
Abstract
Aims. This study aimed to give an up-to-date description of the views and knowledge that health professionals in New Zealand (NZ) have about complementary and alternative medicine (CAM) and its use in the context of integrative medicine. Study design. A self-administered questionnaire. Methods. Doctors in the Otago region of New Zealand (n = 235 out of 395, 59% response rate) answered questions addressing attitudes toward the principle of integrative medicine, attitudes indigenous Ma-ori holistic views of health, and attitudes about CAM. Information on physician demographics was also gathered. Results. Almost all doctors (95%) agreed that they should address all aspects of a patient’s health, whereas around 60% agreed that CAM can be integrated into a treatment regime to provide the best care for a patient. Most (93%) agreed that in a NZ context, it is important to be aware of Ma-ori holistic views of health. Doctors had many concerns about CAM, and only 26% personally used any CAM therapies themselves. However, many doctors wanted to learn more about CAM (58%) and Ma-ori holistic views of health (62%). Doctors who believed that they “knew enough” about CAM were more likely to ask about it and to recommend it to patients. Conclusion. Integrative medicine is increasingly being accepted in medical practice, although many doctors still do not agree with the use of CAM. There is a need for increased patient–doctor discussions of CAM use. Doctors’ lack of knowledge about CAM may be a barrier to communication and should be addressed with specific medical training.
Keywords
Integrative medicine involves a healing-oriented approach that takes account of the whole person—body, mind, and spirit—as well as all aspects of lifestyle.1,2 It makes use of all available therapies, including conventional medicine and those regarded as complementary or alternative. In NZ, integrative medicine also includes indigenous Māori health models such as Te Wheke, Ngā Pou Mana, and Te Whare Tapa Whā. 3 These views of health are based on a holistic approach, where the different aspects of health combine to provide total well-being. The term complementary and alternative medicine (CAM) encompasses any healing practice that does not fall within the area of conventional Western biomedicine and includes practices that are used concurrently with conventional treatments (complementary therapies) and those that are used instead of conventional treatments (alternative therapies).
Use of CAM is widespread, with 38% of the people presenting at a NZ emergency department reporting CAM use, 4 and in the United States, estimates of the prevalence of use showed an increase from around 35% in 20025,6 to 38.3% in 2007, 7 with use in some groups being even higher: 50.8% for some indigenous peoples 7 and 67% for female collegiate athletes. 8 Elsewhere, a sample in Saudi Arabia reported 68% CAM use. 9 Greater use of CAM is typically associated with being female, more educated, having a higher income, and a poorer health status.6,7 A NZ study 10 indicated that many (95%) general practitioners (GPs) have referred patients to CAM therapies, principally acupuncture, chiropractic manipulation, and osteopathy. However, although attitudes toward CAM may be positive, knowledge about specific therapies may be more limited. 11
Use of CAM may be even greater among people with cancer than in the general population, 12 although the prevalence depends on the definition of CAM used as well as the population surveyed. 13 One NZ study found that 49% of cancer patients questioned had used some form of CAM. 14 Other studies also report high rates of use of CAM therapies, from 78% in a sample of American women at high risk of breast and ovarian cancer 15 to 97% of Chinese women with breast cancer, 12 and 98% of people receiving outpatient chemotherapy in Taiwan. 16 Cancer patients also tend to have positive attitudes toward CAM therapies.17-20 Self-reported reasons for patients using CAM included wanting to be hopeful, believing that CAM is nontoxic, and desiring to feel more in control of their treatment. 21
However, many people who use CAM do not discuss this use with their doctors. At least 40% of American cancer patients did not disclose their use of CAM to their doctors. 21 A study in Finland showed that although half of the breast and prostate cancer patients interviewed believed that CAM therapies could be beneficial, only one quarter had spoken with their doctor about these practices. 22 In a Taiwanese sample of patients receiving outpatient oncology care, 66% did not tell their doctors that they were using CAM. 16 This lack of disclosure is of concern, especially because some CAM therapies may interact with conventional medicine or cause side effects.23,24
Against this background, the current study was carried out to investigate among a sample of NZ doctors their attitudes toward and knowledge about CAM as a part of integrative medicine, whether they discussed CAM with their patients, and what roles they saw for CAM use.
Methods
Participants
We aimed to invite all doctors in the Otago region of NZ to participate in the study. Doctors in NZ are based either in a hospital (as specialists) or in the community (as GPs). Lists of all GPs in the Otago area (n = 221) and of specialists on staff in the Dunedin Public Hospital (n = 173, including 8 specialist oncologists) were obtained. Dunedin Public Hospital is the main public hospital for the Otago catchment area. Overall, invitations to participate and questionnaires were sent to 395 doctors. Most oncology patients in the Otago region (>90%) are seen at Dunedin Hospital at some stage (with private oncology being a minor part of oncology practice in Otago), and virtually all oncology patients attend their GP as well. There are approximately 1200 new cancer diagnoses in Otago per annum at an average of 5.4 new cases per GP per annum.
Survey Instrument
The questionnaire was adapted, with permission, from that used by Lee. 25 Demographic questions obtained measures of gender, age, ethnicity, place of medical training, years spent practicing medicine, and present type of practice (hospital or community). Questions regarding beliefs about integrative medicine and CAM were in the form of statements, with which participants were asked to indicate how much they either agreed or disagreed. The response categories used were mostly of a modified Likert-type scale (strongly agree, agree, disagree, strongly disagree). Other questions asked for estimates of the proportion of the doctor’s patients characterized by each statement and what role(s) the respondents perceived for CAM. The questions are shown in Tables 1 and 2. An information sheet was also provided with each survey (see Appendix).
Numbers (and Percentages) of Doctors Who “Agreed” or “Strongly Agreed” With Statements About Integrative Medicine and Adjusted ORs (and 95% CIs) by Demographic Characteristics a

Abbreviations: OR, odds ratio; CI, confidence interval; NZ, New Zealand; CAM, complementary and alternative medicine.
Not all respondents answered every question; percentages are given as a proportion of valid responses (range 215-234). ORs are adjusted for age, sex, where trained, length, and type of practice. Statistically significant differences are shown in bold. Percentages are out of all valid responses and may not add up to 100 as a result of rounding
Doctors’ Reports of the Numbers (and Percentages) of Patients With Whom They Discussed CAM

Abbreviation: CAM, complementary and alternative medicine.
Procedure
Ethical approval for this study was given by the Lower South Regional Ethics Committee. A questionnaire and information sheet was sent via the Dunedin Public Hospital internal mail system to all potential participants, along with a personalized letter inviting participation and an addressed freepost envelope for returning the completed questionnaire. Reply envelopes were numbered to facilitate further follow-up of those from whom replies were not received. Questionnaire completion was taken as consent to participate. After 3 weeks, a second questionnaire was sent to all potential participants who had not yet replied.
Statistical Analysis
Answers to questions were quantified using a simple coding system, entered into an Excel spreadsheet, and analyzed using SPSS for Windows v16.0. Answers based on the modified Likert scales were collapsed into dichotomous categories of agree and disagree and percentages calculated for each. We tested whether agreement with statements was related to sex (male vs female), age (up to 50 years vs 51 years or more), place of medical training (NZ vs elsewhere), length of practice (up to 20 years vs 21 years or more), or type of practice (community, ie GP, vs hospital), using simple binomial regression for crude odds ratios (ORs) and multiple binomial regression for ORs adjusted for all other variables. Reported frequencies of behaviors relating to CAM were also collapsed into dichotomous categories. We tested whether behavior frequency was related to demographic factors using χ2 comparisons for crude associations and binomial logistic regression for adjusted associations. Model selection procedures were used to look at the relationships between behaviors and attitudes regarding CAM. Comments made as to the role of CAM were grouped into categories to determine the most common answers. Results were deemed statistically significant when P < .05.
Results
Of the 395 doctors contacted, 235 completed the questionnaire, producing a response rate of 59%. Respondent characteristics are summarized in Table 3.
Demographic Characteristics of Participating Doctors (n = 235) a
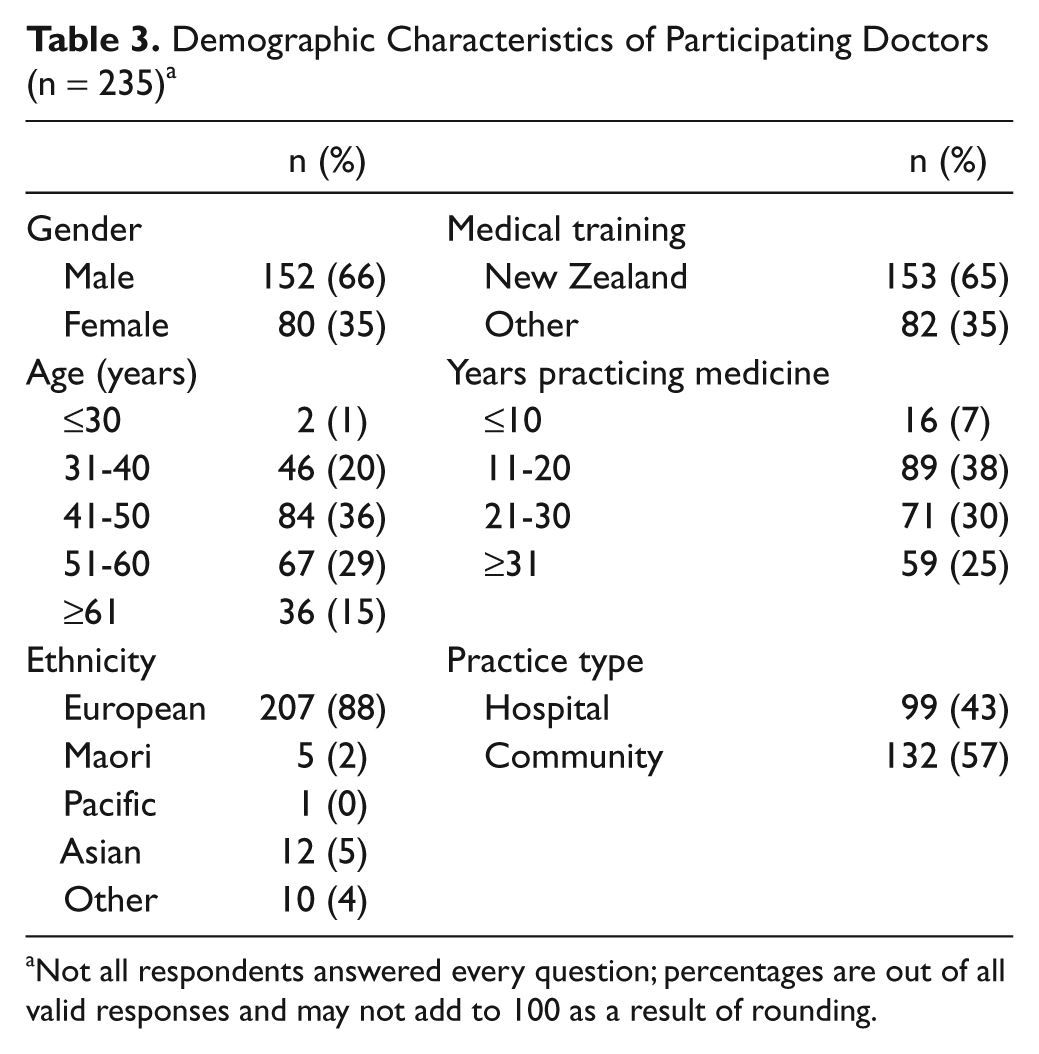
Not all respondents answered every question; percentages are out of all valid responses and may not add to 100 as a result of rounding.
We looked at the relationship of discussions regarding CAM with gender, age, type and length of practice, and location of training using χ2 comparisons to test for crude associations and binomial logistic regression to test for associations adjusted for other terms in the model. For these analyses, responses to questions regarding behavior were collapsed into 2 categories (those asking less than 25% vs more than 26% of patients, estimating that less than 25% vs more than 26% of patients use CAM, and recommending CAM to no patient in the past month vs to 1% or more of patients; see Table 4).
Attitudes Toward CAM
The percentages of positive responses to the questions about attitudes to CAM are shown in the first column of Table 1. Almost all doctors (95%) agreed that the health of a patient’s body, mind, spirit, and lifestyle should all be addressed by doctors, indicating that most people acknowledge the theory of integrative medicine, though only 60% agreed with the idea that complementary and alternative therapies should be integrated into the treatment regime to provide the best patient care and support.
Around half (54%) of doctors were concerned about the reasons why their patients may choose to use CAM, but many more were concerned about how CAM may affect conventional treatment; 89% were concerned about interference with other medications, and 87% were concerned about side effects. A high percentage (86%) was also concerned about the lack of scientific knowledge about CAM therapies, and 84% of doctors were concerned about the cost of CAM therapies. Only 22% of doctors wanted to use more CAM in their practice, and only 26% used CAM themselves.
Knowledge About CAM
Many doctors (58%) wanted to learn more about CAM therapies. A mere 14% thought that they were prepared for CAM integration during their medical training, and only 27% agreed that they had sufficient knowledge to advise patients on CAM use; 93% agreed that in NZ it is important to be aware of Māori holistic views of health, and 62% wanted to learn more about the Māori holistic views of health.
Relationships of Demographic Variables With Attitudes and Knowledge of CAM
We used multiple regression to look at the effects of demographic influences on the attitudes expressed by doctors. The adjusted ORs (Table 1, columns 2-5) show how the odds of agreeing with each statement were related to gender, place of training, time in practice, and type of practice when controlling for all the other terms in the model. (Note: we also calculated crude ORs. In most cases, these corresponded with the adjusted ORs, so only the adjusted ORs are shown. The single exception was the crude finding that younger doctors were more likely than older doctors to acknowledge the principle of integrating CAM, which was significant in simple regression but became nonsignificant when other factors were controlled for). None of the adjusted relationships with age were significant, so these are not discussed further or shown in the table.
Gender
Women were more likely to agree with the principles of holistic health and integration of CAM. Compared with men, women were more likely to agree with using CAM for incurable diseases, to want to use more CAM with their patients, and to want to learn more about CAM.
Training
Doctors trained in NZ were more likely to agree that doctors should address the patient’s body, mind, and spirit and were more willing to accept the integration of CAM for a curable disease. Doctors who trained in a country other than NZ were more likely to want to learn more about the Māori holistic views of health.
Length of practice
Doctors who had been practicing for more than 21 years were less likely to agree that CAM should be integrated into patients’ care.
Location of practice
Doctors who practice in the community were more likely to agree that CAM should be integrated to provide the best patient care. Community-based doctors were also more concerned about the cost of CAM therapies and less likely to believe that they were prepared for CAM integration during medical training.
Discussions About CAM
The percentages of patients with whom doctors discussed CAM are presented in Table 2. More than half of the doctors (n=135, 57%) said that they ask less than a quarter of patients about the use of CAM therapies. Only 39% of doctors believed that more than a quarter of their patients were using CAM. The majority of doctors did not recommend CAM widely: 93% of doctors recommended CAM to less than a quarter of their patients, and 42% did not recommend CAM to any patient at all.
Gender
χ2 Compared with their male colleagues, female doctors were more likely to ask more patients about CAM (59% to 34%; χ2[1, n = 232] = 12.9; P < .01), report that more of their patients used CAM (55% to 32%; χ2[1, n = 201] = 9.6; P < .01), and recommend CAM to any of their patients (78% to 48%; χ2[1, n = 228] = 18.6; P < .01). These differences remained significant after adjusting for all other terms in the model (see Table 4).
Demographic Influences on Doctors’ Reports of the Likelihood of Discussing CAM With Patients a
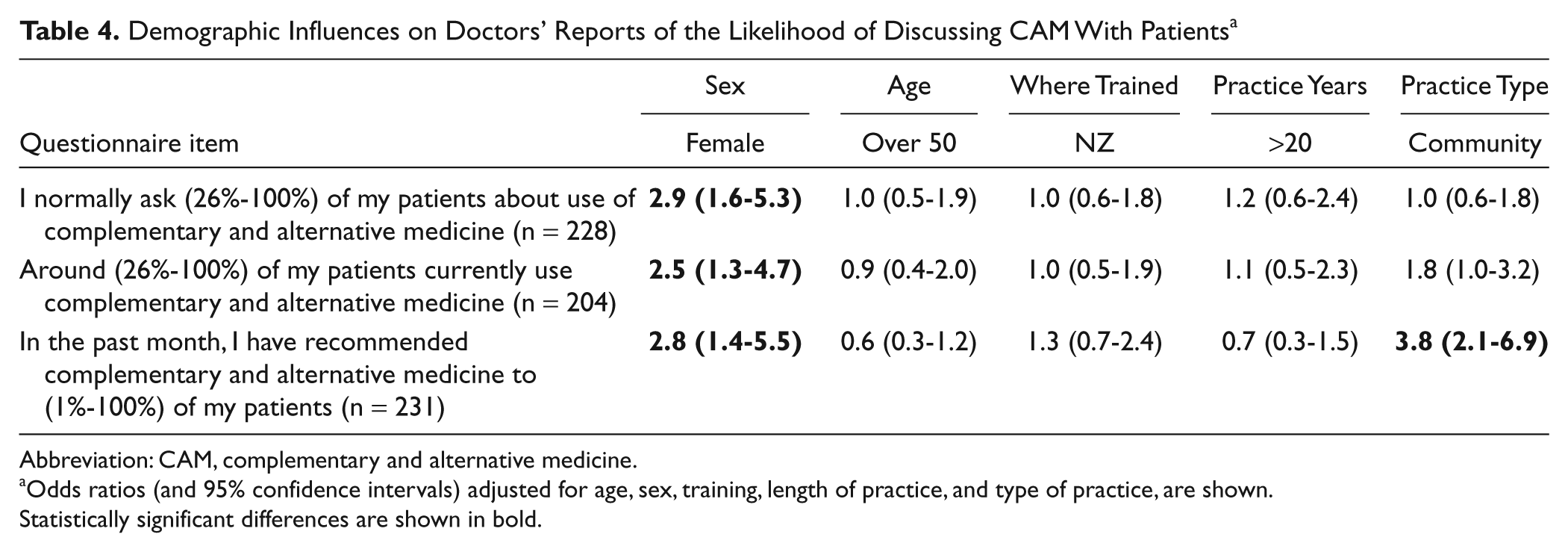
Abbreviation: CAM, complementary and alternative medicine.
Odds ratios (and 95% confidence intervals) adjusted for age, sex, training, length of practice, and type of practice, are shown.
Statistically significant differences are shown in bold.
Age
Doctors younger than 50 years were more likely than those older than 50 years to recommend CAM (68% to 47%; χ2[1, n = 231] = 10.5; P < .01), but this became nonsignificant after adjusting for other terms in the model (see Table 4).
Training
Neither χ2 analyses nor multiple regression indicated any significant differences between doctors trained in NZ and those trained elsewhere, so these results are not shown in Table 4.
Length of practice
Doctors who had been practicing for less than 20 years were more likely to recommend CAM than those who had been practicing for longer (69% to 50%; χ2[1, n = 231] = 8.4; P < .01), but this was not significant after adjusting for other terms in the model (see Table 4).
Type of practice
Community doctors were more likely than hospital doctors to report that more of their patients used CAM (45% to 34%; χ2[1, n = 201] = 5.15; P < .05) and were more likely to recommend CAM to any of their patients (72% to 40%; χ2[1, n = 227] = 23.6; P < .01); only the latter difference remained significant after correcting for other terms in the model (see Table 4).
Relationships Between Doctors’ Beliefs and Behaviors
To look at how the behaviors of asking about CAM and recommending CAM to patients were related to attitudes and demographic variables, we used a forward selection regression model procedure. (In each case, a stepwise model selection procedure resulted in the same final model). Variables considered for inclusion in the models were dichotomous variables for gender, place of training, years of practice, and type of practice, and 4-point responses (strongly agree to strongly disagree) for each of the 16 attitude items listed in Table 1.
The doctors who asked more patients about CAM were more likely to be female, to believe that they knew enough about CAM to advise patients, and to agree with the principle that CAM should be integrated into treatment regime (P < .05).
The doctors who recommended CAM to a higher percentage of patients were also more likely to be female and more likely to believe that they knew enough about CAM to advise patients. In addition, they were more likely to be based in the community (as opposed to a hospital), to want to use CAM more with patients, to use CAM personally, and to be less concerned about the lack of scientific knowledge about CAM and more willing to use CAM for an incurable disease (P < .05).
Perceived Roles for CAM
Doctors were given 4 options for completing the statement, “The major role for complementary and alternative medicine is”: adjunctive therapy (endorsed by 53% of doctors, n = 125), symptom control (17%, n = 40), palliation (9%, n = 21), and sole agent for cure (1%, n = 2). Most (59%, n = 138) endorsed 1 option, whereas some (9%, n = 20) selected more than one, and 33% (n = 77) did not select any. The final alternative was “other” (35%, n = 82), with space for doctors to elaborate. The most common ideas expressed were that the role of CAM was variable and depended on the situation (n = 14, 6%), that CAM fulfilled patient’s wishes or beliefs (5%, n = 12), that the role of CAM was for the patient to feel in control (5%, n = 11), that CAM had a placebo effect (4%, n = 9), that it had no role at all (3%, n = 8), and that CAM could be used for complete holistic care (2%, n = 5) and for psychological benefit (2%, n = 5). There were 18 comments (8%) that could not be categorized.
Discussion
Attitudes Toward CAM
Integrative medicine proposes that doctors should care for all aspects of a patient’s health: mind, body, spirit, and lifestyle. Overall, 95% of the doctors surveyed agreed with this approach to medicine. This is an encouraging result for cancer patients because Myklebust1(p826) has argued that “customizing integrative medicine treatment plans based on individual needs . . . (results) in high patient satisfaction. Furthermore, improvements in physical, mental and emotional well-being (are) indicated, across the spectrum of illness.”
However, NZ doctors were more divided in their opinions about CAM. In all, 60% of doctors agreed with the principle of integrating complementary and alternative therapies into a treatment regime. There was more support for CAM when it was used as a last resort, with more doctors being comfortable with CAM use if a disease was considered incurable (86%) rather than curable (71%). This trend is similar to that seen in a survey of Chinese and American oncologists, with more doctors saying that they would allow the use of CAM for incurable (95%) disease when compared with those saying that they would permit it for curable (63%) disease. 25
As in previous studies, 26 we found that female doctors have more positive views toward CAM than male and older doctors. This is an intriguing find, but as yet, there does not seem to be any evidence as to why this may be so. Younger doctors have also been identified as being more positive toward CAM, 26 which may be an indicator of a changing culture, but our study did not confirm this in a multivariable context. In addition, doctors practicing in the community were more positive toward CAM as compared with their hospital-based colleagues. This may be because they deal with a variety of issues, tend to be more familiar with patients, and have more opportunities to address the total well-being of a patient.
Discussions With Patients About CAM
Our study showed that only around 30% of doctors asked more than half of their patients about CAM use, replicating similar levels of disclosure revealed in previous studies.14,22,27 This relatively low level of enquiry may lead to doctors underestimating the prevalence of CAM use and its importance to their patients. Chrystal showed that 49% of NZ cancer patients questioned were using CAM, 14 but only 33.5% of doctors in the current study believed that any more than a quarter of their patients use CAM. Apart from the differences in patient groups, estimates by doctors in our study may also be low because patients are deliberately not disclosing CAM use to their doctor.
Previous studies have suggested that possible reasons for patient nondisclosure include concern about a negative response from their doctor (withdrawal of health care, absence of support for CAM, or advice against using CAM), patients believing that it was not important for the doctor to know about patients’ CAM use (because of the doctor’s lack of expertise regarding CAM), and the doctor not asking or seeming interested in CAM27-29 as well as patients deciding not to disclose CAM use because they were themselves unsure of the benefits of CAM use. 30
Patients may feel that they would not be supported if they were to inform their doctor about CAM use. 29 Only 18% of NZ doctors would recommend CAM to more than 10% of their patients. This is broadly similar to the 24% found by Lee 25 in a survey of Chinese and American oncologists and suggests that patients may (largely correctly) feel that doctors do not have positive attitudes CAM.
It is clear that doctors need to be well informed about CAM and willing to initiate relevant discussions with their patients.12,27,28,30 However, a recent survey by Lee 25 indicates that most oncologists discuss CAM with only a minority of their patients, and only 22% of oncologists feel that their training has prepared them to discuss CAM with their patients. Many (69%) were not interested in using CAM with their patients, although 95% of them would be willing to participate in the care of a patient with an incurable disease who wanted to use CAM. There are some doctors who are unfamiliar with CAM and have little interest in CAM use. 31 As with the use of CAM therapies, views of health professionals tend to vary across gender, age, and health profession, with younger, female, and nursing staff being the most positive toward CAM. 26 Oncologists, in particular, may have negative perceptions of CAM, and many have concerns about potential interactions with conventional treatments. 32
Knowledge About CAM
Doctors are trained to practice evidence-based medicine and may rule out the use of unproven therapies: many of the doctors in our survey (86%) identified lack of scientific evidence as a major concern about CAM therapies. In addition, unknown therapies may pose a risk to patients. The most common concerns that physicians had regarding CAM therapies was interference with conventional medicine (89%) and side effects (87%). Doctors who were more likely to recommend CAM to their patients were the ones who felt that they knew enough about CAM to advise patients, so it is possible (although not demonstrated) that these are doctors who have sought to educate themselves on potential effects and side effects of CAM therapies.
Perhaps because of these concerns, 58% of doctors in the current study said that they would like to learn more about CAM. This high proportion may be a result of the fact that 73% of doctors surveyed did not believe that they knew enough about CAM to be able to advise patients. This may be a result of insufficient CAM education during medical training (as only 14% agreed that they were prepared for integration of CAM during their training). This may be an issue for medical schools to consider, with the goal of possibly including more teaching about CAM in the curriculum. Previous studies have shown that physicians were a source of information regarding CAM use for only 19% of patients 13 and that patients would like to receive more information about CAM from their doctors. 21 Many doctors (62%) also agreed that they would like to learn more about Māori holistic views of health. As this has been identified as an important aspect of medical practice (93% of the doctors surveyed agreed that this was important), it may also be an aspect of training that needs to be enhanced. Doctors who felt that they knew enough about CAM to advise patients were more likely to ask patients about CAM use and also more likely to recommend CAM to more patients.
Roles
More than half of the doctors surveyed endorsed the idea that CAM could be useful as an adjunctive therapy for cancer, as advocated by integrative medicine. 2
Limitations of the Study
Doctors were recruited from a single geographic area within NZ, which may limit generalizability of the findings. The majority of respondents did not specialize in oncology, although it is likely that all the GPs would include cancer patients in their practices.
Summary
Integrative medicine is increasingly being accepted into medical practice, but many doctors still do not agree with the use of CAM. There is a need for increased patient disclosure of CAM use and for doctors to enquire directly about CAM use. Lack of knowledge regarding CAM may be a barrier to communication between doctors and patients and should be addressed. Medical training and further research could help by providing increased knowledge about and enhancing the acceptance of CAM.
Footnotes
Appendix
Acknowledgements
We thank the Dunedin School of Medicine for providing a Summer Research Scholarship for CB to undertake this project, the Department of Psychological Medicine for supporting the project, Dr Richard Lee for permission to adapt the questionnaire, and especially all the doctors for participation in the survey. Dr Reeder and the Cancer Society Social & Behavioural Research Unit receive support from the Cancer Society of New Zealand Inc and the University of Otago. We also thank Dr Keith Block and 2 anonymous reviewers for their helpful comments.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CB was supported by a Summer Research Scholarship from the Dunedin School of Medicine