
Abstract
Introduction. The high prevalence of complementary and alternative medicine (CAM) use among cancer patients (40%-83%) receiving conventional treatment and the complex relationship between the psychosocial factors that may contribute to or result from CAM use requires further understanding. The authors conducted a descriptive mixed-methods pilot study to understand CAM practices, attitudes, and beliefs among cancer patients at the Loma Linda University Medical Center. Methods. This was the qualitative phase of the study, and no hypotheses were set. A total of 23 face-to-face interviews were conducted, and thematic coding was used to analyze 22 interview transcriptions. There were 14 CAM users (64%) and 8 nonusers (36%). Findings. The themes present among those who used CAM were the following: physicians viewed as one aspect of health care options, a holistic view on well-being, satisfaction with CAM use, and 3 key coping methods (confrontive, supportive, and optimistic) to confront cancer. Themes were not independent of each other. Two themes were present among nonusers; nonusers trusted their physician and were more likely to express evasive coping methods. Discussion. Perceptions and behavioral patterns are complex predictors of CAM use. A better understanding of CAM, medical pluralism, and the perceptions of patients would help health care providers deliver a better quality of care. The promotion of integrative care may help health care providers better identify medical pluralism and would shift focus to patient-centered care.
Keywords
Introduction
Complementary and alternative medicine (CAM) is defined as a group of diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine. 1 It is estimated that in the United States, 38% of adults use CAM each year 2 ; however, the inclusion of certain CAM items is inconsistent. If we expand the definition of CAM to include prayer and the use of supplements, prevalence of CAM use increases to 62%. 3 Studies have also shown an increased use of CAM among cancer patients in the United States, 4 and prevalence is higher than that in the general population.5,6 Prevalence of CAM use ranges from 40% to 83%6-18 depending on CAM modalities included and the study population.6-8
Although it is documented that CAM use is highest among those of higher socioeconomic status (SES) and younger, educated, female cancer patients,19,20 many of these studies were not entirely representative of minority groups.21,22 Disclosure of CAM use has been found to be higher among white non-Hispanics compared with minorities, and disclosure was higher for provider-based CAM.23,24 Self-care CAM, such as herbal use, is consequently less documented. In addition, cultural and social factors that contribute to reasons for using CAM, the type of CAM used, and reasons for disclosure are not extensively documented. 22 Nonetheless, the high prevalence of CAM use among cancer patients receiving conventional treatment indicates a high prevalence of medical pluralism.
CAM use has also been associated with increased optimism7,25,26 among cancer patients, though, as previously mentioned, significance varies by type of CAM. 7 Optimism has been associated with quality of life and positive physical health outcomes.27-29 In turn, optimism is a contributor to how a person will adapt to or cope with a stressful situation.30,31 According to the Jalowiec 32 coping model, there are 8 coping strategies: confrontive, evasive, optimistic, fatalistic, emotive, palliative, supportive, and self-reliant. Coping among cancer patients has also been assessed33,34 and is correlated with quality of life and survival. 35 Thus, there is a complex relationship between the psychosocial factors that may contribute to or result from CAM use.
This increased use of CAM requires further understanding regarding predictors of CAM use among cancer patients. 19 Moreover, the inclusion of minority groups, the broader inclusion of CAM, and perceptions of CAM are necessary to further the understanding of CAM use among cancer patients. A greater understanding of medical pluralism would help increase communication between providers and patients from diverse communities, which is beneficial for 2 reasons. First, health care providers can better understand patient perceptions to improve quality of service. Second, health care providers can have the knowledge to counsel patients about the side effects of CAM or possible interactions when used concurrently with conventional cancer treatment.4,8,36
The purpose of this project is to understand CAM practices, attitudes, and beliefs among cancer patients at the Loma Linda University Medical Center (LLUMC) in Loma Linda, California, and to create awareness among health care providers as to the practices, attitudes, and beliefs of CAM amid cancer patients. This report focuses on the qualitative phase of a descriptive mixed-methods pilot study.
Methods
Data Collection
The inclusion criteria of the study targeted participants who were 18 years of age or older, who had been receiving cancer treatment at LLUMC in Loma Linda during the month of April, 2010, and were to be part of a heterogeneous group. Participants were selected from a convenience sample. Of 25 participants invited to participate, 23 (92%) participated in the study; 1 patient declined because she did not feel well, and the other patient could not participate because he was deaf/mute. In this analysis, 22 participants were included; one was excluded because of the poor quality of the interview tape. Medical records for all participants were reviewed to obtain demographic and clinical data.
This assessment was the first phase of a proposed, larger study: to design and validate an appropriate survey tool and to conduct face-to-face surveys to quantitatively assess CAM practices and beliefs among cancer patients receiving treatment from LLUMC. A mixed-methods approach was used to conduct methodological triangulation and as a means to reduce systematic bias and improve validity of the data. The study protocol was approved by the Loma Linda University Adventist Health Sciences Center Institutional Review Board. All participants gave informed written consent to participate.
Interviews
Interviews were completed in April 2010 at the LLUMC cancer center infusion room by 6 trained graduate assistants from the LLU School of Public Health. Methods were designed to reduce selection bias by selecting a sample population that is more representative of the cancer population attending LLUMC. Interviews were triangulated with respect to day of the week, time of day, patient demographics, and patients’ cancer characteristics.
A total of 23 interviews were completed using a semistructured guideline. A series of questions and probes asked participants to explain their cancer, cancer treatment, side effects, and what they do to control their side effects. Participants were then asked if they had “heard of the term complementary and alternative medicine before” and what they “understood it to be.” The interviewers were trained to be open with the definition of CAM to get the participant to illustrate what his/her perceived medicine or therapy was. If the participant listed anything other than what was prescribed by his/her doctor, he/she was asked if he/she disclosed this information to a health care provider and why not if the answer was negative. The interviewer also asked about the participant’s beliefs in spirituality and benefits of CAM use. Interviewers did not define spirituality for the participants but rather let the participants define spirituality on their own. The interview concluded by asking for the participant’s opinion on what would improve a patient’s communication with his/her provider, in order to empower the participant and show our appreciation for their participation.
Interviews were audiorecorded and were transcribed verbatim by the interviewer. One interview was conducted in Spanish by a bilingual interviewer and was subsequently transcribed into English.
Data Analysis
CAM use was defined as broadly as possible and followed the definition of the National Center of Complementary and Alternative Medicine. If patients identified their practice or use of a product in association with treating their side effects from cancer and/or conventional cancer treatment, treating their cancer, or curing their cancer, it was listed as CAM use.
Thematic coding37,38 was used to analyze interview transcriptions by identifying themes in 2 subgroups: CAM users and CAM nonusers. Following the grounded theory approach, 39 no prior hypotheses were set about patients’ perceptions, attitudes, beliefs, or practices. When possible, juxtaposed themes were identified between CAM users and nonusers. Themes of different coping strategies used were initially evident but generalized. Methods of coping were determined after a literature review revealed similarity between patients’ phrases and statements on the Jalowiec coping model. Themed coding was completed by 1 graduate assistant (KA) with assistance from the PI (JCB).
Findings
There were 14 CAM users (64%) and 8 nonusers (36%). The themes found among CAM users were as follows: physicians viewed as one aspect of health care options, a generalized holistic view on well-being, satisfaction with CAM use, and 3 key coping methods to confront cancer. These themes contrasted with those of nonusers who trusted their physicians and expressed evasive coping.
Characteristics of Participants
Demographics
In all, 68% of the participants were female and 32% were male. Age was diverse and averaged 62 years. The average age of the CAM users was 61.7 years, ranging from 39 to 82 years, whereas the average age of nonusers was 63 years, ranging from 26 to 83 years. Among CAM users, 64% were female, and 36% were male. A total of 21% was Hispanic, 29% Caucasian, 21% African American, 7% Indian, 7% Russian, 7% Chinese, and 7% of mixed race of Irish and Native American descent. Table 1 stratifies participant characteristics by CAM use and nonuse.
Characteristics of the Study Population
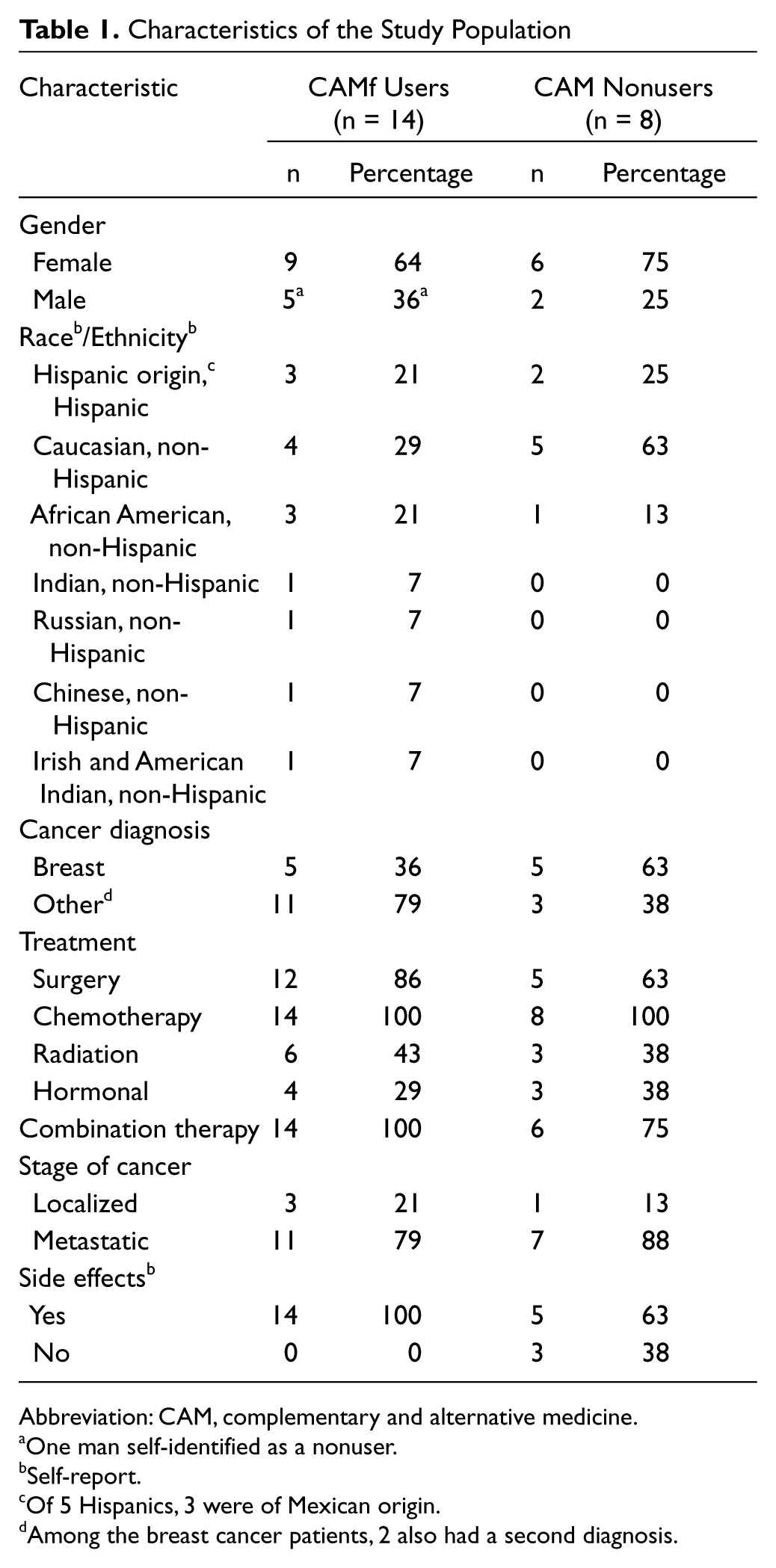
Abbreviation: CAM, complementary and alternative medicine.
One man self-identified as a nonuser.
Self-report.
Of 5 Hispanics, 3 were of Mexican origin.
Among the breast cancer patients, 2 also had a second diagnosis.
Health factors
Cancer diagnosis among men was diverse; each had a different diagnosis (n = 7). Among the 15 women, 10 (67%) had been diagnosed with breast cancer and 2 with ovarian cancer; the other 4 each had a different diagnosis. Two female breast cancer participants had a second cancer diagnosis: ovarian and lung. Cancer stage ranged from 1 to 4; 18% had a localized current disease status, and 82% were metastatic. Treatment plans also varied among participants: 77% had surgery; 100% were receiving chemotherapy, 41% radiation, and 32% hormonal therapy; and 91% were on or had received combination therapy (2 or more). Most participants (86%) said that they experienced effects caused by the cancer and/or side effects caused by the cancer treatment (Table 1). Of those who said “no” to experiencing side effects (n = 3), none reported valuing CAM and did not use CAM currently or in the past.
CAM use
CAM therapies used by participants fit into 6 types: green tea, herbs including herbal supplements and herbal tea, dietary supplements, nutrition, spirituality, and other. Within nutrition-based CAM, participants reported using green tea, herbs (herbal tea, oregano, ginger, white cumin, black cumin, turmeric, a liver supplement, and marijuana), dietary supplements (multivitamins; vitamins A, B12, C, D, and E; calcium; omega-3 in the form of fish oil; magnesium; poly-MVA; Reservatol [resveratrol], garlic, broccoli, and carrot powder, and a “diet cleansing package”), and nutrition (garlic, onion, chilli powder, whole green chilies, mustard seed, leafy greens, fruits, vegetables, juicing, and baking soda combined with syrup). Non-nutrition-based CAM reported by participants included prayer, spirituality, meditation, relaxation, and use of a CAM provider (an acupuncturist and an “alternative doctor”). The perception of spirituality was wide ranging among participants and was generally described as the establishment of spiritual and/or mental well-being by means of prayer, meditation, faith/belief in God, positive thinking, and/or social support.
Two participants, both female, had used CAM prior to their cancer diagnosis. One used prayer, relaxation, and nutrition for overall physical and spiritual well-being, and one had acupuncture to treat chronic back pain. Among the 14 CAM users, 79% used more than 1 CAM therapy type, with a mean of 2.84 therapies used. Also, 13 (93%) of the CAM users expressed belief in CAM and/or valued CAM (Table 2).
Types of CAM Used Among the Study Population (n = 22)

Abbreviation: CAM, complementary and alternative medicine.
Self-report.
When the 1 participant who used CAM but did not express belief in CAM was asked if he had heard of CAM before, his response was as follows:
I heard about it but didn’t put a lot of thought about it because I don’t need it and haven’t had any major complications. (African American man, 66 years old)
It was unclear during the interview whether his use of herbs, dietary supplements, and prayer were directly related to his cancer treatment or even health. His attitudes, beliefs, and comments were consistent with those of nonusers. He did not express the same coping strategies as CAM users but rather placed all his trust in his physician.
Of those who used CAM, 64% reported that they disclosed their CAM use to a health care provider. These participants had disclosed their nutrition-based CAM, as opposed to their spiritual-based CAM. The other 36% of the CAM users were not directly asked if they disclosed their CAM use.
How Participants Perceived Physicians
CAM users: physicians were viewed as only 1 aspect of health care
Physicians, specifically oncologists, were not viewed by CAM users as the sole decision makers for a treatment, and nor were they the sole healers. Physicians/oncologists—most commonly referred to by participants as “doctors”—were needed to treat the physical effects of cancer. When 1 nutrition-based CAM user reported that he had not disclosed his CAM to any of his health care providers, he was asked if there was a reason why he had not mentioned it. His reply was as follows:
They’re more on the medical side of things. They’re more concerned about how I’m feeling, if there’s any side effects. That’s about it. (Hispanic man, 43 years old)
CAM users described the necessity of other aspects of health care to reestablish overall well-being. One aspect was the patient’s attitude and beliefs—beliefs that their cancer could be cured:
I don’t know that they can cure something that you don’t want them to cure. (Irish/Native-American woman, 66 years old)
The need to believe in your care is then linked with the larger aspect of mental and spiritual well-being. Although he was not a spiritual-based CAM user, when asked if he believed spirituality could be classified as CAM, this nutrition-based CAM user replied,
The mind can probably help heal a lot more than what a doctor can. (Caucasian man, 57 years old)
These CAM users articulated that physicians were not the sole healers; beliefs, the mind, and God were also an element of their health. Finally, some CAM users emphasized how to them the most important element of their care was God.
God, He is the owner of my life and He is the only one that will say “this is it, you live or die.” First is God and then the doctors. (Hispanic woman, 52 years old)
CAM nonusers trusted physicians and their prescribed treatment.
This perception of physicians contrasted with CAM nonusers who greatly trusted their physician. When given examples of types of CAM and asked if they had ever used CAM, these nonusers replied,
Treating the cancer, no. Strictly follow doctor’s orders. (Caucasian woman, 77 years old) I really rely on the medicine. I guess I can see results. (Caucasian woman, 83 years old)
When asked if they had ever spoken with a health care provider about CAM, nonuser patients replied,
No, I just figure they’ll tell me what I need to know. (Caucasian woman, 64 years old) No, I just listen what she tells me. I do what I’m told. (Caucasian woman, 66 years old) The doctors know what they’re doing. Because whenever I take medicine, it’s the doctor’s prescription. . . . I trust them. (Hispanic woman, 70 years old)
Holistic View of Well-being
CAM users made a connection between their physical, mental, and spiritual well-being. They associated emotional feelings, such as depression, and/or spirituality with physical pain or physical healing. When talking about the benefits of CAM use, these patients replied,
You feel stronger, you um I think that it has to do with the way you eat and the way you think also. (Hispanic woman, 57 years old) Probably boost up your feelings, decrease a lot of the pain. (Caucasian man, 57 years old)
Because of this connection, many CAM users expressed belief that their cancer treatment should also be holistic. One extensive CAM user (who used nutrition-based CAM and CAM providers) kept reiterating this point about her treatment:
It should be complex not just singular. Its social support and family support and alternative medicine and everything should be together.
The interviewer asked for clarification: “So it’s more than just taking the medicine?”
It’s more than that. It’s the exercise, it’s the spirit, it’s the hope and belief in what you are doing otherwise it’s not gonna work. (Russian woman, 48 years old)
CAM users, therefore, chose to do something in addition to taking their “medication.” They participated and took initiative in their treatment because of the belief that well-being is holistic. A holistic view of well-being meant that the conventional treatment plan was only part of their solution.
Satisfaction With Complementary Medicine Use
CAM users did not express a current or continued dissatisfaction with their conventional cancer treatment. Instead, they expressed satisfaction with the combination of conventional treatment and CAM use, because they did not want to limit themselves to conventional medicine alone. One nutrition and spiritual CAM user contemplated during the interview as to which combination of treatments worked best for her:
So now I’m wondering in my mind, was it the Cisplatin-Gemzar [chemotherapy] combination with the herbs that helped me feel better. I’m gonna try again and I’m coming for chemo. And I’m gonna do the [supplements and teas] again. (Hispanic woman, 57 years old)
This also shows how active this CAM user was in deciding a treatment plan that was best suited for her because she chose to undergo more chemotherapy and to complement it with CAM to help herself feel better.
Many of the CAM users did express knowledge of possible interactions between their conventional treatment and CAM use, as shown by the high disclosure rates. Consequently, some CAM users would only use certain CAM therapies when not undergoing chemotherapy or would stop CAM use if they were unsure of the interactions.
Although patients expressed satisfaction with their complementary medicine use and understood the necessity to undergo conventional treatment, there was still a concern with chemotherapy. These patients contrasted the potential harm to the body caused by the conventional treatment with the lack of harm caused by CAM, believing that CAM is natural and benign. One nutrition and spiritual CAM user articulated her understanding of chemotherapy and its contrast with CAM:
[CAM] doesn’t harm your body. I feel that what’s really harming your body is the chemo itself. Even though you gotta kill the bad things, you gotta kill the good things. I wish they would find something that would just kill the bad and do well with the other. (Hispanic woman, 57 years old)
Methods of Coping
Another theme found among participants was the type of coping methodology 40 used. CAM users took more control of their treatment options and how they were going to manage their life after diagnosis. These patients expressed confrontive, supportive, and/or optimistic coping methods. This is a noteworthy difference from CAM nonusers, who were more likely to be evasive in their coping methods.
Confrontive coping
All CAM users expressed confrontive coping, though some expressed it more strongly. Confrontive coping, based on the Jalowiec coping model,
40
may include setting up an action plan, trying to change a situation, learning something new to deal with a problem, or handling things 1 step at a time. CAM users linked an action with their feeling. That action or action plan was a way to reduce or eliminate a negative feeling or enhance a positive feeling. Feelings expressed by CAM users were both physical and emotional. Coping methods were most likely to be expressed when the patients were asked what they did to control their side effects. An example of a confrontive response by a nutrition and spiritual CAM user was the following:
I just go and eat a lot of fruits and vegetables and it relieves the anxiety. A little bit of natural juice, orange juice and then just juice it up and that relieves my stomach a lot too. (Hispanic woman, 57 years old)
Confrontive coping was also expressed in the diction used by CAM users. A verb used by some CAM users (n = 4) was “fight”:
Just fighting for every day for what it is. (Caucasian woman, 82 years old) I think it’s [nutritional CAM] going to help me with just fighting itself. It’ll help my body not allow the cancer to come back and to fight it and to be a lot healthier. (Hispanic man, 43 years old)
This was another difference between CAM users and nonusers; CAM nonusers never included the word “fight” to describe their action plans. In addition, a CAM user was more likely to actively be a part of his/her cancer treatment plan. This was commonly in the form of learning something new, such as doing his/her own research. Action plans were also expressed in the context of continuing the CAM use regardless of its proven efficacy.
I’m actually taking the Poly-MVA and I’m talking to my oncologist and he said it’s probably going to be ok but he’s not sure. I did some research online and I found that it’s ok to take it with chemotherapy. So I’m going to continue taking it. I don’t know if it’s working, but someone in the condition like me, just trying to do everything that you can. Ya know, just trying to get some cure. (Russian woman, 48 years old)
This CAM user not only sought information and spoke with her oncologist, but she developed her own therapy to do everything she could. Similar to other CAM users, the decision to seek and use CAM was a confrontive approach to her problem. She was able to play an active role in her treatment plan rather than being passive and only taking her prescribed treatment.
Evasive coping.
Unlike CAM users, who were more likely to use confrontive coping strategies, nonusers were more likely to respond evasively. When a nonuser was asked if she had any side effects, she responded,
I’ve been very good. I’ve never been sick. I never felt anything.
However, as the interview continued, she contradicted herself by describing side effects she experienced from her conventional cancer therapies:
One medicine I took on Thanksgiving Day took my voice away. . . . I’m sure I have some other ones but the biggest one for me was the nausea. (Caucasian woman, 66 years old)
Similarly, another nonuser initially said that her only side effect was feeling tired then later contradicted herself by speaking of other side effects, such as weight loss, vomiting, and increased blood pressure, later in the interview. Nonusers responded evasively by trying to get away from the problem and also by depicting their side effects as not being that important.
Hhmm now not really. I just feel kinda tired. Course, my fingernails came off and my hair came off. (Caucasian woman, 83 years old)
When asked if she had any side effects, this woman initially replied that she only felt tired. Similar to other nonusers, she went on to say that she did have other side effects; however, she described her hair falling out as if it was not that important.
Supportive coping
Supportive coping was expressed in many different forms. CAM users were more likely to say that social and family support was important. For some CAM users, support involved talking the problem over with family or friends. To other CAM users, support also involved depending on others for help. To some, it was even necessary to have that support to cope with their cancer diagnosis and treatment. Furthermore, CAM users were more likely to discuss the importance of forming or being a part of support groups with those who had been in or were in a similar situation:
When we sit in the waiting room, I have three daughters, you can tell when somebody is down . . . really down. They don’t want to make eye contact. We just kind of sit around them and start talking and help them. I think we’ve helped several of them, spiritually. They come in and they’re gloomy and they don’t want to look at you. Some of the time the girls and I get them talking. You know, their spirits are lifted a little bit, I think. The big thing is to keep up your spirits. That’s the biggest thing. (Caucasian woman, 82 years old)
Although some CAM users mentioned the importance of attending structured support groups, this nutrition and spiritual CAM user talked about giving support to others in the waiting room. Other CAM users too mentioned personally extending support to other patients. Many patients also said that they listened to their health care providers, though they mentioned this in the context of active 2-way communication. The diction used, again, is in contrast to that of nonusers. CAM users viewed this as “advice” rather than “doctor’s orders.” These patients not only sought support, but they valued it.
The last form of supportive coping was praying or putting trust in God. For some CAM users, this was also a spiritual-based CAM therapy. When asked if she believed that spirituality could be a form of CAM, this woman replied yes but that she did not use spirituality as her CAM. She then immediately stated,
Often times I really need to pray. I just often times need to talk to someone and I just do it and its really helping me. (Russian woman, 48 years old)
Although praying and spirituality were not used as CAM, seeking support was a coping strategy for her.
Optimistic coping
Optimistic coping was expressed in terms of thinking positively, thinking things could be much worse, comparing yourself to people in a similar situation, and trying to see the good side of a situation.
40
Optimism often referred to beliefs that the patient would have positive health outcomes. When asked if he believed spirituality was CAM, this spiritual CAM user replied,
Oh! Positive thinking is good. See, I’ve always had this thing, I’ll get better; even when they say I’m really bad. I’m not worried about it. I’ll say, “I’ll get better, I’ll get better.” I don’t let it control me. Think positive and it will do you wonders. (Caucasian man, 67 years old)
After he made this statement, he continually reiterated that he believed positive thinking was his “medicine,” and he went on to tell us how he would try to extend his optimism to other patients in the cancer center. Similar to other CAM users, if a participant’s coping methodology was optimism, it was a clear theme within their entire interview. For instance, another CAM user repeated the phrase “it could have been worse” 3 times during her interview, unprompted. The same CAM user, who used nutrition-based CAM and a CAM provider, also continually expressed optimism by comparing herself with others who were in the same situation. Another nutrition and spiritual CAM user contrasted herself with others and also described the benefits of spirituality as a coping strategy that extended to a day-to-day “attitude adjustment.”
A lot of [other patients] can benefit from an attitude adjustment. I mean it’s really easy to be feeling down and depressed and you know that you’re going to die but in that case, everybody is going to die. And you have to live every day. (Irish/Native-American woman, 66 years old)
Among many spiritual-based CAM users, spirituality, optimistic coping, and supportive coping were interrelated; thus, comments made depicted multiple coping strategies simultaneously.
Discussion
This qualitative assessment provides insight into the beliefs, perceptions, and practices of CAM users among cancer patients receiving biomedical treatment. It also provides insight into the attitude of patients who choose CAM after cancer diagnosis. Participants that sought and used CAM were more likely to view physicians as just one aspect of their care and to perceive well-being to be holistic. Behavioral patterns associated with CAM use were confrontive, supportive, and optimistic coping strategies, whereas, evasive coping strategies were associated with CAM nonuse. The main finding was that multiple themes were responsible for CAM use, and themes were not independent of each other.
The perception of physicians and well-being among CAM users illustrated an awareness of whole-person care on behalf of the patient. The themes of perceptions toward physicians, holistic well-being, and satisfaction with complementary medicine use among CAM users were interrelated, and no single theme was found to be more prevalent than another. Because all patients were currently receiving and believed in the benefits of receiving conventional cancer treatment, “alternative medicines” implied complementary practices. 10 Patients who sought CAM did not choose CAM over biomedical therapy but chose to use complementary medicine to achieve holistic well-being. These results are consistent with other studies that found that CAM users were not dissatisfied with their conventional treatment when deciding to use CAM but valued the perceived therapeutic gains of CAM and its lack of negative side effects regardless of its ability or inability to cure cancer.41-47 Together, these themes demonstrate the belief in and use of integrative medicine and medical pluralism. This is defined by the Consortium of Academic Health Centers for Integrative Medicine as “the practice of medicine that reaffirms the importance of the relationship between practitioner and patient, focuses on the whole person, is informed by evidence, and makes use of all appropriate therapeutic approaches, health care professionals, and disciplines to achieve optimal health and healing” (2004). The Institute of Medicine also proposed a needed “recognition of medical pluralism, p. 169.” (2005).
The perceptions of CAM users contrasted with that of nonusers. CAM users expressed concern over the side effects caused by conventional treatments, whereas nonusers did not place priority on the side effects caused by conventional treatments. 48 Nonusers also trusted their physician and his/her treatment plan. As found in another study, some nonusers devalued CAM and lacked confidence in its efficacy. 48 These findings also support those in the literature that CAM nonusers believed that the decision to use CAM is made when there is distrust in biomedicine.49,50
All cancer patients cope with their diagnosis and treatment in some way, though there are various means of doing so. CAM users sought CAM as a means of doing more than “tolerating the problem. 32 ” The act of doing research and seeking CAM remedies reflected taking a confrontive approach to their problem. Some forms of supportive coping were also confrontive: for instance, seeking support, asking questions, and being open-minded when communicating to others. Openness to experience and spirituality have also been shown to be predictors of CAM use. 51 Moreover, cancer survivors rated confrontive, supportive, and optimistic coping strategies as the most effective used among the 8 coping styles, and these 3 coping strategies were associated with better quality of life and survival. 35
Our present work also demonstrates an association between optimism and CAM use.7,25,26 Optimism has been significantly associated with better physical health outcomes, including in cancer. 29 Optimism can also determine the choice of coping strategies for people who are faced with a life-threatening challenge.33,34 These findings suggest that optimism is not only associated with CAM use but is also viewed as a form of spiritual-based medicine practiced complementary to biomedicine. Furthermore, CAM users believed that CAM, in addition to optimism and coping strategies, may contribute to better health outcomes or improved quality of life.
Though optimism is associated with CAM use, it is not necessarily a predictor for CAM use alone. Optimism is not an absolute predictor of behavior because it is only the belief that good outcomes will occur, 52 whereas self-efficacy is the belief that one has the ability to perform in a way that will lead to good outcomes. 53 Self-efficacy leads to better coping among cancer patients, which is associated with better quality of life and survival. 54 Because self-efficacy is a predictor of the type of coping strategy a cancer patient will use, it is most likely a predictor of their decision to use CAM therapies.
Our findings also demonstrated that CAM users were active in developing their treatment plan. An important difference between those deciding to try CAM and those solely taking biomedicine was that in the former case the patient was the one seeking and deciding on the treatment, as opposed to a physician telling the patient what to do. Other studies described this as a patient’s sense of control.42,48,55 These findings suggest that it is more than just a sense of control, however. The patient’s active role in his/her treatment plan improves the patient’s quality of life. 56 Furthermore, the decision to seek and use CAM and the act of doing so may in turn empower the patient. Our findings are consistent with those of other studies that demonstrate that CAM use creates a sense of empowerment.37,38,57-59
This study has a number of limitations. There is a possibility of misinterpretation of the data because of the subjectivity of the analysis. As this was a nonrandomized, convenience sample, there is potential for systematic bias. Because of the small sample size and differences between CAM users and nonusers, the study cannot demonstrate internal validity. Stratification and other statistical analyses were not possible because of the small sample sizes. There were also more CAM users interviewed than nonusers, though the goal of the study was to better determine themes among CAM users.
Despite these limitations, our study provides further insight into CAM use among cancer patients. Data triangulation was used to reduce selection bias by sampling over the duration of a month, on every day of the week and at various times during the day, and all patient types were included. Thus, the diversity of participants is more reflective of the general cancer patient-care setting. The broad definition of CAM (including types of CAM use that are neglected in other studies) may also allow more generalizability. This may more accurately reflect what patients perceive CAM to be. Furthermore, interviewing patients face to face was a unique advantage over using predefined, written surveys to better understand perceptions, attitudes, and beliefs and their complex relationships with CAM use or nonuse. Other data collection methods would not illustrate well the existence of the complex model found here. Conducting face-to-face interviews and having the support from LLUMC’s cancer center clinicians and staff also helped us achieve a very high response rate to include patients who may not have participated otherwise.
Future research should analyze differences in perceptions, attitudes, and practice of different CAM modalities. Specifically, predictors of nutrition-based CAM versus non-nutrition-based CAM would be most relevant in this population because of the potential for treatment interactions. Themes are not independent of one another, which should be taken into consideration to enhance decision-making models. Moreover, studies has yet to establish a model temporally associating self-efficacy, coping, CAM use, and empowerment. To further explore these relationships, the present authors have developed a survey tool to examine a cross-sectional association between perceived health, perceived control, self-efficacy, hope, coping methods, the value placed on CAM, and CAM use among cancer patients. The survey tool has been pilot tested, but will require further study to evaluate construct validity.
In conclusion, perceptions and behavioral patterns are complex predictors of CAM use. The increasing prevalence of complementary practices and perceptions of holistic well-being indicates awareness of and desire for medical pluralism. A better understanding of medical pluralism can give health care providers deeper insights into how patients make treatment decisions. Integrative care, which focuses on patient-centered care, seeks to empower patients in making informed decisions about whether or not to use CAM. Thus, a better understanding of CAM, medical pluralism, and the perceptions and preferences of patients can help health care providers deliver a better quality of care. Finally, by an improved understanding of cultural diversity and patient preferences, integrative care demonstrates a deeper commitment to the basic ethical principles of the care of patients. 60
Footnotes
Acknowledgements
We want to thank and acknowledge the support and cooperation from Dr C. S. Chen, MD, PhD, and the LLUMC Cancer Center and its infusion nurses. We want to thank all participants for their time and willingness to participate in the interviews. We would also like to recognize the LLU School of Public Health graduate research assistants for their contributions (Holly Schuh, Kristen Gunther, Mayra Barcenas, Biblia Kim, and Vinay Kumar) and the LLU School of Pharmacy research assistants (Anastacia Chetty and Annie Nazarian).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this project was provided by the Center for Health Disparities and Molecular Medicine, Loma Linda University, Loma Linda, CA National Institute of Health, grant # P20-MD001632.