
Abstract
Recent studies based on epidemiological models published in this journal and elsewhere have demonstrated encouraging patterns suggesting that herbal treatment may improve prognosis in advanced colon and lung cancer patients. Various problems exist with data from nonrandomized studies of this type, but a strong signal of potential positive effect can be seen. The therapeutic mechanisms of traditional Chinese medicine in metastatic cancer are discussed against a hypothetical, dualistic antiproliferation model and immune-stimulation model of tumor progression and regression. Recommendations are made for a strategy to demonstrate more conclusively the efficacy of adjunct herbal treatment during cancer chemotherapy and for discussions with patients until such time as the efficacy trials are completed.
Introduction
In 2008, nearly 13 million new cancers were detected, 1 and many more patients continued to live with cancer. In the Western world, the incidence of cancers of the lung, colorectum, prostate, breast, and endometrium has increased steadily, doubling over the past 50 years. Moreover, in developing countries with a very high population density, such as China, an even more impressive increase has been observed over the past 2 decades.2-4 In Figure 1, these 2 phenomena are exemplified for breast cancer incidence in Norway and Shanghai, China.
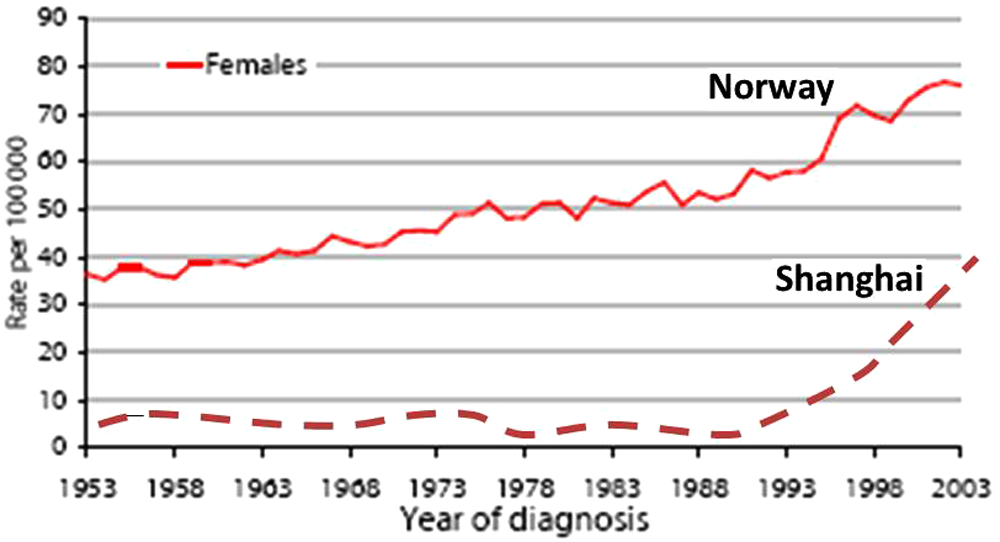
The incidence of breast cancer in Norway has steadily increased since 1950 and, in 50 years, approximately doubled (data from the Norwegian Cancer Registry). The incidence of breast cancer in Shanghai has traditionally been very low, compared with Norway, but since 1990, a sharp increase has occurred. As a result, the incidence by 2000 was 10 times higher than before 1990 (we acknowledge Prof Z. Shao, Fudan University Shanghai Cancer Center for the Chinese data)
Although the survival for certain malignant tumors has greatly improved since the 1970s, for many other common cancers, prognosis has only marginally improved, and for still others, it continues to be poor. Chemotherapy is notorious for its side effects, and in advanced cancers, it often has little effect. It is therefore understandable that cancer patients, especially those with a poor prognosis, do not restrict themselves to conventional medicine but seek help wherever they can.
Herbal traditional Chinese medicine (TCM) treatment in cancer has been reported to increase chemotherapy efficacy, reduce toxicity, prolong survival time, improve quality of life (QOL), and strengthen immune functions. 5
How Many Cancer Patients Use Herbal Medicine?
How many patients use herbal medicine each year? One study estimated that 48% of cancer patients use complementary and alternative medicines. 6 Many Chinese cancer patients believe that combining Chinese and Western medicine is effective, and 63% of those in Hong Kong receiving chemotherapy used Chinese medicine before, during, or after Western medicine treatment. 7 Similar figures were found in Shanghai for patients with stage 4 lung cancer. 8 It is interesting to note that nearly two thirds of Chinese patients treated with “Western” cytotoxic drugs did not tell their physicians that they were using TCM herbs. This implies that Western medicine doctors could easily underestimate TCM use. 7 If the above-mentioned 48% is also valid for the rest of the world, 6 at least 10 million cancer patients and probably many more use some form of herbal medicine each year. The total annual amount involved for cancer patients in the Western world alone therefore must make this a multi-billion-dollar business. In agreement with this, in 2009, it was mentioned in the Shanghai Daily newspaper that the annual sales figures of all TCM products in China were around 200 billion US dollars.
TCM herbs are easily accessible within China. In the United States, pan-Asian medicines also are easily available, many as “dietary supplements” according to US regulations. However, from April 30, 2011, the annual, nearly 1 million new European Union (EU) cancer patients who wish to use herbal medicine treatment will face considerably more difficulty in getting such treatment. From that date onward, the EU drastically limited the use of a number of medicinal herbs. 9 In the United Kingdom, herbal medicines sold must now be manufactured under Good Manufacturing Practice to ensure the quality of the finished product, and safety should also be demonstrated. 10 Of course, this is in itself a good rule and intended to protect future patients against abuse. However, herbal businesses are often small, and providing such proof is very costly. As a result, a number of herbal medicine sellers have terminated practice, and some Norwegian herbal medicine practices, who previously bought their high-quality herbs in the United Kingdom, have been unable to purchase herbs for quite a while and have had to terminate their practices. It is interesting to note that a number of Western pharmaceutical companies, over the past years, have bought Chinese TCM companies and also established large research and development laboratories in Europe and elsewhere to evaluate traditional herbs for medically active components. The reasons for these enormous investments no doubt have to do with seeking the best for cancer patients, but perhaps also with expected future profits.
Why has the EU so dramatically restricted the use of medicinal herbs? The official arguments used against current herbal medicine are that they can have toxic, life-threatening side effects or dangerous interactions with conventional drugs; are polluted with dangerous substances; and that they strip desperate patients of their money by means of scientifically unproven medications. 11 The first argument (life-threatening side effects of the herbs) is of course related to their effects, but it should be remembered that many accepted conventional cancer drugs are also well known for their many serious side effects. But are the side effects of TCM and Pan Asian herbs really serious? Hard facts are rare. In Norway (nearly 5 million inhabitants), 50 serious side effects of herbs (heart arytmias, liver damage) were registered in 2010 by the Norwegian Regional Drug Information Center. More detailed studies are certainly required. It is also quite reasonable that herbs should be produced according to Good Manufacturing Practice and not contain toxic substances such as pesticides or heavy metals, as has sometimes occurred. None of the readers of Integrative Cancer Therapies will argue that drugs—or herbs—should be given to patients if there is no hope for any benefit.
However, a point that is much more debatable is whether prospective clinical randomized trials are the only solid proof for a medical effect, and if all medications and laboratory tests have gone through such rigid tests before they were begun to be used. If so, it could also be argued that many widely used Western medical treatments should be withdrawn 12 (Booth A, University of Sheffield, UK, personal communication with JPB, July 29, 2011).
However, all this does not diminish the importance or the legitimacy of the question of whether any proof exists for the effectiveness of herbal medicine in metastatic lung and colon cancers. Consequently, we must continue to consider existing evidence and collect new proof that herbal treatment is useful in patients with metastatic cancers of these and other organ sites. In China, Liu’s 1996 lung cancer study is widely cited as proof of efficacy. 13 Three recent studies published in this journal observed that herbal medicine was associated with improved prognosis in patients with widespread metastatic cancer of the lung and colon.7,14,15 Moreover, comparable results were obtained in pancreatic cancer with metastases to the liver. 16
It is important to draw the attention of the readers of Integrative Cancer Therapies to these results. We will also consider the possible therapeutic mechanisms and discuss what still needs to be done to get irrefutable evidence for the usefulness of these medicines and gain worldwide acceptance for adjuvant herbal treatment in patients with metastatic cancers of the lung and colon.
Metastatic Lung and Colorectal Cancer, Treatment Possibilities and Poor Prognosis
Sadly enough, the prognosis of patients with pulmonary and colorectal cancers is especially poor: roughly two thirds of these cancers are detected in an inoperable, advanced stage, when the first clinical signs occur. On the other hand, compared with the 1980s, chemotherapy for metastatic lung cancer has improved and resulted in significantly better survival. 17 In spite of this, the median survival still is less than 12 months, and the death rate at 2 years is very high. The situation for colorectal cancer patients is comparable. Only about one third of the patients are operable at the time of diagnosis, and even then, about one third of these patients still die within 5 years.
The expectations of target therapy are very high and promising. For example, about 10% of patients with metastatic inoperable pulmonary adenocarcinoma bear epidermal growth factor receptor mutations. In this subgroup, median survival can be increased by 3 to 4 months with target therapy. 18 This may not sound impressive, but added survival of 3 months is a major step forward when compared with the 6 to 9 months of median follow-up of patients treated with modern chemotherapy alone. When similar specific treatments are developed for other cancer subtypes, it may in the future help further improve the prognosis of patients with a very poor life expectancy. However, the prices for target therapies can be hefty: Tarceva and Iressa treatments of epidermal growth factor receptor–mutated pulmonary cancers in Norway may be as high as US$ 150 000 to 200 000 per year. Even in Western countries, cost-benefit analyses of targeted treatment has led to questions being raised by health care administrators and decision makers. The costs of target therapies are certainly far beyond what most middle- and lower-class patients can pay in developing countries, where very many cancer patients live.
Estimated Costs of Palliative Care and TCM/Integrative Procedures, Compared With Conventional Chemotherapy and Target Therapy
Although the costs for medical care vary greatly between different countries, it is tempting to assess the approximate costs of TCM/integrative medicine compared with conventional chemotherapy and target therapy. The following estimates for Norway are approximate prices and do not take into account all possible variables, but they are still reasonably correct and good enough for the current goal—namely, to compare the costs of accepted Western medicine and herbal cancer therapies. The costs for cytostatic drugs alone for advanced lung cancer are approximately US$ 20 000 per year, whereas targeted therapy drugs of Western companies are about 7 to 10 times more expensive. Approximately the same prices hold for China. In Shanghai, China, TCM herbs for cancer patients cost 4000 to 10 000 Chinese Yuan (US$ 700-1600) per year, a fraction of the costs of chemotherapy and target therapy. It is clear that many other aspects such as the health care provider’s honorarium also play a role, but these figures make it clear that TCM herbal medicine can be very inexpensive.
Is TCM Herbal Treatment Effective in Metastatic Lung and Colon Cancer?
It is obvious from the above discussion that the relatively inexpensive herbal medicines could be a legitimate alternative, if they are really effective in improving the survival of patients with distant metastatic lung and colon cancer. In what follows, we present an overview of the current evidence.
In Liu’s 1996 study on 304 patients with stage IIIb and IV adenocarcinomas of the lung, TCM herbal treatment alone was more effective than using conventional chemotherapy available at that time. The 1-year survival rates were 61% and 37% (P < .01), median survival times were 13.7 and 8.7 months (P < .01), and 5-year survival rates were 24% and 0% (P < .01), respectively, for herbal and chemotherapy treatments. 13 However, target treatment was still unknown when the latter study was performed and, as mentioned, chemotherapy has also become more effective since then. There is no information about selection bias in the article.
Guo et al 8 from Shanghai, China, analyzed the prognostic effect of personalized TCM herbal treatment in stage 4 adenocarcinomas of the lung in patients diagnosed and treated from 2006 to early 2009 at the famous Longhua TCM hospital in Shanghai. All new patients were consecutive, fully ambulant outpatient clinic patients with performance scores of 0, 1, and 2, and all received platinum-based chemotherapy (PBT). The TCM group were patients treated by different TCM specialists in Shanghai. The controls were carefully age-, sex-, diagnosis-month, and performance-score matched concurrent similar patients from a large database of the Respiratory Hospital in Shanghai (which is a very large, modern Western medicine hospital not far away from the Longhua TCM hospital). All 133 patients in the 2 study cohorts received conventional PBT alone or PBT with/without second-line targeted therapy, with/without TCM. Patients with (1) combined chemotherapy, targeted therapy, and TCM; (2) chemotherapy + TCM without targeted therapy; and (3) chemotherapy only had 12-month survival rates of 94%, 78%, and 27%. For the same groups, median survival time was not reached (mean survival time of 30.9 months) and was 22.6 and 5.0 months, respectively. Thus, the additional use of TCM herbs with platinum treatment was associated with greatly improved survival. There was no difference in survival among patients with respect to whether they were treated by a well-known, very experienced, or other general TCM specialist.
The next lung cancer study was performed by McCulloch et al 14 in San Francisco, CA. They investigated the effect of pan-Asian medicine + vitamins (PAM+V) therapy, which included lifestyle counseling as well as herbs and vitamins, on survival in consecutive, non-small-cell lung cancer (NSCLC) patients treated during 1988-1993 with conventional chemotherapy (n = 239). Controls were selected from the Kaiser Permanente Northern California and California Cancer Registries. Long-term use of PAM+V beyond completion of chemotherapy reduced death in stage IIIB by 83% and stage IV by 72%, compared with chemotherapy only. When PAM+V was combined with conventional therapy, it reduced the risk of death in stage IIIA by 46% and stages IIIB and IV by 62% and 69% versus conventional therapy alone. Survival rates for stage IV patients treated with PAM+V were 82% at 1 year, 68% at 2 years, and 14% at 5 years. Thus, PAM+V treatment combined with conventional therapy compared with conventional therapy alone was associated with improved survival in NSCLC, and the effect was dose dependent.
The 2 studies differ in their design, enrollment period, chemotherapies and herbs given, lack of target therapy in McCulloch’s study, and a number of other details. In spite of this, it is striking that the survival rates with additional TCM herbal medicine in Guo’s study and PAM+V in McCulloch’s study, compared with chemotherapy, are of the same order of magnitude (78% and 82%; Table 1; Figure 2). The somewhat worse prognosis in McCulloch’s chemotherapy-only patients compared with Guo’s patients could be either because of more effective chemotherapy in 2007-2009 than in 1988-1993 or a result of the fact that Guo studied adenocarcinomas only, whereas McCulloch studied all histological subtypes of NSCLCs.
Comparison of the 2 Recent Studies in Lung Cancer
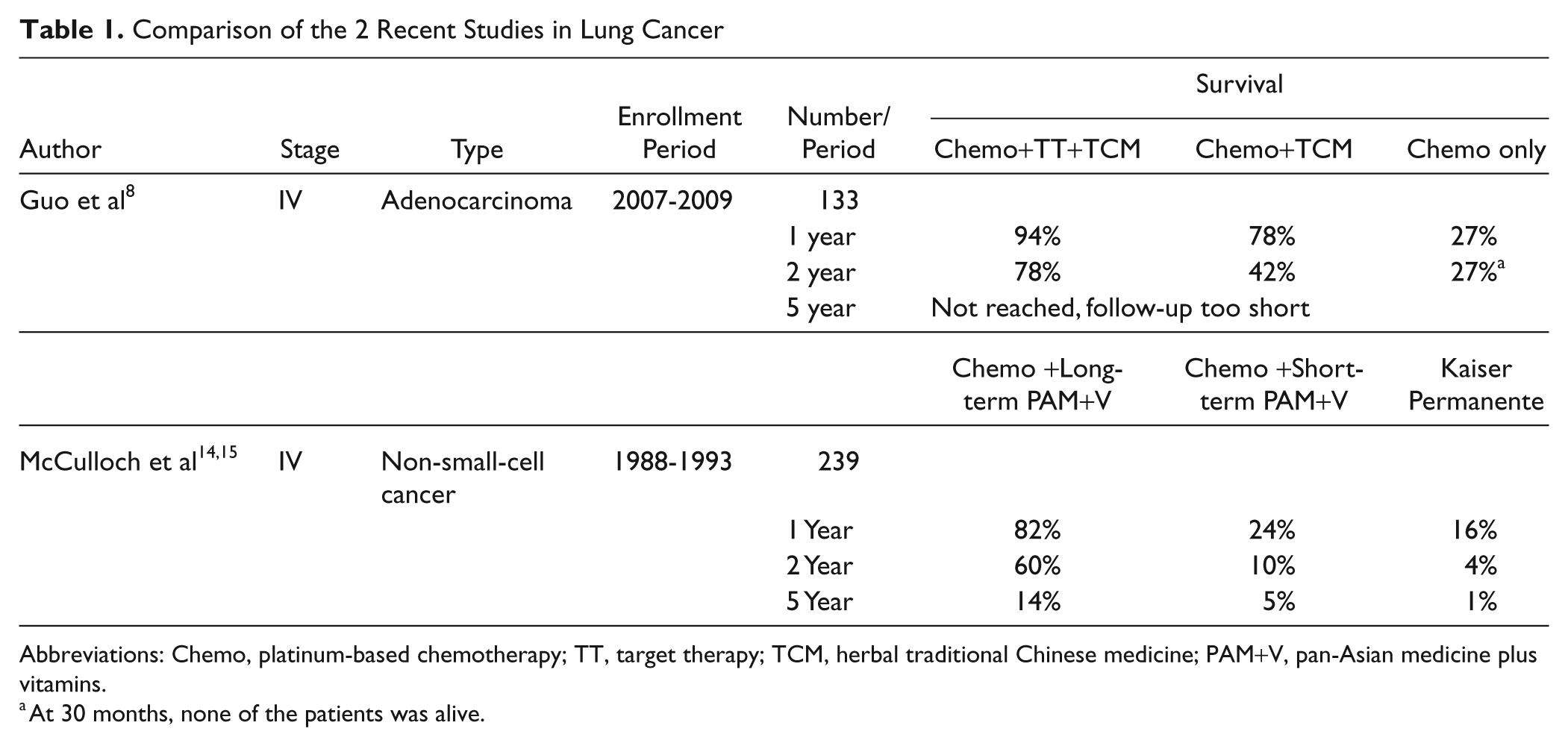
Abbreviations: Chemo, platinum-based chemotherapy; TT, target therapy; TCM, herbal traditional Chinese medicine; PAM+V, pan-Asian medicine plus vitamins.
At 30 months, none of the patients was alive.

The third study, on colon cancer patients (N = 193), was from the same center as the previous study. 15 PAM+V combined with conventional therapy reduced risk of death in all stages (stage I by 95%, stage II by 74%, stage III by 29%, and stage IV by 75%). There was no significant difference between short-term and long-term PAM+V.
Possible Therapeutic Mechanisms of TCM
What are the therapeutic mechanisms of TCM in metastatic cancer? The answer can be given from Chinese TCM and Western medicine points of view.
In China, TCM herbs are given on the basis of the TCM syndrome differentiation as diagnosed by the TCM herbal specialist. Patients with the same disease (ie, stage IV adenocarcinoma of the lung) may have different TCM syndromes. The TCM herbs are adjusted to the individual patient’s syndromes to improve the prognosis. The treatment principle widely used in China is strengthening of qi, yin, and yang and removal of internal heat. Details of how advanced lung cancer is treated in Shanghai can be found elsewhere. 8 McCulloch et al14,15 also discuss their different treatment aspects, but they do not discuss TCM syndrome differentiation. Most important in the consideration of the therapeutic working mechanisms of TCM herbs is that they are in principle the same as Western medicine drugs. However, rather than following single pathways, they follow multiple pathways and are multilayered and multitargeted.19,20
In Western medicine terms, the herbs may act by means of direct (antiproliferative, apoptosis-inducing) and indirect effects on the tumor (by reducing tumor-favoring neuroendocrine conditions and/or stimulating antitumor effects of the immune system).
When considering the possible cell-biological pathways through which medicinal herbs have an effect on cancer, it is interesting to note that there has been an increase, over the past decades, mostly of adenocarcinomas (breast, prostate, endometrium, and digestive tract cancers), and in China, many lung cancers today are also adenocarcinomas. Breast, endometrium, prostate, and other adenocarcinomas often carry steroid hormone (estrogen, progesterone, and testosterone) receptors. Moreover, many pulmonary adenocarcinoma patients are women, suggesting that here also, an endocrine relationship is important. 21 One NSCLC study suggested differential expression by sex and influence on survival in men of nuclear estrogen receptor (ER)-β in lung cancer, particularly in adenocarcinomas, 22 but others found that higher cytoplasmic ER-α expression correlated with worse recurrence-free survival.23,24
Yet another study found that neither ER-α nor ER-β alone were prognostic in NSCLC, whereas combined expression of ER-β and aromatase were, but only in women ≥65 years. However, the final subgroups in the latter study were rather small. 25 Analysis of tumor ERs and serum estrogen in NSCLC showed that patients with the highest tertile of serum estrogens had a worse survival (P combined < .001). Furthermore, in that study, increased tumor ER-α levels worsened survival. 24 Dual treatment with estradiol and progestin increased the numbers of putative tumor stem/ progenitor cells, 25 which is clearly a bad sign.
These somewhat conflicting results may be a result of the fact that different technologies are used (including tissue microarray or whole tumor sections and variable nonstandardized immunohistochemical methods), and there is a mixture of genders and also endocrine situations because of age differences, adenocarcinomas, and other histological subtypes of NSCLCs. Yet it seems that a hyperestrogenic endocrine environment and ER content of the cancer cells is important for lung cells to transform into malignant cells and stimulate further tumor progression.
But why would there be such an increase in pulmonary, colorectal, and breast adenocarcinomas since 1990 in China? It is tempting to consider that factors other than estrogens (E2), progesterone, androgens, and their receptors are also involved. Changes in lifestyle, which could be simplified as “more calories, less physical exercise” and that have become usual in the United States and other Western countries, are also becoming very “normal” in developing countries such as China and India. These diet and lifestyle factors lead to obesity, which is now officially regarded by the World Health Organization as a serious risk factor for cancer. Patients with diabetes have a higher risk of breast cancer. On the other hand, breast cancer patients who exercise more than 5 hours per week have an improved survival relative to sedentary patients. 26 Obesity is associated with higher estrogen levels, as noted by the prompt drop in serum estradiol following intentional weight loss. 27 Taken together, these data suggest that glucose, insulin, and insulin-like growth factors (IGFs) also may play a role in carcinogenesis and perhaps also the prognosis for adenocarcinoma patients. 28 Indeed, many body cells contain insulin and IGF receptors on their cell surfaces, which, through different molecular pathways, may cause hyperstimulation of cell growth.
It could be that the combined dual effects of steroid hormones and insulin/IGFs are strongly synergistic and stimulate cell proliferation of cancer cells with E2, progesterone, and perhaps also androgen receptors, on the one hand, and insulin and IGF receptors, on the other. As a result, genetically damaged cells with a malignant genotype will be overstimulated to grow quickly and hardly have time to phenotypically develop complicated proteins, such as MHC-1 antigens on their cell surface. MHC-1 is essential to attract and “anchor” CD8 cells, which can then kill tumor cells. It is interesting to note that a Japanese study found that a high expression of MHC-1 in lung cancers correlated with a dense infiltrate of CD8-positive tumor killer cells in the microenvironment of lung cancers. On the other hand, lack of MHC-1 expression was associated with a low level of CD8 infiltrates. Moreover, high MHC-1 expression and dense CD-8 infiltrates were strongly associated with a good prognosis, independent of stage. 29 In a totally different neoplastic lesion—cervical intraepithelial neoplasia grades 2 and 3 (CIN2-3)—dense CD8 infiltrates also correlated with prognosis, that is, spontaneous regression. Nonregressive CIN2-3 lesions were characterized by low numbers of CD8 immunoreactive cells but, on the other hand, had many CD138-positive plasma cells in their microenvironment. The latter can be interpreted as an ineffective chronic inflammation. CD25-positive T-reg cells also seem to play a role. 30
The above-mentioned facts have led us to the following hypothetical dualistic antiproliferation model and immune-stimulation model of tumor progression and regression, which could also be used to explain the possible effects of TCM herbal treatment in cancer patients (Figure 3). Tumor initiation occurs very frequently and is caused by a combination of genetic hits by carcinogenic factors. Many of these genetically damaged cells die. However, some survive, and tumor progression of these mutated cells is stimulated by hyperstimulation of E2, insulin, and IGF, among others. These neoplastic cells have an enormous growth advantage over normal cells, grow expansively, and invade the surrounding stroma. As a result, a small tumor develops, which can vary in size from 10 to 50 µm to less than 1 mm (1000 µm). Because of rapid proliferation, these cells hardly get time to mature and, therefore, will not make (enough) differentiation proteins. One of these proteins is MHC-1, which is normally expressed on the cell surface. It functions as an “anchorage” place for immune-reactive immune cells, such as CD-8, which can kill an abnormal cell when anchored through MHC-1. However, cancer cells that express MHC-1 very weakly positively, or not at all will not be attacked by CD-8 cells. An ineffective immune reaction will develop, characterized by CD138-positive plasma cells and many CD25-positive T-reg cells. This reduces the number of CD-8 cells. The result is a rapidly growing malignant tumor.

Simplified illustration of the events during carcinogenesis and how herbal treatment could interact with the hypothetical dualistic proliferation-stimulating model in cancer cells, and the effect of MHC-1 expression and CD-8 positive immunoreactive T-cell reaction against cancer cells
If this model is correct, the effects of herbal medicine, in addition to lifestyle interventions, could be antiproliferative by different mechanisms, among others by harmonizing (ie, normalizing exceedingly high or low values) serum levels of estrogens, progesterone, androgens, and other hormones of the neuroendocrine axis; insulin; and IGFs. This would slow down proliferation of the cancer cells. As a result, tumor cells would have more time to express MHC-1. The immune-system stimulating effect of the TCM herbs increases CD4 and CD8 numbers, and these T-helper and tumor-killing T-cells will not only stochastically infiltrate the tumor stromal microenvironment where the vessels are located, but now be goal oriented, chemoattracted by MHC-1-positive cancer cells.
The hypothetical dualistic antiproliferation model and immune-stimulation model of TCM herbal treatment in cancer patients could easily be tested in prospective studies. To avoid interlaboratory variation, it is important in such evaluations that standardized and carefully calibrated laboratory tests are used, preferably carried out in the same laboratory. Interestingly and in support of the hypothesis, the nonadenocarcinoma NSCLC subtype seems to benefit from the administration of figitumumab (CP-751,871), a fully human anti-IGF 1 receptor (IGF-1R) mAb. 31 Moreover, most actions of this insulin analogue have hitherto been explained by direct stimulation of the growth potential of neoplastic cells and by its IGF-1-related properties. Negative effects on the progression of adenocarcinomas by hyperinsulinemia and the insulin analogue glargine (A21Gly, B31Arg, B32Arg human insulin) have recently been suggested. Recent evidence showed that insulin-stimulated angiogenesis could be an additional factor involved in tumor progression and clinical outcomes associated with cancer. 32
Mechanistic therapeutic aspects of TCM herbs in cancer, which also require particular attention, are the antifatigue and antidepressive effects. Fatigue is well known during common, nonmalignant diseases such as influenza. However, when the virus is cleared, the extreme tiredness is suddenly “switched off.” Fatigue is common in autoimmune diseases such as primary Sjögren’s syndrome, in which the activated interleukin (IL-1) system is a possible biological factor associated with fatigue.33,34 Cytokines also may play a role in depression in cancer patients. In an excellent study in Integrative Cancer Therapies, Jehn et al 35 from Berlin, Germany, describe that depression occurs in approximately 25% of all cancer patients and provide strong evidence that the cytokine IL-6 and alteration of the hypothalamic–pituitary–adrenal (HPA) axis play a crucial role in the etiology of depression in cancer patients. IL-6 is produced not only by a variety of immune cells during inflammation but also by non–immune cells such as endothelial cells, endocrinal cells, and tumor cells.36,37 Its production can be stimulated by catecholamines and suppressed by glucocorticoids.38,39 Furthermore, IL-6 is a potent activator of the HPA axis, characterized by an increased production of cortisol and depressive mood.40,41 Depression in cancer is associated with increased plasma IL-6 concentrations and dysfunction of the HPA axis. It could be possible that the antifatigue and antidepressive effect of TCM herbs is related to their suppressing IL-1 and IL-6 and balancing the neuroendocrine immune system.
Again, this hypothesis can easily be tested, and if there is a proven effect of TCM or pan-Asian medication on such measurable patient characteristics, it would certainly help in the wider acceptance of complementary medicine modalities. The above discussion is just one example of how Western neuroendocrine and cell-biological thinking can be used to explain how TCM herbs may perhaps work. It should be possible and not too expensive to arrange a special international task force of collaborating health care providers who could conduct a prospective blood analysis of these factors in cancer patients before and during pan-Asian medicine/TCM/complementary and alternative medicine treatment and during or after conventional chemotherapy and correlate these with the QOL and survival. Systems biology can also be very useful in helping us further develop mechanistic explanations and test the effect of TCM herbal treatment. 42 Indeed, much more basic and applied clinical mechanistic research has to be done.
Other Explanations for the Improved Prognostic Effect of TCM Herbal Treatment
It has been argued that the improved prognosis of TCM-treated patients is merely a result of the better access that more educated, economically well-to-do patients have to such treatments and the consequent effect social differences have on these aspects. Better-off patients could simply afford to pay for eventual additional treatment and therefore have better access to top-quality conventional treatments (eg, target therapy) or perhaps live in a better social environment, with better palliative terminal care. In support of this hypothesis, it has recently been shown that early integrated palliative terminal care significantly influences the survival of terminally ill patients. 40 However, we have argued that socioeconomic or racial differences between our TCM and control groups can be regarded as excluded, 8 thereby strengthening the hypothesis that TCM herbal treatment is really effective in metastatic lung cancer.
Another explanation could be that TCM herbal treatment has no effect on the metastatic tumor cells at all but prolongs survival by improving the QOL (related to emotional functions, cognitive functions, nausea, and vomiting) or specific lung-cancer-related symptoms (coughing, phlegm, shortness of breath, and fatigue among others).43-46 This might in turn motivate patients in such a manner that their will to live is strengthened. The resulting better feeding status could perhaps also prolong survival.
A third possible explanation forwarded is that lag time to treatment, composed of patients’ delay in locating TCM doctors and doctors’ delay in seeing patients, could explain the better survival of chemotherapy+TCM-treated patients, compared with chemotherapy-only patients, as follows. With a median survival of 5 to 7 months, approximately one third of the patients will die within 3 months after the initial diagnosis: about 10% in the first month, 10% in the second month, and the rest in the third month (see also the survival curve of PBT-only patients in Guo et al 8 ). Take as an example a group of 100 patients with an overall 1-year survival of 30%, i.e., with 30 patients surviving for at least 1 year. Let us further suppose that a TCM doctor who treats the patients has a constant 3 months waiting time (doctor’s delay) between the first call of a patient and the first time the patient can be seen. This means that even if all the 100 patients make a first-time appointment with the TCM specialist at the time of their diagnosis, 30 of the 100 patients will already have passed away by the time of their first appointment. Consequently, only 70 patients are left. Of these 70 patients, 40 more will die before the end of the first year. The survival rate of these 70 patients therefore will be 30/70=43%, much better than the 30% survival of the original 100 patients. In any cancer population, there is a median survival curve that is potentially controlled in part by biological host factors—that is, some patients may be in better overall health or have better resistance to disease, whereas others may have comorbidities or be in a poor nutritional state. The latter patients are likely to be among the 30 who passed away before seeing the TCM physician. The population seeing the TCM physician will then be relatively enriched in patients who are in better overall health or who are more resistant to their disease. This population would naturally survive longer than the entire lung cancer population. Alternatively, let us suppose that TCM herbal treatment has no effect at all. Then one would still find that the overall survival of 30/70 = 43% to be much better than the 27% of the whole group. However, even with as little as 2 and 1 months’ delay by the TCM doctors (the last one probably is the only realistic one), the survivals would be 37.6% and 33.3%—relative “improvements” of 25% and 11%. We have shown elsewhere that this “lag time to treatment caused survival improvement” is much lower than the improvement in 1-year survival after chemotherapy+TCM treatment (nearly 80% absolute, a difference of absolute 50%, or relatively 167%). 48
Strong and Weak Points of the Studies
The 3 studies summarized in the section “Is TCM Treatment Effective,” all point to the same effect of herbal treatment, although the designs and many other factors differed in the studies. Yet the fact that the improvement in prognosis is so similar suggests that the common factor (herbal treatment) has an overriding strong prognostic effect. Although the overall herbal treatment differed between the Chinese and US studies, a number of the herbs used were the same. The lead time to treatment varied: roughly 1 month in the study by McCulloch et al14 and 3 months in the study by Guo et al. 8 Still, the results were very similar.
However, there are also weak points. Two of them were from the same research group (McCulloch et al14,15). The studies were not randomized before the studies started; they were retrospective (McCulloch et al) or prospective but case controlled (Guo et al 8 ). Also, the studies were not population based. Self-selection of patients to TCM clinics may have caused significant selection bias: Do the patients seeking herbal treatment have a healthier lifestyle, or do they have a socioeconomically better survival probability? Guo et al 8 argue in the discussion of their study that this is not likely the case in their patients, but final proof is not available.
One cannot therefore regard the studies as definitive. Rather, the results can be said to be suggestive and encouraging.
Steps to Be Taken to Get Reliable Unequivocal Results
Medical oncologists and herbal medicine specialists using integrative medicine techniques should spend more effort in the coming years to obtain undeniable proof that TCM treatment of metastatic, highly malignant cancers “really helps”—that is, it can be regarded as scientifically sound. It is therefore important to consider which phase 1, 2, and 3 trials should be undertaken.
First, there is the intriguing lack of prognostic effect of TCM syndrome differentiation in Guo’s study. Although this may be a result of issues with reproducibility, it is also possible that herbal treatment according to TCM syndrome effectively eliminates the possible negative prognostic effects of particular syndromes. In China, TCM syndromes certainly dictate the herbal combinations to be given to different patients, and trials should thus at least balance the distribution of TCM syndromes among groups or be restricted to a single TCM syndrome to equalize the herbal treatments to be applied. An initial study should assess the distribution of TCM syndromes in the potential study population and ensure reproducibility of syndrome differentiation among the study physicians responsible for TCM treatment.
Second, there is the problem of efficacy of individual herbs. As a chemical formula for the effective components is lacking for most herbs, one must rely on evidence of therapeutic effect of the herbs that comes through experience. However, it is exactly the experience of many TCM doctors that the same herbs may not be always equally effective. This may be a result of variation in the quality of the same herb produced by different manufacturers, and even when carefully controlled under Good Agricultural Practice of the same company, variability may be a result of seasonal or climatic variations of the herb’s effective component. It is therefore of the utmost importance that food and herb international preparation and testing guidelines be developed and strictly followed.
Third, formal phase 1 trials should assess the safety and potential for adverse herb-drug interactions of the herbal formulas to be used with conventional chemotherapy-treated patients as controls. Although this seems futile to Chinese TCM doctors who have long observed that the side effects of TCM herbal treatment are minimal, it is important to have formal validation for this in the Western world. Animal experiments are also of importance.
Fourth, a large, multicenter, prospective randomized, preferably population-based, trial should be undertaken in patients with advanced NSCLC, comparing standardized conventional PBT with PBT plus TCM herbal treatment. The stage, performance score, and gender and neuroendocrine, radiological, and immune status of the patients should be known before, during, and after treatment. Moreover, the radiology and pathology and preferably also EGF-R, steroid receptor status, and immune profile of the primary tumor should be known. A similar prospective trial that also includes targeted therapy should be performed. Regular controls of the above-mentioned neuroendocrinological and immune parameters and objective diagnosis criteria based on radiological and pathological data are mandatory. There should not be the slightest doubt about the initial inclusion criteria.
What Is to Be Done for NSCLC Patients Until Such Definitive Results Are Available?
An answer to the question of how to counsel NSCLC patients until such definitive results are available depends on different factors, which may vary from one country to the other. The following therefore cannot be anything other than widely useful considerations for discussions with patients; they are definitely not absolute guidelines.
There are the legal aspects related to doctors giving TCM integrative therapy. It is well known that many patients with metastatic cancer use over- the-counter herbs, vitamins, and food supplements, irrespective of what their treating doctor says.
Discuss the bottom-up reality where desperate patients will do anything to prolong survival and improve QOL.
Also mention the effect of early palliative care. 47
Recognize the role of integrative therapy and psychological effects. Health care providers should “care” and not only emphasize the conventional “cure.”
Discuss with patients that chromosomes are not our fate but that diet, lifestyle, and psyche can change gene expression.
Depending on the patient, discuss the possibilities of placebo and nocebo effect and that both may have an effect on the QOL.
Although the data in this area are not yet sufficient to provide guidelines for patient counseling, the studies we review provide encouragement to further investigate the role of TCM integrative therapy. Many of the aspects of clinical trial design regarding such investigations are clear from prior work, and we hope that progress will be made toward relevant trials in the near future.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.