
Abstract
Hypotheses. Men who have a brother with prostate cancer have a 2-fold increased risk of being diagnosed with prostate cancer. Strategies employed by these men to reduce prostate cancer risk are not well understood. Preliminary studies have shown that men with a family history of prostate cancer have a high rate of vitamin and supplement usage aimed at the prevention of prostate cancer. Study design. The authors analyzed data from a cross-sectional study of men with familial and hereditary prostate cancer and their unaffected brothers. A total of 542 unaffected men who had at least one brother who had been diagnosed with prostate cancer regarding their use of vitamins and supplements, as well as the motivation for use, were interviewed. Methods. The associations between subject characteristics and vitamin and supplement use were evaluated using an unconditional logistic regression modeling approach. Results. Overall, 59.2% and 36.5% of men reported ever using and currently using, respectively, one or more vitamins or supplements (including multivitamins). One third of men took a vitamin or supplement that has been targeted for prostate health or cancer prevention, including green tea, magnesium, male hormones, saw palmetto, selenium, soy, vitamins A, C, E, and zinc. Increasing age at time of survey was associated with vitamin/supplement use (odds ratio [OR] = 1.03; 95% confidence interval [CI] = 1.01-1.05). After adjusting for age at time of survey, being younger than an affected brother was associated with vitamin and supplement use (OR = 1.51; 95% CI = 1.01-2.25). A total of 25% of men reported obtaining information from books or articles as the most common source of information. Conclusions. The findings indicate that men at an increased risk for prostate cancer report a high rate of vitamin and supplement use, including supplements targeted for prostate cancer prevention. Men with a family history of prostate cancer represent a target population for future chemopreventative agents.
Keywords
Introduction
Prostate cancer is the most common noncutaneous malignancy diagnosed among men in the United States. In addition to older age and African American race, a positive family history is a strong recognized risk factor for this disease. Men with one first-degree relative diagnosed with prostate cancer have an approximate 50% increase in risk of developing prostate cancer; however, when this relative is a brother, the relative risk increases 2-fold compared with men with no family history of disease. 1 There are no existing preventative guidelines for men with a family history of prostate cancer, and the strategies employed by these men to reduce prostate cancer risk have not been well studied.
Much media attention has been devoted to promoting vitamins, supplements, and herbs that may reduce risk of prostate cancer. However, many of the assertions have not been consistently shown across studies. The Nutritional Prevention of Cancer study, a randomized trial of selenium supplementation begun in 1996, found that selenium significantly reduced the incidence of prostate cancer. 2 Similarly, the Alpha-Tocopherol, Beta-Carotene Cancer Prevention study, a randomized controlled trial among male smokers, supported the role of vitamin E in the reduction of both prostate cancer incidence and mortality. 3 However, recent results from the Selenium and Vitamin E Cancer Prevention Trial (SELECT), a randomized, placebo-controlled trial, showed that selenium and vitamin E, either alone or in combination, were not associated with statistically significant differences in prostate cancer incidence. 4 Despite an observed alleviation of symptoms among men with benign prostatic hyperplasia, saw palmetto supplementation was not found to be associated with prostate cancer risk in a cohort study of 35 171 men. 5
The use of vitamins and supplements has increased dramatically over recent decades, with consumers expecting improvements in health, disease prevention, and reduced risk of mortality. 6 About 40% of the US general population takes some form of vitamin or supplement, with multivitamins being the most commonly used.7,8 Although clinical deficiency of vitamins or minerals, other than iron, is uncommon in the United States, annual sales of supplements to Americans are reported at about $23 billion. 9
In this study, we describe the use of vitamins and supplements in a cohort of men at increased risk of prostate cancer based on their family history of the disease and analyze correlates of use, as well as motivating factors leading to vitamin and supplement use in these men. Understanding the prevalence and patterns of usage of agents aimed at reducing prostate cancer risk elucidates the degree of concern among men at high risk for developing the disease, as well as the potential for testing and use of future chemopreventative agents. This study was conducted between 2002 and 2008, during which time the evidence supporting the role of vitamins and supplements in prostate cancer prevention was in flux.
Materials and Methods
The subjects were all participants in the University of Michigan Prostate Cancer Genetics Project (PCGP), a large-family-based cohort study of inherited forms of prostate cancer. The PCGP enrollment criteria include families with two or more living family members in a first-degree or second-degree relationship diagnosed with prostate cancer or men diagnosed at or younger than 55 years with no family history of prostate cancer. A complete family history of cancer of any type in first-, second-, and third-degree relatives was obtained from all participants. Reported prostate cancer cases were confirmed by medical record review if possible, otherwise independent confirmation of diagnosis by two or more relatives was used.
The minimal criterion for inclusion into the present investigation was one first-degree relative (brother) with prostate cancer. After enrollment, the affected men (probands) were asked to contact an unaffected brother to invite them to participate. The University of Michigan Medical School Institutional Review Board reviewed and approved all protocols. All participants consented to complete a computer-assisted telephone survey using BioDBx software, version 4.0 (Ann Arbor, Michigan, Regents of the University of Michigan, 2002). Participants were asked as part of the survey to self-report use and duration of use of different medications, vitamins, and supplements among unaffected brothers. Participants were asked to provide information on demographic and behavioral characteristics (age, education, marital status, household income, occupation, and smoking history). Information on race and proband age was obtained from the proband.
Participants were asked a series of questions regarding their use of vitamins, herbal supplements, and prescription medications, including those substances implicated in published reports or marketed for the prostate health or prostate cancer prevention. Vitamins and supplements were selected if they were widely used (i.e. vitamin A, B, or D) or had been implicated in improving prostate health or prostate cancer prevention based on a review of published studies. Subjects were asked to recall if they had ever used each vitamin or supplement for at least 3 consecutive months and whether they were currently taking any vitamin or supplement, including those not specifically mentioned by the interviewers. Data were collected as to the source of information for each vitamin or supplement. Interviewers also collected data regarding current use of all prescription medications, particularly the use of finasteride.
The data analysis was performed using the Statistical Analysis Systems software, version 9.1.3 (SAS Institute, Cary, NC). Prevalence measures were calculated for each demographic variable, smoking history and use of vitamins and supplements. Crude associations between the demographic/behavioral variables and the current use of any vitamin or supplement, use excluding multivitamins, and use of prostate-specific vitamins or supplements were evaluated using χ2 tests and multivariable analysis was accomplished using an unconditional logistic regression modeling approach. Age was analyzed as a continuous covariate, and all other variables were dichotomized; for responses related to household income and education, the dichotomization was based on the median value. The final multivariable models included age at time of survey, the only variable that was statistically significant (P ≤ .05) in the univariate analyses. Variables were excluded in a backward stepwise fashion, leaving only those significant at a P value of .05 or less.
Results
We analyzed survey data from 542 men without prostate cancer and with a positive family history for the disease, 290 (53.5%) of these men had at least 2 affected first-degree relatives (Table 1). In our study, most men were married (84.0%), had more than 16 years of education (51.7%) and were current or past smokers (53.5%). The median age of our participants was 56 years (range 33 to 88 years) with 64% of men being older at the time of survey as compared with the age that their affected brother was diagnosed with prostate cancer.
Characteristics of Unaffected Brothers of Men With Prostate Cancer Enrolled in the Prostate Cancer Genetics Project (n = 542)

Overall, 71.2% of men in our study had ever used and 59.2% of men were currently using a vitamin or supplement at the time of survey (Table 2). The prevalence of ever use and current use of multivitamins was 50% and 36.5%, respectively. Approximately one third of men were, at the time of survey, currently using a vitamin or supplement marketed as a cancer chemopreventative or for prostate cancer prevention (green tea, magnesium, saw palmetto, selenium, soy, vitamins A, C, and E, and zinc) as well as the medication, finasteride. Vitamins C and E were both being currently used by about 17% of men, whereas selenium was used by 5.5% of men. The prevalence of finasteride usage was less than 2%.
Use of Vitamins and Supplements Among Unaffected Brothers of Men With Prostate Cancer (n = 542)
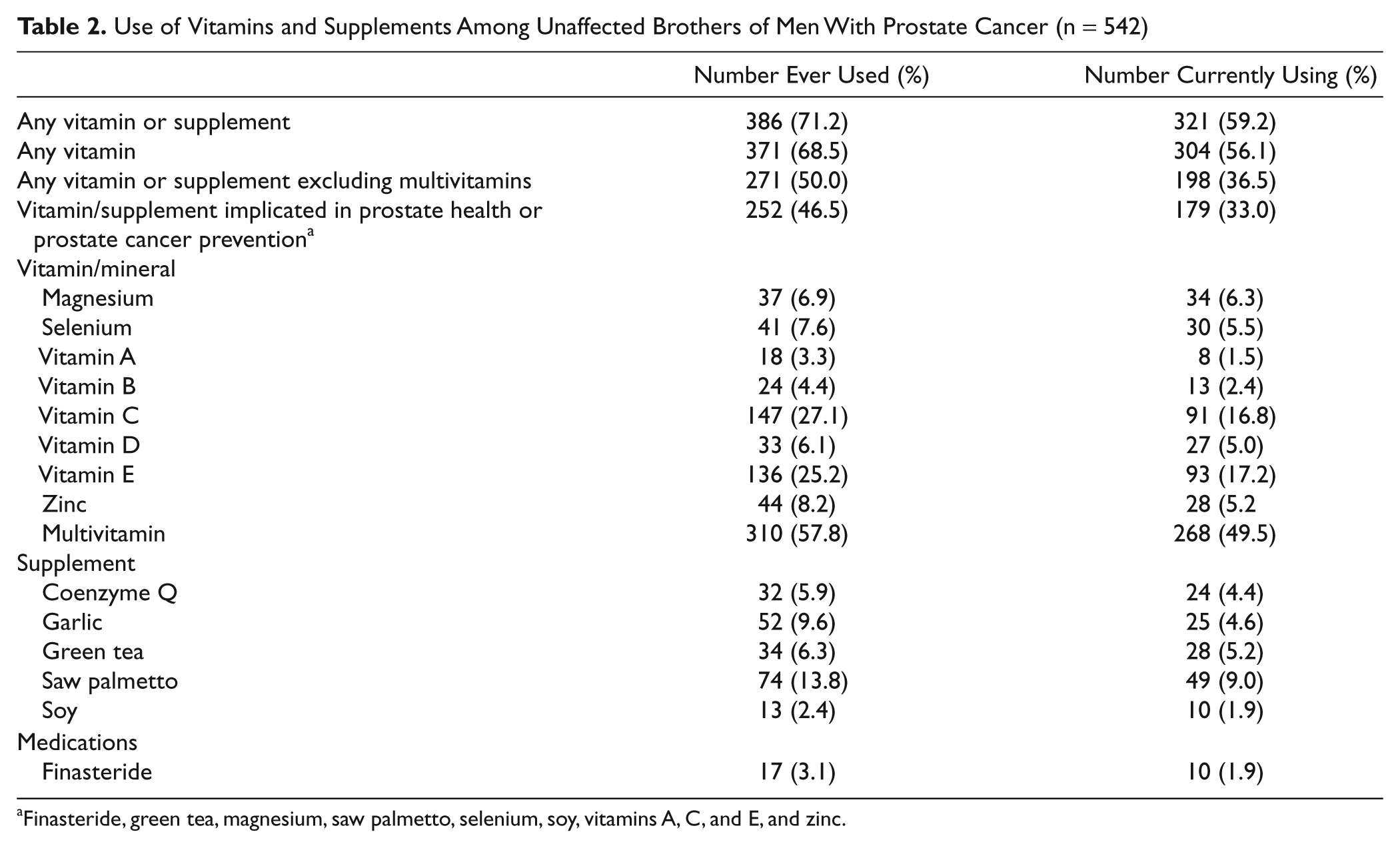
Finasteride, green tea, magnesium, saw palmetto, selenium, soy, vitamins A, C, and E, and zinc.
Our study found that increasing age at the time of survey was significantly associated both with use of all types of vitamins and supplements (odds ratio [OR] = 1.03; 95% confidence interval [CI] = 1.01-1.05) and with vitamins and supplements, excluding multivitamins (OR = 1.04; 95% CI = 1.02-1.06; Table 3). Furthermore, in age-adjusted models, being younger than an affected brother was significantly associated with vitamin or supplement usage excluding multivitamins (OR = 1.61; 95% CI = 1.09-2.69) and with usage of prostate-related vitamins and supplements (OR = 1.51; 95% CI = 1.01-2.25). Use of vitamins and supplements and prostate-related vitamins and supplements was also associated with an increase in the number of first-degree relatives who were affected with prostate cancer, being married, higher educational attainment (>16 years vs <16 years), and higher household income (≥$75 000 vs <$75 000); however, these associations were not statistically significant.
Association of VS Use With Characteristics Among Unaffected Brothers of Men With Prostate Cancer (n = 542) a

Abbreviations: VS, vitamin and supplement; OR, odds ratio; CI, confidence interval; MV, multivitamin; ref, reference.
Models are adjusted for age at time of survey.
Younger or Older as compared to affected brother.
In addition to the high rates of single vitamin and supplement usage, we also observed evidence of multiple supplement usage among men who are current users or ever users of vitamins and supplements. In all, 61.9% and 52.6% of ever and current vitamin and supplement users, respectively, reported use of at least 2 vitamins or supplements (Table 4). Overall, 35.7% of ever vitamin/supplement users and 29.9% of current vitamin/supplement users reported using 3 or more vitamins and supplements. The median usage among both ever and current users was 2 vitamins and supplements.
Multiple Vitamin and Supplement Use Among Unaffected Brothers of Men With Prostate Cancer

Beginning in 2006, a subset of study participants were queried as to their reasons for taking vitamins and supplements (n = 135), 93.3% identified general health concerns and 14.1% identified prostate health concerns as their motivation for use. A subset of study participants (n = 290) were also asked to provide information as to their sources of information on vitamin and supplement use. Of these men, 22.8% cited family members, 23.8% cited a book or article, 15% cited a physician other than their urologist, 14.5% cited the Internet or news report, whereas only 3.5% cited their urologist as a source of information on the use of vitamins or supplements for cancer prevention.
Discussion
Our results demonstrate that nearly 60% of men at high-risk for developing prostate cancer based on their family history are currently using a vitamin or supplement. Approximately one third of men are currently using a vitamin or supplement implicated in the prevention of prostate cancer/promotion of prostate health, with the majority of men using multiple vitamins or supplements. Other than multivitamins, vitamin C, vitamin E, and saw palmetto were among the most used vitamins and supplements. Vitamin and supplement use was significantly associated with increasing age and younger birth order (as compared with an affected brother).
Although the purpose of this analysis was to assess correlates of vitamin and supplement use in this cohort, the high prevalence of use provides insight into the motivations and information-seeking behavior among this cohort of men. The prevalence of current vitamin or supplement usage in our study is similar to the prevalence among 50- to 71-year-old males in the National Institutes of Health–AARP Diet and Health Study. 10 Among healthy male physicians, the prevalence of supplement use was 29%. 11 Our results were also consistent with a recent survey, which found that 50% of men at high risk for prostate cancer (defined as African American ethnicity, positive family history, or positive BRCA1 gene mutation) took one or more supplements to prevent prostate cancer, and more than 25% took 3 or more agents concomitantly. 12 The prevalence of vitamin and supplement use in our study was similar or higher than other highly educated populations and groups at high risk for developing cancer.10,11,13 We acknowledge that the high education and income levels observed among our study population may contribute to the particularly high prevalence of vitamin and supplement use in our study.
Despite conflicting published evidence on the relationships between vitamin and supplement use and prostate cancer incidence, evidence suggests that more research in this area may be warranted. In a randomized double-blind placebo-controlled trial of men with a history of prostate cancer, a soy-based dietary supplement was shown to delay prostate-specific antigen (PSA) progression after potentially curative treatment. 14 Another randomized double-blind placebo-controlled trial in men with untreated prostate cancer who had rising PSA levels found that a dietary supplement (verum, administered for 6 weeks) containing plant estrogens, antioxidants, including carotenoids, selenium, among other substances resulted in decreased free PSA values and reduced testosterone levels as compared with the placebo group. 15 Although these randomized trials included men already diagnosed with prostate cancer, such results highlight that the association between vitamin and supplement use and prostate cancer risk require further study. Well-designed studies with clear clinical end points, sufficient power, and placebo controls may elucidate some of the inconsistencies seen among observational and small randomized trials. Almost 100 studies involving prostate cancer and some form of dietary supplementation are ongoing and registered with clinicaltrials.gov; 70 of these studies are randomized trials. 16 The ongoing research interest in identifying vitamins and supplements which may reduce the risk of incident or recurrent prostate cancer is consistent with the strong motivation among men at high risk of developing prostate cancer to pursue risk reduction strategies.
Finasteride and dutasteride are the only chemopreventive agents which have been shown to decrease the risk of prostate cancer.17-19 The low prevalence of finasteride use found in our study (2%) may indicate that men are not discussing chemopreventative strategies with their physicians or that men at risk for prostate cancer are more likely to take vitamins and supplements and not as willing to take prescription medications. Our results indicate that men are seeking information on vitamin and supplement use and obtaining information from sources other than their physicians. In a recent study, men with prostate cancer identified their physicians as the most common source of information about vitamins and complementary medicines, with twice as many patients identifying physicians as being advocates rather than critics of vitamin, supplement, and herbal medicine usage. 20 However, nondisclosure of vitamin and supplement usage to medical providers is common among patients being treated for cancer. 21 Physicians should address risk reduction strategies with patients at increased risk of prostate cancer, including those with a family history of prostate cancer.
Among the strengths of this study is a unique cohort of unaffected men with a strong family history of prostate cancer. Participants have been recruited consistently since 2002 providing an opportunity to investigate temporal differences in vitamin and supplement usage. The results presented here are comparable to the results published in 2004 using pilot data (n = 113) from the same cohort. 22 The potential limitations include external validity as the men in our study may not be representative of the overall population of men with a family history of prostate cancer. Men who agreed to participate in a study may be more willing to employ methods aimed at prostate cancer risk reduction and more aware of their risk of prostate cancer resulting from participation in a genetic study. Similarly, our assertion that men with a family history of prostate cancer may be more likely than the general population of men at risk for prostate cancer to use vitamins and supplements cannot be concluded in the absence of a comparison group. A limitation of the current study is the lack of data from a control group of men without a family history of prostate cancer or cancer, in general. However, comparison of our findings with the general population indicates that usage of vitamins and supplements is higher among our participants as compared to the general adult U.S. population. Furthermore, about 50% of men in our study had completed at least 16 years of education and had a household income of at least $75 000, indicating that these men are not representative of all men in the population at risk for developing prostate cancer. However, our findings were consistent with another study of unaffected men with a family history of prostate cancer that found that up to 55% of men were using some form of complementary therapy. 23 The internal validity of this study should also be considered; however, previous findings from this cohort reported that once a brother facilitated contact with their unaffected sibling, the response rate among unaffected men was high (90%). 22 Another limitation of this study is that the vitamin and supplement use data was self-reported, which may have resulted in misclassification. However, the degree of misclassification would likely not vary depending on any of our tested correlates, therefore, any error in the recall of information would tend to bias our results toward the null.
Men with an increased risk of prostate cancer due to family history of the disease report a high rate of vitamin or supplement usage and represent an excellent population in which future prostate cancer chemopreventative agents may be tested. Given the few strong established risk factors for prostate cancer, focusing chemopreventative strategies on these men known to be at increased risk presents the ideal opportunity to study agents that may reduce prostate cancer risk. Furthermore, the high rates of usage among our study population reinforces the continued interest in designing trials to study the effects of dietary interventions, supplement use and alternative therapies and helps to identify a target population that not only stands to benefit from an effective chemopreventative agent, but is also motivated to participate in and adhere to such interventions. These findings also highlight the potential challenges of designing studies among these men given their high baseline rate of vitamin and supplement usage. The high rate of vitamin and supplement usage by men with a family history of prostate cancer may indicate that these men are concerned about prostate cancer prevention and are willing to alter their behavior in order to decrease their risk of prostate cancer. Although these men may not be representative of the general population of men given their increased risk of prostate cancer, the shared increased risk among this homogeneous group of men may provide a platform to assess the association between vitamin and supplement use and prostate cancer. Furthermore, the predicted increased number of prostate cancer diagnoses among men with a family history of the disease may allow for more accurate measures of association. Physicians should recognize the interest in strategies to reduce prostate cancer risk among these men and discuss evidence-based information as to the benefits of vitamins and supplements, as well as prescription medications, such as finasteride and dutasteride.
Conclusions
Despite conflicting findings as to the prostate cancer risk reduction properties of vitamins and supplements, men at an increased risk for the development of prostate cancer report high vitamin and supplement usage and are highly motivated to use agents aimed at reducing disease risk. Designing studies in this high-risk population may also be complicated by their high rate of long-term usage of vitamins and supplements and may lead to over or underestimates of effect of vitamins and supplements in an intervention study. However, studying men with a family history of prostate cancer may offer an ideal cohort to assess the potential for risk modification resulting from vitamin or supplement use. Physicians should discuss the benefits and risks associated with chemopreventative agents, particularly finasteride, with men with a family history of prostate cancer. There remains a need to provide high-quality evidence as to how men can reduce prostate cancer risk using chemopreventative and dietary strategies and men with a family history of prostate cancer represent an ideal population for testing future risk reducing agents.
Footnotes
Christina M. Bauer and Miriam B. Ishak contributed equally to this work.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This work was supported by S.P.O.R.E. in Prostate Cancer P50 CA69568 and by the University of Michigan Comprehensive Cancer Center.