
Abstract
Oxygen is one of the important factors for wound healing and infection control. The revascularization procedure is amended to correct the tissue hypoxia problem by increasing the blood flow to obtain an adequate amount of oxygen. Hypoxic wounds are still the issue in the cases of unsuccessful or incomplete revascularization. The issue needs to be clarified and confirmed by proper methods for management to achieve wound healing and prevent limb loss. Oxygen therapy may benefit in the case of remaining hypoxia or wound infection in postrevascularization.
Keywords
Tissue hypoxia is the main factor that impedes wound healing in peripheral vascular disease (PAD) patients with chronic ulcers. The decrease or abrupt of the inflow of oxygenated blood perfusion is caused by vascular abnormalities like stenosis or occlusion. Revascularization to return blood inflow perfusion to the ischemic area is considered the mainstay of treatment in critical-threatening limb ischemia (CLTI), especially in those presented with wound and tissue loss. The goal of the treatment operation is achieving the hemodynamic correction of the blood flow to the problem area by any efforts for the anatomic correction of pathologic vessels by open-bypass surgery or endovascular method. 800 per 100 000 of the world population reported suffering from CLTI with 70% treatable by revascularization 1 and the population trend is increasing. 2 Complete ulcer healing rate after revascularization reported 70% to 80%.3‐5 Persistent microcirculatory deficit was one of the causes of unfavorable ulcer healing outcomes after the operation, especially in indirect revascularization.6‐8 Angiosome or wound perfusion targeted revascularization concept initiated to solve it, especially in diabetic CLTI. 9 Ischemic-reperfusion injury affects the environment of peri-ulcer tissue with a higher level of local inflammation level from reactive oxygen species substances after an abrupt increase of the blood flow to the ischemic area after successful revascularization.10,11 Injury to the cells of the affected area is a mandatory phenomenon presented with an ischemic turn to necrosis of the transitional area and silence local infection in a diminished oxygen state flaring up more overt from septic thrombosis of small vessels and escalating growth of bacteria in reestablish oxygen environment in the early postprocedural period. 12 Huge a higher need for oxygen consumption of tissue and cells to combat microorganisms compared with the normal healing process in an infective state of the wound. 13 This makes wound infection a strong factor in delayed wound healing and limb loss in postrevascularization if it is not well managed.6,8,14,15
Oxygen therapy should be considered one of the necessary supporting factors for the wound to accelerate healing in any of the postrevascularization wounds that proved or suspected with persistent hypoxic state or demonstrate any signs, symptoms, or evidence that are interpreted as wound infection.
Role of Oxygen in Wound Healing
Adenosine triphosphate (ATP) is the main source of life. Oxygen is one of the essential components of cellular ATP production, especially in the oxidative phosphorylation process of the mitochondrial respiratory chain. 16 Thirty-six to thirty-eight ATPs were produced in normal cellular oxygen levels compared with 2-4 ATPs in hypoxic conditions. The gap of energy shortage impairs a general physiologic cell function.
Oxygen plays a crucial role in all phases of wound healing. The normal defense mechanism of our body to combat foreign bodies in open skin defects like microorganisms by white blood cells (WBCs) depends on an adequate amount of oxygen. 17 The temporary hypoxic state of affected tissue is a physiologic response of the inflammatory phase of wound healing. This is the consequence of the imbalance of the surge of oxygen consumption of immune cells and the impairment of oxygen supply from the diffusion defect of edematous tissue in the postinjury response resulting in a transient hypoxic environment of the affected area. This state induces hypoxia-inducible factors (HIF) signaling pathways that stimulate macrophages, B-cells, and T-cells’ action for effective action of bacterial, foreign bodies, and dead cell eradication. 18 A chronic hypoxic state repeating this action of WBCs turns the active immunologic response into exhaustion and can lead to susceptibility to infection problems. Prolonged inflammation will end up in the ineffective process of bacterial and necrotic cell clearance.
The normal proliferation and migration of keratinocytes and fibroblasts require normal oxygen concentration. 19 A low level of oxygen environment increases angiogenesis in the acute period but lowers the production of new formation of cells and vessels in the long term.20‐22 Collagen production and hydroxylation were disturbed in the hypoxic wound base. 21 Delayed epithelization and poor quality of wound granulation are the outcomes of retard of the proliferative phase. 23 Maturation cannot be achieved due to the slow progression of cells and extracellular matrix proliferation and formation. In terms of scar, hypoxic conditions lead to higher collagen type I and lower collagen type III production. 22 Worse scars present as a complete wound healing in case of achieved healing. Hypoxia can cause abnormalities in all phases of wound healing as seen in Table 1.
Effect of hypoxia on wound healing.
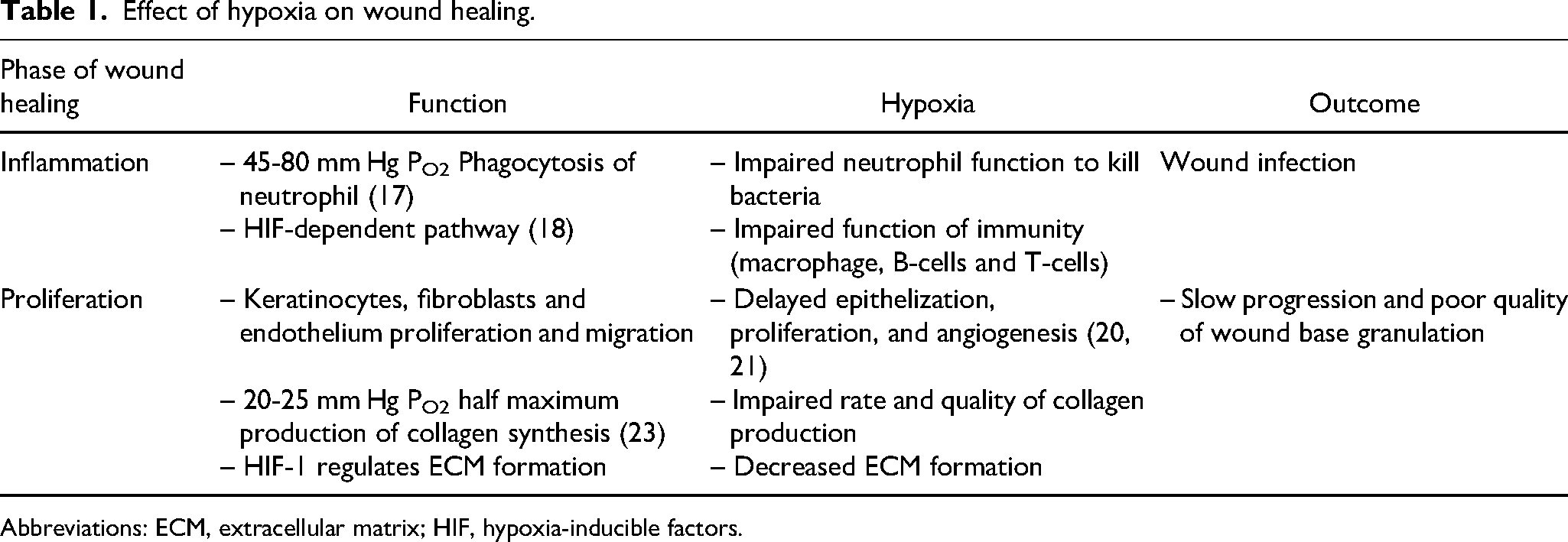
Abbreviations: ECM, extracellular matrix; HIF, hypoxia-inducible factors.
Evaluation of Perfusion or Oxygenation Status of Postrevascularization Wounds
Limb perfusion at the macrovascular level can be assessed by pre- and intraoperative radiological studies. Restore anatomic abnormalities and the blood flow at the macrovascular level might not be a good predictive factor for complete wound healing especially in diabetic and end-stage renal failure patients whose pathophysiology was generalized to all levels of vessels involved.24,25 The evaluation of collateral vessel perfusion is one of the areas that is limited in data. Most microvascular perfusion assessments are performed in indirect method measurement and with limitations of studies with patients with poststenting, postbypass graft, or wound lesions. Impairment of microvascular flow to the wound implies a wound hypoxic state which might benefit from oxygen therapy.
An increase in ABI ≥ 0.23 or an increase in TBI ≥ 0.21 was reported independently association with wound healing in 218 CLTI patients (HR: 1.87; 95% CI [1.12, 3.15]; P = .018), (HR: 1.63; 95% CI [1.02, 2.59]; P = .039) respectively. 26 Acceptable an increase in ABI ≥ 0.15 is used in clinical practice as a marker of successful revascularization27,28 might not be a good cut point in predicting wound healing. The comparison study of the correlation of ABI with microcirculation postrevascularization in a small CLTI population (n = 26) showed a negative result. 29 The information on using ABI and TBI as noninvasive microvascular perfusion monitoring is lacking. The current data is based on small population information.
Transcutaneous oxygen tension (TcPO2) measurement is reported more sensitivity and specificity to evaluate micro perfusion than immediate postoperative ABI.30,31 TcPO2 less than 20-30 mm Hg predicted a lower ulcer healing rate in ischemic ulcers.32‐34 This cut-point value was studied to predict ulcer healing for trigger intervention purposes but did not provide strong concrete evidence enough for postprocedural monitoring. TcPO2 > 40 mm Hg can predict wound healing outcomes in the group that underwent the procedure. 35 Unclear issue with the optimum time for using this measurement in postrevascularization wound monitoring. The formation of collateral vessels in the wound is believed to occur in 2 weeks making TcPO2 not a good intraprocedural parameter compared with systolic toe pressure. 35 Previous studies reported a peak increase of TcPO2 at 4 weeks postoperative period and stable at 6 to 8 weeks.31,36‐38
Skin perfusion pressure (SPP) is one of the good noninvasive measurements of skin microcirculation using laser Doppler, radioisotopes, or photoplethysmography. Calcified vessels are not affecting the SPP. 39 The cutoff value is still in debate with 30 to 50 mm Hg.40‐42
Intraoperative wound blush obtainment is one of the good independent predictors of wound healing. Previous studies showed higher wound healing and limb salvage rates in the wound blush group.43‐45 The intraoperative negative wound blush group may need to consider direct or indirect revascularization or the number of visible functioning arteries that can provide blood flow to the ulcer, significantly below the knee level CLTI. Indirect single functioning below the knee artery might be considered inadequate microcirculation of the wound. Microcirculation flow or tissue oxygenation status should be more investigated.
Postprocedure wounds with evidence of impaired microcirculation perfusion or with signs of wound infection might benefit from oxygen therapy. In our center's experience, vascular surgeons will not routinely measure a wound's blood perfusion or oxygenation that intraoperatively successful procedure achieving direct wound blushing or direct 2-functioning of below the knee level vessels. In the postoperative cases that obtained partial flow with no wound blushing with indirect single-functioning vessel to the wound or doubted with blood supply to the wounds are investigated in perfusion or oxygenation in 2 to 4 weeks which depends on how good or bad the wound clinical progression.
Options for Oxygen Therapy
Oxygen support in wound treatment is classified into local and systemic therapy. The systemic treatment needs the adequate function of the respiratory and cardiovascular systems to supply oxygen to the target cells. At atmospheric pressure, tissue and cells get oxygen from oxyhemoglobin in red blood cells (RBCs) transported via the blood vessels from large to small into the capillary nest. RBCs act like big trucks carrying and transporting oxyhemoglobin to the destination as many tissues and cells. The successful shipping of oxyhemoglobin will need good quality roads that are our blood vessels. At the target tissues and cells, oxyhemoglobin will release oxygen to the cells via diffusion effect. PAD patients referred to the blockage of the blood vessels while shipping oxygen on the processing limited type of vehicle that can be used. Five liters of total blood plasma volume in an adult weight of 70 kg running all around our body can carry very few amounts of oxygen at seal level height in our daily life.
Hyperbaric oxygen therapy (HBOT) provides a high concentration of oxygen to the target tissues and cells by application of high pressure to increase the dissolution capacity of oxygen into the blood plasma. Under the pressure of 3 atmospheres absolute with 100% oxygen concentration breathing, the combined blood oxygen content in whole blood reaches 23.0 mL O2/dL from 16.2 mL O2/dL in a daily environment (21% oxygen concentration, sea level with 12 g/dL of hemoglobin concentration). 46 This 42% of additional plasma oxygen can replace the function of hemoglobin for oxygen transporting made HBOT can be used as a bridging treatment for severe anemia patients as one of the indications of HBOT treatment by the Undersea and Hyperbaric Medical Society. 47 The high oxygen concentration in blood plasma runs to all areas of the body and supplies oxygen to the cells by diffusion effect even in low blood supply area or too small intravascular diameter for RBCs to travel past that caused by the severe stenosis of the blood vessel. HBOT can provide oxygen to correct the hypoxic state that activates many cells, substances, and enzymes to resume their functions. The elevation of cellular oxygen level increases the amount of reactive oxygen and nitrogen species (ROS and RNS). These complex particles activate many mechanisms that promote the phases of wound healing by modulation the function of WBCs, improving inflammation, and increasing growth factor synthesis. Moreover, ROS and RNS activate peripheral mobilization of stem or progenitor cells from bone marrow to the affected area to ameliorate the neovascularization pathway. 48 Infection and biofilm are related factors in the delayed healing of chronic wounds including postrevascularization wounds. An optimum supply of oxygen facilitates WBCs’ antimicrobial function to eradicate organisms effectively directly and hyperoxia conditions provide chemical biomodulation for antibiofilm effect and synergistic effect of antimicrobial medication.49,50 Limit direct evidence of the study to support the benefit of HBOT on postrevascularization wound healing. One of the well-conducted multicenter randomized clinical trials of HBOT in diabetes with ischemic lower extremities ulcer (DAMO2CLES) by Santema et al published in 2018 concluded that the additional HBOT provided no significant effect of improving wound healing with trending in lowering of major amputation index. 51 This study included 71 postrevascularization ulcers with the confirmed moderate ischemic condition by an absolute ankle systolic blood pressure < 70 mm Hg or an absolute toe systolic blood pressure < 50 mm Hg or a forefoot transcutaneous oxygen pressure (TcpO2) < 40 mm Hg, 33 ulcers in the controlled arm, and 38 ulcers in the HBOT arm with nearly half (62 of 120 patients) of the study population with Wagner grade II ulcer. The result of this study cannot provide a concrete conclusion of the benefit or uselessness of HBOT on postrevascularization ulcers in the non-DM population and in the DM group from too small of a sample size.
The limitations and contraindications of the pressure effect and HBOT itself prevented many PAD patients from receiving treatment. Most of them are fragile hosts with multicomorbidities that are unfit to tolerate the systemic physiologic change from the hyperbaric chamber. Local HBOT treatment is the new treatment for diabetic foot ulcer (DFU) and venous leg ulcers first published by Pasek J. et al in 2022 and 2023.52,53 It reported promising results in wound area and pain reduction. However, the data on this new treatment in postrevascularization ulcers is unavailable.
Topical oxygen therapy has many groups like providing oxygen gas directly to the wound surface by oxygen generator device, agents, or compound chemical dressing that release oxygen or its radicals after exposure to wound exudate and hemoglobin spray increasing the oxygen carrier capacity through wound exudate from surface to wound base.
Tang TY et al conducted an observational clinical trial on chronic DFU with an oxygen generator device (NatroxTM) reported >75% of wound closure with pain reduction. 54 The mean TcpO2 of the population in this trial is 34.1 ± 19.6 mm Hg with 18 of 20 patients having a history of previous endovascular revascularization procedure treatment. There is no control group to compare in the result. So, the benefit of this device on postrevascularization wound treatment is inconclusive.
Hunt and Elg studied the clinical effectiveness of hemoglobin spray (Granulox®) in chronic DFU treatment resulting in significant wound closure, wound size reduction, and pain. 55 This study excluded patient who needs to be treated with revascularization without mentioning a history of the previous revascularization procedure. The benefit of hemoglobin spray in postrevascularization ulcers is still lacking in information.
Discussion
Oxygen is a vital component in all phases of wound healing, alleviating the process of eradicating microorganisms for infection prevention and breakage of biofilm.18‐22,48‐50 The revascularization procedure's purpose is to optimize the flow of blood perfusion to provide an adequate amount of oxygen for normal cell function. Some patients may not achieve a successful outcome from the increased flow operation and remaining hypoxia.
The method to identify hypoxia state is no gold standard and the timing to measure is still in doubt. Mostly of physicians will wait for 2 to 6 weeks or till clinical run down to clarify these issues in postrevascularization cases. This area of interest is still in land that needs more study to confirm the method and timing.
The evidence of oxygen therapy in postrevascularization ulcers is limited and mostly is not of good quality. Based on limited evidence HBOT trends to lower major amputation rates without evidence of the benefit of wound healing. For the local oxygen therapy option, further study needs to be followed to conclude the benefit.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.