
Abstract
Hypothesis. Naturopathic treatment will benefit patients with hepatocellular carcinoma (HCC). Study design. Retrospective analysis of case series of HCC patients treated with naturopathic agents. Methods. HCC was diagnosed by dynamic computed tomography (CT) imaging and α-fetoprotein (AFP) or PIVKA II, or by histology. Tumor staging was determined by CT. A modified Childs–Pugh scoring was used to assess liver disease. Patients were treated with orally administered combinations of 12 naturopathic agents. Patients were monitored clinically and by CT tumor imaging, serial tumor markers, and liver function tests. Results. Patient characteristics: 101 patients with HCC (67 men and 34 women, age 67.2 ± 8.8 years) were treated for a median of 13.4 months (range 0.8-100.8). Of these 84% had cirrhosis, 63% had hepatitis C virus, 18% had hepatitis B virus, 1% had both, and 9% had metastatic disease. Median modified Childs–Pugh score was 6 (range 3-13). Barcelona Clinic Liver Cancer tumor stages of 0, A, B, C, and D were found in 36%, 25%, 20%, 14%, and 6%, respectively. Median AFP was 40 (range 0-311,000). Median PIVKA II was 59 (0–378,000). Previous treatment was included none (27%), resection with relapse (20%), transarterial chemoembolization (50%), radiofrequency ablation (28%), percutaneous ethanol injection therapy (15%), chemotherapy (14%). Outcomes: Initial treatment was with 2.6 ± 0.8 agents (range 2-4). Overall, patients were treated with 3.7 ± 1.2 agents (range 2-7). There was a significant correlation between number of agents administered and survival (P < .0001). Patients treated with ≥4 agents survived significantly longer than patients treated with ≤3 agents (40.2 vs 6.4 months, P < .0001). This difference could not be attributed to statistically significant differences in severity of liver disease or tumor stage, delay in treatment, previous treatment, concurrent nondrug treatment, or censoring effects. The greatest effect was seen in patients treated with at least 4 agents that included Cordyceps sinensis. This prolonged survival was without toxic side effects and appeared to potentiate the survival benefit of conventional therapy. Conclusion. Treatment of HCC with a regimen of ≥4 agents prepared from natural products was associated with prolonged survival in a substantial portion of patients. The data provide level II evidence for the efficacy of naturopathic therapy in HCC.
Keywords
Introduction
Hepatocellular carcinoma (HCC) is the third most frequent cause of cancer death both globally and in Japan, where the age-adjusted death rate from HCC is approximately 23 per 100 000 per year. 1 In recent decades, approximately three fourths of HCC in Japan has been associated with chronic infection with hepatitis C virus (HCV). 2 During the past decade, the prevalence of HCV-associated HCC has begun to decline, perhaps associated with preventive measures and with interferon treatment of existing infection. 3 On the other hand, the incidence of HCC not associated with HCV or hepatitis B virus (HBV) infection, and of HCC in women, is increasing. 4
Surgical resection, liver transplantation, and radiofrequency ablation (RFA) are considered potentially curative treatments for HCC. 5 However, only a minority of patients are eligible for surgery or transplantation at the time of diagnosis, and the rate of eventual relapse with all of these therapies is high.2,5,6 Other treatments, including percutaneous ethanol injection therapy (PEIT), transarterial chemoembolization (TACE), chemotherapy, and most recently, therapy with kinase inhibitors, are not curative but can prolong survival.5,7 However, particularly for patients with advanced liver disease and inoperable tumors, the prognosis for long-term survival with HCC is very poor.
The use of naturally occurring botanical and microbial products, which is one of the principles of naturopathic medicine, is another category of treatment to be considered in patients with end stage malignancy for which there is no curative treatment. However, for clinicians who seek to practice evidence-based medicine, this form of therapy poses significant difficulties and limitations. These include lack of standardization of different preparations, lack of data regarding mechanism of action, and a paucity of controlled trials. Although randomized controlled studies that meet conventional standards have been reported for a variety of herbal products in the treatment of several diseases other than malignancy, 8 herbal treatments for cancer have rarely been subjected to this degree of scrutiny.
For more than 20 years, we have designed and applied treatments based on natural substances to a variety of conditions, including malignancies. We have found that patients with HCC in particular seem to benefit from this therapy. In a number of cases, the tumor was found to decrease in size, the tumor marker levels decreased substantially, and the patient survived comfortably for more than 5 years. Here we have summarized our results in applying our naturopathic therapy to HCC. We show that there is a strong correlation between survival and the number of preparations administered, thereby providing evidence for efficacy.
Patients and Methods
Patients
We began administering naturopathic treatment to patients with HCC in 1998. Records were available for review for 153 patients. The records for some patients seen between 1998 and 2002 have been lost, but all available records are included, including records of all patients seen since 2002. Fifty-two patients were seen once and either did not qualify for treatment or did not return. Eight of these are known to have died a median of 22 days after presentation, whereas the fate of the others is not known.
Consent
All treatment protocols were approved by the ethical review board of our hospital, which includes physicians, nurses, and pharmacists. On their initial visit to the hospital or clinics, patients and their families are given a 90-minute orientation to our approach to treatment. This includes mention of the likelihood that the case will be included in a presentation or publication. Those who agree to treatment are accepted as patients. For inpatients, written consent both for treatment and for inclusion in presentations or manuscripts is obtained on admission. For outpatients, written consent for inclusion in presentations or manuscripts is obtained on initial preparation of the preparation or manuscript. On completion of the manuscript, oral confirmation of consent is obtained from surviving patients who can be contacted. Inclusion of patients in the manuscript is also reviewed and approved by the ethical review board.
Diagnosis of Hepatocellular Carcinoma
This analysis describes 101 patients who were given naturopathic treatment
The diagnosis of HCC was based primarily on characteristic dynamic computed tomography (CT) imaging (early contrast enhancement during the arterial phase with washout during the portal venous phase), with serum levels of α-fetoprotein (AFP) and/or prothrombin induced by vitamin K absence or antagonist II (PIVKA II, also called des-gamma carboxy prothrombin) providing supportive evidence.5,9 In cases that had previously undergone surgical resection, the diagnosis was confirmed by histopathology. Patients who had undergone resection were excluded unless the tumor had recurred after resection and was no longer operable. Patients who had undergone PEIT, TACE, RFA, and/or chemotherapy were included. Patients were not prevented from continuing these therapies after beginning naturopathic therapy.
Staging
Tumor staging at the time of treatment initiation was performed according to the Barcelona Clinic Liver Cancer (BCLC) classification.10,11 Liver disease was assessed at the time of initiation of naturopathic treatment by a modification of the Child–Pugh classification, 11 in which the platelet count was substituted for the prothrombin time (platelet count ≥100 000 = 1 point, <100 000 and ≥50 000 = 2 points, <50 000 = 3 points). Because of this modification, and because performance staging was not done, the actual BCLC classification that we used was a modification. The tumor staging itself followed the standard BCLC classification, as follows:
(0): 1 HCC < 2cm: carcinoma in situ
(A): 1 HCC or 3 nodules <3 cm
(B): Multinodular
(C): Portal invasion or N1/M1
(D): Terminal stage
Treatment
Patients were treated with combinations of the natural agents listed below. Blood cell counts, measures of hepatic and renal function, urinalysis, tumor markers, tumor size on imaging, and chest x-ray were monitored.
The survival data reported here was assessed from the time of initiation of naturopathic treatment. Patients lost to follow-up were considered to have died 1 day after the last kept follow-up visit, and thus the calculated survival figures are minimum estimates. Survival data were analyzed by Kaplan–Meier statistics, using Prism software.
Agents
The following naturopathic treatments were used, given as oral preparations.
Cordyceps sinensis
This came from wild-grown, natural Cordyceps sinensis that was subjected to far infrared ray heating, brewing with Aspergillus oryzae and lipophilization with sesame oil, as previously described.12-14 This process has been shown to activate antioxidant, tumoricidal, and other biological activities contained in natural products.12-15 C sinensis is a parasitic fungus that infects insects, which has long been used in traditional Chinese medicine. The active ingredient in C sinesis, cordycepin, has been known since 1950 to be a purine nucleoside analogue, 3′-deoxyadenosine, and acts as an antimetabolite of adenosine.16,17 This compound was shown more than 40 years ago to have anticancer activity in both human and rodent systems in vitro and in rodents in vivo.17,18 The mode of action is thought to be related to the termination of nucleic acid synthesis.19-21 Moreover, it has been shown that cordycepin exerts a variety of pharmacologic effects in different tumor cell lines, and rodent systems, including inhibition of polyadenylation, stimulation of adenosine A3 receptors, and induction of apoptosis.19,22,23
TT, OT, B-T
These are closely related Chinese natural products that are harvested and produced in Taiwan that have been widely used in traditional Chinese medicine for centuries. TT consists of extracts of Bezoar bovis, Talcum crystallinum (Kadinum), Rhei rhizoma, Hoelen, and Arecae semen. B-T consists of extracts of Bezoar bovis, Kadinum, Rhei rhizoma, Phellodendri cortex, Arecae semen, and Mori folium. OT consists of extracts of Bezoar bovis, Kadinum, Rhei rhizoma, Hoelen, Arecae semen, Mori folium, and Crassocephalum crepidioides.
HTT
This is a modification of TT containing Harpago, a variety of pedaliaceae from the Kalahari Desert in Africa.
WBF
This is another traditional Chinese product containing extracts of Zizyphi fructus, Kadinum, Moutan cortex, Puerariae radix, Ginseng radix, Zingiberis rhizoma, Rhei rhizoma, Glycyrrhizae radix, Saposhnikoviae radix, and Trichosanthis radix.
Natural antioxidants (NAO)
This preparation was developed and is produced by the authors, as previously described. It is produced from wheat germ, rice bran, soybean, hato mugi (a type of oriental wheat), wheat, sesame, green leaf extracts from Japanese green tea and Yuzu oranges. The extracts are subjected to far infrared ray heating, brewing with A oryzae (koji), and with lipophilization with sesame oil treatment as described above for C sinensis. We have used this product successfully for a variety of therapeutic applications.12-15,24-26
UCR
This is derived from Guacatonga (Casearia sylvestris), a tropical plant grown in the clay soils of the Amazon. It is taken as tea and is said to show antitumor activity.27,28 It is also used to treat benign digestive disorders.
TIM
This is an extract of the bark of Tecoma ipe Mart, a tree that grows throughout South and Central America. It contains naphthoquinones, furanonaphthoquinones, and other compounds reported to have anticancer, antimicrobial, and anti-inflammatory properties. 29
BG103
This is β-glucan extracted from the edible Agaricus blazei mushroom, reported to be effective in several types of malignancy. It shows in vivo immunomodulatory and anti-inflammatory antitumor effects.30,31 Other extracts from this mushroom have been shown to have specific antitumor activity against hepatoma cells.32,33
BWS
This is derived from the seeds of loquat, known to be rich in amygdalin, which has been claimed to have anticancer activity.
BG105
BG105 is “Chaga,” an aqueous extract of an edible mushroom, Inonotus obliquus, that grows in northern Asian latitudes, for example, in Siberia, Hokkaido, and Mongolia. It has been reported to inhibit the protease of HIV-1. 34 Recent literature has extensively documented antioxidant, antitumor, and hypoglycemic activity.35-39 The agent is used in Japan for a variety of benign and malignant conditions.
Sandbath treatment
The sandbath is produced from stones that emit far infrared radiation (4-14 µm). This treatment has been reported to inhibit the growth of tumor cells in mice. 40 The patients undergoing this treatment also received intravenous multivitamin infusions.
Regimen
WBF was specifically applied for HCC, and other agents were generally given for the overall purpose of inhibiting tumor growth. Agents were added or substituted when there was evidence of tumor progression (increase in AFP, PIVKA II, lactate dehydrogenase [LDH], or tumor size on CT scan). In particular, C sinensis was generally used for signs of tumor progression. Detailed therapeutic regimens for the patients tested are described in the Results section.
Lifestyle counseling
Patients were routinely counseled to get adequate sleep, and to avoid overwork, mental stress, and dietary fat.
Data Collection
Data were obtained from the medical records. In addition to demographic data, routine laboratory data mentioned above, and all administered therapies, the following were obtained: tumor imaging by CT, presence or absence of cirrhosis, underlying liver disease (eg, HCV, HBV, alcoholism, other), presence and location of metastases, AFP, PIVKA II, previous outside treatments, including surgery, outside treatments occurring during naturopathic therapy, and dates of such treatments.
Results
Patient and Disease Characteristics
The data presented here are from the 101 patients who were started on treatment with the natural products described in the Patients and Methods section, who returned for follow-up and for whom records were available. The characteristics of these patients are shown in Table 1. Most of them had underlying cirrhosis (84%), and most of them had chronic infection with HCV (63%), HBV (18%), or both (1%). Nine patients had metastatic disease.
Characteristics of Total Patient Population a

Abbreviations: HCV, hepatitis C virus; HBV, hepatitis B virus; AFP, α-fetoprotein; PIVKA II, prothrombin induced by vitamin K absence or antagonist II; BCLC, Barcelona Clinic Liver Cancer stage; TACE, transarterial chemoembolization; PEIT, percutaneous ethanol injection therapy; RFA, radiofrequency ablation.
Comparisons of frequencies by Fisher’s exact test, medians by Mann–Whitney test, means by t test, and tumor stage distribution by χ2 test.
Metastases were to lung (6), adrenal (2), bone (2), spleen (1); one patient had metastases to 3 sites.
More than a quarter (27%) of the patients had had no previous treatment. Of the remainder, 20% had had surgical resection of the primary tumor, with subsequent relapse. Other prior treatments included TACE (50%), RFA (28%), PEIT (15%), and chemotherapy (14%). Thirty-three percent had undergone one of these treatment modalities, whereas 40% had undergone 2 or more. Thirty-eight percent of patients underwent one or more conventional forms of treatment concurrent with naturopathic treatment.
The median modified Childs–Pugh score was 6, ranging from 3 to 13. As shown in Table 1, the BCLC tumor stage was grade 0, A, or B in 81 patients, and grade C or D in 20 patients. There were 25, 33, 18, 12, and 13 patients, respectively, in BCLC stages 0, A, B, C, D (as modified, above) at the time of presentation.
Treatment Regimens
Patients were treated with combinations of the natural products described in the Patients and Methods section. A total of 12 different agents were used. The 6 most commonly used were HTT, WBF, NAO, BG103, C sinensis, and BWS, which were given to 96, 95, 72, 39, 27, and 17 patients, respectively. The most common combination was that of HTT, WBF, and NAO, which was given to 66 patients, with or without BG103 and/or C sinensis. Another 25 patients were given HTT and WBF without NAO, with or without other agents. Patients were usually started on 2 or 3 agents (mean ± SD = 2.6 ± 0.8), and other agents were added or substituted later if there was evidence of tumor progression. Patients attended clinic monthly or bimonthly until they died, were lost to follow-up, or were too debilitated to attend. Median time from beginning of treatment to death or last clinic visit was 13.4 months, range 0.8 to 100.8 months, mean ± SEM = 25.7 ± 2.7 months.
Strong Correlation Between Survival and Number of Agents Administered
Fifty patients were eventually treated with 4 or more agents. In these patients, the fourth agent was added a median of 8 months after starting treatment (range = 0-80 months). Eight patients were started initially on 4 or more agents. Overall, 101 patients were treated with 3.7 ± 1.2 agents (mean ± SD). As shown in Figure 1A, there was a strong positive correlation between the duration of survival following the initiation of treatment and the number of agents used (r2 = .3575, P < .0001). In contrast, there was a complete lack of correlation between the time interval from diagnosis of HCC to the start of naturopathic treatment (lag time to treatment) and the number of agents used (Figure 1B), but there was a positive correlation between overall survival and the number of agents used (Figure 1C). These findings provide evidence that the naturopathic treatment itself, rather than patient selection or previous treatment, exerts a positive effect on patient survival.
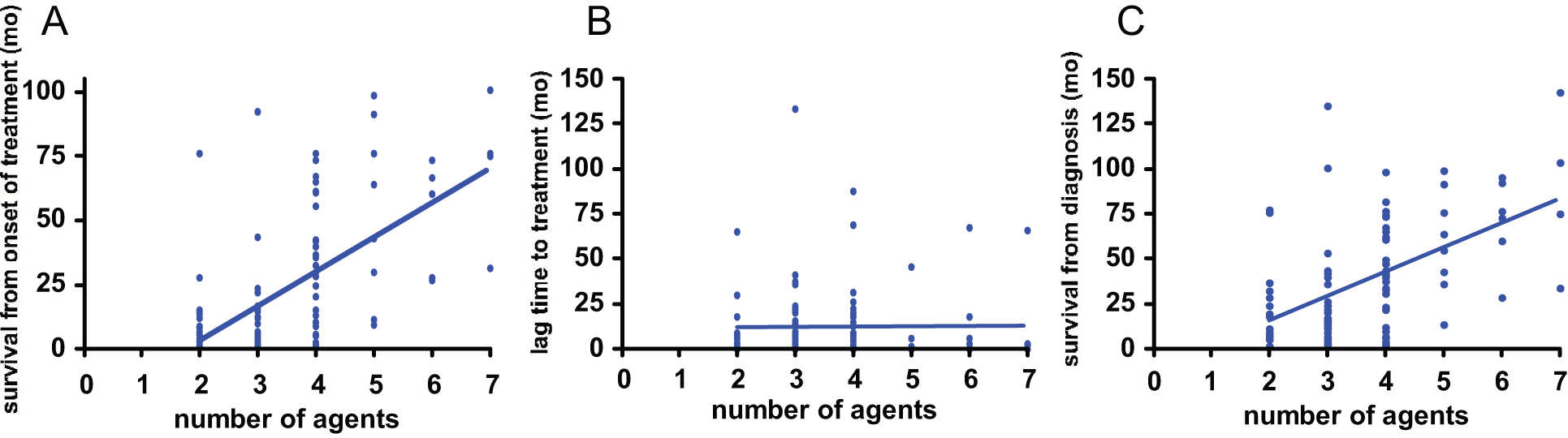
(A) Positive correlation between number of agents used and survival after onset of treatment in 101 patients with hepatocellular carcinoma (HCC); r2 = .364, P < .0001. (B) No correlation between number of agents used and time interval from diagnosis of HCC to onset of naturopathic treatment; r2 = .000, P = .941. (C) Positive correlation between number of agents used and overall survival; r2 = .288, P < .0001
Comparing the survival curves of the 50 patients treated with ≥4 agents (4.7 ± 1.0, mean ± SD) and the 51 patients treated with ≤3 agents (2.7 ± 0.5, mean ± SD), there was a dramatic difference in median survival (40.2 vs 6.4 months, respectively, P < .0001; Figure 2). As shown in Table 1, there was no significant difference between these 2 groups with respect to most of the presenting characteristics. The three exceptions were the proportion receiving chemotherapy, the median serum AFP level (50 vs. 24) and the median time interval between the diagnosis of HCC and the onset of natural product therapy (7.6 vs. 2.0 mo).

Survival of 101 patients with hepatocellular carcinoma
Evidence That the Increased Survival in Patients Treated With ≥4 Agents Is Biologically Significant
Although the correlation between the number of agents given and survival potentially suggests an effect of treatment, several potential artifacts need to be considered. It is possible that the correlation might simply reflect a censoring effect, that is, the disproportionate addition of more than 3 agents to the regimen of patients who had already survived longer. It is also possible that the patients treated with ≤3 agents had more advanced disease at the outset. Another possibility is a difference in the use or response to conventional therapy.
Further examination of the data indicates that these possibilities were not major underlying factors. First of all, the difference in median survival, 34 months, was far greater than the 8-month median time lag between the start of treatment and the addition of the fourth agent. Second, in the group treated with ≥4 agents, there was no correlation between overall survival after onset of treatment and the interval between onset of treatment and addition of the fourth agent (r2 = .015, P = .397, ie, not significantly different from 0).
Moreover, the advantage favoring the patients treated with ≥4 agents is seen even when patients are excluded from the analysis who died early in the course of treatment, and might therefore not have survived long enough to have a fourth agent added. As shown in Figure 3A, 21 patients who died within the first 3 months after the start of treatment are excluded. Seventeen of these patients were treated with 3 or fewer agents. In the remaining 80 patients, the dramatic difference in median survival between patients treated with ≥4 agents and patients treated with ≤3 agents is still evident (42.2 vs 12.3 months, P < .0001).
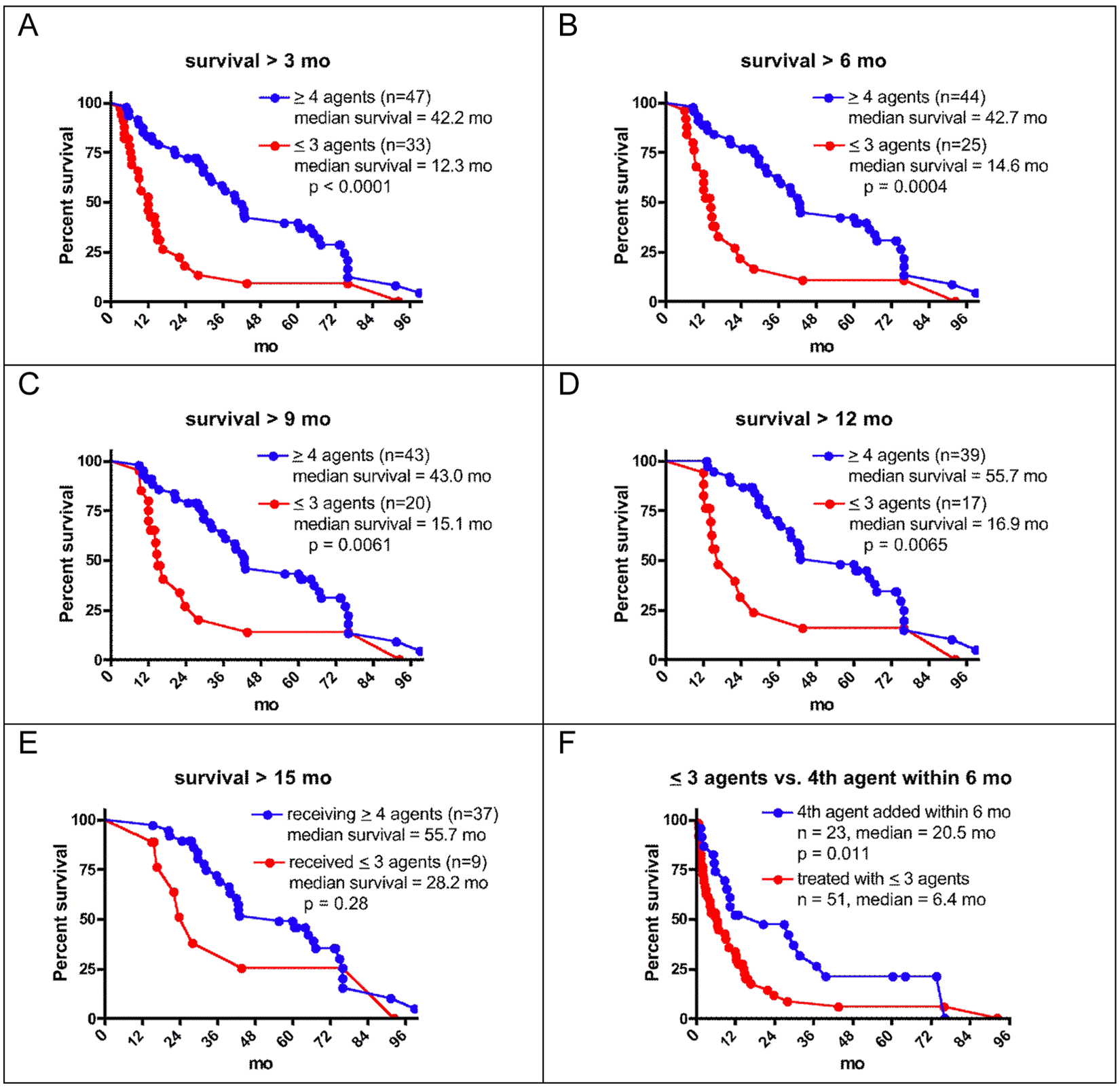
(A-E). Survival from the start of natural product therapy in patients who survived more than 3, 6, 9, 12, or 15 months on this therapy. For all 5 analyses, there is longer survival after the onset of treatment in patients treated with ≥4 agents, compared with patients treated with ≤3 agents. The differences are statistically significant for the first 4 groups. (F) Survival from the start of natural product therapy for all patients treated with ≤3 agents (n = 51), compared with patients treated with ≥4 agents for whom the fourth agent was started within 6 months of starting therapy (n = 23). The fourth agent was added a median of 1.0 month after onset of therapy. There is a significant survival advantage to the group given ≥4 agents (median survivals of 20.5 vs 6.4 months, P = .011)
The characteristics of this subgroup of 80 patients are shown in Table 2. In these patients who survived to at least 3 months on treatment, the only significant difference between the 33 patients treated with ≤3 agents and the 47 patients treated with ≥4 agents was the median interval between diagnosis of HCC and onset of our treatment. This difference was smaller (3.5 months) than that seen in the total patient population seen in Table 1 (5.6 months), and again the difference in means was not statistically significant. As a group, the patients treated with ≤3 agents thus do not appear to have had significantly more severe disease than the patients treated with ≥4 agents.
Characteristics of Subset of 80 Patients Surviving at Least 3 Months After Start of Natural Product Therapy a

Abbreviations: See footnote to Table 1.
Comparisons as in Table 1.
Metastases were to lung (6), adrenal (2), bone (2), spleen (1); one patient had metastases to 3 sites.
In Figure 3B, the 69 patients who survived at least 6 months are considered. The significantly longer survival advantage for the patients treated with ≥4 agents is still evident (42.7 vs 14.6 months, P = .0004). The characteristics of this subgroup of 69 patients are shown in Table 3. There are no statistically significant differences in any of the characteristics between the 25 patients treated with ≤3 agents and the 44 patients treated with ≥4 agents. Similar analyses are shown in Figure 3C-E for the subgroups of patients who survived >9, >12, and >15 months, respectively. Highly statistically significant differences are seen between the treatment groups in the >9 and >12 months subsets, in each case favoring the group treated with ≥4 agents. The same trend was seen for those surviving >15 months but was not statistically significant.
Characteristics of Subset of 69 Patients Surviving at Least 6 Months After Start of Natural Product Therapy

Abbreviations: See footnote to Table 1.
In Figure 3F, comparison is shown between the survival of the 51 patients who were treated with ≤3 agents and the 23 patients who were treated with ≥4 agents for whom the fourth agent was added within 6 months of the onset of naturopathic treatment. This time point was chosen because it was the median survival time for the patients who were treated with ≤3 agents. In this group, the median time to addition of the fourth agent was 1.0 month (mean ± SD = 1.8 ± 2.3). There was a definite survival advantage to the group receiving ≥4 agents (median survival 20.5 vs 6.4 months, P = .011). The characteristics of these 2 groups are compared in Table 4. The only significant difference was seen in the proportion of patients who had previously received chemotherapy, but chemotherapy was not associated with any difference in survival in either group (data not shown).
Characteristics of Subset of 23 Patients Started on a Fourth Naturopathic Agent Within 6 Months, Compared With the 51 Patients Treated With ≤3 Agents

Abbreviations: See footnote to Table 1.
In the 50 patients who received ≥4 agents, the survival after the addition of the fourth agent was significantly greater than the overall survival of the group receiving ≤3 agents (13.5 vs 6.4 months, P = .005; Figure 4). Moreover, as can be seen in Figure 4, the survival after the addition of the fourth agent was biphasic, with approximately half the patients dying within 10 months. The median survival after addition of the fourth agent of the 24 patients who survived at least 10 months after addition of the fourth agent was 36.5 months, and their overall median survival was 67.5 months. This suggests that a subgroup of patients show a robust response to the addition of the fourth agent. The 26 patients who died within 10 months of addition of the fourth agent and the 24 patients who survived more than 10 months did not differ significantly from each other in any of the parameters shown in Tables 1 to 4 (data not shown).
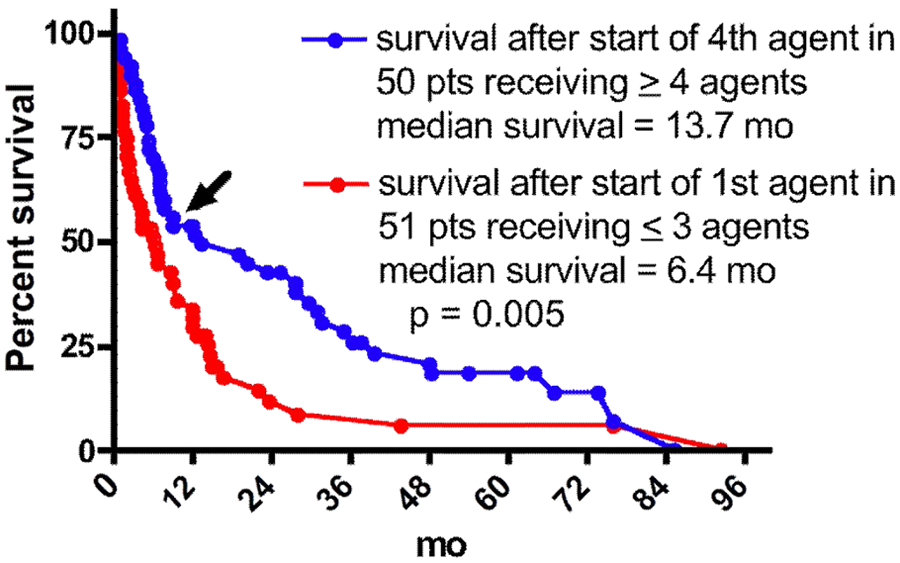
Prolonged survival after start of the fourth agent
Possible Additional Benefit of Cordyceps sinensis
Among the natural product agents used, C sinensis was given almost exclusively in the context of at least 4 agents. Overall, 27 patients received this agent, and 25 of them also received at least 3 other agents. There was a dramatically greater median survival in the patients given C sinensis compared with all of the other treatment combinations (42.7 vs 15.7 months from the onset of therapy, P < .0001; Figure 5). Among the patients treated with ≥4 agents, significantly more who received C sinensis showed prolonged survival after addition of the fourth agent in Figure 4. Even when compared with the other patients receiving other regimens containing at least 4 agents, the patients receiving C sinensis and at least 3 other agents showed significantly longer survival (55.7 vs 32.5 months, P = .047; Figure 6).

Comparison of patients surviving >3 months on therapy treated or not treated with Cordyceps sinensis
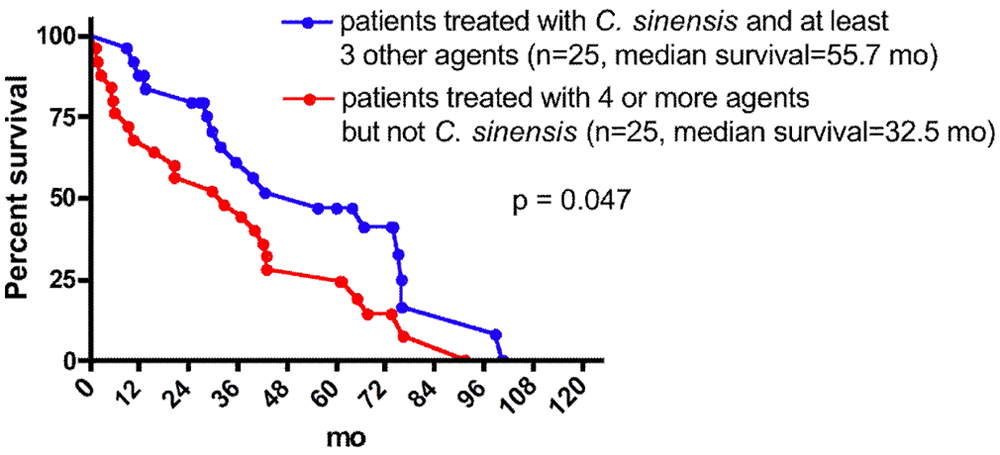
Comparison of patients treated with Cordyceps sinensis and patients treated with other regimens that included at least 4 agents
Although the data in Figures 5 and 6 suggest the possibility that C sinensis has a significantly greater therapeutic effect than other natural products, it should be noted that some of the patients treated with C sinensis were also given up to 6 other agents. Out of the 27 patients treated with C sinensis, 2 received a total of 3 agents, 10 received 4 agents, 5 received 5 agents, 6 received 6 agents, and 4 received 7 agents. In contrast, none of the patients not treated with C sinensis received more than 5 agents. When survival of the 15 patients who received C sinensis along with 3 or 4 other agents is compared with that of the 25 patients who also received 4 or 5 agents, but not including C sinensis, there was no significant difference in median survival (Figure 7). In comparison with these 2 groups, the patients receiving C sinensis and either 5 or 6 other agents showed significantly longer median survival (75 vs 35.8 months for C sinensis with 3 or 4 other agents, and vs 32.5 months for patients treated with 4 to 5 other agents, P = .022; Figure 7). However, whether this effect depends specifically on C sinensis was not determined, since no patients not receiving C sinensis were treated with 6 or 7 total agents and thus no comparison can be made.

Apparent advantage of Cordyceps sinensis is seen only in combination with at least 5 other agents
To consider the possibility that the apparently longer survival with the higher number of agents is due to a censoring effect, the interval from the start of treatment until introduction of C sinensis was compared between the group (n = 10) receiving a total of 6 or more agents and the group (n = 15) receiving a total of 4 or 5 agents. There was a trend toward a longer interval in the first group compared with the second (mean of 34.5 ± 19 vs 20 ± 24 months), but it was not statistically significant (P = .118 by t test).
Further Evidence for Prolonged Survival in Patients Treated With ≥4 Agents
Sandbath and multivitamin therapy were treatments administered to inpatients in our hospital in Kochi, and were generally not available to patients seen in our outpatient clinics. The inpatients also tended to have more advanced disease. Table 5 shows the characteristics and survival of patients in relation to whether or not they underwent sandbath treatment. These patients also received intravenous multivitamins and other nonspecific measures associated with inpatient therapy. The 38 patients who underwent this treatment had significantly more advanced tumor grades than the patients not undergoing this treatment, and there was also a trend for higher modified Childs-Pugh score, serum AFP, and serum PIVKA II. Overall, the sandbath and vitamin treatment was associated with longer median survival that was not statistically significant (24.7 vs 14.6 months, P = .727). There was, however, dramatically longer survival shown by patients receiving 4 or more agents, compared with patients receiving 3 or fewer agents, irrespective of whether they underwent sandbath treatment (42.9 vs 6.7 months, P < .0001) or not (36.9 vs 6.0 months, P = .0006). This provides additional evidence that the number of natural product agents that were administered was a principal determinant of survival in the 101 patients with HCC in this study.
Characteristics of Patients With Respect to Sandbath Therapy

Abbreviations: See footnote to Table 1.
Data From Consecutively Treated Patients
As noted above, some records from patients treated between 1998 and 2002 were lost. However, several patients who showed prolonged survival started treatment during that interval. To eliminate the potential for bias toward favorable outcomes, the data were also analyzed for the 84 patients consecutively treated since 2002 for whom complete records exist. The characteristics of these patients are shown in Table 6. There were no significant differences between the 49 patients receiving ≤3 agents and the 35 patients receiving ≥4 agents with respect to any of these characteristics. However, as shown in Figure 8, the latter group showed significantly longer median survival (29.8 vs 6.0 months, P < .0001). As shown in Figure 9, this significant difference persists if the patients not surviving 3 months of treatment are not considered (30.0 vs 12.2 months, P = .0016).
Characteristics of Consecutively Treated Patients Treated Since 2002

Abbreviations: See footnote to Table 1.
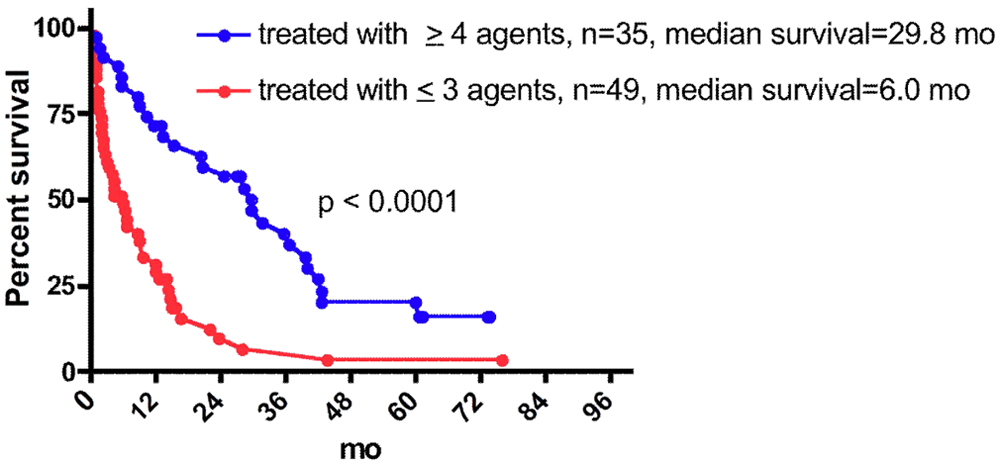
Survival of consecutively treated patients since 2002
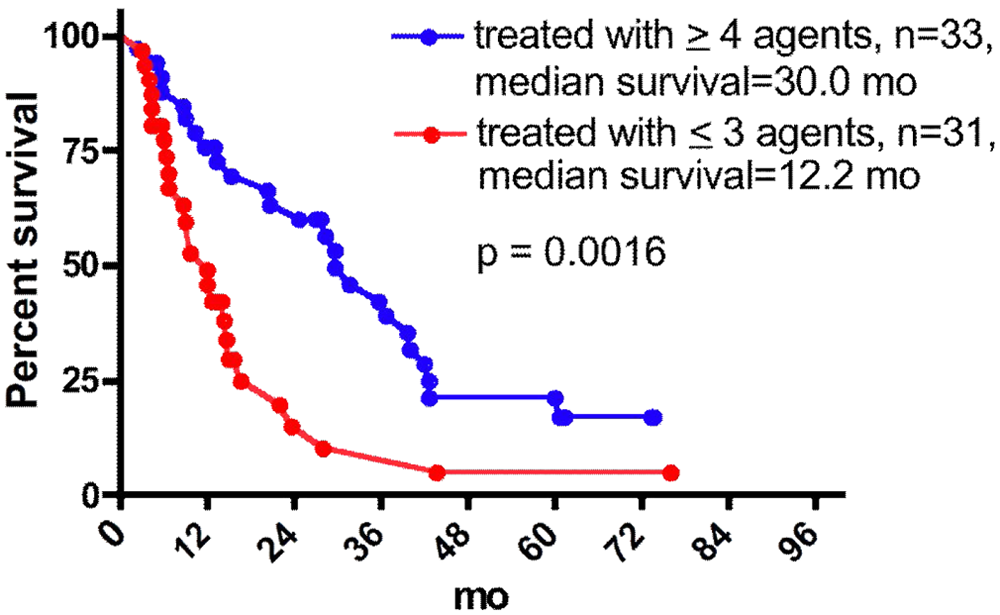
Survival of consecutively treated patients since 2002 treated >3 months
Effect of Conventional Therapy
As noted above, three fourths of the patients had undergone previous treatment, and 38% underwent conventional treatment (TACE, PEIT, RFA, or chemotherapy) concurrent with naturopathic treatment. Overall survival from onset of naturopathic therapy was not significantly longer in the patients who underwent any conventional therapy, compared with those who did not (Figure 10A), although there was a trend toward a beneficial effect of conventional therapy. Panels B, C, and D of Figure 10 show a subgroup analysis of the survival in patients who had no outside therapy, previous outside therapy, or both previous and concurrent outside therapy, respectively. In each of these groups, the patients who received 4 or more naturopathic agents survived significantly longer than those receiving ≤3 agents. The most dramatic effect was seen in patients given 4 or more agents who underwent both prior and concurrent conventional therapy.

Survival according to conventional treatment before or during naturopathic treatment
Of the patients who received C sinsensis, the median survival was 31.8, 28.4, and 76.2 months, respectively, for the groups that had no outside therapy, previous outside therapy, or both previous and concurrent outside therapy. This is consistent with the observations above that any benefit seen with naturopathic therapy was maximal in the patients given C sinsensis.
Effect of BCLC Stage on Survival and Comparison With Published Literature on Conventional Treatment
In an attempt to compare survival outcomes in our patients with those treated conventionally, we examined survival according the modified BCLC classification stages and compared these with published studies. As shown in Figure 11, survival was inversely correlated with the BCLC stage, whether determined from the time of diagnosis or from the beginning of naturopathic therapy. Moreover, survival in each stage was comparable to that reported in the 3 studies cited.41-43 These studies were picked because they are recent, used the BCLC classification in a large number of patients, and included 2 from Asian populations.

Comparison with the literature of survival data based on Barcelona Clinic Liver Cancer (BCLC) classification
The patient survival within each BCLC stage was also analyzed with regard to the number of naturopathic agents given and the use of C sinensis. As shown if Figure 12, in patients with either early or advanced stage HCC, significantly longer survival was seen in the patients given ≥4 agents, or who were given C sinensis. The small group of patients with stage C or D disease that received these treatments showed a median survival (~30 months) that was 2- to 10-fold longer than that reported in published studies.

Survival data based on Barcelona Clinic Liver Cancer (BCLC) classification and naturopathic therapy
Discussion
Evidence for a Therapeutic Effect From Natural Product Agents
In a series of patients with HCC that was not amenable to curative treatment, treatment with at least 4 of the natural product preparations described in this paper was associated with significantly longer survival than treatment with 3 or fewer agents, and administration of more than 5 agents was associated with even longer survival. Several lines of evidence described in the Results section argue in favor of this being a true biological effect, thus suggesting that these agents have efficacy in this disease. The same effect was seen, irrespective of whether all patients were considered or only the subset of patients that survived at least 3 months of treatment (ie, those most likely to have benefitted from treatment). Since most of patients who died within 3 months were treated with ≤3 agents, this latter analysis removes a potential source of bias in favor of the ≥4 agent group. The same effect was also seen regardless of whether the patients were treated as inpatients or outpatients or were given sandbath and multivitamin therapy or not. It was also seen when only the subset of consecutively treated patients was considered, and it was seen in patients with both early (BCLC stage A) and advanced (BCLC stage C or D) disease. Survival in these patients was comparable or possibly even superior to that reported in recent series using a similar HCC disease classification scheme.
Most of the patients received conventional therapy for HCC, either before or concomitant with naturopathic therapy, or both. Overall survival was comparable in patients who did not undergo any conventional therapy and those who did. In all three groups of patients with respect to conventional therapy (none, only prior, or prior and concomitant), significantly longer survival was seen in the patients given ≥4 naturopathic agents compared with those given ≤3 agents. A similar effect was seen with C sinsensis.
Potential Artifacts and Study Limitations
Since the analysis is retrospective, the study population was not randomized, and the treatment was not placebo-controlled, and since most of the patients had previously undergone and/or continued to undergo other forms of therapy, several potential sources of artifact and limitation need to be addressed. The first is the possibility that the patients showing longer survival had less aggressive tumors and/or less severe liver disease, either intrinsically or as a result of previous treatment. This potential explanation is largely excluded by the comparisons shown in Tables 1-4 and 6, in which the patients receiving ≤3 agents and the patients receiving ≥4 agents are shown to be comparable, not dissimilar from what might be expected of 2 groups selected in a prospective, randomized fashion. Moreover, even among the group of patients treated with sandbath therapy who did show more severe disease (Table 5), treatment with ≥4 agents showed highly significantly prolonged survival compared with treatment with ≤3 agents.
The one significant difference seen in Table 2 is a longer median interval from diagnosis to the onset of treatment in the group receiving ≤3 agents, compared with the group receiving ≥4 agents (5.5 vs 2.0 months). This difference is also seen when the whole patient group is considered (Table 1, 7.6 vs 2.0 months), and when the subgroup of patients surviving >6 months is considered (Table 3, 6.1 vs 1.8 months). In all these cases, the difference in median survival was much greater (~28-34 months) than this interval. It is conceivable that the longer interval between diagnosis and onset of naturopathic treatment in the patients treated with 3 agents reflects a greater disease burden and severity with more rapid progression to demise. However, as noted above, the comparisons between the 2 groups shown in Tables 1-4 and 6 do not support this. Moreover, a subgroup with a longer lag time to treatment may also be expected to have a better median survival, because the most severely affected patients will have died before monitoring of the population starts. A subgroup with a shorter lag time to treatment is thus considered to be more representative of the entire original population. 44
A second possible source of artifact would be if the increased survival in the patients receiving ≥4 agents simply reflected the addition of the fourth agent and higher number treatments only in patients who had already survived longer already. However, as described in the Results section, the survival advantage for the group treated with ≥4 agents was still seen even after the patients dying up to 12 months after starting treatment were excluded (Figure 3A-D). It was also seen when the subgroup of patients started on a fourth agent within 6 months (at median of 1 month) were compared with those treated with ≤3 agents (Figure 3F). In addition, there was no correlation between overall survival after onset of treatment and the interval between onset of treatment and addition of the fourth agent, or the lag time to naturopathic treatment after diagnosis (Figure 1B). Moreover, the median increase in survival was far greater than the median interval from onset of treatment to addition of the fourth agent, even taking into account the longer interval from diagnosis to treatment in the group receiving ≤3 agents. Finally, prolonged survival was seen following the addition of the fourth agent, compared with the overall survival patients receiving ≤3 agents, particularly in a subgroup of patients (Figure 4).
A third factor to consider is the large number of patients who were presumed to have died but for which there was no definite confirmation. With regard to the conclusions, this would only be a confounding factor in the unlikely event that a disproportionate number of the patients receiving ≤3 agents and presumed to have died had actually survived much longer than assumed, compared with patients receiving ≥4 agents. In general, our patients are conscientious about follow up visits, and the assumption that permanent failure to follow up indicates death is a reasonable one.
Another factor to consider is the effect of conventional therapy. On one hand, the overall effect was not dramatic (Figure 10A). On the other hand, the prolonged survival in the group given ≥4 naturopathic agents and undergoing both prior and concomitant conventional therapy (Figure 10D) suggests the possibility of an additive or synergistic interaction that merits further investigation.
The retrospective and nonrandomized nature of the study also prevent us from excluding the possibility that the patients surviving longer might have been initially in better health, or to have had other, unmeasured characteristics that accounted for prolonged survival, unrelated to the number of agents they received. Furthermore, the patients were a self-selected group and may not be comparable to the patients described in the literature on conventional treatment.
Patients seeking out naturopathic treatment may generally be more proactive in managing their own health, and may thus have a survival advantage over the “average” HCC patient.
Another limitation of the study was the lack of a mechanism to monitor compliance. Although the patients were generally compliant with outpatient clinic visits, whether they were in fact taking the agents prescribed could not be accurately verified. As noted above, lack of complete mortality data on the patients lost to follow-up is another limitation.
Possible Mechanisms
If the apparent therapeutic effect of the natural agents is in fact real, then there must be at least one underlying mechanism, and possibly more than one, since there was substantial variation in the regimens given to patients. As presented above, a number of the preparations used have been shown or claimed to have antitumor activity.
As shown in Figures 5-7 and 12, our data suggested that C sinensis is one of the more effective agents used, especially together with at least 5 other agents. Although the active ingredient, cordycepin, has been used extensively for its antitumor effect in vitro, its reported use in treating patients with malignancy is largely confined to a very limited literature on combination therapy for leukemia. 45
The potential mechanism of the natural antioxidant preparation is described in the references cited above.12-15,24-26,40 The dramatically greater effect of ≥4 agents compared with ≤3 agents suggests a certain degree of synergy amongst the preparations used. Of the 50 patients who received ≥4 agents, all but 1 received HTT and WBF, and all but 7 received these 2 agents plus NAO. Systematic comparison of more standardized regimens in a prospective fashion may help elucidate this phenomenon and optimize therapy.
In conclusion, we have presented prime facie evidence that treatment of HCC with a regimen of at least 4 agents prepared from natural products is associated with prolonged survival in a substantial portion of patients. The apparent prolongation that we observed is comparable to, or exceeds, conventional treatment for advanced HCC and is associated with minimal toxicity and side effects. Our naturopathic treatment also seems to show a potentially beneficial interaction with conventional therapy. The data provide level II evidence 5 for the efficacy of naturopathic therapy and the rationale for more rigorously controlled trials.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.