Helsinki Declaration. Patients and their caregivers indicated their willingness to participate in the study after the details of the study and the treatment involved had been explained to them. The subjects provided written informed consent and were also informed that they had the right to withdraw from the study at any time during the course of the study.
Study Design
This was a single-center, randomized, investigator-blinded clinical trial at the Mangalore Institute of Oncology and was conducted between January 2012 and September 2012. It was estimated that a minimum sample size of 40 subjects per treatment group would enable detection of clinically significant differences between treatment groups at a α level of .05 with a power of .80. At the start of the study, all participants were verified to have no infected tooth, ulcers, or mucositis of the oral cavity. Of the eligible 93 patients, 84 satisfied the inclusion criteria and 80 agreed to participate in the study (Figure 1). The subjects were randomized using opaque envelopes to either povidone-iodine group (arm A) or turmeric (arm B). One of the authors oversaw the randomization. The sealed dark brown opaque envelopes (80 in total) used for randomization contained a card folded 4 times with the alphabet A or B (40 each) and were accordingly assorted to the respective arms.

Patient flow in the randomized controlled study.
All patients who participated in this study received external irradiation from a linear accelerator (Varian Medical systems, Unique 2012, Palo Alto, CA) at an average energy level of 6 MV. All planned fields were treated every day with no more than one fraction of 2 Gy per day, five times a week without any intended gaps for a planned target dose of 70 Gy (7 consecutive weeks). Whenever chemoirradiation was planned, carboplatin infusion (70 mg/m2/day intravenous) was administered on a weekly basis 3 hours before exposure to the first weekly radiation 43 (Figure 2).

Schedule of chemoradiotherapy and oral treatment.
Standard oral, dental, medical, and supportive care was provided to all subjects of both cohorts by a qualified dental physician. The patients were also instructed to clean their teeth with a soft toothbrush 4 times a day. If spontaneous gum bleeding occurred they were instructed to only rinse with the study solutions and avoid aggravating the injury with toothbrush. A feeding tube was placed only when it was needed. Oral cavity smears for microbiological testing were carried out only in patient with clinical suspicion of a local infection and antimicrobials (antibiotics and antifungal agents) were administered only after culture sensitivity test. Additionally, rinsing with analgesic solutions was prescribed only if required. All patients were given dietary counseling and were recommended dietary supplements (protein enriched powders) to meet the nutritional requirements of the body.
Study Mouthwashes
Patients randomized to arm A used povidone-iodine solution diluted 1:100 (betadine 1 mL and 100 mL water; active comparator condition), while those randomized to arm B used turmeric. The patients of both the arms were trained by one of the authors to swish the oral cavity and expectorate in the presence of an attentive primary caregiver with instruction to adhere to the procedure as specified. They were also requested to swish after food and to abstain from eating for 30 minutes after use of mouthwash. The patients of the arm A were instructed to swish their mouth with 10 mL of the povidone-iodine mouthwash, twice a day (morning and night), for a period of 6 weeks as described by Madan et al. 44
Turmeric solutions were suggested to be freshly prepared by dissolving the contents of standard turmeric powder (orangish yellow colored powder) available from the Himalaya Drug Company, Bangalore, India, in the form of capsules (batch no. L-AUS-133). The technical details of the turmeric powder are as follows (ash value 3.016% w/w, pH of 1% w/v solution in water 6.71, curcumin 2.42% w/w, lead 0.420 ppm, cadmium 0.030 ppm, arsenic 0.394 ppm, and mercury 0.283 ppm). In conventional Ayurvedic treatment, a paste of turmeric is made by grinding the dried roots and then boiled and cooled water and used for gargling to ameliorate ulcers of the mouth. In this study, we kept this principle in mind and adopted the procedure described above.
The caregivers were instructed to dissolve the contents of one turmeric capsule (400 mg) in approximately 80 mL of boiled and cooled water. The patients were instructed to swish their mouth with 10 mL of the turmeric solution for about 2 minutes and expectorate. The procedure was to be repeated 4 times at each time point and was to be performed for a total of 6 times in a day (1 hour prior to radiation, 1, 2, 4, and 6 hours after radiation, and once before going to bed) as indicated. During the course of the treatment, one of the investigators (CD) checked for the number of capsules being used on a weekly basis and repeatedly instructed the volunteers of both arms to adhere to the mouthwash instruction on every alternate day. The primary caregivers were also requested to monitor the volunteer’s diet, medication when prescribed, oral hygiene, and skin care practices.
Outcome Measures
Mucositis was assessed before the start of the radiation treatment (during the mould preparation) and at weekly intervals during radiation therapy in accordance to the RTOG (Radiation Therapy Oncology Group) guidelines. The scale grades from 0 to 4, indicating progressively more severe degrees of oral mucositis. 2 Scores 1 and 2 were grouped as “tolerable mucositis” and scores 3 and 4 were termed “intolerable mucositis.” 2 The observer recorded the grade of erythema or ulceration in upper and lower lips, right and left cheeks, right and left ventral and lateral tongue, floor of mouth, oropharynx, soft palate/fauces, and hard palate. A visiting orodental pathologist, unaware of the intervention received by the subjects, graded the mucosal reaction in the oral cavity using a battery-powered torchlight as described earlier. 2 The same observer also graded the mucositis in the inaccessible oropharnageal areas using the laryngoscope (Tele rigid telelaryngoscopy, model 8700CK, Karl Storz, Tuttlingen, Germany). As only one blinded researcher evaluated all the patients, calibration of assessors was not required and when differing grades of mucositis were present in the same oral cavity, the highest score was recorded as described earlier. 2
Statistical Analysis
Analysis of variance was used to compare the extent of severe mucositis score on a weekly basis, testing equality of proportion for the delay in incidence and the number of tolerable and intolerable mucositis, while the χ2 was used to compare the total incidence of worst-ever grades of ulceration, the number of treatment days lost due to intolerable mucositis and weight loss.
Results
Of the total 93 patients who reported to the Department of Radiation Oncology, Mangalore Institute of Oncology, Mangalore, India, during January 2012 to October 2012 for the treatment of head and neck malignancies, 80 patients, who fulfilled the inclusion/ exclusion criteria, participated in this trial and were randomly allocated into 1 of the 2 groups. The summary of the distribution of patients in the 2 groups based on age, sex, location of cancer, stage of cancer, treatment breaks, and difference in weight before and after the treatment is represented in Tables 1 and 2.
Patient and Tumor Characteristics.

Treatment Characteristics.
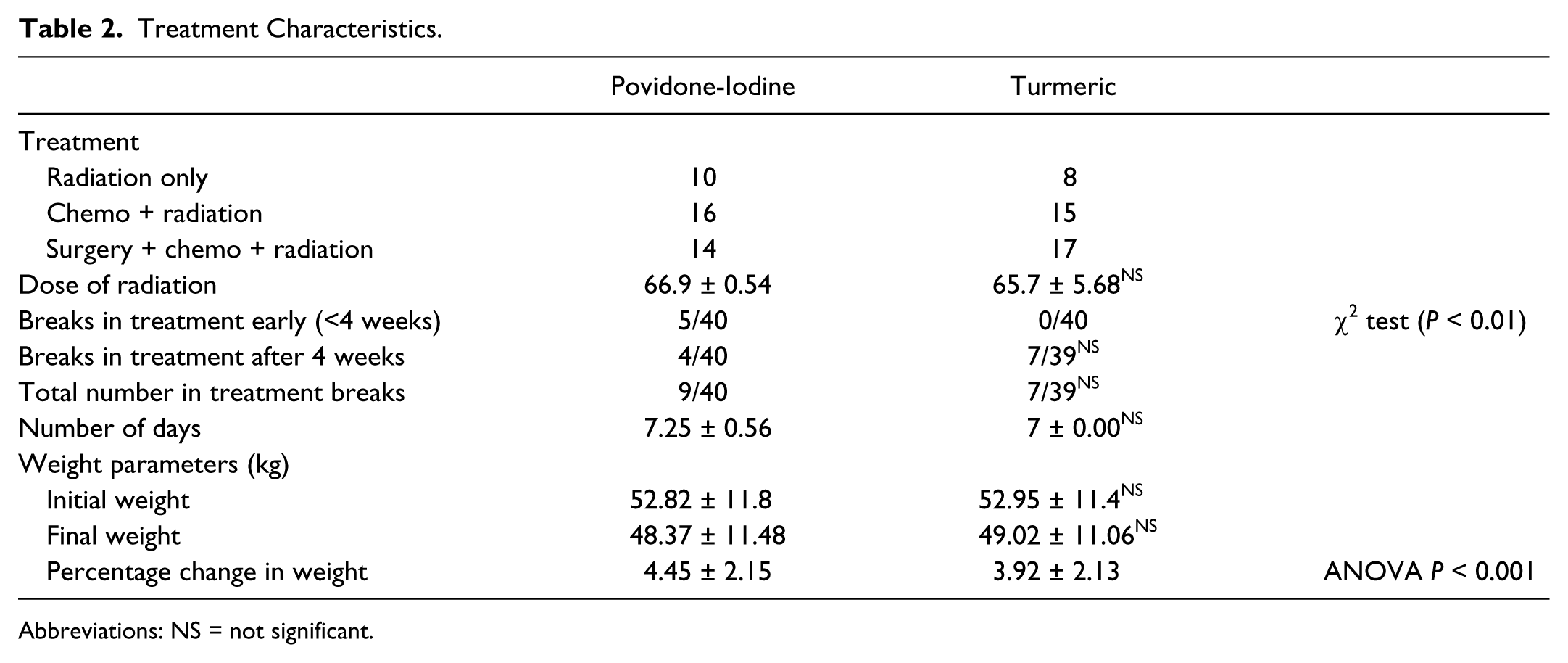
Abbreviations: NS = not significant.
The study population consisted of 16 women and 64 men, whose age ranged from 26 to 85 years (mean 55.96 ± 12.25 years) and patients in both arms reported good treatment compliance. One patient in the turmeric group opted out of the planned cancer treatment after 34 Gy of radiation because of personal reasons. The remaining 39 patients in the turmeric and 40 of the povidone-iodine arm persisted with the planned treatment and also complied with the instructions on gargling, diet and dental care.
Radiation exposure caused mucositis in both the cohorts and the mean mucositis score is represented on a weekly basis in Figure 3. The onset of tolerable and intolerable mucositis was delayed in the patients using turmeric and testing equality of proportion showed a statistically significant difference between the groups throughout the study (Figures 4 -6). Additionally, in the turmeric group, only 14 of 39 patients developed intolerable mucositis, while in the povidone-iodine group, 34 of the 40 patients developed intolerable mucositis and was significant (P < 0.0001; Table 2).
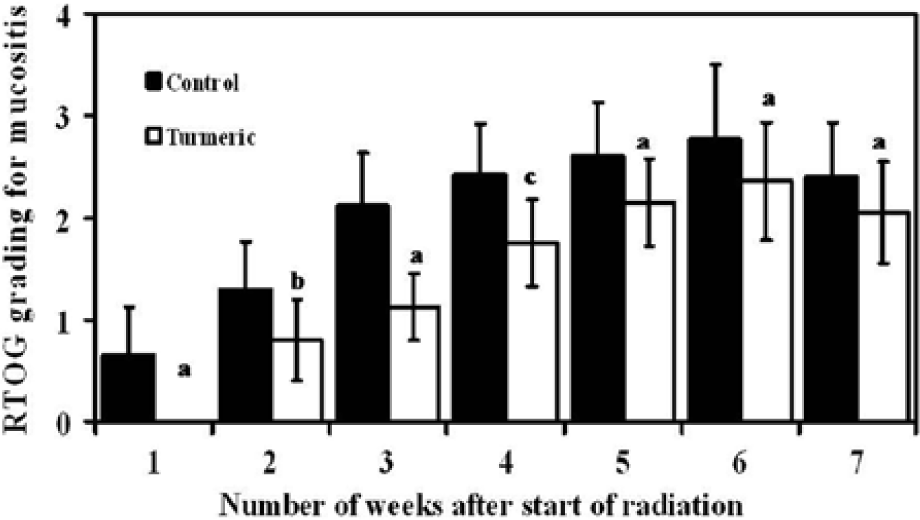
Graphical representation of the mucositis in the study groups through the radiation treatment period (analysis of variance: “a” indicates P < 0.0001; “b” indicates P < 0.003; “c” indicates P < 0.001).

Graphical representation of the incidence of mucositis through the treatment period. Squares = povidone-iodine; circles = turmeric (testing of equality: “a” indicates P < 0.0001; “b” indicates P < 0 .001).

Graphical representation of the incidence of tolerable mucositis through the treatment period Squares = povidone-iodine; circle = turmeric (testing of equality “a” indicates P < 0.0001; “b” indicates P < 0 .001; “c” indicates P < 0 .002).

Graphical representation of the incidence of intolerable mucositis through the treatment period. Squares = povidone-iodine; circle = turmeric (testing of equality “a” indicates P < 0.001; “b” indicates P < 0.0001; “c” indicates P < 0 .004; “d” indicates P < 0.003).
With respect to the number of treatment days lost, of the 39 patients in the turmeric arm, 7 (17.95%) experienced treatment interruption/delay caused by treatment reaction and all at the sixth or seventh week of radiation. The corresponding number for patients in the povidone-iodine arm was 9 (24%) of whom 5 needed treatment break at early stage (before 40 Gy; 4 weeks) and 4 toward the fifth to seventh week of the treatment after completing 40 Gy (Figure 6). The number of treatment days lost were 7.25 ± 0.56 and 7 ± 0.00 days, respectively, for povidone-iodine and turmeric group and was statistically not significant (Table 2). Additionally, it was also observed that when compared with the povidone-iodine (4.45 ± 2.15) group, the weight loss was less in the turmeric cohorts (3.92 ± 2.13) and was statistically significant (P < 0.001).
Discussion
Extensive research in the recent past has unequivocally shown that the kitchen spice turmeric and its principle compound curcumin possess myriad medicinal benefits and is of immense use especially in ameliorating inflammatory-mediated diseases and ailments of the gastrointestinal tract.10-13 In the present study, exposure to ionizing radiation caused mucositis in both povidone-iodine and turmeric cohorts (Figure 2). However, in the participants using turmeric, the clinical appearance of mucositis was delayed and the intolerable mucositis was reduced, indicating turmeric to be effective in preventing mucositis.
Our results are similar to that of previous studies with honey, where various investigators have observed it to be effective in preventing against radiation-induced mucositis.2,6,45-49 However, the apprehension that honey would enhance the radiation-related caries in cancer patients topically applying them during the course of the radiation50,51 is a major concern as this would enhance dental caries and compromise the quality of life of the cancer survivors. In contrast, when compared with honey, turmeric may not have long-term adjunct effects as studies have shown it to be also beneficial in the treatment of various periodontal diseases.40,52-54 Literature studies also show that turmeric possesses selective antineoplastic activity on neoplastic cells, chemopreventive effects, and antimetastatic activities,14-23 all of which can be beneficial in the prevention of recurrence and distant spread of the cancer.
In cancer treatment, unplanned treatment interruptions and decrease in the planned treatment dose reduce the treatment efficacy, control of locoregional growth, and affect survival. 55 In this study, it was observed that when compared with the povidone-iodine arm, the cohort receiving turmeric had reduced treatment breaks and toward the end of the treatment schedule (5 weeks after the start of the treatment; Figure 3).The patients in the turmeric group were able to maintain better food intake because of reduced mucositis to the effect that the lower weight loss might have been due to better food consumption owing to reduced mucositis, although this was not measured specifically. Previous studies have shown that curcumin possesses anti-inflammatory56,57 and antinociceptive effects58,59 in relevant animal models of study, and it is quite possible that by reducing the inflammation and pain, turmeric might have contributed toward better dietary practice in these cohorts.
To the knowledge of the investigators, this is perhaps the first report to show the effectiveness of turmeric in preventing radiation-induced mucositis. However, literature does indicate that high dose of curcuminoids (6000 mg/d in 3 divided doses) was efficacious in controlling signs and symptoms of oral lichen planus and to also reduce erythema, ulceration, and total modified oral mucositis index scores. 42 Additionally, preclinical studies with laboratory rats have also shown that a formulation containing curcumin, α-tocopherol, and sunflower oil was effective in preventing radiation-induced oral mucositis. 60 Together, these observations clearly indicate the usefulness of turmeric in preventing mucositis and substantiate our observations.
The process of mucositis is complex and includes initiation, upregulation, and generation of messenger signals, signaling and amplification, ulceration, and healing stage. 1 At a cellular level, exposure to ionizing radiation causes generation of free radicals (reactive oxygen species and reactive nitrogen species), 1 DNA strand breaks and to activate transcription factors (NF-κB). 1 Additionally, the immune cells also produce pro-inflammatory cytokines (tumor necrosis factor-α, interleukin-1 [IL-1], IL-6), which exacerbate the tissue injury and cell death.1,61,62 Numerous studies in the past with various experimental models have equivocally shown that turmeric/curcumin possess free radical scavenging effects on both reactive oxygen species and reactive nitrogen species, to reduce the levels of pro-inflammatory cytokines and NF-κB11-13 and triggering of these mechanisms could have contributed toward the observed protection in the study.
In addition to the cellular inflammatory effects, the denuded epithelium may also provide access to the oral microbial flora and this may contribute to the underlying pathogenesis and exacerbate the condition. 63 Turmeric/curcumin has also been reported to possess antimicrobial effects, including against the clinically relevant methicillin-resistant Staphylococcus aureus strains 64 With regard to the bacteria involved in the process of oral mucositis, in vitro studies with Moraxella catarrhali, a facultative upper respiratory tract pathogen have shown that curcumin possess bactericidal effects to inhibit bacterial adherence and invasion to Detroit 562 (pharyngeal cells) and to reduce Mcat-induced pro-inflammatory activation by suppressing release of pro-inflammatory cytokine IL-8. 65 Pre-incubation of Detroit cells with 200 µM curcumin for 5 to 60 minutes resulted in complete suppression of the release of tumor necrosis factor-α, IL-6, IL-8, monocyte chemoattractant protein 1, granulocyte macrophage-colony stimulating factor, and vascular endothelial growth factor. 65 Additionally, the investigators have also observed that repetitive exposure to curcumin caused recurring suppression of cytokine/chemokine expression. 65
Turmeric has been used as a wound healing agent for centuries32-35 and animal studies have shown that when compared with untreated controls, the application of curcumin enhances faster wound closure of punch wounds in curcumin-treated animals. 37 Histopathological observations indicate that in the cohorts where turmeric was applied, increased levels of reepithelialization of epidermis; migration of myofibroblasts, fibroblasts, and macrophages to the wound bed; promotion of neovascularization and greater deposition of collagen was pronounced and that this effect was mediated by increased levels of transforming growth factor-β1. 37 Additionally, studies have also shown that turmeric and its principal compound curcumin possess anti-inflammatory 66 effects, promote reepithelialization, 67 and enhance healing of wounds created in skin exposed to radiation.36-39 In lieu of all these observations it can be postulated that the beneficial effects of turmeric in preventing radiation-induced mucositis can be best explained by its anti-inflammatory, antioxidant, antimicrobial, modulating cytokines, and by enhancing wound healing process.
Summary and Conclusion
The notable observation of this study is that turmeric was effective in preventing/reducing radiation-induced mucositis and that the effect was better than the standard povidone-iodine used as an active comparator. In our study, the patients in arm A rinsed only twice per day with povidone-iodine solution, while the patients in arm B swished with turmeric solution 6 times a day. This schedule of 6 times a day for the turmeric cohorts was adopted on recommendation of senior Ayurvedic physicians, who recommend similar protocol of treatment for treating oral ulcers while that for the povidone-iodine described by Madan et al 44 is a widely used protocol locally in Mangalore. It is quite possible that this increase in swish in arm B might have also contributed to the observed protection and needs to be validated with different number of swishes with turmeric solution. The use of active placebo (water only) was avoided on ethical grounds and to avoid the risk of developing any mucositis and associated oral complications. The second important aspect that merits further study is that the study arm assigned to turmeric intervention was not blinded to the patients. Turmeric has distinctive organoleptic properties and has been used regularly as a culinary and therapeutic agent for centuries in Asia. It is quite possible that the psychological influence of turmeric’s beneficial effects may have also had played a role in the therapeutic effects observed in the turmeric cohorts and needs to be validated in future studies with exactly matching nontoxic control and including the pain scale and quality of life assessment through questioners/interviews. As far as the authors are aware, only metanil yellow resembles turmeric powder. However, the use of this chemical was not considered because of its toxicity profile. Turmeric has an excellent safety profile and wide acceptability. Within the authors’ admitted limitations, it can be concluded that turmeric has a significant effect in delaying and reducing radiation-induced mucositis. As a conclusion, our study shows for the first time that regular turmeric swish is effective in preventing the radiation-induced acute mucosal inflammation and could be of immense use in clinics when the existing lacunae are bridged.
Footnotes
Acknowledgements
The authors are extremely grateful to Dr Prahlad Patki and Dr Rafique of Himalaya Drug Company of Bangalore for providing the necessary information on turmeric.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.