
Abstract
Introduction. Listening to music can positively benefit neurophysiological and emotional responses as well as promote relaxation, which may be especially beneficial for cancer patients undergoing painful and anxiety inducing treatments. The purpose of the present study was to conduct an evidenced-based systematic review and meta-analysis of randomized controlled trials of music interventions to reduce anxiety for adult cancer patients undergoing medical treatment. Methods. A systematic literature search was conducted and data were abstracted from all eligible studies. Studies were included if they tested a music therapy randomized controlled trial in adult cancer patients (in active treatment), assessed anxiety postintervention using a validated measure, were published in English (or were translatable), and accessible in full text. Studies were qualitatively reviewed by the first author and 2 raters independently assessed each study using the PEDro scale. Standardized mean differences between experimental and control groups were calculated for studies meeting a specified methodological rigor score with accessible means and standard deviations postintervention. Heterogeneity and publication bias were explored. Results. Thirteen randomized controlled trials were included with 4 eligible for meta-analysis. Studies varied in intervention methodology and utilization of anxiety measures. Almost all studies reported either a significant difference in anxiety between groups postintervention or a significant decrease in anxiety over time in the music intervention group. Meta-analytic results of 4 studies (4/13) demonstrated that differences in anxiety between experimental and control groups were not significant in the main analysis or subgroup analysis. Studies demonstrated heterogeneity in anxiety results. Publication bias was not evident. Conclusion. The meta-analytic results failed to demonstrate a positive effect on anxiety among adult cancer patients in treatment but may in part be attributed to the small sample size. These findings are in contrast to a prior meta-analysis that analyzed all studies regardless of methodological rigor. More research is needed to ascertain the most optimal intervention methodology and which cancer populations or treatment modalities are appropriate for such an intervention.
Introduction
The American Cancer Society 1 estimated that there will be more than 1.6 million cancer cases diagnosed in the United States in 2012. Although cancer treatment has advanced over the years and resulted in increased survival, the treatment phase can be arduous and in some cases, life threatening, depending on cancer diagnosis and treatment modality. 2 Consequently, patients may experience psychological distress. In fact, it has been reported that cancer patient’s risk of psychiatric distress is almost twice as much of the general population’s 3 with up to 30% of patients experiencing anxiety. 4
The American Psychological Association 5 defines anxiety as “an emotion characterized by feelings of tension, worried thoughts and physical changes like increased blood pressure.” Anxiety can have significant consequences for the cancer patient. For example, research has demonstrated that anxiety is associated with comorbid depression as well as impaired health-related quality of life in cancer patients. 6 Moreover, anxiety has been associated with exacerbation of symptoms and is influential in patient treatment decision making and response to treatment.7,8 Given the potential for significant ramifications of anxiety in cancer patients, intervention is critical.
One approach to decreasing anxiety that has been used and recommended for cancer patients is music therapy. 9 Music therapy has been defined as “the clinical and evidence-based use of music interventions to accomplish individualized goals within a therapeutic relationship . . .” 10 Listening to music can positively affect neurophysiological and emotional responses, facilitating relaxation in the patient. 11 Music interventions are a burgeoning area of research for cancer patients and although the benefits are delineated in the literature, studies have also demonstrated no benefit. Differences in findings may be attributed to heterogeneity in samples, intervention methodology, inconsistent outcome measures, and flawed research designs. When such problems arise, a systematic review and meta-analysis may be useful in assessing and reporting on the current state of the literature.
Bradt et al 12 conducted a Cochrane meta-analysis on music interventions for improving psychological and physical outcomes in cancer patients. The authors concluded that music interventions may have a beneficial effect on cancer patients. However, Bradt et al 12 did not restrict their review to randomized controlled trials (RCTs). Although a subgroup analysis of RCTs was conducted, this analysis included all studies irrespective of methodological quality. Moreover, pediatric studies were not excluded from the meta-analysis. Consequently, inclusion of such heterogeneous and ambiguous data reduces the utility and impact of this previous meta-analysis and may mislead investigations in this area. Therefore, the present study aims to clarify the effect of music intervention RCTs on anxiety for adult cancer patients using a more rigorous approach. Only studies meeting recommended methodological rigor were included in the meta-analysis portion of this study.
Methods
Search Strategy
The first author conducted the literature search using PubMed, PsycINFO, Web of Science, CINAHL, and WorldCat Dissertations databases. A comprehensive list of keywords were used, including “music,” “music therapy,” “music intervention,” “cancer,” “neoplasm,” and “malignancy.” For databases allowing a more advanced search, articles were restricted to RCTs. The following inclusion/exclusion criteria were used to select articles: (a) used an RCT design, (b) tested a music intervention, (c) used an adult population (defined as a minimum age of 18 years) with a current cancer diagnosis, (d) assessed a measurable anxiety outcome, (e) used validated measures, (f) published in English or capable of being translated, and (g) accessible in full text. Validated measures consisted of those that have undergone psychometric evaluation with demonstrated sensitivity and specificity.
Data Extraction
The first author systematically abstracted data from all articles reviewed in full text using an evidence table. Abstracted data included the authors and year in which the study was published, country in which the study was conducted, characteristics of the sample (eg, size, gender, age, cancer diagnosis, and treatment type), the intervention and control group’s methodology, relevant anxiety measures, means and standard deviations postintervention for the experimental and control groups, and the most important findings. When means and standard deviations were not reported, authors were contacted and the data were requested.
Quality Assessment
Two independent reviewers, blinded to the study authors, authors’ affiliations, and journal, used the PEDro scale 13 to assess the quality of the final set of eligible studies. The PEDro scale was used as it has demonstrated sufficient reliability for assessing RCTs. 13 In this tool, 10 of the 11 items (ie, criteria 2-11) are awarded 1 point if satisfied and a total summation of the items is used to calculate a quality score as high or low. High scores are classified as achieving a minimum of 6 points whereas anything less would be classified as a low score. 13 However, using a modified cutoff of a 5 for inclusion in a meta-analysis has been recommended as it is difficult to blind subjects or therapists within a RCT. 13 Therefore, the present study used a modified cutoff score of 5 (ie, ≥5 = “high quality”) with the rationale that blinding subjects or therapists to a music intervention is almost impossible. In the present study, we included all studies in the systematic review and only high-quality studies in the meta-analysis.
The independent raters were required to use a standardized rating sheet to record study details for qualitative grading. A fixed marginal kappa analysis 14 was conducted and revealed 91% agreement in coding across studies. Kappa values of .75 or higher reflect excellent agreement between raters. 15 Overall rater agreement was strong across categories of the PEDro scale ranging from 82% to 100% agreement. The criterion that had the greatest discrepancy between the raters pertained to whether the data were analyzed using an intention to treat analysis, which was often not explicitly stated by authors (ie, item number 9 on the PEDro scale). This criterion resulted in an agreement of 64%. Where discrepancies occurred, they were discussed and resolved by consensus.
Criteria for Meta-Analysis
Studies from the total sample are eligible for the meta-analysis if they (a) assessed anxiety using a theoretically similar measure and (b) have accessible means and standard deviations.
Statistical Analysis
Comprehensive Meta-Analysis software 16 was used to perform the meta-analysis. Given that the group of eligible studies for the meta-analysis used some variability in tools depicting the same outcome, standardized mean differences with 95% confidence intervals were calculated for each study included in the meta-analysis. For studies testing differences among 3 groups, data for the nonmusic intervention experimental group were excluded. Summary effect sizes for the difference between intervention and control groups and corresponding standard errors were also pooled. Effect sizes of 0.20, 0.50, and 0.80 were considered small, medium, and large, respectively. 17 Heterogeneity was explored using Cochran’s Q (P < .05), I2, and τ2. Because of the homogeneity among studies, a random effects analysis was used. Publication bias was also explored using a funnel plot, Begg and Mazumbar’s rank correlation test, Duval and Tweedie’s trim and fill method, and Orwin’s classic fail-safe N.
Results
Initial queries yielded a total of 606 studies in which the titles were screened. A total of 566 of these studies were excluded for various reasons including duplicates of the same study (n = 86), failure to focus on adult cancer patients (n = 302), lack of randomization and/or a control group (n = 135), or otherwise irrelevant to music interventions (n = 43). Following this, abstracts were reviewed for 40 studies of which 25 were deemed ineligible for various reasons, including failure to focus exclusively on adult cancer patients (n = 5), lack of randomization and/or a control group (n = 14), and lack of a validated anxiety tool (n = 6). After reviewing the full text of the resulting 15 studies, 2 studies were further eliminated because of failure to focus exclusively on cancer patients. In total, 13 studies met all eligibility criteria and are included in the present study. Of these studies, 6 assessed the same construct using theoretically similar measures with accessible means and standard deviations,18-23 one of which did not meet the minimum cutoff score for the PEDro scale. 22 However, one study 18 was excluded because data were presented as change scores rather than raw data; therefore, 4 studies were included in the meta-analysis.19-21, 23 See Figure 1 for a flowchart representing the study selection process.

Flowchart for study selection process.
Quality Ratings
The 13 studies averaged a quality rating score of a 5.31, with scores ranging from 3 24 to 9. 20 All studies achieved random assignment (item 2) since the present study only included RCTs and all studies provided between-group statistics (item 10). Ferrer 25 and Harper 24 are the only studies that did not specify eligibility criteria (item 1) or report similar groups at baseline (item 4). Cassileth et al 18 and Hanser et al 20 are the only studies that reported concealed allocation (item 3) and blinding subjects (item 5). Only one study 20 reported blinding the therapist (item 6) or assessor (item 7). Seven studies18-20,23,25-27 reported having one key outcome from greater than 85% of subjects allocated to groups (item 8). Eight studies18-21,23,26-28 reported whether or not subjects received the treatment as allocated or used an intention to treat analysis (item 9). See Table 1 for PEDro quality ratings.
PEDro Quality Assessment Ratings.

Studies included in the meta-analysis.
Study Characteristics
Studies were conducted between 2001 and 2011 (see Table 2). The majority of the studies (n = 10) were conducted in the United States,18-21,23-25,27-29 although one was conducted in Italy, 26 one in Taiwan, 22 and one in China. 30 Sample sizes ranged from 20 to 98 with a total of 709 cancer patients across all studies. Three studies focused on females only20,26,29 whereas the remaining studies included both females and males. Mean age of participants ranged across studies from 51 to 63 years. Three studies focused exclusively on breast cancer patients,20,26,29 one on leukemia patients, 28 and one did not report cancer diagnosis. 25 The remaining studies included patients with various cancer diagnoses. Cancer stage was variable across studies and in some cases, within studies. Similarly, cancer treatment ranged across studies and in some cases, within studies. However, 7 studies reported that patients received chemotherapy, which was sometimes in combination with other treatment20-22,25-28 and 5 studies reported that patients received radiation treatment, which was also sometimes in combination with other treatment.18,20,23,27,30 See Table 2 for a complete list of study demographics.
Study Demographics.

Studies included in the meta-analysis.
Nature of Interventions
The content, delivery, dose, and duration of the interventions varied (see Table 3). The majority of the interventions were individualized to the patient’s musical preferences and/or clinical needs by allowing them to choose from a specific selection and/or providing music appropriate for the patient’s emotional state. In 4 of the interventions18,20,27,28 a certified or trained music therapist met with participants to facilitate or instruct participants on the exercises. One study 25 did not specify who delivered the intervention and the remaining studies were facilitated by the patient simply by listening to music provided to them, or through an instructed prerecorded tape/compact disc.
Study Characteristics and Relevant Findings.

Abbreviations: STAI, State-Trait Anxiety Inventory; POMS-SF, Profile of Mood States–Short Form; HAD, Hospital Anxiety and Depression Scale; VAS, Visual Analogue Scale; BAI, Beck Anxiety Inventory; Zung SAS, Zung Self-Rating Anxiety Scale.
Studies included in the meta-analysis.
Seven of the interventions were delivered solely during medical oncology treatment.21-25,29,30 Similarly, in the study by Danhauer et al, 19 patients received the intervention during treatment but also had the option to listen to music while waiting for treatment. Likewise, in the study by Hanser et al, 20 patients received the intervention during treatment or for those not receiving treatment, in a consultation room. Remaining studies specified that the intervention was delivered solely when patients were waiting for treatment, 26 during their hospital stay,18,28 or over the course of treatment. 27
Length of intervention sessions varied between studies and sometimes within studies. Danhauer et al 19 reported that intervention sessions lasted anywhere from 5 to 40 minutes whereas the intervention in the study by Binns-Turner 29 lasted 4 hours. Clark et al 27 and Kwekkeboom 21 did not indicate the length of their intervention sessions, although Clark et al 27 did indicate that patients were provided with a 90-minute musical tape.
In addition to variability in length of intervention sessions, there is also variability in number of intervention sessions. Eight studies tested interventions that were delivered on one occasion19,21,22,24-26,29,30 Burns et al 28 indicated that patients received up to 8 sessions whereas Cassileth et al 18 indicated that patients received a median of 5 sessions. Clark et al 27 specified that patients received an intervention anytime over the course of treatment and similarly, Smith et al 23 specified that patients received intervention sessions over the course of daily treatment sessions for a minimum of 5 weeks.
Three of the interventions delivered live music.18,20,25 Burns et al 28 did not specify how the music was delivered and the remaining 9 studies delivered music through headphones or earphones. Some intervention methodologies included more than simply listening to music. For example, the intervention in the study by Burns et al 28 also included music imagery and relaxation. Similarly, the intervention in the study by Clark et al 27 included progressive muscle relaxation, imagery, and positive self-talk. The intervention in Ferrer’s study 25 included encouraging patients to request songs and sing along while Hanser et al’s study 20 included improvisation, song writing, and playing percussion instruments. When studies included more than one intervention conditions that were not all music related, details for the nonmusic conditions are not included in the present review.21,22
Anxiety Measures
Several different scales were used to assess anxiety (see Table 3). Six studies used the English version of the State-Trait Anxiety Inventory (STAI),19,21,23,24,28,29 whereas one used the Italian version 26 and one used the Chinese version. 22 The state anxiety subscale results were used for the present study’s meta-analysis. The remaining studies included the Profile of Mood States anxiety subscale, 18 the Hospital Anxiety Depression Scale–Anxiety subscale,20,27 the Zung Self-Rating Anxiety Scale, 30 the Beck Anxiety Inventory, 24 and an anxiety Visual Analogue Scale. 25 The 4 studies included in the meta-analysis used the STAI19,21,23 and the Hospital Anxiety Depression Scale. 20
Anxiety Findings
The majority of studies (85%) reported significantly less anxiety in the music intervention group compared with the control group postintervention using means or change scores18,24,25,27,29,30 and/or a significant decrease in anxiety from pre- to postintervention in the music intervention group.19,22,23,26,28 Two studies (15%), however, did not report these findings.20,21 In fact, both of these studies reported contrary findings where the intervention group reported greater anxiety. Kwekkeboom 21 reported that this finding was because of methodological and procedural difficulties listening to the music via headphones during treatment, whereas Hanser et al 20 did not offer a potential explanation for the finding (see Table 3).
Meta-Analysis Results
The pooled analyzed results revealed no significant difference in anxiety between the music intervention and control groups (P = .99) with a pooled standardized mean difference of −0.003 (−0.51, 0.52; see Figure 2). A test for heterogeneity demonstrated a significant difference across studies (P = .03, Q = 9.24 (3), I 2 = 67.53%, T 2 = 0.19). A funnel plot was retrieved using the Begg and Mazumdar rank correlation tests. However, because of insignificant results (Kendall’s τ = 0, P = 1.0), we cannot definitively exclude the possibility of publication bias. Although it is noteworthy to mention that publication bias was not evident in the funnel plot (see Figure 3). Moreover, using Duval and Tweedie’s trim and fill method, no studies were trimmed to the right or left of the mean strongly suggestive of the absence of publication bias.
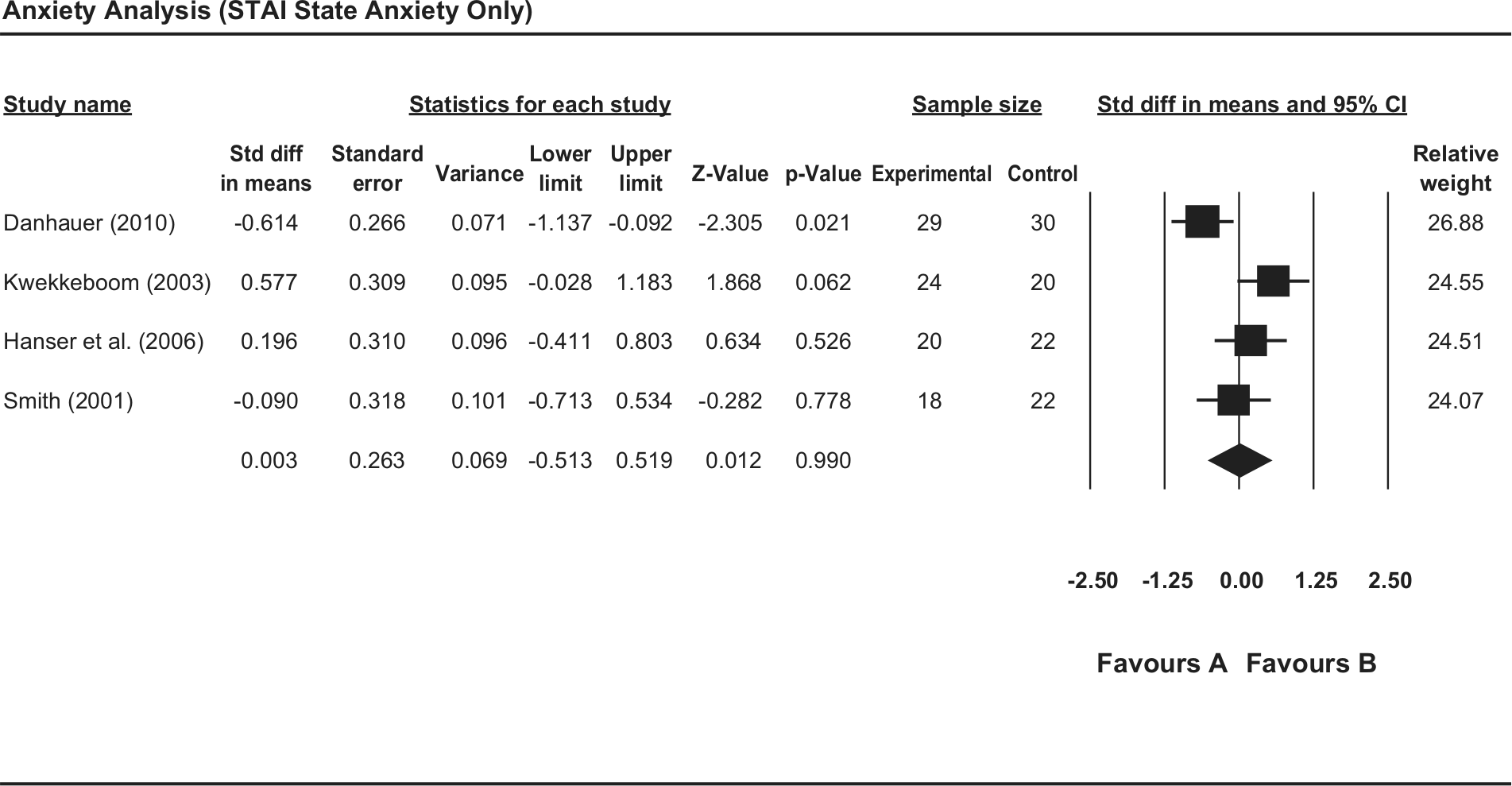
Forest plot for total sample.
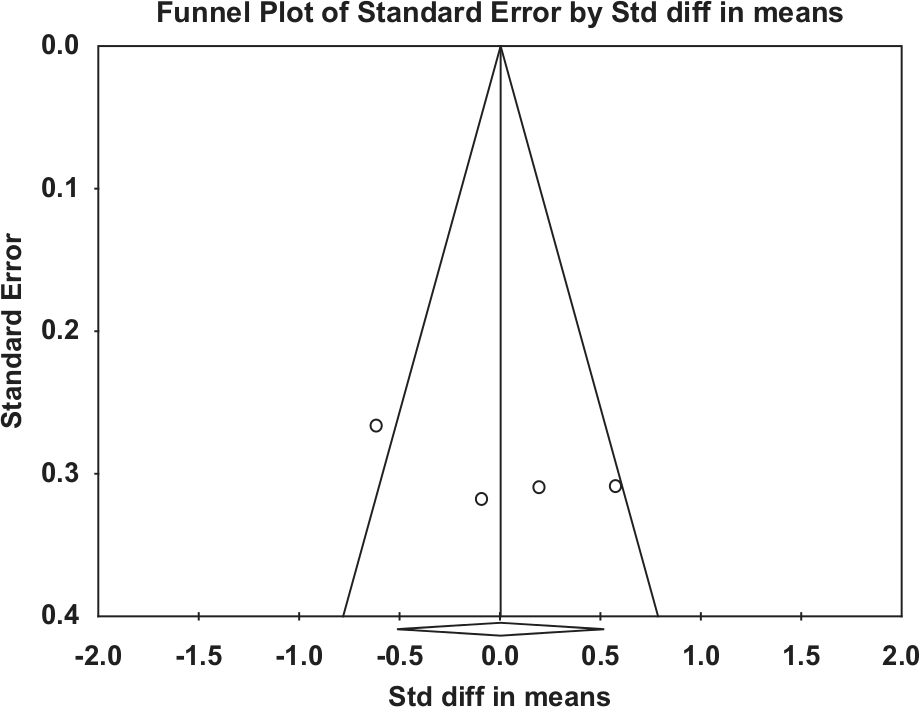
Funnel plot for total sample.
Subgroup Analysis
A separate analysis was conducted for the 3 homogenous studies, all of which used the STAI-state anxiety subscale.19,21,23 The pooled analyzed results again revealed no significant difference in anxiety between music intervention and control groups (P = .88) with a pooled standardized mean difference of −0.06 (−0.75, 0.64; see Figure 4). A test for heterogeneity again demonstrated a significant difference across studies (P = .01, Q = 8.53 (2), I2 = 76.56, T2 = 0.29). The funnel plot using the Begg and Mazumdar rank correlation test yielded insignificant results (Kendall’s τ = 0.33, P = .60) failing to definitively exclude the possibility of publication bias. Publication bias was not demonstrated in the funnel plot (see Figure 5), and Duval and Tweedie’s trim and fill method indicated no significant bias toward the publication of these studies.
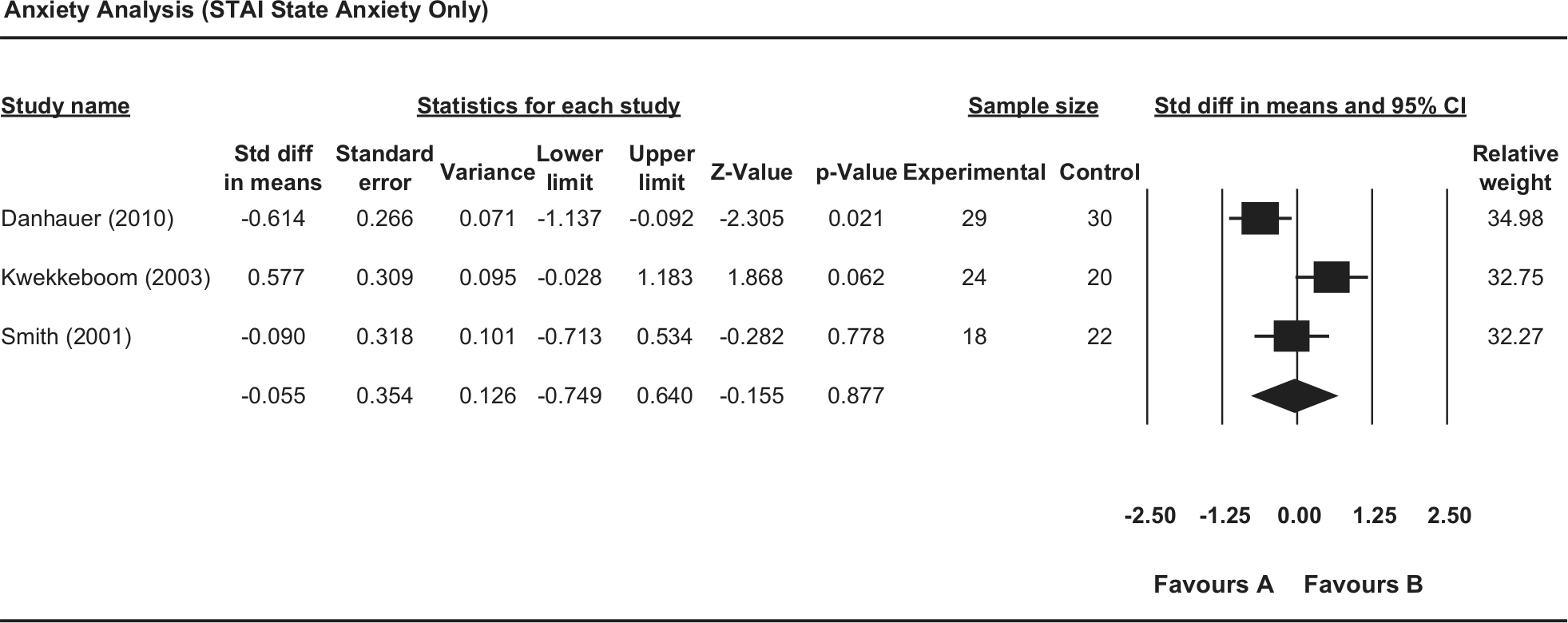
Forest plot for subgroup analysis.
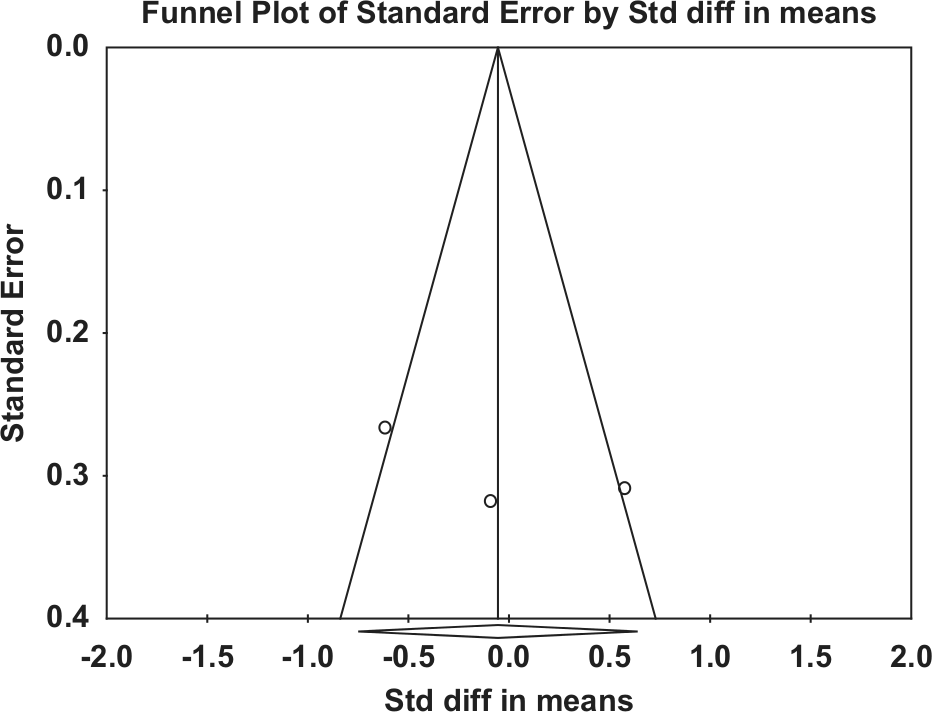
Funnel plot for subgroup analysis.
Discussion
This is the first meta-analysis and systematic review that has complied with recommended methodological rigor using the PEDro scale and evaluated the impact of music RCTs on anxiety in adult cancer patients. Although our review of 13 RCTs suggests a positive benefit of music interventions on anxiety, the meta-analysis results indicate that music interventions may not have a true effect on the mitigation of anxiety among adult cancer patients. Our meta-analytic results fail to corroborate a prior meta-analysis and review that reported a beneficial effect of music interventions on anxiety among cancer patients. 12 The difference in findings between these meta and analytic investigations may be attributed to the rigorous screening and inclusion criteria in our study versus the study by Bradt et al. 12 For example, Bradt et al 12 included studies regardless of methodological rigor whereas the present study only included studies meeting a cutoff score of 5 using the PEDro scale. Moreover, our study focused exclusively on adult cancer patients whereas that by Bradt et al 12 included pediatric studies as well.
This present investigation has several strengths. First, only RCTs were included both in the systematic review and meta-analysis. Second, only studies meeting methodological rigor recommendations using the PEDro scale were included in the meta-analysis portion of this study. Third, this study focused exclusively on adult cancer patients, thus eliminating the potential for age as a confounding variable to outcomes Finally, although the meta-analytic results do not suggest a benefit of anxiety reduction from music intervention, the review of all studies suggests that music interventions may still offer clinical utility as a nonpharmacological agent to mitigate anxiety in adult cancer patients.
Although the current investigation includes only a small number of studies, this remains representative of the current clinical application of music intervention in this field. Moreover, this highlights the need for more music-based investigations using approaches with stronger methodological rigor. Additionally, many of the current studies of music intervention include variable study samples and use a range of divergent intervention methodologies as demonstrated in the heterogeneity of studies reviewed in this meta-analysis. For example, cancer diagnosis, oncology treatment, and music intervention approach all varied across studies. Consequently, because of this heterogeneity, it is difficult to generalize the results of the present analysis to delineate the optimal type of intervention for the adult cancer populations.
Specifically, more conceptual and practical development of this field is needed. Inconsistencies in intervention methodology across studies underscore the need for identification of optimal intervention components to significantly reduce anxiety among cancer patients. Future studies should explore differences in application such as whether the music is delivered live or is prerecorded and whether some types of music are more beneficial than others. In addition, a common theme throughout many of the studies was the lack of a theoretical framework to provide a rationale for the delivery of the intervention, including choice in music. Such a rationale would improve scientific rigor and increase the probability of clinical translation. 31 Future studies should attempt to standardize approaches and obtain more homogenous populations regarding cancer diagnosis and medical treatment modality in order to achieve translational results.
Conclusion
This meta-analysis did not identify a positive effect for music intervention on reducing anxiety in the adult cancer population, although the majority of studies reported a positive benefit. Consequently, the efficacy of music interventions in decreasing anxiety in adult cancer patients remains unclear. However, this systematic review and meta-analysis augments the current knowledge in the field while highlighting the limitations. Future research should strengthen the support for music interventions by standardizing the application of the music agent. Advancement of this complementary intervention is necessary prior to further efficacy evaluations so that resources are used efficiently and patients’ participation is meaningful.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.