
Abstract
Fatigue is one of the most frequent and distressing complaints reported by patients with cancer. Describing relationships among disrupted circadian rhythms and cancer-related fatigue is important to the design and testing of interventions that target specific underlying etiology of fatigue. The purpose of this article is to review the literature on whether evidence exists to support the notion that disrupted circadian rhythms provide a mechanism of cancer-related fatigue. Searches were conducted from January 1950 to January 2010, to locate pertinent articles using 4 electronic databases: PubMed, MEDLINE, CINAHL, and Scopus. Results identified 42 quantitative research studies, which were then retrieved. After reviewing the articles, 15 were selected as meeting the established criteria of the study and were critiqued. Statistical approaches varied across studies, which may influence generalizability of results. Although commonalities across studies did emerge, there was a lack of consistency in variables studied, and most studies did not identify a theoretical framework. More research needs to be conducted using consistent types and characteristics of disrupted circadian rhythms in relation to fatigue, including temporal relationships between circadian rhythms, fatigue, and cancer.
Introduction
Fatigue is one of the most frequent and distressing complaints of patients with cancer; 60% to 99% of patients studied experience some level of fatigue, and more than 60% rate their fatigue as moderate to severe.1-3 Fatigue related to cancer and its treatments differs from fatigue related to activity or exertion. Whereas healthy individuals report fatigue to be a normal, regulating phenomenon that helps them schedule their daily rhythm and disappears after a good night’s sleep, patients with cancer report unpleasant, distressing, and activity-limiting fatigue throughout the day. 4 Although cancer-related fatigue is pervasive, the phenomenon is poorly understood. Fatigue has been attributed to various factors, including stress, 5 endocrine imbalances,6-8 insomnia,9,10 biochemical changes secondary to disease and treatment, weight change, and internal and external environmental conditions.3,11 Other researchers have suggested that the causes of fatigue include physiological factors (eg, anemia, pain), psychological factors (eg, anxiety), and chronobiological factors such as altered circadian rhythms.12,13
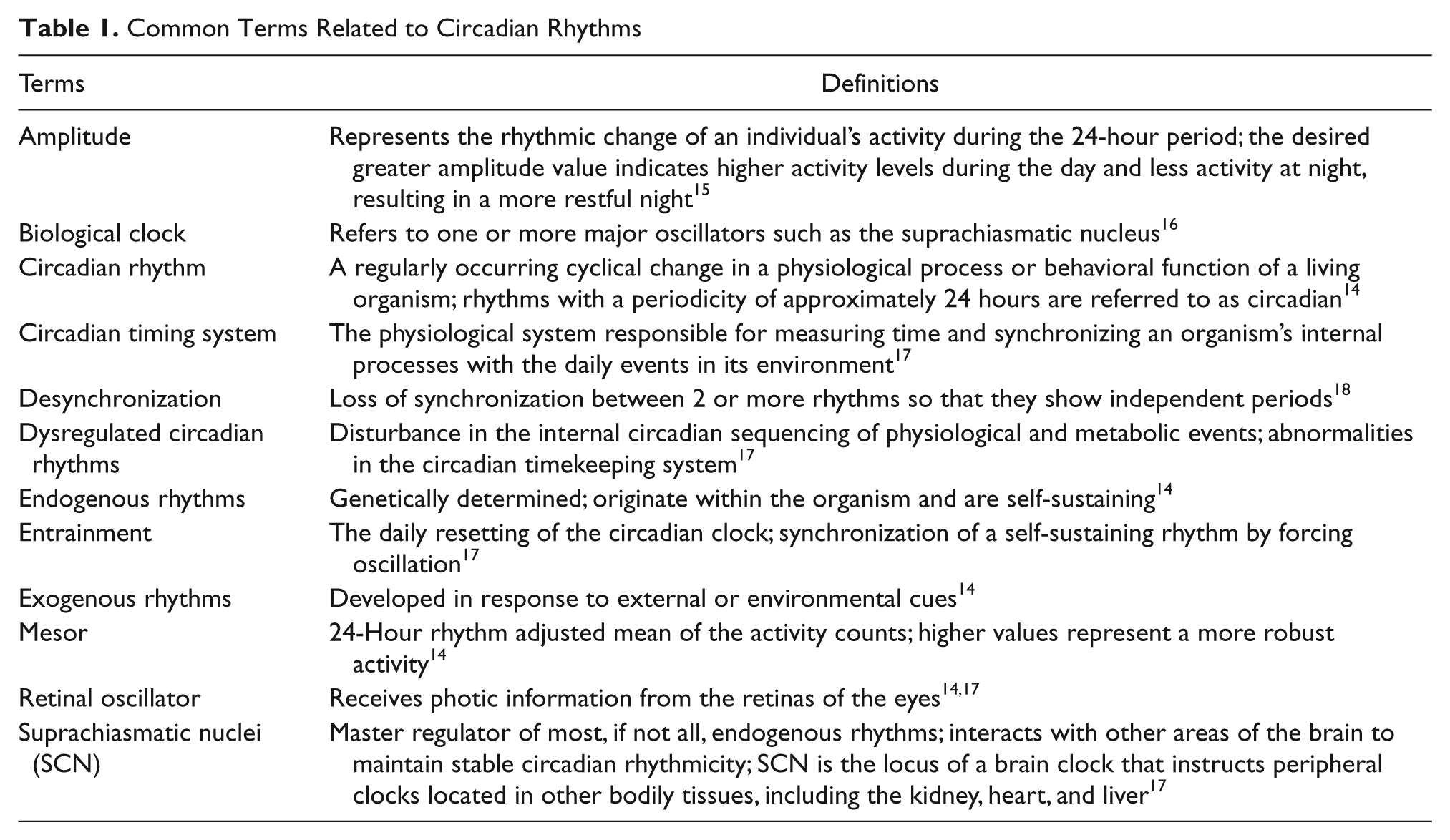
Circadian rhythms are exogenous or endogenous physiological patterns that run on an approximate 24-hour cycle and modulate several biological functions. 14 A rhythm that develops in response to external or environmental cues is called an exogenous rhythm, whereas genetically determined endogenous rhythms originate with the organism and are self-sustaining, even in the absence of external time cues. Determining the amplitude of a rhythm is important because it indicates the strength of the circadian system. The desired larger amplitude value indicates higher activity levels during the day and less activity at night resulting in a more restful night. 15 Table 1 provides definitions of commonly referenced terms in literature examining circadian rhythms.
Common Terms Related to Circadian Rhythms
The Circadian Timing System
The physiological system responsible for measuring time and synchronizing an organism’s internal processes with the daily events in its environment is known as the “circadian timing system.” 18 The function of the circadian timing system is to provide a temporal organization of physiological processes and behavior to promote effective adaptation to the environment. The scheduling of behavioral and physiological events is one of the most critical functions performed by the circadian timing system. Not only does the timing system control the basal level of physiological systems, but it also influences the responsiveness of each system to challenges at different times of the day. If the daily timing of the challenge is highly predictable, an internal circadian clock can enable the animal to place the appropriate homeostatic mechanisms “in a state of alert.” 18 But if the daily timing of the challenge is unpredictable (eg, cancer, chemotherapy side effects), the internal circadian clock may not be capable of placing the appropriate mechanism in alert status.
The central circadian system has 3 major components and functions. The first component is signaling inputs, the most dominant being the timing of exposure to ambient light perceived by specialized sensors in the eye, which results in neurophysiologic changes in the central clock in the hypothalamus. 17 The second component is the central oscillator, which produces electrophysiologic signals that arise from paired populations of neurons in the suprachiasmatic nuclei (SCN), and the third component is made up of afferent nerve fiber groups projecting from the SCN to the hypothalamus and represents the output network. 17
When the circadian system malfunctions, rhythm disorders occur, which can be classified as disorders of phase relations (timing), disorders of amplitude (magnitude of change), and disorders of entrainment (synchronization).14,18 Optimal functioning of most physiological, psychological, and behavioral processes requires synchronization of the body’s circadian rhythms; evidence supports the theory that disrupted circadian organization increases cancer risk and progression rate and decreases dimensions of quality of life. 19
For people with cancer, altered physiology related to the disease and/or treatment appears to play a prominent role in disrupting circadian regulatory processes.20-22 Disruption of the daily sleep–activity rhythm, which concurrently reflects both endogenous circadian clock function and environmental synchronization, is apparent among patients with cancer.23,24 Mormont et al 22 found evidence that suggests the individual’s circadian function is associated with some dimensions of a patient’s psychological distress and quality of life and that patients with marked rest/activity rhythmicity had better quality of life and reported less fatigue. As a consequence, disruptions in sleep patterns account for many of the symptoms that affect patients with cancer and fatigue. 25
The etiology of circadian rhythm disruption in cancer patients is complex and multifactorial. 22 Increasingly research suggests that there are profound physiological and pathophysiological consequences of circadian disruption at the cellular levels of biological and social organization.19,26 Hrushesky et al 19 suggest that specific core clock genes (Per2 and Per1) suppress tumors because their genetic absence doubles tumor numbers and decreasing their expression in cancer cells doubles cancer growth rate, whereas their overexpression decreases cancer growth rate and diminishes tumor numbers.
No systematic review of the literature has been done on the topic of fatigue, circadian rhythms, and cancer. Although research studies examining circadian rhythms and their relation to cancer-related fatigue are limited, recent findings suggest that this is a significant area of investigation and that there is an acute need for a focused review on this topic.10,27 Therefore, the purpose of this systematic review is to examine relationships among altered circadian rhythms and their relationship with fatigue in the context of cancer. The main aims are to (a) critique quantitative research studies that focus on cancer-related fatigue as a primary outcome, (b) examine types of circadian rhythms that were assessed and measured, and (c) critically evaluate findings and conclusions.
Methods
The databases PubMed, MEDLINE, CINAHL, and Scopus were searched for articles published between 1950 and 2010. For inclusion, studies had to meet the following criteria: published in a peer-reviewed journal, quantitative design, human subjects, English language, and cancer patients, fatigue, and circadian rhythms. A medical librarian provided assistance in conducting this search using the terms fatigue, circadian rhythms (altered circadian rhythms), and cancer (neoplasms). The first search using PubMed netted 42 articles. By limiting the search to experimental research articles, written in English, and limited to adult humans, 36 articles were retrieved. After initial review of the articles, 15 were identified as meeting our established criteria.
In the second search, using the MEDLINE database, the mesh terms fatigue, circadian rhythms, and cancer (neoplasms) were used, which netted 14 articles; all 14 articles were also included in the 36 articles retrieved from the PubMed search. Limiting the search to quantitative research articles, English, and adult humans reduced the number to 4. Using the CINAHL (EBSCO host) database, the search produced 13 articles using the terms fatigue, circadian rhythms, and cancer. By limiting the search to quantitative experimental research, English, and adult humans, 4 articles were retrieved and included in the review. All 4 articles were included in the initial PubMed search. Last, using the Scopus database, 21 articles were found using the search terms fatigue, circadian rhythms, and cancer. Limiting the search to quantitative research articles, English, and adult humans resulted in 3 articles, also identified in the original PubMed search. In summary, 15 articles were reviewed using the criteria described above (Table 2).
Research Studies on Fatigue, Circadian Rhythms, and Cancer

Abbreviations: FACT-F, Functional Assessment of Cancer Therapy–Fatigue; BFS, Bidimensional Fatigue Scale; FCS, Fatigue Catastrophizing Scale; WAS, Work and Social Adjustment Scale; HADS, Hospital Anxiety and Depression Scale; EORTC-QLQ, European Organisation of Research and Treatment of Cancer–Quality of Life; EORTC-BR, European Organisation of Research and Treatment of Cancer–Breast Module; CRF, cancer-related fatigue; CRFS, cancer-related fatigue syndrome; RCT, randomized-clinical trial; PFS, Piper Fatigue Scale; DFI, Daily Fatigue Intensity; BMI, body mass index; QOL, quality of life; PSQI, Pittsburgh Sleep Quality Index; KPS, Karnofsky Performance Status; MFSI-SF, Multidimensional Fatigue Symptom Inventory–Short Form; FOSQ, Functional Outcomes of Sleep Questionnaire; FACT-B, Functional Assessment of Cancer Therapy–Breast; CES-D, Center for Epidemiologic Studies Depression Scale; HPA, hypothalamic–pituitary–adrenal; MAF, Multidimensional Assessment of Fatigue; FSCL, Fatigue Symptom Checklist; HDI, Hamilton Depression Inventory; POMS, Profile of Mood States.
Although other articles were found, they did not use a quantitative design, did not focus on fatigue and/or use a fatigue-sensitive instrument, or the sample did not consist of adult patients with cancer; therefore, these articles did not meet the criteria used for this review. For example, Dogliotti et al 39 studied stages I-II and stages III-IV breast cancer, stages III-IV lung cancer, and advanced gastrointestinal cancer patients, and they reported a significant rhythm of serum melatonin in advanced cancer patients; Touitou et al 40 reported deeply altered cortisol circadian rhythms in breast and ovarian cancer patients who had received first-line chemotherapy and hormonal treatment regimens. However, fatigue was not a primary outcome of these studies and therefore were not included in the review.
Several review articles addressed different circadian rhythms, cancer, and a variety of symptoms, including fatigue. A current review by Miller et al 7 provides a thorough overview of neuroendocrine mechanisms and the role of disrupted circadian rhythms in behaviors such as cancer-related fatigue. However, only 1 systematic review article was found on circadian rhythms and fatigue, and that article focused on shift work–related fatigue. Review articles provide an excellent description of the work that has been done to date and, more important, important research that still needs to be conducted.
Results
The studies from this review illustrate the range and variability of the work on circadian rhythms and fatigue in patients with cancer. This article provides a systematic review of relevant articles describing the relationships among disrupted circadian rhythms, fatigue, and cancer; it highlights the research work accomplished and, more important, areas needing more investigation. Key questions generated from this systematic review are the following: (a) Does research provide adequate evidence to suggest that altered circadian rhythms provide an underlying mechanism of cancer-related fatigue? (b) What critical gaps exist in the literature with respect to altered circadian rhythm activity and cancer-related fatigue?
Instrumentation
Although the empirical evidence currently available on the role of circadian rhythms and cancer-related fatigue is limited, there is general agreement as to the nature and significance of this topic in symptom management of patients with cancer. A critical concern identified in the literature is that several different instruments were used to measure fatigue from one study to another, some of which focused specifically on measuring fatigue as an outcome and others that did not. Instruments used in some of the critiqued studies measured several symptoms, including fatigue, depression, anxiety, and quality of life, and did not necessarily focus on cancer-related fatigue. However, the instruments used, whether fatigue scales or symptom assessment measures, did have established reliability and validity (Table 3).
Instruments Used to Measure Fatigue in Critiqued Articles

Unfortunately, not all authors identified and included key parameters of circadian measurement such as amplitude and mesor. It should be noted, however, that while classic circadian parameters were not reported, it does not necessarily mean they were not measured. It is possible that they were not related to the patient outcomes. Another key concern was the lack of consistency regarding the use of different terms when referring to disrupted circadian rhythms. When researchers used the term dampened, it was not clear whether they were referring to lower, altered, or dysregulated. Of the articles retrieved for inclusion in the review, all but one used sleep wrist actigraphy as a sleep measure. Overall, the type of cancer varied across studies, and sample sizes of individual studies were small.
Fatigue and Disrupted Circadian Rhythms in Patients With Cancer
Whereas all 15 articles described an association between fatigue levels and selected circadian rhythm disruption in patients with cancer, there were inconsistencies among circadian rhythms and types of cancer patients studied. The majority of articles that focused on circadian rhythms and cancer-related fatigue were on breast cancer. Several articles focusing on lung, colorectal, and nonspecific cancer populations were identified; however, they did not focus on cancer-related fatigue.
Breast cancer
Early research on disrupted circadian rhythms in patients with cancer reported that patients with breast cancer whose sleep was disrupted at cycle midpoints are at risk for cancer-related fatigue and that the cumulative effects of less daytime activity, more daytime sleep, and night awakenings are associated with higher fatigue levels. 38 It was also noted that a disruption of circadian rhythms was significantly correlated with increasing symptoms of fatigue and depression in patients with breast cancer receiving chemotherapy. 21 Other researchers examined predictors of fatigue in patients with breast cancer 30 days after adjuvant chemotherapy and found that the strongest predictor was the fatigue level of the individual prior to receiving the initial chemotherapy treatment. 30 Berger et al 29 reported disrupted circadian activity rhythm parameters in breast cancer patients receiving adjuvant chemotherapy when compared with healthy adults, but these values were similar to values of patients with cancer. They found significant changes in key circadian rhythm parameters (mesor, amplitude, peak activity, and 24-hour autocorrelation values) over time in both groups. Over the course of chemotherapy treatments, more robust circadian activity rhythm parameters (except acrophase and circadian quotient) were associated with lower fatigue (P < .05). In a separate study, Berger et al 36 reported that women with breast cancer (n = 25) reported mild fatigue and sleep actigraphy results that showed time awake after sleep onset exceeded the desired <30 minutes.
Researchers have examined fatigue, sleep, and circadian rhythms in women with breast cancer 72 hours prior to chemotherapy and found that these women reported high fatigue levels and disturbed sleep. 36 Although circadian rhythms were in general robust, breast cancer patients with more delayed circadian rhythms experienced more daily dysfunction (P < .01). 31 Other researchers have also found that fatigue levels were high and sleep was disturbed even before patients with breast cancer received chemotherapy; however, they found that fatigue levels intensify even more after beginning chemotherapy.9,31 Thus, being fatigued before chemotherapy is even initiated may make fatigue more pronounced during chemotherapy. In summary, the literature is consistent in reporting significant associations between circadian rhythm disruption and higher levels of fatigue (and sleep/wake disturbances) in patients with breast cancer.15,29-31,36,38
Fatigue and Biological Markers in Patients With Other Cancers
There is evidence that alterations in the neuroendocrine system can have negative effects on biological processes. Biological underpinnings, such as cortisol, proinflammatory cytokine activity, and transforming growth factors, are factors in cancer-related fatigue. These circulating biologics display significant circadian rhythms that, when altered, have the capacity to contribute to and indeed may be indicators of fatigue, insomnia, and depression. Researchers have reported that a positive correlation exists between diurnal cortisol rhythms and fatigue in patients with cancer.16,34,39,41 Significant differences have been found in fatigue severity and sleep disturbances between disease-free breast cancer survivors with or without cancer-related fatigue. Whereas actigraphy data have demonstrated significant differences in sleep quality and disturbances, no significant differences were found in the 24-hour urinary free cortisol levels or circadian rhythm. 16
Research has shown that patients with cancer (breast, lung, colon, skin) were more fatigued than controls, had worse sleep quality, more disrupted circadian rhythms, lower daytime activity levels, and worse quality of life. 33 Levin et al 25 concluded that patients with advanced lung cancer experienced greater circadian activity/sleep disruption and endured a greater interference with function, increased anxiety and depression, disrupted nighttime sleep, greater daytime fatigue, and poorer quality of life. 25 Other researchers have found that elevated serum cytokines correlated with altered behavior, serum cortisol rhythm, and dampened 24-hour rest–activity patterns in patients with metastatic colorectal cancer. In a retrospective clinical study with colorectal cancer patients, Rich et al 33 identified a significant correlation between dampened circadian rhythm, poor quality of life scores, high serum levels of proinflammatory cytokines, and flattened cortisol rhythms. More specifically, they found significant correlations between serum cytokines (TGF-α and interleukin-6), circadian patterns in wrist actigraphy, serum cortisol, and fatigue and poorer performance status in 80 colorectal cancer patients with either normal (group 1, n = 40) or dampened (group 2, n = 40) circadian rhythms. 33 Findings from a recent prospective study indicated that transforming growth factor (TGF-α) inhibited hypothalamic behavior and that elevated levels of TGF-α were associated with higher levels of fatigue and flattened circadian rhythms in colorectal cancer patients. 17 Innominato et al 42 suggest that the circadian timing system constitutes a novel therapeutic target; interventions that normalize circadian timing system dysfunction may affect quality of life, including fatigue and survival. However, since their article does not include fatigue as an outcome, it was not included in the review.
Although significant data were gleaned from the literature that provide a platform for further research, the research does not consistently use similar terms and definitions or the same data collection measurements across patient populations, which may influence research findings. In addition, the absence of using a theoretical framework to guide investigations (and whether the data supported the framework), and the lack of generalizability of study results, may have limitations for the application of results to clinical practice.
Patterns Identified and Limitations
Investigating circadian rhythms in humans is difficult, especially those with illness and treatment-related effects. Moreover, the measurement of circadian rhythms is challenging, and especially challenging in individuals with cancer. Unfortunately, some of the research that has been conducted on circadian rhythms and cancer-related fatigue poses significant limitations. For example, the literature does not always identify the primary outcome or outcomes being studied, or specify why a particular rhythm was selected to be studied. There is a lack of consistency in types of measures used and in describing characteristics of rhythms, such as amplitude, mesor, or period. Moreover, some of the research results contain a spectrum of different variables being studied from one study to another. Last, statistical analyses of similar variables are not consistent, thus interpretation of findings may present methodological and statistical limitations.
Based on this review of the literature, the following patterns appear salient in this body of research. First, the heterogeneity of terms used throughout the literature makes it difficult for readers to compare studies and interpret their findings. For example, several terms are used interchangeably when describing disrupted circadian rhythms, including dysregulated, altered, dampened, flattened, or desynchronized. This poses some confusion in interpreting the data since there is a lack of clarification as to whether these terms were actually describing the same measure or whether they pose the same meaning from one researcher to another. It is also not clear whether different environmental factors may have played a role in analyzing the data collected. For example, descriptions of laboratory techniques used in the analysis of biologics and the range of normal values of specimens referenced are not consistently documented in the studies. Another characteristic of the literature is that sample sizes are relatively small (N < 100). Finally, consistency from study to study varied considerably regarding reporting of validity and reliability of instruments used, and most studies were limited to a specific type of cancer. Within the breast cancer studies, some samples are limited to patients with early-stage cancers, some with metastatic cancer, and some to breast cancer survivors. Thus, the generalizability of study findings across patients with different cancers or at different stages of cancer may be limited.
Moreover, the circadian rhythms measured in these articles vary across studies (eg, sleep/wake cycles, cortisol, body temperature). Perhaps most concerning is the variability of the primary outcomes studied. From a conceptual viewpoint, examining sleep/wake circadian rhythms in newly diagnosed breast cancer patients compared with examining rhythms of melatonin, cortisol, and rest/activity in patients with colorectal cancer metastases cannot be easily interpreted or generalized.
In summary, while the majority of articles included homogeneous patient populations, lacked consistency in defined terms and measures, and had small sample sizes, key findings demonstrated clinically relevant and salient findings to form a valid platform for the continuation of this area of investigation.
Conclusions
A growing body of literature suggests that patients with cancer suffer from a variety of physical, affective, and cognitive symptoms either directly or indirectly from the cancer or its treatment. The management of cancer-related fatigue is an important and challenging problem for patients and health care providers. Although cancer-related fatigue is pervasive and distressing, our lack of understanding its underlying etiology has greatly hindered our efforts to develop and test interventions targeted at mitigating levels of fatigue in patients with cancer.
Evidence suggests that stress associated with the diagnosis and treatment of cancer may cause circadian rhythms to become disrupted and that altered circadian rhythms are likely associated with symptoms related to cancer and/or treatments such as fatigue. Recognizing the significance and critical regulatory function of circadian rhythms may be the catalyst needed to initiate the development and testing of interventions that may prevent or restore balance within the context of symptoms sensitive to disrupted circadian rhythms. As new developments occur in this area of scholarly work, application of research findings may translate into developing and testing tailored therapeutic interventions for cancer-related fatigue and the related symptoms of sleep disturbances and psychological distress.
Footnotes
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.