
Abstract
Ingrown toenails are a common reason for referral to orthopedics and podiatry clinics. Recurrence and infection are common complications in ingrown toenail surgery. This study investigates the effect of an electrocautery matrixectomy on the recurrence and clinical outcomes in the Winograd technique applied in ingrown toenail surgery and whether prophylactic antibiotic use is necessary for these surgeries. One hundred forty-three patients who underwent surgery for ingrown toenails were analyzed retrospectively. Eighty-two patients underwent the Winograd procedure with electrocautery matrixectomy, whereas 61 patients underwent the Winograd procedure. While 78 patients were given prophylactic antibiotics, 65 patients were not. Patient satisfaction was evaluated with a surgical satisfaction questionnaire (SSQ). A visual analog score was used to evaluate the pain. Recurrence was observed in 3 toenails in the Winograd and electrocautery groups, while recurrence was observed in 9 toenails in the Winograd group (P = .018). In both groups, there was no statistically significant difference between the infection rates between patients who took antibiotics and those who did not (P > .05). There was no statistically significant difference between the groups in terms of SSQ scores (P > .05). It was observed that the surgery performed had a positive effect on pain, and this effect was statistically highly significant in both groups (P < .05). The outcomes of the present study suggest that the addition of an electrocautery matrixectomy to the Winograd technique in the surgical treatment of symptomatic Ingrown toenails may decrease recurrence rates. Additionally, this study showed that oral antibiotics, when used in addition to Ingrown toenail surgery, do not reduce postoperative morbidity.
Introduction
Ingrown toenails (IGTN) are a common problem that negatively affects the quality of life. Patients often require treatment when symptoms, such as pain, rash, localized infection, and discharge, affect their daily activities. Surgery is a good treatment option in cases where conservative methods fail. 1 Various surgical techniques have been previously described. 1 Although a partial nail avulsion and chemical matrixectomy with phenol are preferred by dermatologists, a wedge resection with a nail matrix destruction (Winograd technique) is still popular, especially among orthopedic surgeons. 2 However, the recurrence rate after the Winograd technique has been reported between 7% and 20%.3,4 Adjuvant methods, such as phenol matrixectomy, sodium hydroxide matrixectomy, laser matrixectomy, CO2 matrixectomy, and an electrocautery matrixectomy, have been reported to reduce these recurrence rates.5,6 While phenol matrixectomies have produced abundant data, there are a limited number of studies on electrocautery matrixectomies.7,8
Another important complication of IGTN surgery is infection. An infection may develop either during the preoperative or postoperative period. Therefore, the use of oral antibiotics as an adjunct to IGTN surgical treatment is widespread and is often touted as an essential component in the treatment process.9,10 However, there are different opinions about the necessity of antibiotic use. It has been reported that prophylactic oral antibiotic therapy before a surgical procedure reduces the risk of developing an infection. 9 Some authors have reported that antibiotic prophylaxis before or during a phenol matrixectomy reduces the risk of developing an infection. 11 Others have stated that a localized infection will resolve after the IGTN removal without the need for antimicrobial agents.12–17 Therefore, antibiotic use as an essential component of IGTN treatment remains controversial. 18 Also, there is no consensus on the necessity of antibiotic prophylaxis in other dermatological surgeries. 19
For these reasons, our study sought to answer 2 questions. (1) Does the addition of an electrocautery matrixectomy to the Winograd technique influence the clinical results? (2) Is it necessary to use antibiotics in the perioperative period in patients with IGTN?
The aims of this study were to investigate the effect of an electrocautery matrixectomy on the recurrence and clinical outcomes in the Winograd technique applied in IGTN surgery and whether prophylactic antibiotic use is necessary for these surgeries.
Materials and Methods
Study Design
This study was a retrospective study of adolescents and adults who underwent the Winograd procedure 20 with or without electrocautery matrixectomy 8 for IGTN. The local ethics committee approved the study. All patients were informed about the surgical treatment and written informed consent was obtained for the intervention. In addition, the patients were informed that the medical results of each patient could be used for scientific purposes, and their consent was obtained.
Patients
Patients who applied to our outpatient clinic due to IGTN between 2011 and 2020 were analyzed retrospectively. There were 143 (45 females, 98 males) patients who underwent the Winograd procedure 20 with or without electrocauterization 8 procedure who were included in the study (Figure 1). All patients were followed up for at least 3 months after surgical treatment. No exclusion was made based on age. The main complaints were a pain in the big toe, discharge, difficulty wearing shoes, and deformity of the nail. Heifetz staging was used for classifying the IGTN. This staging system comprises 3 stages; stage 1 is characterized by edema of the nail fold on the sides, erythema, and curling of the nail fold into the nail bed. With stage II, there is a discharge with an acute and active infection. Stage III entails a chronic infection, granulation tissue around the nails, and hypertrophy of the surrounding tissues. 21 Exclusion criteria were patients with peripheral artery disease, diabetes mellitus, and those using oral anticoagulants.
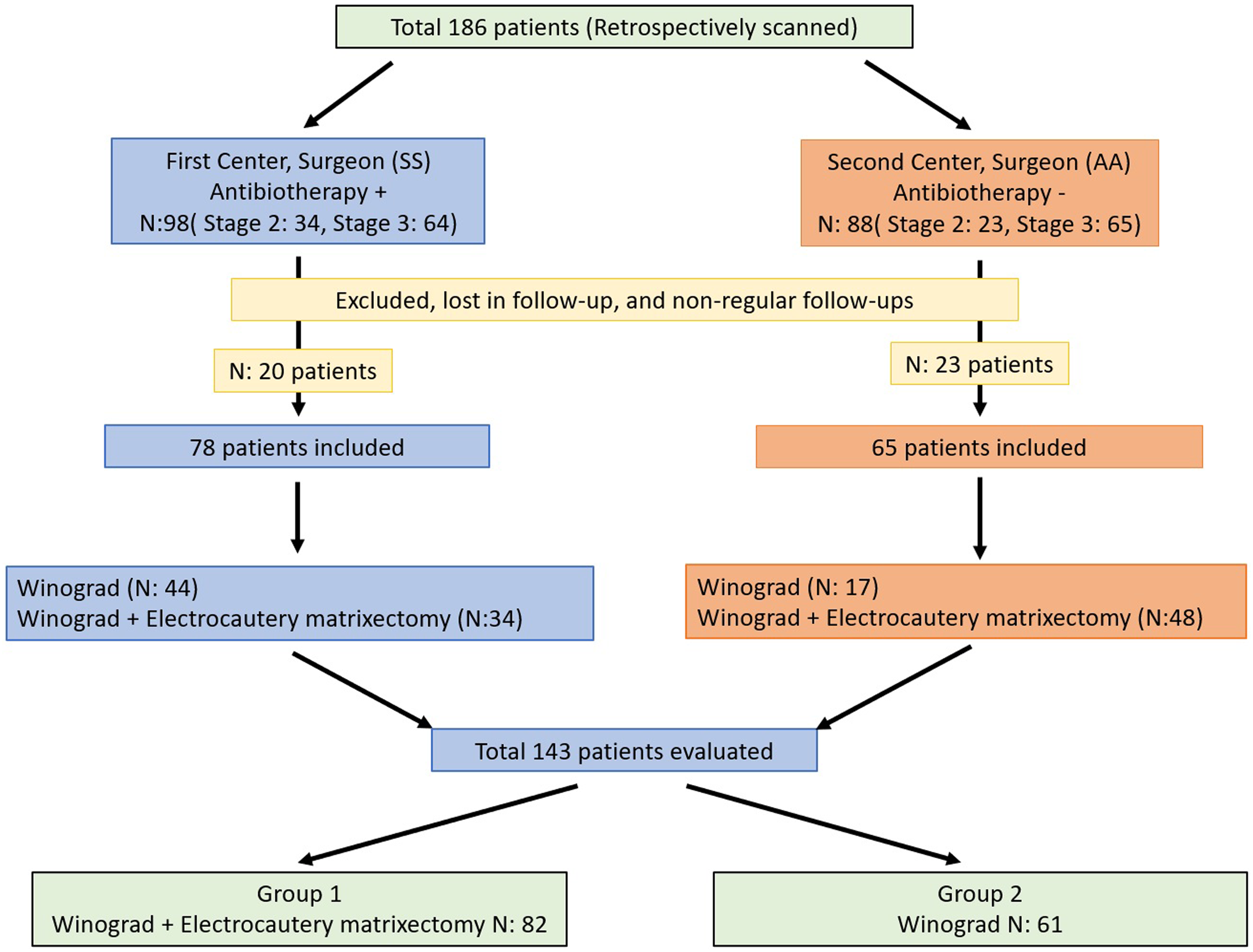
Flowchart of cases.
Surgical Procedure and Groups
All surgical procedures were performed in the outpatient department using standard methods. The Winograd procedure, 20 with or without electrocautery matrixectomy, 8 was performed by 2 different surgeons (SS, AA) in separate centers. The surgeons were experienced surgeons who had done many ingrown toenail treatments and had academic publications.25,26 To compare the effect of an electrocautery matrixectomy on recurrence, the patients were assigned to 2 groups as Winograd + electrocautery matrixectomy (Group 1, n: 82) and Winograd only (Group 2, n: 61). While the surgeon in 1 center applied routine pre- and postoperative antibiotic therapy to his patients in addition to the surgical treatment in daily practice, the surgeon in the other center did not administer antibiotic therapy. On the other hand, surgeons at both centers used both surgical techniques (Matrixectomy alone or Matrixectomy + Electrocautery). Which technique would be chosen for which patient was determined after the patients were informed in detail: the stage of the disease, the preference of the patient (primarily) or the surgeon. To evaluate the effect of prophylactic antibiotic use, patients were divided into subgroups according to whether they took antibiotics or not. In the first examination, 42 patients were stage II, and 101 were stage III (Figure 2).

(a) Heifetz stage 1 ingrown toenail. (b) Stage 3 ingrown toenail.
Surgical Technique
A povidone-iodine solution was used for asepsis. The big toe was anesthetized using 2 to 4 mL of 1% lidocaine hydrochloride as a ring block (Figure 1). When a pin-prick sensation was lost, a tourniquet was applied. A clamp was placed on the tourniquet to prevent forgetting the tourniquet at the end of the surgery. First, the granulation tissue covering the nail groove was excised (Figure 1). Subsequently, the lateral nail, which corresponded to approximately one-quarter of the entire nail, was cut vertically 5 to 10 mm proximal from the nail skin border to the phalanx using a #15 scalpel tip. Then, starting from the proximal oblique region, using the blade at an inclination of 40 to 45°, the nail, nail bed, and germinal matrix in the area were excised with an incision deep enough to touch the phalanx (Figure 1(b)). During the electrocautery matrixectomy, the germinal matrix was cauterized using unipolar type electrocautery for 2 to 3 s at 40 W (Figure 1(c)). In both types of surgery, the nail beds and hypertrophic tissues of the lateral nail fold were excised according to the shape of the nail, and the residues were cleaned with a curette. The wound was then washed with serum. Wound edges were closed with 3.0 prolene thread. In the antibiotic group, patients were treated with oral antibiotic therapy for 5 to 7 days before and after the intervention with either sodium fusidate (1 500 mg/day) or cephalexin (500 mg/orally every 12 h). The antibiotic chosen was based on its effectiveness against coagulase-negative staphylococci species, especially Staphylococcus epidermis, which is the most frequently cultured pathogen in infected toenails. 22 Surgical treatment was applied to the patients whose wound exudate stopped or continued a little. In addition, surgery was postponed for some patients whose wound exudation did not decrease and/or infection continued despite 5 to 7 days of preoperative antibiotic therapy. Infectious diseases specialist was consulted with the suspicion of resistant and/or mixed infection. These patients were not included in the study.
Mobilization was allowed from the second postoperative day. The patients were seen in the outpatient clinic 2 days after surgery, as well as in the first week, second week, and between 10 and 14 days. The sutures of the patients were removed on the 12th to 14th days. After suture removal, patients were allowed to return to their daily activities. All patients were followed for at least 3 months for recurrence and infection. Recurrence and infections during the follow-up period were noted (Figure 3).
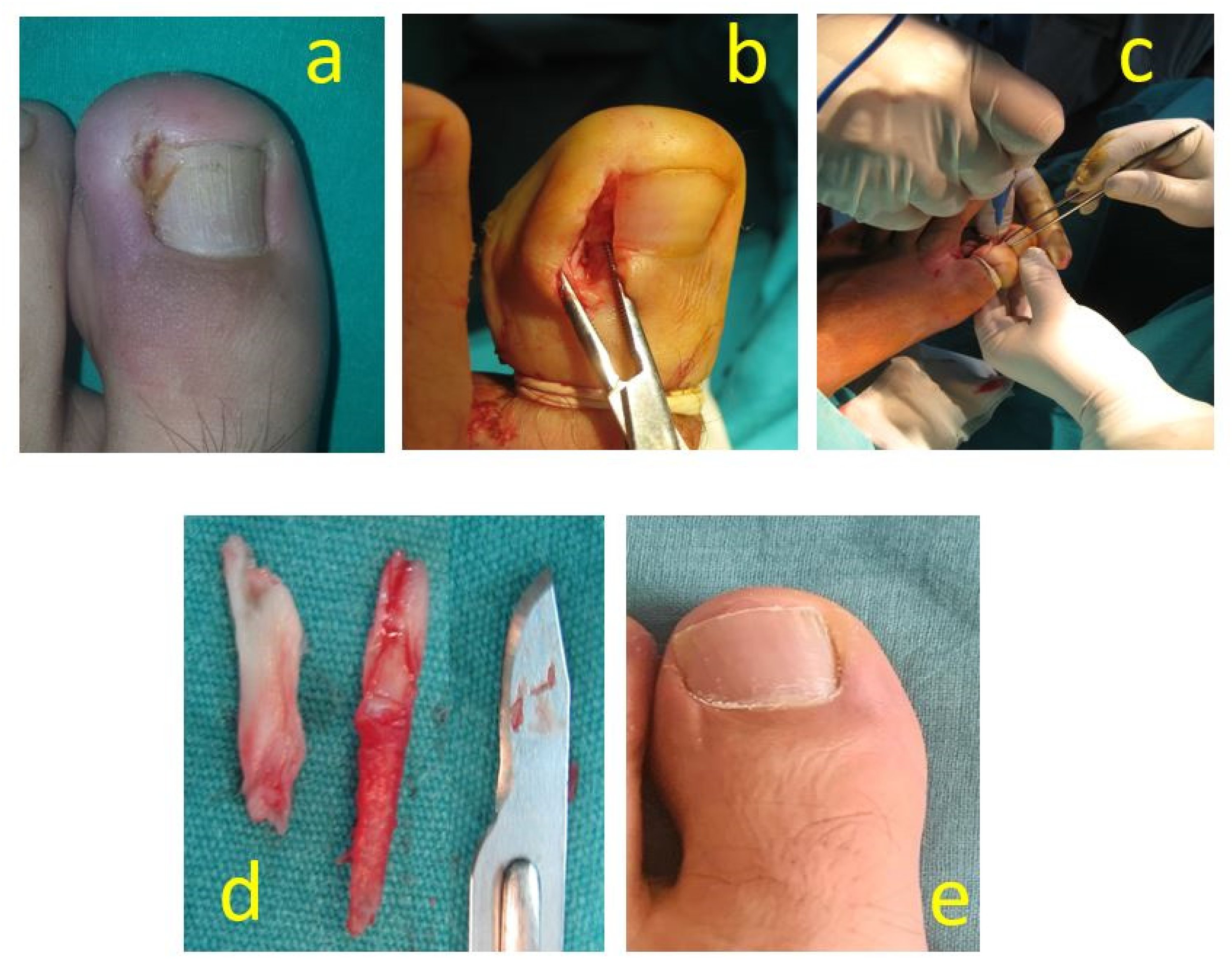
Forty-one-year-old male toe ingrown nail case photos. (a) Preoperative stage 2 toe ingrown nail, (b) intraoperative segmental nail bed and matrix excision, (c) electrocauterization, (d) excised nail and matrix tissue, and (e) postoperative first year.
Outcomes Measures
The surgical satisfaction questionnaire (SSQ) 23 was used to assess the surgical procedure and obtain the patients’ preliminary measurement results. Pain, return to daily activities, cosmetic appearance, and general satisfaction were evaluated using the SSQ (Figure 4). For secondary measurement results, a visual analog scale (VAS) was used. The pain levels of the patients were assessed with the VAS before and after the surgical procedure. For our tertiary results, recurrence and postoperative infection rates were evaluated. VAS scores were evaluated preoperatively and on the 30th postoperative day.
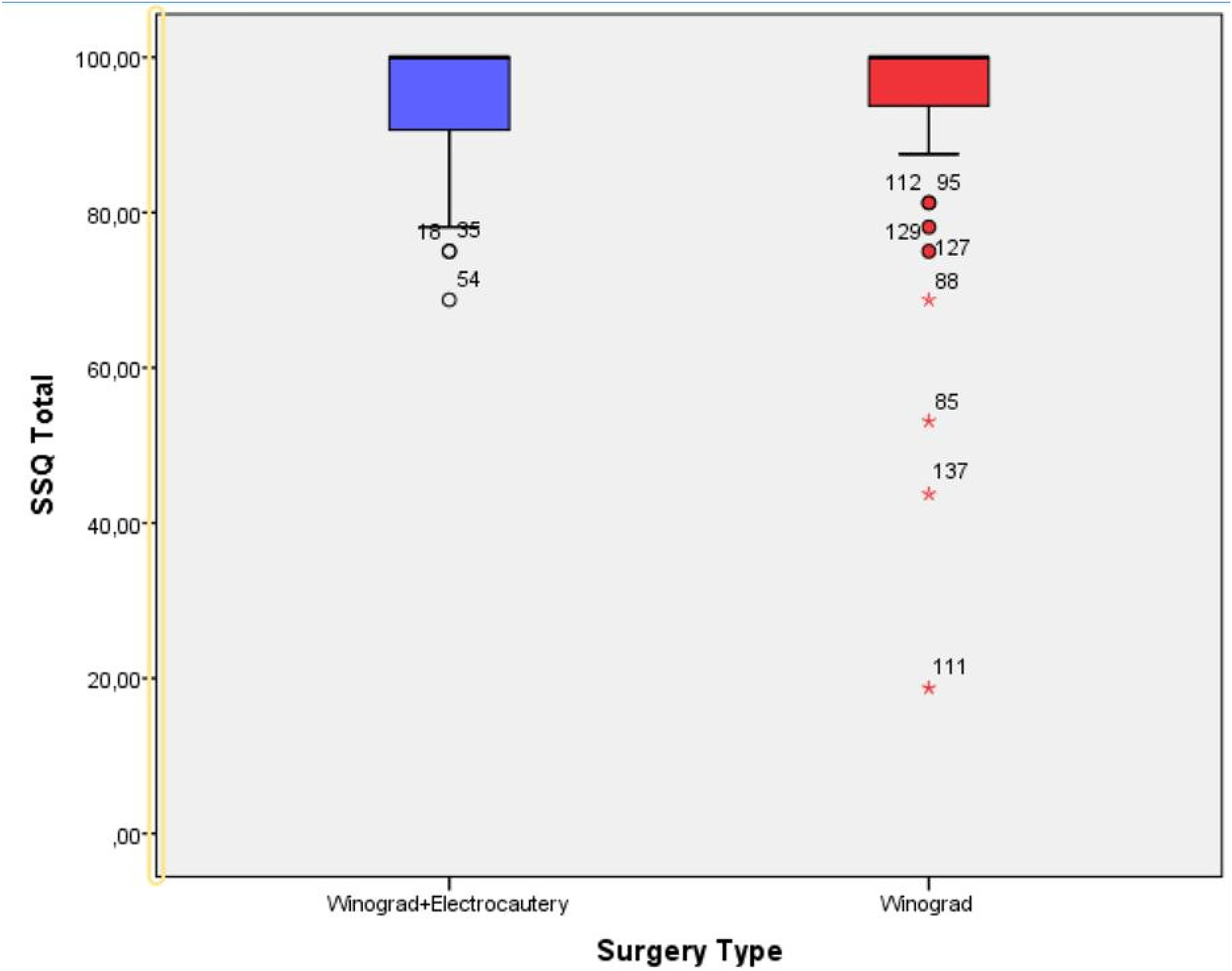
Graph showing surgical satisfaction questionnaire (SSQ) scores of groups.
The SSQ was applied to patients whose last controls were made in the outpatient clinic in the third month. The SSQ consists of 8 items concerning the patient's personal satisfaction with the results of the surgical procedure. The questions were scored with a value of: 4 for “very satisfied”; and 0 for “very unsatisfied.” The mean scores were multiplied by 25. If more than 2 questions were not answered, the questionnaire was considered incomplete. A potential score ranged from 0 to 100. The higher the score, the higher the degree of surgical satisfaction. Items 1 and 2 were used to calculate the pain subscale; items 3, 4, and 5 assessed the return to daily life; and items 6, 7, and 8 evaluated the general satisfaction level. To evaluate the esthetic satisfaction, a question about the appearance of the big toe after surgery was asked, “Are you satisfied with the aesthetic results of the post-surgery nail?” Yes or no answers were recorded.
Statistical Analysis
The SPSS Statistics® 20.0 (IBM Corporation) package program was used for all statistical analyses. Whether the assumption of normality of distributions was achieved was determined using visual graphics as well as appropriate statistical methods. In comparing the 2 independent groups, independent samples t-tests were used for the data with a normal distribution, while the Mann–Whitney U-tests were used for data that did not show a normal distribution. The Wilcoxon sign test was used for the comparison of the 2 dependent groups. Cross-tables were created to evaluate categorical data, and Chi-square tests were used for statistical analyses. Binary logistic regression was performed to identify independent risk factors for recurrence and postoperative infections, and the general and surgical factors, including age, gender, preoperative VAS scores, type of surgery, surgeon's effect, preoperative Heifetz grades, symptom duration, operative time, and prophylactic antibiotic use, were included in the model. A P-value of <.05 was accepted as being statistically significant.
Results
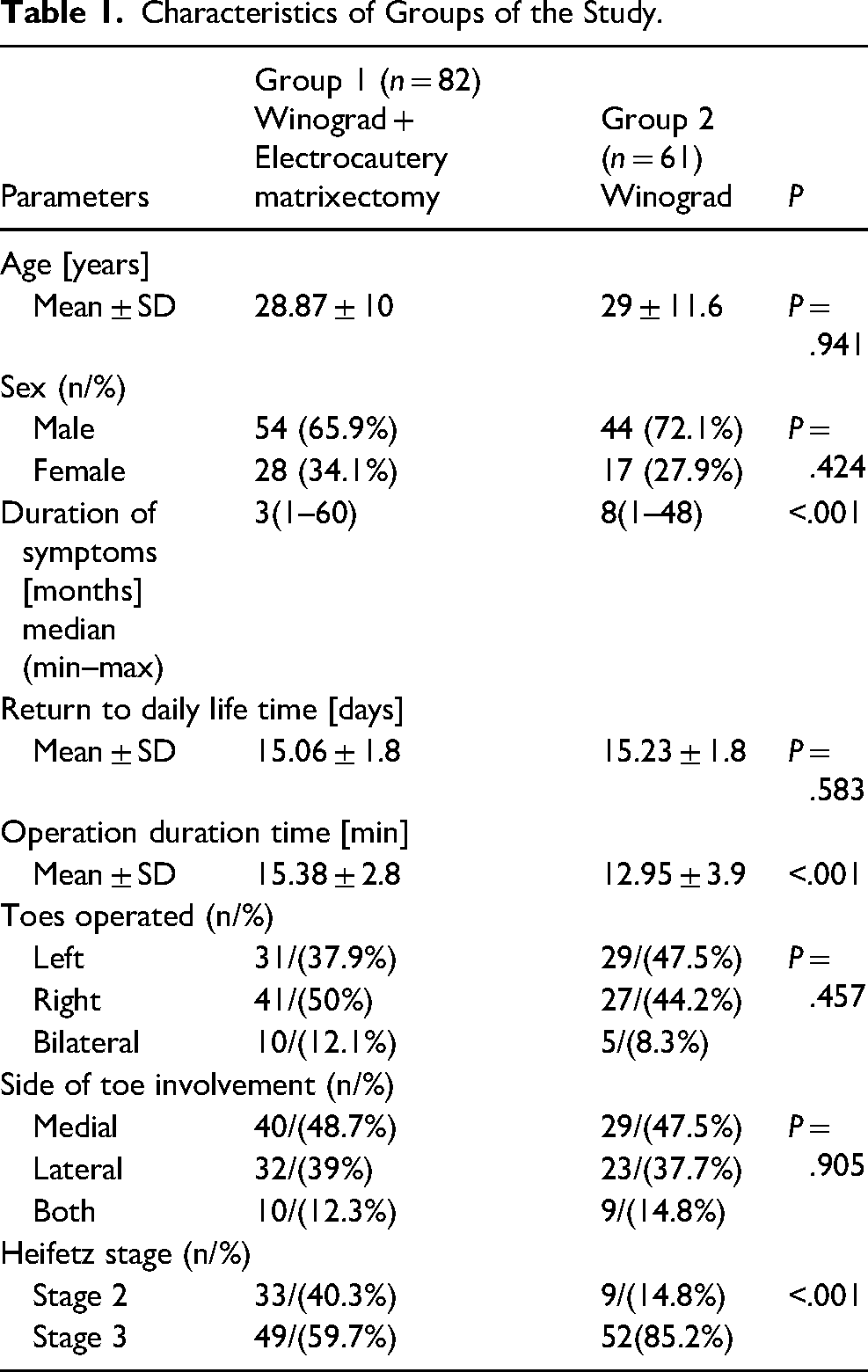
Participants in this study were 98 men and 45 women. The demographic and surgical data of the groups, according to the type of surgical procedure, are given in Table 1. There were no significant differences in sex in either group (P = .424). While the mean age was 28.87 ± 10 years in the Winograd + electrocautery matrixectomy group, it was 29 ± 11.6 years in the Winograd group. Thus, with regard to age, there was no significant difference between the groups (P = .941).
Characteristics of Groups of the Study.
There was a significant difference between the groups in terms of preoperative VAS scores (P < .001; Table 2); however, postoperative VAS scores were not significantly different between the groups (P = .424; Table 2). Alternatively, preoperative and postoperative VAS scores were significantly different for both group 1 and group 2 (P < .001 for both; Table 2).
Outcomes by Groups.
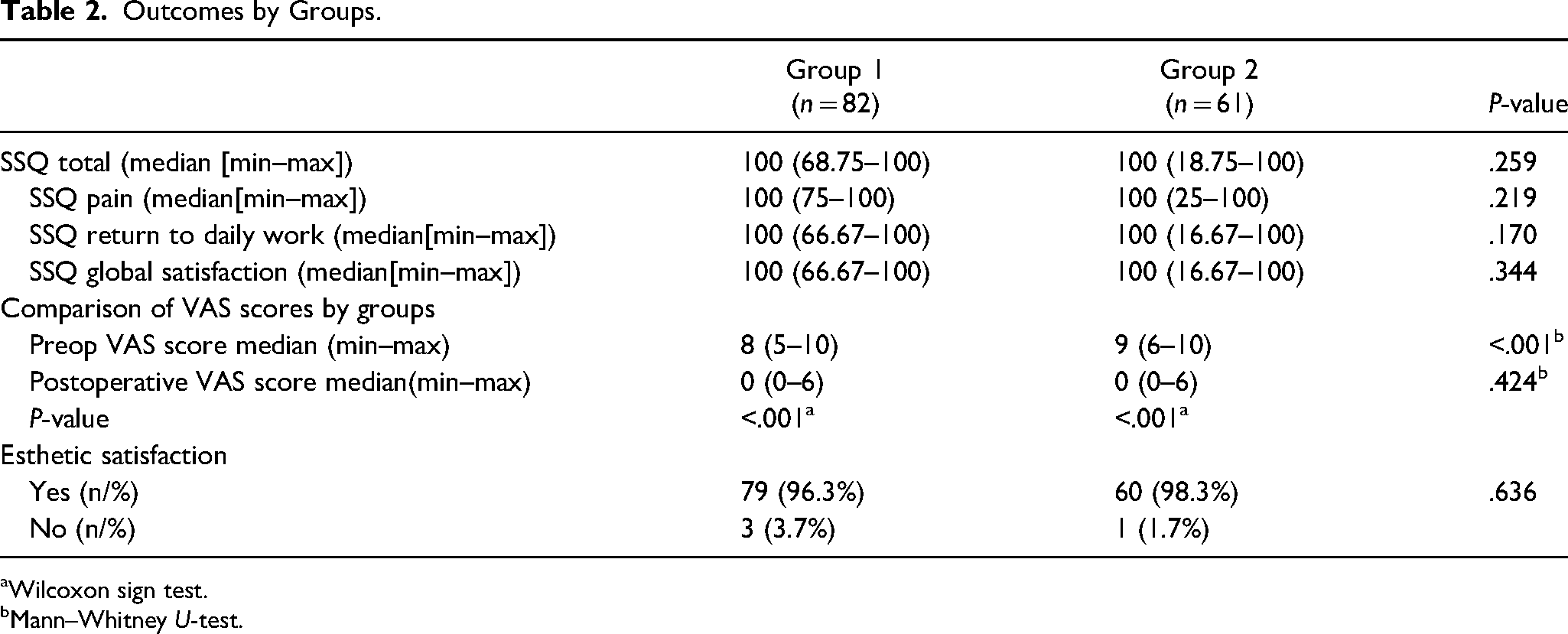
Wilcoxon sign test.
Mann–Whitney U-test.
SSQ scores were determined at the third month evaluation. The median (min–max) SSQ values of both groups were 100 (68.75-100) and 100 (18.75-100), respectively, and the difference between these was not significant (P = .259; Table 2). When the situation was evaluated in terms of SSQ subgroup scores, the SSQ pain scores were 100 (75-100) in group 1, while the postoperative scores were 100 (25-100) in group 2. There was no significant difference between the groups (P = .219). While the SSQ return to daily work score of group 1 was 100 (66.67-100), the score of group 2 was 100 (16.67-100), which was a nonsignificant difference (P = .170). Furthermore, SSQ global satisfaction scores for group 1 were 100 (66.67-100) and not significantly different (P = .344) than that seen in the group 2 postoperative score of 100 (16.67-100). The esthetic satisfaction rates for group 1 and group 2 were 96.3% and 98.3%, respectively (P = .636; Table 2).
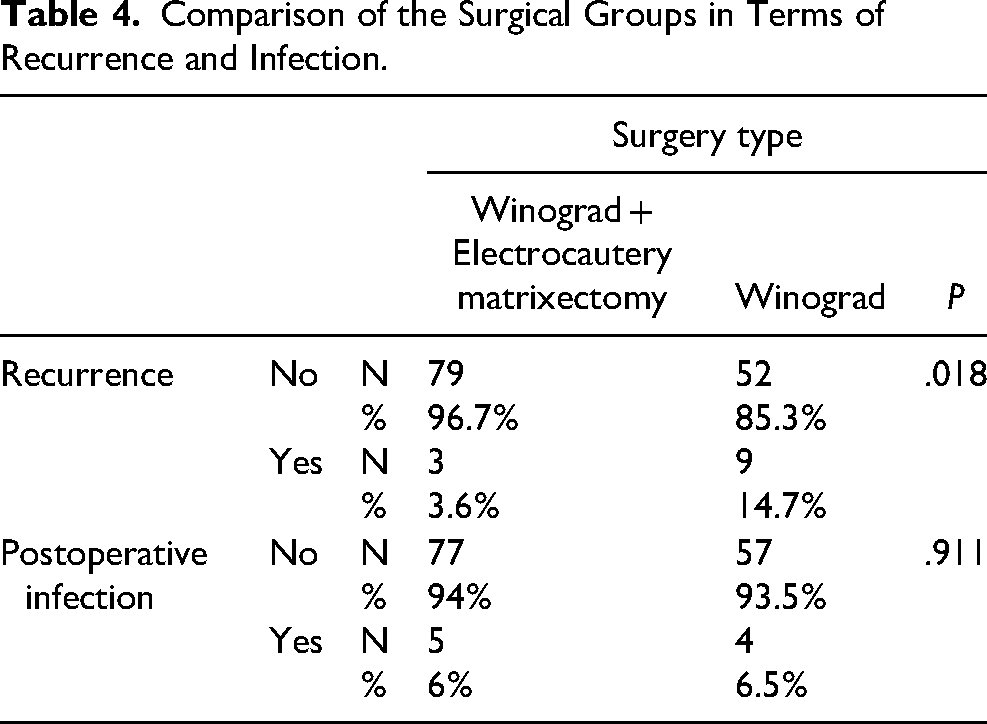
Recurrence was observed in 3 patients in group 1 and 9 patients in group 2. There was a significant difference between the 2 groups (P = .018). Regression analysis was performed to determine the effects of age, gender, preoperative VAS scores, type of surgery, surgeon's effect, preoperative Heifetz grades, symptom duration, and antibiotic use on the presence of recurrence. In the analyses performed, it was observed that the effect of only the type of surgery (P = .045, OR: 4.9; CI 95%: 1.04-23.7) among these variables was statistically significant. It was determined that the effects of age (P = .74), gender (P = .69), preoperative VAS score (P = .65), prophylactic antibiotic use (P = .68), preoperative Heifetz grades (P = .57), duration of symptoms (P = .61) and the effect of the surgeon performing the operation (P = .74) on recurrence was not statistically significant.
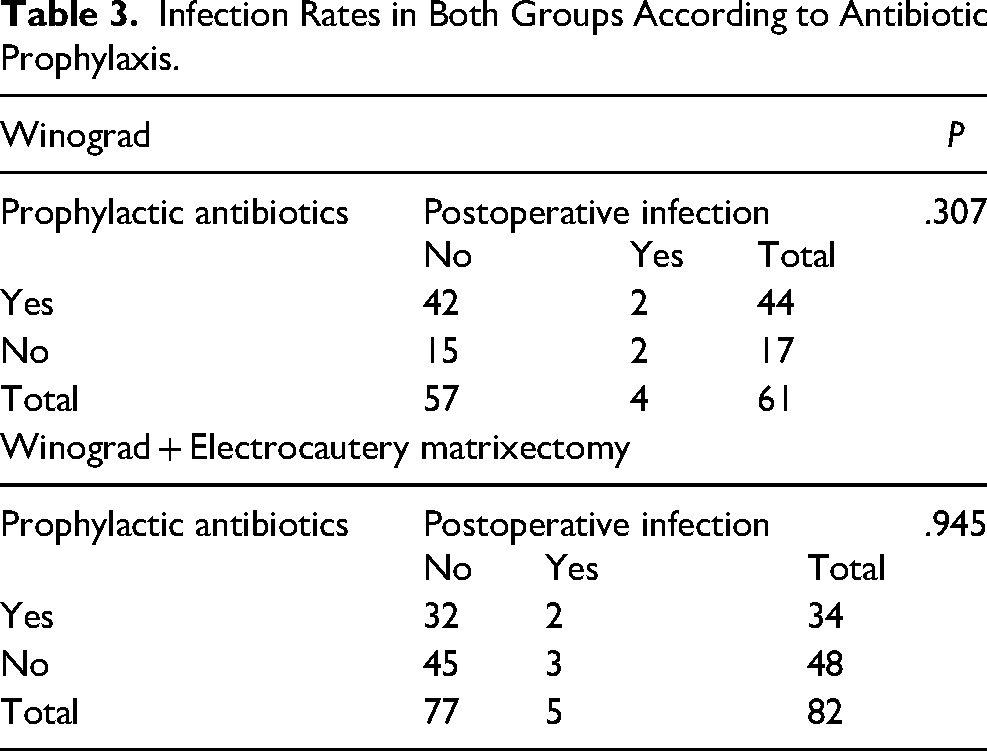
Postoperative infection was observed in 5 patients in Group 1 and 4 patients in Group 2. However, there was no significant difference in postoperative infection rates between the groups (P = .911). Regression analysis was performed to determine the effects of age, gender, type of surgery, surgeon's effect, preoperative Heifetz grades, symptom duration, operation duration, and prophylactic antibiotic use on the presence of postoperative infection. According to the analysis results, age (P = .47), gender (P = .94), prophylactic antibiotic use (P = .60), preoperative Heifetz grades (P = .31), symptom duration (P = .13), operation duration (P = .75) and surgeon's effect (P = .57) were found to have no statistically significant effect on postoperative infection. The patients who developed an infection were treated with appropriate oral antibiotics after the culture antibiogram was performed. All patients recovered smoothly within 2 weeks.
Discussion
The primary results of this study show that the Winograd technique was a very effective method in terms of pain, cosmetics, and the ability to return to work. However, the application of an adjuvant electrocautery matrixectomy with the Winograd technique significantly decreased the possibility of recurrence. An important secondary result of this study was that the use of prophylactic antibiotics in IGTN surgeries had no significant effect on postoperative infection rates. Moreover, high satisfaction rates were found in both groups of patients (Table 2).
Dabrowski and Litowińska 24 applied a nail preserving and suturing technique without a matrixectomy on 54 toenails of 37 patients. They stated their recurrence rate was low, and the satisfaction rate with the SSQ was high (86.4 ± 10.4). In our study, similar results were obtained with a 94.2 ± 11.1% satisfaction rate.
IGTNs, which negatively affect daily activities and social life, are frequently seen between the ages of 12 and 30 years. 25 The mean age in our study was 28.9 ± 10.7 years. Some studies have reported successful results with high efficacy rates, low recurrence rates (∼3.2%), and low postoperative infection rates (4%).15,18,24,26,27 Despite the lack of scientific evidence for the superiority of various techniques, many studies have shown that surgical procedures with substantial nail and matrix preservation are successful. This suggests that it is successful and satisfactory for patients with its low recurrence rate in IGTNs (Table 3).
Infection Rates in Both Groups According to Antibiotic Prophylaxis.
The Winograd technique is a very popular technique among podiatrists for the treatment of IGTNs because of its successful results.3,4 In this study, the recurrence rate after the original Winograd technique was 14.7%. However, the recurrence rate in the electrocauterization group was significantly lower at 3.6% (Table 4). We think this difference is due to the combination of the electrocautery matrixectomy. It is possible that cauterizing germinal matrix residues will have a positive effect on recurrence. Electrosurgical ablation of the nail bed is a highly successful alternative that produces less discharge (Figure 1(c)). 28 Special high-frequency unit matrixectomy electrodes, coated on one-side with a nonconductive coating, can be used to prevent injury to the normal overlying tissue of the proximal nail fold (ie, cuticle) when cutting the nail bed. 8 Similar to our study, CO2 laser matrixectomy also reduces pain, and recurrence. 6 Different recurrence rates have been reported in the literature, which may be dependent on the surgeon's experience, ability and knowledge of nail anatomy. Camurcu et al reported a recurrence rate of 7.9% in their study. 3 Kuru et al 29 reported a recurrence rate of 10.7% in patients who underwent a wedge excision modification of the Winograd procedure and emphasized the importance of complete exposure and excision of the germinal matrix to avoid recurrence. In a similar study in which Köse et al 2 applied the Winograd technique, a 13.2% recurrence was reported. In a study comparing the Winograd method with the sleeve method, there was a recurrence rate of 12% and 10%, respectively. 30 In another study, Ince et al 31 compared the Winograd method with the knot technique and found recurrence rates of 17.7% in the Winograd technique and 2.2% in the knot technique (Table 5).
Comparison of the Surgical Groups in Terms of Recurrence and Infection.
Brief Table About Ingrown Toenail.
Infection rates after IGTN are reported between 3% and 4.2%.32,33 There is some evidence that perioperative antibiotic prophylaxis provides a 50% reduction in infection risk when used with clean surgery. 34 A review by Fernandez et al 16 suggests that for stages IV and V IGTNs, specific antibiotic therapy should be administered with a partial ablation of the nail before surgery until the infection resolves and the process passes to stage II or III. Although postoperative wound infection is a potential complication of dermatological surgery, systemic antibiotic prophylaxis is not necessary for this infrequent complication, except in exceptional cases. Fernandez et al also reported that the disadvantages of antibiotic prophylaxis, such as increased cost, adverse drug reactions, antibiotic resistance, and drug interactions, should not be ignored, and they do not recommend the use of preoperative antibiotic prophylaxis in IGTN surgery, except in selected patients with infection. 16 Moreover, a Cochrane review revealed that antibiotic use did not make a difference in infection rates. 35 Few studies have investigated the effect of antibiotic therapy in surgery. Heidelbaugh et al 14 suggested that if a partial nail avulsion is performed in the early stages of IGTN, the localized infection can resolve spontaneously without the need for antibiotics. Bos et al 15 questioned the necessity of perioperative antibiotic treatment in surgeries performed even in the presence of an IGTN infection. They recommended not using prophylactic antibiotics for various reasons, including side effects, cost-effectivity, development of resistance, and drug interactions. They also stated that general recovery and the time required to return to work is ∼2 weeks. The results of these studies support our results. In our study, the average time needed to return to work was 15.1 ± 1.9 days, similar to previous reports. So, the use of antibiotics associated with nail surgery treatment has not been established. Scientific evidence for oragainst antibiotic use in surgical treatment to improve the pathology's clinical course is weak.16,17 Also, there is no consensus on the necessity of antibiotic prophylaxis in other dermatological surgeries. 20 Therefore, antibiotic use as an essential component of IGTN treatment remains controversial. Reyzelman et al randomly allocated 154 patients into 3 groups and reported that the use of oral antibiotics as an adjunct therapy in the IGTN treatment did not play a role in reducing the healing time or postoperative morbidity. 18
We could not find a similar study in the literature to compare to our study in a one-on-one comparison. Many studies have reported that the Winograd procedure is satisfactory in the surgical treatment of IGTNs.36–39 However, there are aspects that make the current study different from previous studies. For instance, we investigated the effect of an electrocautery matrixectomy on recurrence in addition to the Winograd technique, and we also investigated the effect of perioperative antibiotics on infection.
The limitations of our study include its retrospective nature, nonrandom election of the surgery type, there was no research in terms of bacteriological and fungal infection in patients other than postoperative infections, and we had a limited number of cases. Also, there may be advantages or disadvantages in terms of treatment outcomes in multicenter studies. Comparison of different treatment practices, different sample groups can be considered as an advantage. On the contrary, it may create a disadvantage in terms of factors such as surgical treatment technique choice, and antibiotic use. These can create proportional differences between groups. This may have caused a disadvantage in terms of the number of patients who used the modified technique or were given antibiotics. The situation that caused this disadvantage may have affected our results.
The results of this study show that the addition of an electrocautery matrixectomy to the Winograd technique in the surgical treatment of symptomatic IGTNs may decrease recurrence rates. Additionally, this study showed that oral antibiotics, when used in addition to IGTN surgery, do not reduce postoperative morbidity. Likewise, it did not affect patient satisfaction. We think this may have important implications for future IGTN treatment protocols. In the age of healthcare management, where costs are essential, and more importantly, in terms of antimicrobial resistance, it can be considered that prophylactic antibiotics are not necessary for IGTN surgeries.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
The study is conducted with adherence to ICMJE criteria. The study was approved by the local ethics committee. (Approval Number: 10354421-2020/24-6).