
Abstract
Anthracyclines are potent antineoplastic agents associated with cardiotoxicity, which may lead to congestive heart failure, causing impairment of autonomic cardiovascular function as assessed by heart rate variability (HRV). This decreases survival rates. This study aimed to determine whether music therapy intervention improves autonomic function in anthracycline-treated breast cancer patients, and if so, whether such improvements persist after cessation of the intervention. Participants were 12 women with breast cancer who had undergone mastectomy or breast-conserving treatment and adjuvant chemotherapy; they attended 8 weekly music therapy sessions, each lasting 2 hours. Electrocardiogram traces (5 minutes) for HRV analysis were recorded 4 times: prior to the first music session, T1; after the fourth music session, T2; after the eighth music session, T3; and 4 weeks after the completion of music therapy, T4. HRV parameters were subjected to a nonparametric Friedman test on the differences between T1 and T2, T3, and T4. The standard deviation of normal intervals and the total power of HRV parameters, related to global autonomic function, were significantly higher at T3 than at T1. The root-mean-square differences of successive normal R–R intervals and high-frequency (HF) HRV parameters, related to parasympathetic activity, were significantly increased, but no change was seen in the LF/HF ratio of HRV parameters (which is related to sympathetic activity) during the music therapy. Global autonomic function and parasympathetic activity had not changed significantly at T4 relative to T1. The authors provide preliminary evidence of the benefits of music therapy for anthracycline-treated breast cancer survivors.
Keywords
Introduction
Anthracyclines such as doxorubicin and epirubicin are potent antineoplastic agents that have been used increasingly in recent years for the treatment of breast cancer. Breast cancer patients who present with only locoregional lymphatic metastases and are treated with surgery and adjuvant anthracycline-containing chemotherapy have a reduced risk of disease progression.1,2 However, anthracycline-induced cardiotoxicity, which may lead to congestive heart failure, is a well-known side effect of this treatment. 3 Cardiotoxicity can become clinically overt shortly after the commencement of anthracycline treatment but may also manifest many years later. 4
Congestive heart failure impairs the autonomic regulation of cardiovascular function.5,6 Heart rate variability (HRV) analysis is a commonly used, reliable, and noninvasive tool for assessing autonomic function. 7 Decreased HRV is a marker of cardiovascular autonomic dysfunction 8 and a predictor for cardiovascular risk and increased mortality9,10; it can be used as a sensitive tool in the early detection of anthracycline-induced cardiotoxicity. Previous research has demonstrated that HRV is significantly lower in breast cancer patients who have been treated with anthracycline chemotherapy than in healthy, age-matched females. 11 Moreover, recent research has found that a decreased HRV is associated with significantly shorter survival in cancer patients. 12 Therefore, it is likely that the clinical outcome of anthracycline-treated breast cancer patients will improve if their autonomic function is improved.
Music therapy involves the skillful use of musical elements by an accredited music therapist to improve a person’s mental and physical health. It provides a unique form of emotional and spiritual support and can reduce levels of stress and anxiety. 13 Some studies have shown that listening to relaxing music induces positive emotions and increases parasympathetic nervous system activity.14,15 A recent investigation also suggested that music therapy enhances parasympathetic activity and decreases the likelihood of congestive heart failure events in elderly patients with cerebrovascular disease and dementia. 16
Based on previous findings, it is reasonable to hypothesize that music therapy intervention could also improve autonomic cardiovascular function in breast cancer patients. The aim of the present study was to determine whether a long-term (weekly for 8 weeks) music therapy intervention improved the autonomic function (as assessed by HRV) of anthracycline-treated breast cancer patients, and if so, whether such improvements persisted after the cessation of music therapy.
Methods
Study Participants
The participants in this pilot study comprised 12 women with breast cancer recruited from the Hope Society for Cancer Care, Taipei, Taiwan, who met the following inclusion criteria: completed mastectomy or breast-conserving treatment and adjuvant chemotherapy treatment, no history of cardiovascular disease, and normal respiration rate of between 9 and 24 breaths/min. The patients had been treated with adjuvant anthracycline-containing chemotherapy. Five patients had been treated with 6 cycles of chemotherapy, consisting of 5-fluorouracil, doxorubicin, and cyclophosphamide (total cumulative dose of doxorubicin was 450 mg/m2). Two patients had been treated with 4 cycles of chemotherapy, consisting of doxorubicin, and cyclophosphamide (total cumulative dose of doxorubicin was 300 mg/m2). Five patients had been treated with 4 cycles of chemotherapy, consisting of doxorubicin and cyclophosphamide followed by paclitaxel (total cumulative dose of doxorubicin was 300 mg/m2). The mean age was 48 years (range 29-60 years), and the mean interval since the completion of adjuvant chemotherapy at recruitment was 13.2 weeks (range 4-32 weeks). The procedures used in this study were approved by the Institutional Review Board of National Yang-Ming University, and all patients provided informed consent to participate.
Music Intervention Program
Patients attended 8 weekly music therapy sessions, each lasting 2 hours. Sessions were provided within a group setting (comprising 12 patients, 1 music therapist, and 1 nursing staff) and comprised 3 activities. The first activity was aimed at establishing a rapport between the therapists and the participants through singing and listening. The songs used in the first activity were popular Taiwanese songs with pleasant, moderate rhythms and tempos. The second activity involved learning how to play musical instruments and featured different instruments in each session. The musical instruments used included egg shakers, Cadeson bongos, hand-bells, metallophones, recorders, and ukuleles. This activity used the learning of a simple musical instrument to establish the participants’ self-confidence. The third activity involved performing on a musical instrument with accompaniment from the therapist’s electric keyboard. The aim of this activity was to encourage participants to express themselves and to stimulate relaxed and positive emotions.
In these activities all patients listened to the same songs simultaneously and played all the instruments. When there were too few musical instruments (metallophones and ukuleles) to allow the 12 patients to play simultaneously, the patients played the instruments in turns to ensure that all patients played all the instruments. The performing level required in the third activity was simplified, so that the patients did not need a high level of musical skill—they only needed to play 5 to 10 notes, which ensured that all patients performed at the same level of intervention.
The activities were led by a single professional music therapist who actively engaged the patients in their musical performances, and a nursing staff observed the patients’ physiological state and participation level and assisted in ensuring that the music therapy progressed. Therapy records were maintained by the therapist and nursing staff based on their observations during each session of music therapy, and these included the patients’ participation and musical skill levels. These records were used by the therapist to make minor modifications to the therapy activities and by the nursing staff to understand which patients needed more assistance in playing the instruments. This procedure ensured adequate quality control of the music therapy intervention.
Measures and Apparatus
Electrocardiogram (ECG) traces (5 minutes) for HRV analysis were recorded on 4 occasions: (1) at a time prior to the first music therapy session, T1; (2) after the fourth session, T2; (3) after the eighth session, T3; and (4) 4 weeks after the completion of music therapy.
HRV, a physiological phenomenon whereby the time interval between heart beats varies, is measured by calculating the variation in the beat-to-beat interval from a clear ECG waveform. In this experiment, the participants were asked to sit and rest for 5 minutes to allow their heart and respiration rates to stabilize. Participants whose respiration rate was outside the normal range (either lower or higher) of 9 to 24 breaths/min were excluded to ensure that the breathing only influenced the high-frequency (HF) band (0.15-0.40 Hz) of HRV. An ECG signal was then recorded for 5 minutes. ECG recordings were obtained from lead I of the bipolar leads using an ECG event recorder (VitalECG, Aescu Technology, Taipei, Taiwan). The recorded data were digitized at a sampling rate of 500 Hz and stored for later analysis.
The HRV was determined in ECG signals using a standard procedure. 8 The R point of each QRS complex was defined from each heart beat, and the R–R intervals (RRs) were calculated sequentially from 5-minute-long ECG signals and checked for artifacts. The calculated time-domain analysis indices of HRV included the mean RR, the standard deviation of normal intervals (SDNN), and the root-mean-square differences of successive normal RRs (r-MSSDs).
In the frequency-domain analysis of HRV, sequential RRs were interpolated linearly to produce a continuous signal and then were resampled at 3 Hz. The HRV spectrum was obtained using power spectrum density analysis based on the fast Fourier transform with a Hamming window. The HRV spectrum was subsequently quantified into standard frequency bands, including total power (TP, 0.01-0.4 Hz), low frequency (LF, 0.04-0.15 Hz) power, and HF (0.15-0.40 Hz) power, and the ratio of LF to HF power (LF/HF). Logarithmic transformation (ln) was used to correct the skewness of the distributions in TP, LF power, HF power, and LF/HF.17,18
Statistical Analyses
The results were analyzed statistically using the statistical software package SPSS (version 15.0, SPSS, Chicago, IL, USA). Data are expressed as mean and standard deviation values. The study hypothesis was tested by subjecting the HRV parameters to a nonparametric Friedman test on the change from baseline (T1) to T2, T3, and T4. Post hoc comparisons were performed using the nonparametric Wilcoxon signed rank test procedure. All time points were compared with T1, and the Bonferroni correction for multiple comparisons was used. The level of statistical significance was set at P < .016 (P < 05/3).
Results
The study participants (n = 12 women) were 48.0 ± 8.2 years old (range 29-60 years). Each participant was evaluated 4 times. Outcome measures were changes in the following HRV parameters: RR, SDNN, r-MSSD, ln(LF power), ln(HF power), ln(TP), and ln(LF/HF). (See Table 1 for details.) The Friedman test was used to analyze HRV parameters across the 4 time points.
Heart Rate Variability Measurements a Between Music Therapy Sessions in 12 Patients With Breast Cancer

Note: RR = R -R interval; SDNN = standard deviation of normal intervals; r-MSSD = root-mean-square differences of successive normal RRs; ln, logarithmic units; TP = total power; LF = low frequency; HF = high frequency.
Data are mean ± SD values.
P < .005 versus T1 by nonparametric Wilcoxon signed rank test.
P < .016 versus T1 by nonparametric Wilcoxon signed rank test.
RR, SDNN, r-MSSD, ln(HF power), ln(LF power), and ln(TP) differed significantly from baseline (T1) at T2, T3, and T4, whereas no significant change was found for ln(LF/HF). Post hoc comparisons indicated that the mean RR, SDNN, r-MSSD, ln(HF power), ln(LF power), ln(TP) values increased significantly from T1 to T2 (P < .016) and from T1 to T3 (P < .016), but there was no significant change from T1 to T4. The changes in HRV parameters are shown in Figure 1.
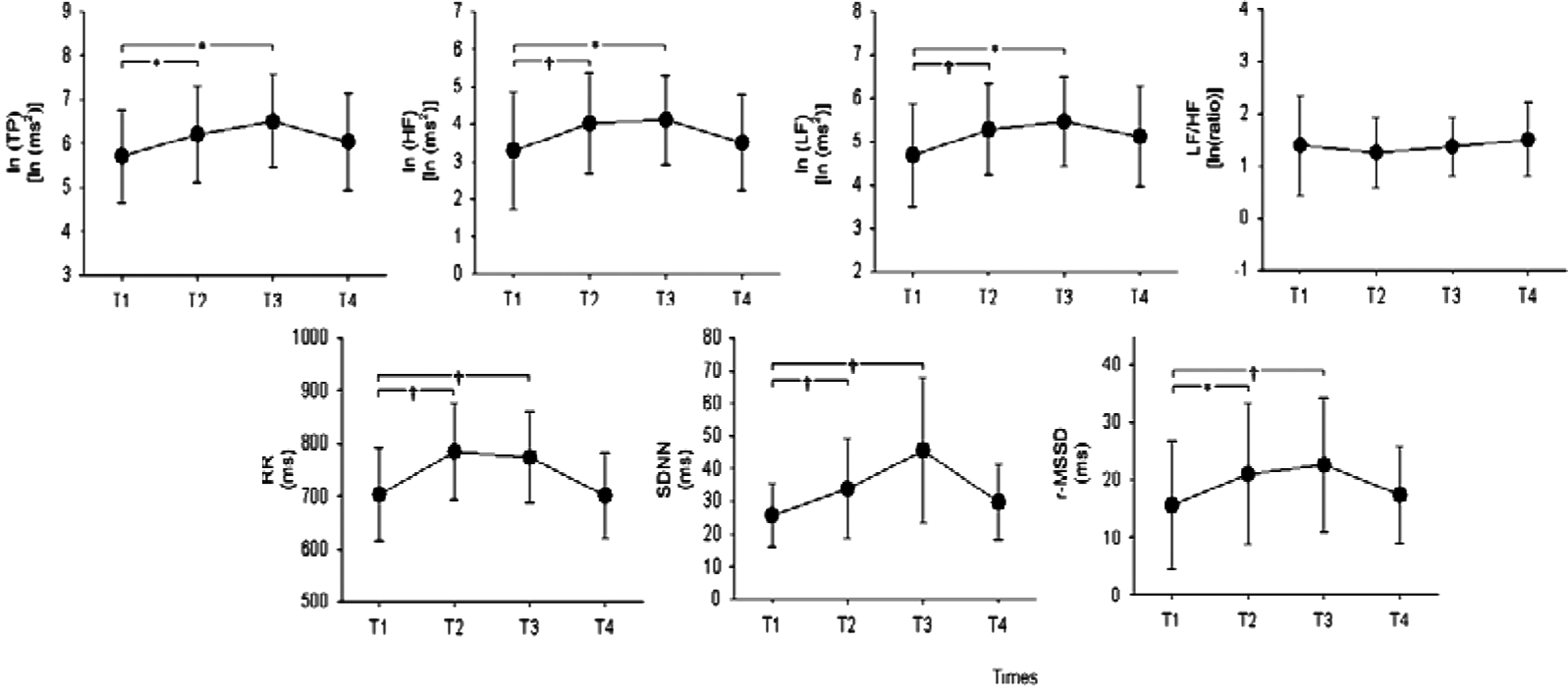
Changes in R–R interval (RR), standard deviation of normal intervals (SDNN), root-mean-square differences of successive normal RRs (r-MSSD), ln(TP [total power]), ln(high-frequency [HF] power), ln(low-frequency [LF] power), and ln(LF/HF ratio) between music therapy sessions in patients with breast cancer. *P < .016, † P < .005 versus T1 by nonparametric Wilcoxon signed rank test. Data are mean and SD values
Discussion
We investigated whether long-term music therapy intervention improves autonomic function among anthracycline-treated breast cancer patients, and if so, whether this change was sustained following the cessation of music therapy intervention.
HRV analysis showed that the time-domain (SDNN) and frequency-domain parameters (TP) had increased significantly by the end of the 8-week course of music therapy. The SDNN and TP of HRV are well known to be representative of the global autonomic function of the heart, 8 and hence, our results suggest that the global autonomic function can be improved with 8 sessions of music therapy intervention. We also found that the time-domain (r-MSSD) and frequency-domain parameters (HF power) were related to parasympathetic activity,8,18 in that they had increased significantly by the end of the 8-week music therapy period compared with baseline. In addition, the RR exhibited a similar pattern of heart-rate changes. The frequency-domain parameters (LF power) were jointly contributed by both sympathetic and parasympathetic nerves, 19 in that they had also increased significantly by the end of the 8-week music therapy period compared with baseline. On the other hand, the frequency-domain parameter LF/HF related to sympathetic activity20,21 did not show any significant changes during the music therapy period, suggesting that the 8 sessions of music therapy intervention particularly increased parasympathetic activity. These findings are consistent with those of other studies showing that music enhances parasympathetic nervous system activity.14-16
The findings of a previous study also suggest that the parasympathetic nervous system is activated by music therapy and appears to protect against congestive heart failure events in elderly patients with cerebrovascular disease and dementia by reducing the levels of both epinephrine and norepinephrine. 16 Therefore, music therapy intervention may also help breast cancer patients control the progression and relieve symptoms of cardiac damage, which is a result of treatment with anthracycline-containing chemotherapy.
We also investigated the changes in autonomic function following the cessation of music therapy intervention. We found that global autonomic function (SDNN and TP) and parasympathetic activity (r-MSSD and HF) had not changed significantly 4 weeks after the music therapy intervention was terminated (T4) as compared with baseline (T1). These results suggest that 8 sessions of music therapy intervention can promote autonomic function while therapy is being undertaken but that these improvements do not persist after the intervention terminates.
This investigation had 2 limitations: the small number of participants and the lack of a parallel control group. Music therapy is not popular for cancer patients in Taiwan at present, and the Taiwanese personality is characterized by shyness. As such, many cancer survivors feel embarrassed and are unwilling to go outside, which is why only a small number of participants was included in the study. The study results therefore only provide preliminary evidence that regular music therapy intervention can promote autonomic function. Further research is needed to determine the effects of a higher number or higher frequency of intervention sessions on autonomic function and whether these improvements can be sustained in breast cancer patients.
Conclusion
This study provides preliminary evidence of the benefits of music therapy for anthracycline-treated breast cancer survivors. Regular music therapy appears to be useful for promoting autonomic function, although further research is necessary to determine whether more (or more frequent) sessions of music therapy intervention can promote and maintain autonomic function after music therapy is stopped.
Footnotes
Acknowledgements
The authors thank Hui-Chen Lee for her assistance with the statistical analysis and the Hope Society for Cancer Care, Taipei, Taiwan, for their support of this research.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.