
Abstract
Little is known about whether and how to treat mental images of childhood ritualistic sexual and physical abuse, which may include bizarre elements. Patients experiencing disturbing mental images of childhood ritualistic abuse pose a significant clinical challenge due to the lack of clear treatment guidelines. To advance the understanding of therapeutic options for such complex cases, we present a case study of a highly fantasy-prone middle-aged woman experiencing intrusive images of bizarre ritual abuse, which were treated using Imagery Rescripting (ImRs). These images had not been successfully addressed in previous treatments. The patient underwent 14 sessions of ImRs, during which symptoms of posttraumatic stress disorder (PTSD; assessed with the PCL-5), emotional tolerance, mastery over the images, and feelings of guilt were monitored. Pre- and post-treatment assessments included the CAPS-5 interview for PTSD. A semi-structured interview was conducted six months after treatment to assess the patient’s experience. Results showed a reliable reduction in PTSD symptoms, increased control over the images, improved emotional tolerance, and decreased guilt. No adverse effects, such as the creation of new images, were observed. We discuss the implications of these findings in the context of current knowledge about the treatment of childhood ritual abuse-related imagery, explore clinical principles, and offer recommendations for further implementation.
Theoretical and Research Basis for Treatment
Mental Images of Ritual Sexual Abuse
Patient reports of intrusive mental images about ritual sexual abuse pose several challenges for researchers as well as clinicians (Hendriks et al., 2023). Ritual abuse involves acts of sexual sadism carried out in groups against children. It includes bizarre forms of sexual abuse combined with macabre elements, such as extreme physical violence and threats (Nierop & van den Eshof, 2008). The credibility and validity of reports of mental images of ritual sexual abuse are the subject of scientific and clinical debate, particularly because of the bizarre elements, the lack of evidence for the occurrence of such events, and because the reports often ‘grow’ or expand over time (Nierop & van den Eshof, 2008). When confronted with this type of reported mental images, clinicians can draw on more general guidelines for dealing with mental images, as discussed in national professional codes of conduct. For example, the Dutch Professional Code of Psychotherapy (Nobel et al., 2018) includes a statement that what patients refer to as ‘memories’ may or may not be an accurate representation of reality. Therefore, psychotherapists are warranted to discuss the differentiation between ‘memories’ and reality with their patients.
Additional challenges are that clinical studies on the treatment of intrusive mental images about ritual sexual abuse are not available and that specific treatment guidelines are lacking. These challenges were made explicit in a study conducted at the request of the Dutch government, in which clinicians (N = 11) were interviewed about the barriers and facilitators to adequate treatment of patients with mental images of ritual sexual abuse. These clinicians expressed that lack of knowledge was one of the key factors in offering treatment to this group of patients (Hendriks et al., 2023). The purpose of the current study was to advance the understanding of treatment options for these complex cases.
Considerations in Treating Patients with Mental Images of Ritual Sexual Abuse
The debate about images of ritual abuse is closely related to the so-called “memory wars,” a scientific debate about whether memories of abuse can be fabricated (Battista et al., 2023) and what interview or psychotherapeutic techniques may encourage the formation of false memories. Research has shown that all types of psychotherapy stimulate memory retrieval and contribute to the reinterpretation of past events. Attempts at memory retrieval can also result in the distortion of existing memories and the creation of new mental images, especially when imagery based techniques are used (Gezondheidsraad, 2004, p.106; Herndon et al., 2014; Loftus, 1994). Offering treatment for mental images that include bizarre elements may inaccurately validate mental images as ‘memories’ of true events. This could lead to PTSD-like symptoms. In addition, it may lead patients to pursue legal action against the alleged perpetrator(s), increasing the risk of false accusations (e.g., Hendriks et al., 2023). This may be particularly relevant for individuals with high fantasy proneness. Fantasy-proneness is characterized by vivid mental imagery (Klinger et al., 2009) and a heightened ability to become deeply immersed in imagined scenarios (Bacon & Charlesford, 2018). This trait may be associated with an increased risk of memory distortion and the creation of new mental images during treatment. In the context of psychological treatment, at least two questions arise, namely whether imagery-based treatment should be offered for mental images of ritual sexual abuse and, if so, what type of (imagery-based) treatment.
In clinical practice, patients who experience distressing mental images related to a reported traumatic event are typically screened for PTSD. When PTSD is indeed classified, several trauma-focused therapies are available. Exposure-based interventions (also known as prolonged exposure; PE) and Eye Movement and Desensitization and Reprocessing (EMDR) are the gold standard treatments for PTSD (NICE, 2018), both of which include imagery-based interventions (Cusack et al., 2016; Weber et al., 2021). However, as noted above, imagery-based interventions carry a risk of distorting memory or even inducing false memories. In a systematic review of studies of false memories induction using various techniques (e.g. guided imagery, suggestive statements), Muschalla and Schönborn (2021) it was found that potentially harmful false beliefs or false memories were induced in 20–50% of participants. This presents clinicians with a dilemma. That is, the clinician must weigh the desire to treat the images against the potential consequences, including image distortion and the creation of false mental images.
Imagery Rescripting for PTSD
Based on shared decision making (Hamblen et al., 2019), Imagery Rescripting (ImRs; Smucker et al., 1995) was selected as the preferred intervention for the case that is presented here. Previous research has shown that ImRs, when used as a standalone treatment, positively affects PTSD symptoms in patients with PTSD related to childhood trauma, such as experiences of physical and sexual abuse (Kip et al., 2023; Raabe et al., 2022). ImRs has also been shown to be feasible, safe, and effective in reducing the distress caused by other mental images that do not correspond to reality. Examples include the treatment of nightmares (e.g., Albanese et al., 2022) and psychotic experiences such as verbal hallucinations (Adams et al., 2020; Clarke et al., 2022; Ison et al., 2014; Paulik et al., 2019). Similar to other guideline trauma-focused therapies such as PE and EMDR, ImRs relies heavily on imagery; however, the exposure to the mental image is limited in duration. The goal of ImRs is to rewrite the mental images to change their emotional and cognitive meaning (Arntz & Weertman, 1999). The patient recalls the traumatic event only to activate the mental image and associated emotions. Rescripting begins immediately after the activation of the mental image. Therefore, there may be less chance of validating or creating false mental images in ImRs.
ImRs treatment consist of three phases (Arntz & Weertman, 1999). In the first phase, the patient is guided to mentally relive the distressing image in the first person, as vividly as possible. The goal of this phase is to access the emotional and sensory details of the images, helping both the therapist and patient understand the key needs, emotions, and unmet responses. In the second phase, either the therapist, the current adult self, or a compassionate other (imagined) enters the image to intervene. The purpose of this phase is to prevent the traumatic experience from happening, protect the younger self, confront perpetrators, and offer comfort and validation. The intervening actions can be performed by the therapist (usually in the first sessions) or by the patient (usually in the later sessions). In the third phase, the patient revisits the image with the new outcome. This phase helps to consolidate new beliefs and emotional responses. The rescripts during ImRs typically involve the individual gaining more control, or arriving at a more positive resolution to an unresolved emotional situation. Indeed, an increased sense of mastery and controllability over the emotions elicited by the mental images mediated treatment efficacy when ImRs was used to treat mental images that were part of nightmares (Kunze et al., 2019). In ImRs the patient’s fantasy can be used to intervene and rewrite the mental images, thereby reducing feelings of anxiety, fear, shame and guilt. As such, ImRs can be a good treatment option, especially in the case of a fantasy-prone patient.
Present Study
In this case study we report on the use of ImRs with a patient suffering from mental images related to reports of childhood ritual abuse in a cult. To this end, we examined the course of symptoms and elements of change during treatment. Based on the available literature, it was expected that ImRs would be effective in reducing her PTSD symptoms.
Case Introduction
Ann (pseudonym) is a middle-aged, divorced woman. She was referred for trauma-focused treatment by the psychiatrist of a local Flexible Assertive Community Treatment (FACT) team. Specific details have been changed to protect her anonymity and she reviewed and approved the content of this case report prior to submission.
Presenting Complaints
During intake, Ann reported symptoms of re-experiencing negative images, flashbacks, nightmares, dissociation, hypervigilance (‘the feeling of being constantly ‘on’’), and negative feelings such as depression, anxiety, shame and guilt. Her flashbacks and nightmares were related to the reported ritual sexual, physical and emotional abuse that she stated to have experienced in a cult during her childhood. Ann has experienced psychological symptoms since childhood. At the time of intake, Ann expressed suicidal thoughts, such as ‘life doesn’t make sense with all my mental problems’ and ‘it feels like there is no way out of this’. She did not report any suicidal tendencies or behaviors. She admitted that she sometimes lost her perspective on life and said that she did not want to suffer anymore. She also reported that she was motivated to get treatment and wanted to live a life with less suffering. She had previously developed a safety plan that included helpful behaviors were specified, such as seeking distraction, cuddling with her baby doll, and socializing with others. Her ex-partner, friends and mental health care professionals provided sufficient social support, making her symptoms manageable most of the time. However, her daily flashbacks and dissociative episodes made life unpleasant and at times unbearable. She did not report any obvious avoidance behavior, but she did not like to visit her family. She visited them no more than once a year. The death of her most recent partner 2.5 years ago had led to an exacerbation of the trauma-related symptoms, which is why she was now seeking trauma-focused treatment.
History
During her childhood, Ann lived with her father, mother and brother. She stated that some family members took her to a religious cult when she was four years old. Most of the time, the people in the cult were friendly, and she was allowed to play there. When she did her “job,” which included being sexually abused, she was given ice cream. She reported that once, at the age of 14, she became pregnant as a result of the abuse, and the cult members performed an abortion with knitting needles and Ann was forced to eat the fetus. She reported being drugged during this event and that she only remembers fragments of the event. This was one of the mental images she suffered from. Other traumatic events she reported were physical abuse and sexual abuse by multiple cult members, both family and non-family, including physical threats with a weapon. The mental image she suffered from most was the moment that she was forced to shoot a child as part of the cult’s Christmas ritual.
She has suffered from depressive feelings and suicidal ideations since elementary school, and in her twenties she suffered from anxiety and burnout. Her psychological problems have prevented her from completing her education after high school, maintaining a (voluntary) job, and leading a fulfilling social, life. Ann had previously engaged in self-harming behaviors by cutting or scratching her arms, typically during moments of dissociation. She reported having control over the self-harming tendencies at the time of treatment. In addition to these symptoms, she was diagnosed with autism spectrum disorder (ASD) about two years ago. Ann is a widow and divorcee with grown children. She divorced her first husband, the father of her children, about a decade ago, but they remained in good contact and lived near each other.
Treatment History
Twelve years ago, she began her first trauma-focused treatment in a group setting, but she did not complete it because she did not feel safe in the group. About six years ago, she underwent three sessions of EMDR but discontinued treatment because she felt overwhelmed. For the past several years, she has been in outpatient residential care (FACT) receiving support and practical help.
Assessment
Measures
Clinician-Administered PTSD
The CAPS-5 is a 20-item clinical interview that assesses both DSM-5 PTSD diagnostic criteria and PTSD symptom severity (Weathers et al., 2018; Boeschoten et al., 2018). Scores range is 0–80, with higher scores indicating greater severity. A change in the CAPS-5 score of >15 is considered a reliable change, and a total score below eight at the end of treatment is considered clinically significant (Marx et al., 2022). The CAPS-5 was administered by two trained clinicians.
Self-reported History of Trauma
The Life Event Checklist for the DSM-5 (LEC-5; Boeschoten et al., 2014; Weathers et al., 2013) was used to screen for exposure to traumatic events. It assesses varying degrees of exposure to 16 events that are known to potentially lead to PTSD, and one additional item assessing any other intense stressful event not captured in the first 16 items. The LEC-5 was administered at intake.
Self-reported PTSD Symptoms
The PTSD Checklist for DSM-5 (PCL-5) is a 20-item self-report questionnaire that assesses PTSD symptoms (Blevins et al., 2015). Total PCL-5 scores range from 0 to 80 with higher scores indicating greater symptom severity. A change in PCL-5 score of >12 between baseline and follow-up assessment is considered a reliable change, and a total score of <28 on the PCL-5 is considered as clinically significant (Marx et al., 2022).
Depressive Symptoms
Depressive symptom severity was measured using the Beck Depression Inventory, 2nd edition (BDI-II-NL). The BDI-II-NL is a 21-item self-report measure of depressive symptoms occurring over the past 2 weeks. Items are scored from 0 to 4, with higher scores indicating greater symptom severity (Beck et al., 1996). Total score ranges from 0 to 63. Total scores of 0 to 13 are considered no or minimal depression, 14 to 19 are considered mild depression, 20 to 28 are considered moderate depression, and 29 to 63 are considered severe depression.
Fantasy Proneness
Fantasy proneness was assessed using the Dutch version of the Creative Experiences Questionnaire (CEQ; Merckelbach et al., 2001). The CEQ consists of 25 yes-no items that can be divided into three subgroups of questions: (1) the developmental antecedents of fantasy proneness (“As a child I was encouraged by adults to fully indulge myself in fantasies and daydreams”), (2) intense involvement in fantasy (“I spend more than half of my day fantasizing or daydreaming”), and (3) consequences of fantasizing (“I tend to confuse my fantasies with mental images of real events”).
Working Alliance
The therapist version of the Working Alliance Inventory (WAI) was used to examine therapeutic alliance (Horvath & Greenberg, 1989; Vertommen & Vervaeke, 1996). The WAI consists of 12 items that can be rated on a 7-point Likert scale, with scores ranging from 0 “never” to 6 “always”. Items include “My patient and I are working toward the goals we have upon” and “My patient and I seem to trust each other”.
Treatment Integrity
To assess adherence to treatment procedures, the therapists completed a checklist during and after each session indicating whether they fulfilled all required elements of each treatment session (e.g. discussing homework, rescripting). They also indicated which mental image was rescripted, how many minutes of rescripting took place, whether it was therapist or patient rescripting, whether emotions were activated, and whether there were any significant events (e.g. medication changes, crisis contact).
Personalized Therapy Outcomes
Therapy outcomes were assessed by three single items: (1) tolerability of emotions (“To what extent can you tolerate the emotions triggered by the memory”), (2) mastery of content (“Since the last session, to what extent have you had control over the content of the memory?”) and (3) feelings of guilt (“How credible is the idea that you are guilty?”). The patient rated each item on a visual analog scale (VAS) ranging from 0 (not at all or very bad) to 100 (very much or very good) during each treatment session and at follow-up.
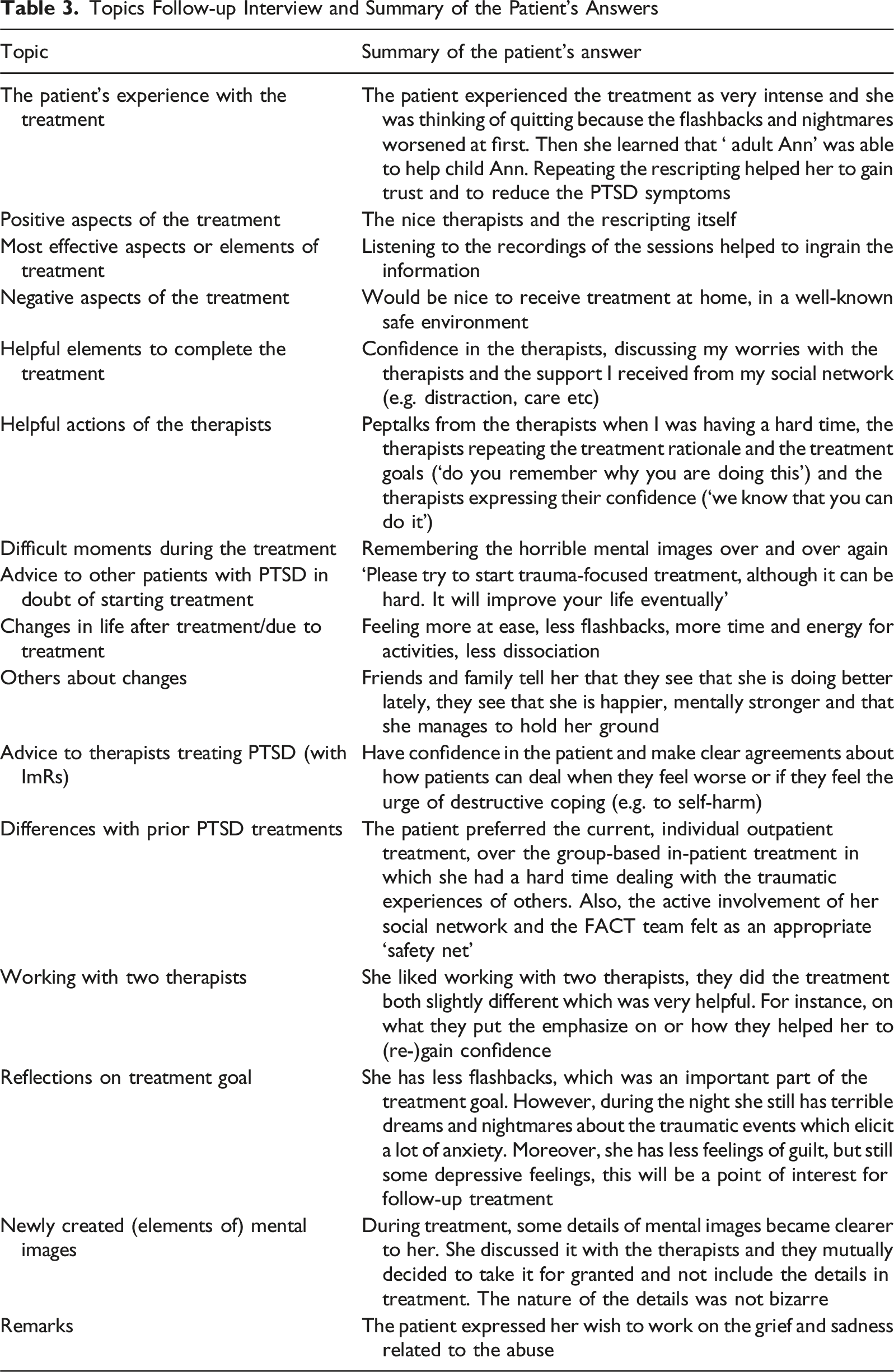
Patient Experience
After the follow-up, the patient was interviewed by the first author about her experience with the treatment. During the interview, the interviewer followed a list of topics that included positive and negative aspects of the treatment, reflections on the treatment goals and her experience with creating or re-finding mental images. The list of topics was compiled together by the first, second, and last author. The patient’s responses were summarized by the first author and the patient had the opportunity to read the summary and to provide feedback.
Procedure
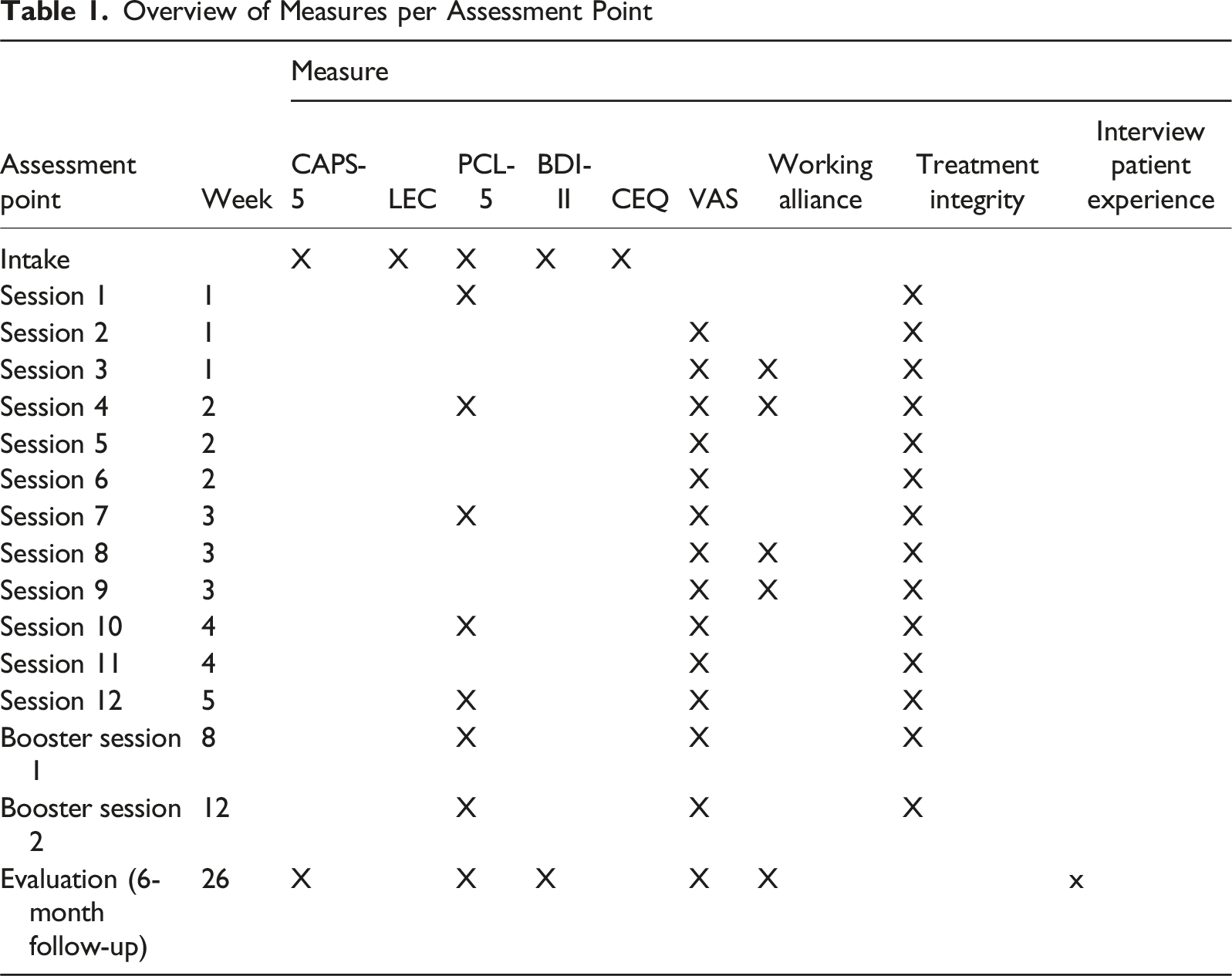
Overview of Measures per Assessment Point
Case Conceptualization
Ann’s symptoms were diagnosed as PTSD by the therapists during intake, with a total PTSD symptom severity total score of 63 on the CAPS-5 interview. Her most prominent and distressing symptoms were the flashbacks of physical and sexual abuse and dissociative experiences that occurred on a daily basis. She also reported having nightmares, feelings of anxiety, negative cognitions about herself, such as “it is my own fault”, feelings of guilt and a loss of interest. Also during the intake interviews, she experienced dissociative episodes or flashbacks and needed a break for a few minutes. During the flashbacks, the patient reported seeing blood on the walls, which may indicate that her reality testing was fluid. In terms of co-morbidity, depressive symptoms were evident, with a total severity score of 28, which can be considered ‘severe’ (Beck et al., 1996). Ann reported symptoms of sadness, pessimism, feelings of guilt and worthlessness and loss of interest. Ann regularly experienced loss of perspective and was easily overwhelmed by emotions, but she was not considered to be at acute risk for suicidality. With regard to fantasy proneness, Ann completed the CEQ prior to treatment and had a score of 24 out of 25, indicating a high level of fantasy proneness.
Based on shared decision making (Hamblen et al., 2019), ImRs (Smucker et al., 1995) was selected as the preferred intervention. The treatment choice was limited by pragmatic circumstances. That is, at the institution where the patient discussed in the current case study received care, two treatments for PTSD are offered: Prolonged Exposure (PE; Foa et al., 2007) and ImRs. In order to decide which of these two treatments would be used, a team of experienced trauma therapists was consulted and the patient was informed about these options. The patient was open to both treatment options and relied on the therapists’ advice, but after discussing the options, she expressed a preference for ImRs. Although Ann found the prospect of trauma-focused treatment frightening, she was very motivated and felt ready for it. Another prognostically favorable factor for treatment was that Ann felt supported by her ex-husband, a good friend, and the FACT-team. Her high level of fantasy proneness was considered valuable for the rescripting, as she would be better able to visualize the interventions and the rescripted mental images. Ann’s primary treatment goal was to reduce flashbacks and dissociative episodes in daily life.
Course of Treatment and Assessment of Progress
Course of Treatment
Ann received 14 sessions of ImRs in total. Prior to treatment, Ann received two preparatory sessions in which the treatment procedures and an outline of the therapy were discussed. The treatment was evaluated six months after the first session together with the therapists, the referring therapist, and the patient.
Preparatory Phase
During the two preparatory sessions Ann received an explanation of the time investment, the treatment (psychoeducation, the procedures during the sessions, homework), procedures of crisis management, and what she could expect in terms of effects and challenges, such as a temporary increase in symptoms that might feel overwhelming or possible exhaustion. The patient followed the institution’s standard treatment procedures. This means that the FACT team remained responsible for medication and crisis management. The FACT team was available for Ann in the case of crises, but did not provide any other psychological treatment during the ImRs. These procedures were discussed with Ann and the FACT team. It was also explained to her that medication should remain stable and how her support system (ex-partner and FACT team) could provide support during the treatment. Her ex-husband was present at one of the preparatory sessions to discuss what kind of help and support she would need during the treatment and how he could support her. In further preparation of the ImRs, Ann and the therapist created a list of the mental images to target, which guided the content of the sessions. That is, for each session it was decided which particular mental image would be treated using ImRs, starting with the most distressing image. The therapist explained that the rule of thumb was to schedule two sessions for the treatment of one mental image. Five mental images were eventually selected by Ann, resulting in ten sessions for which the content was scheduled at the beginning of treatment. The other four sessions could be used for repetition or other memories that were not scheduled on beforehand.
Treatment Phase
Overview of the Content of Each Session
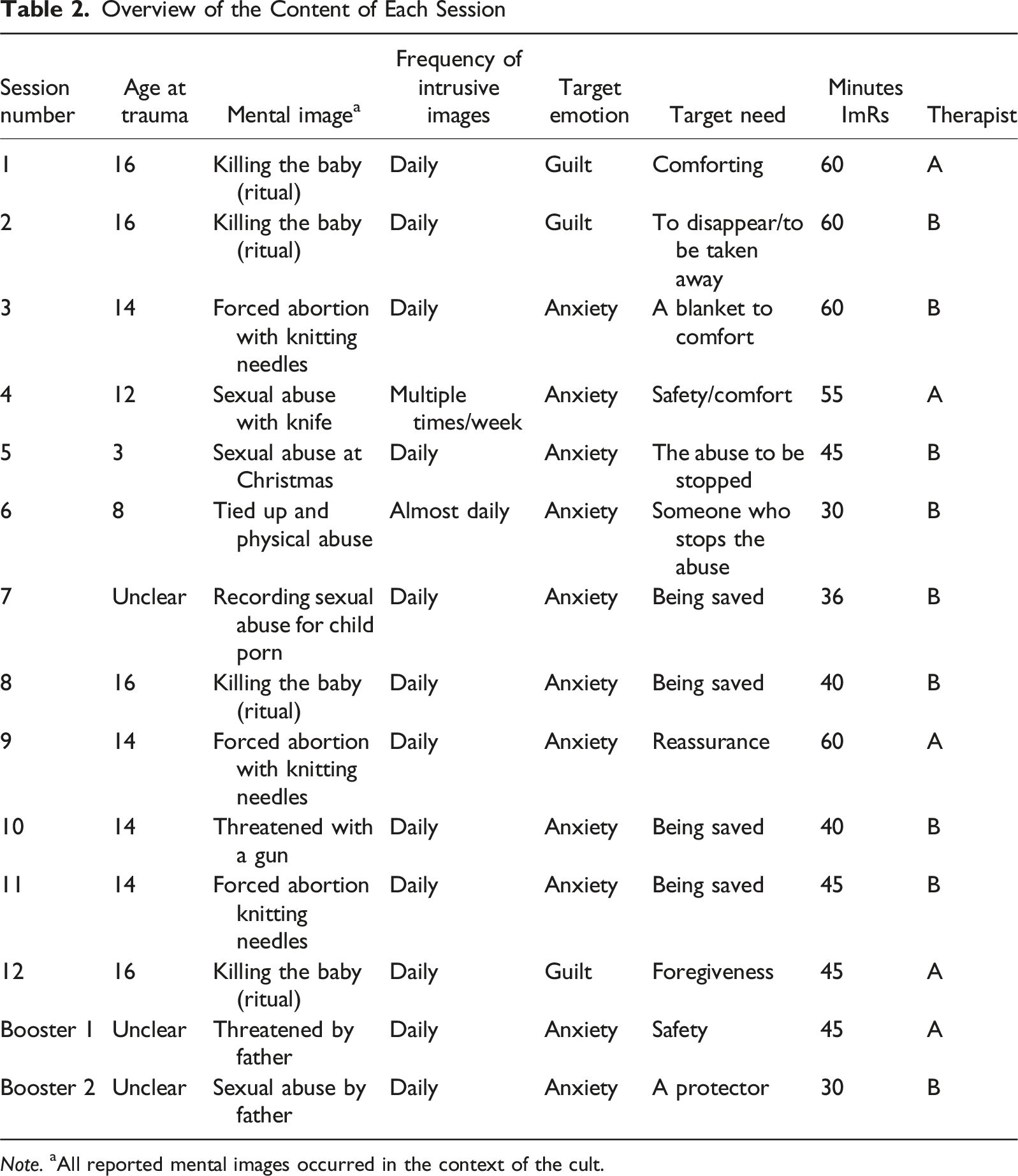
Note. aAll reported mental images occurred in the context of the cult.
During the first two sessions, the therapist led the rescripting process. Starting in the third session, Ann did most of the rescripting herself, guided by the therapist. The targeted emotions in all sessions were anxiety and guilt. The target needs varied from wanting to disappear or be taken away from the scene of the traumatic event, to wanting protection, to preventing the traumatic event from happening, to wanting comfort. Ann was able to ensure that the younger version of herself (“Little Ann”) was safe. She took care of her by explaining that she was not to blame. Ann also made sure that the perpetrators were punished and could not harm “Little Ann” again. For example, she sent them to Siberia. During the rescripting, Ann confronted her mother about her responsibilities and lack of protection. In session seven, she confronted her father about his unacceptable behavior. Throughout the ImRs sessions, Ann successfully rescripted the mental images by bringing “Little Ann” to safety, ensuring that the perpetrators could not harm her again, and addressing the responsibilities of the adults who should have protected her. Ann recorded all ImRs sessions and was asked to listen to the recording at least once between sessions, i.e. three times a week in total, as homework. She listened to the recordings of the sessions five times a week because she felt it really helped her in reducing her symptoms. During the treatment, Ann exhibited moments of severe dissociation, which manifested as vacant stares, a lack of responsiveness, difficulty communicating, and reported memory gaps. These moments occurred several times over the course of treatment. In case of these dissociative symptoms during the sessions, the therapists dealt with this by remaining present and calm, allowing her time to reorient and regain her focus.
Rescripting also took place during the booster sessions. After the second booster session, Ann did not receive any trauma-focused treatment and the therapists and Ann had no treatment-related contact.
Assessment of Progress
PTSD Symptoms
Self-reported PTSD symptoms, as measured with the PCL-5, improved considerably during treatment (see Figure 1). Between intake and the first treatment session, the PCL-5 score increased slightly. Ann reported having more physical responses when she was reminded of the abuse, including breathing difficulties and heart palpitations, increased irritability and self-harm tendencies. In the third session (week one) Ann was able to confront her mother during the rescripting and expressed her anger towards her mother. Afterwards Ann expressed that she felt empowered and relieved. However, during the weekend between session three and four Ann experienced an increase in flashbacks and nightmares. It helped er to listen to the recordings to calm down. After week two (session six), her symptoms decreased. She experienced less anxiety and guilt, felt less estranged from others, was less irritable, was less inclined to hurt herself, and was less alert and vigilant. In session seven Ann was able to confront her father with his behaviors during the rescripting, which made her feel strong. However, when she came home after the session she felt very stressed, jumpy and emotional. Also during the weekend after session eight, she felt overwhelmed by emotions. She called the In Home Team (a service provided by the referrer) to help her calm down. In line with this, she reported an increase of symptoms on the PCL-5 in week three. Specifically, the negative thoughts about herself, the feelings of guilt and estrangement increased slightly. She also got more vigilant again. After week four Ann started to feel better again and reported having less negative thoughts and feelings and started regaining interest in daily activities for instance. This decrease in symptoms continued during the two booster months and follow-up. Consistent with previous research (Burger et al., 2023), Ann’s PTSD symptoms increased during the first few weeks of treatment and showed the greatest decrease between the second booster session and the 6-month follow-up. PCL-5 Total Scores From Intake to 6-Month Follow-Up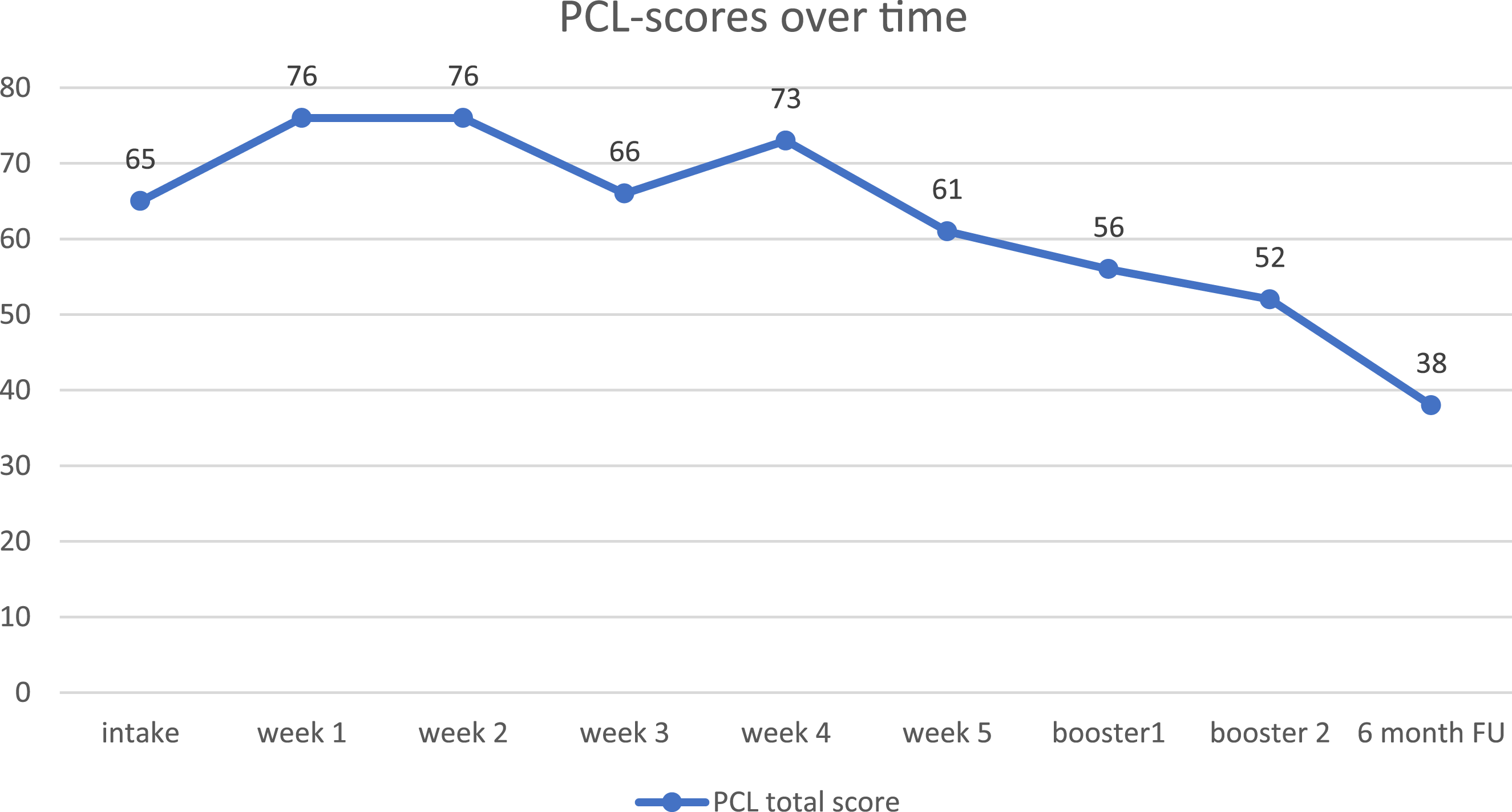
Personalized Therapy Outcomes
To assess personalized therapy outcomes, Ann completed ratings on three items “mastery of content”, “tolerability of emotions” and “guilt feelings” on a VAS, ranging from 0-100 during each session, beginning with session 2. The VAS scores for each session are shown in Figure 2. A summary of the VAS scores per session can be found in Table S1 in the Supplemental Materials. Overall, the scores of “mastery of content” (controllability) and “tolerability of emotions” increased between the first measurement (session 2) and session 12 and continued to increase during the booster months and the follow-up period. Her levels of experienced feelings of guilt decreased between the first measurement occasion (session 2) and session 12 and continued to decrease during follow-up. Her feelings of controllability of the memory content at follow-up (VAS = 78) and the tolerability of emotions (VAS = 82) can be considered high. Her levels of guilt experienced at follow-up (VAS = 13) can be considered low to moderate. The relatively lower levels of controllability and tolerability during booster session 2 as compared to booster session 1 and the 6-month follow-up could be related to the targeted image during session 12 (sexual abuse by father), which was more distressing for the patient as compared to previous images. VAS Scores (0-100) of Controllability, Tolerability and Guilt From Session 2 to 6-Month Follow-Up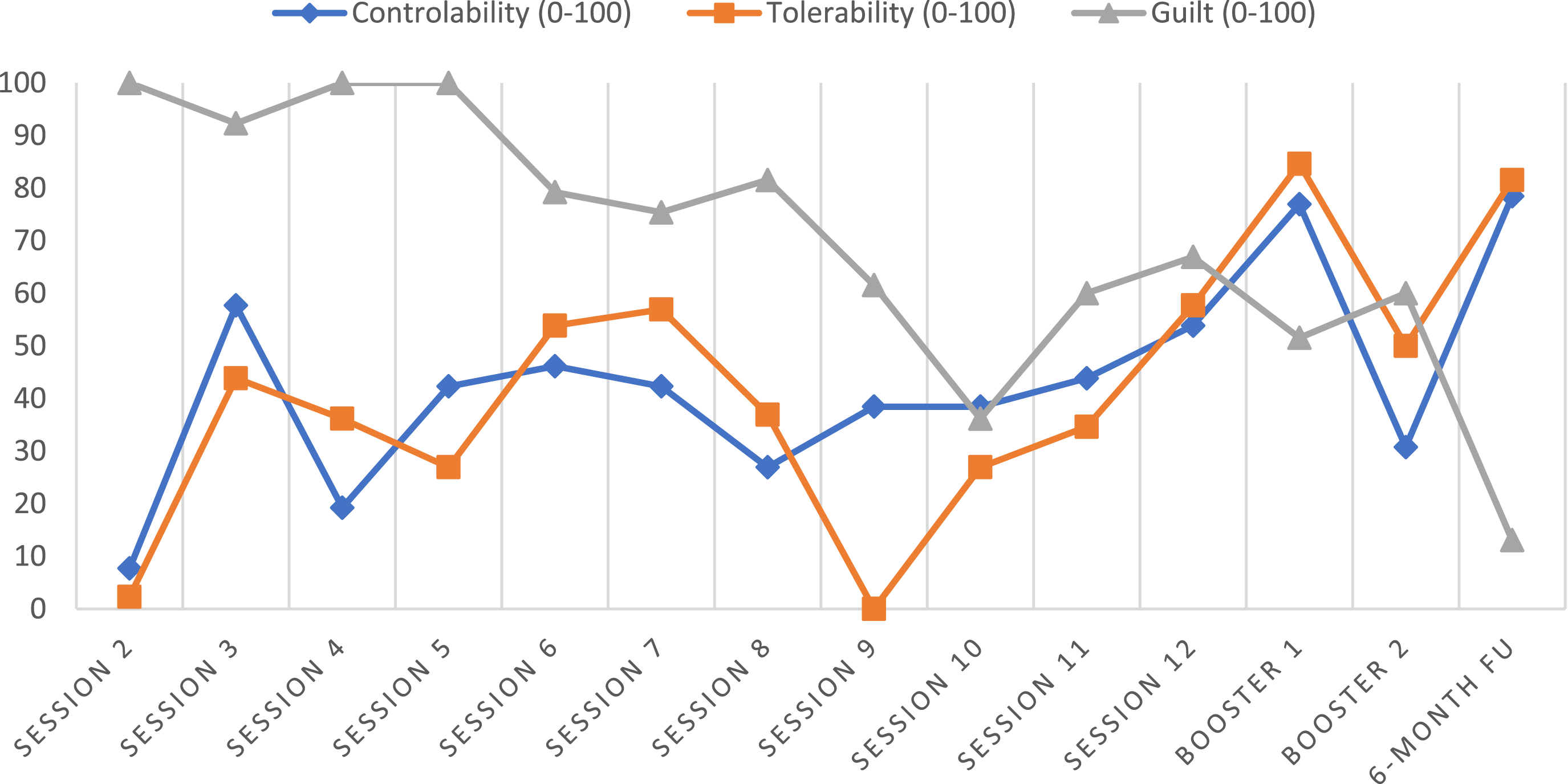
Complicating Factors
Ann has been previously diagnosed with ASD. The symptoms associated with ASD have the potential to impede the generalization and integration of the information that patients acquire during treatment. Consequently, this was regarded as a potential complicating factor. However, preliminary findings from case reports also indicate that treatment for PTSD can be effective in patients with ASD (Rumball, 2018). According to the literature on the subject, there is no evidence that the protocols for trauma-focused treatments, such as ImRs, need to be adjusted for patients with PTSD and comorbid ASD (Rumball, 2018).
In terms of protocol deviations, the therapists reported one issue: Ann had taken a benzodiazepine (Lorazepam) prior to session 12. This act was in violation of the treatment agreement. Ann mentioned that the purpose of the medication was not to alleviate symptoms of PTSD or feelings of anxiety related to the session. Rather, she took it due to the recent loss of her pet. No problems or ruptures in the therapeutic alliance were reported.
Access and Barriers to Care
There were no significant barriers to care that arose prior or during intervention that impacted the treatment of Ann.
Follow-up
Three months after the second booster session (six months after the treatment began), Ann was invited for a treatment evaluation. In addition to the self-report questionnaires and the structured interview about her PTSD symptoms, her experience with the treatment was assessed via a semi-structured interview.
As can be derived from Figure 1, at the end of treatment, her self-reported PTSD symptoms, as measured with the PCL-5, had considerably improved during treatment. The change in PCL-5 scores can also be considered reliable, as the total PCL-5 score decreased from 65 at baseline to 38 at follow-up (Δ = 27). In line with the symptom change as measured with the PCL-5, the sum score of the CAPS-5 decreased from 63 at pretreatment, to 45 at follow-up, 6 months after treatment began (Δ = 18). The change in CAPS-5 scores can be considered a reliable reduction in PTSD symptom severity. Ann reported that she still had intrusions and nightmares about the ritual abuse, but they bothered her less. More precisely, the dissociative responses, as well as the negative thoughts and feelings related to the mental images of the abuse, remitted. She felt less guilty and reported fewer negative beliefs, such as “I am to blame” or “I deserve to suffer,” than before the treatment. She felt she could handle the mental images better than before treatment. She participated in more activities, such as volunteering, shopping, and visiting friends. These activities also gave her more pleasure than before. However, her sleeping problems and difficulty concentrating remained similar to pre-treatment. She participated in more activities, such as volunteering, shopping, and visiting friends. These activities also gave her more pleasure than before. However, her sleeping problems and difficulty concentrating remained similar to pre-treatment. The post-treatment CAPS-5 and PCL-5 scores indicated that the patient was still experiencing a significant amount of PTSD symptoms (Marx et al., 2022). As Ann reported significant depressive symptoms at intake, in addition to PTSD symptoms, depressive symptoms were assessed pre-treatment and at follow-up. The BDI-II score at baseline was 28, which can be considered ‘severe’ (Beck et al., 1996). Depressive symptoms decreased over the course of treatment. At follow-up, the BDI-II score was 17, which can be considered ‘mild’.
Topics Follow-up Interview and Summary of the Patient’s Answers
Four months after the 6-month follow-up the patient contacted one of the therapists to report that she had been hospitalized because she was hearing voices with negative messages. These voices were also giving her messages related to the reported traumatic events. However, the patient reported that her PTSD symptoms had not returned. She felt that the psychotic symptoms were unrelated to the PTSD treatment. In fact, one of her ways of coping with the voices was to listen to the recordings of the ImRs sessions to recall her sense of empowerment. This is consistent with earlier findings from a series of cases in which imagery rescripting was found to reduce traumatic intrusions, voice frequency, and distress (Paulik et al., 2022). After several months, Ann reported that she was taking antipsychotic medication, and that the voices in her head had decreased significantly.
Treatment Implications of the Case
This study examined the effects of ImRs for PTSD in a patient experiencing mental images of childhood ritualistic sexual and physical abuse. We aimed to contribute to the limited literature on the treatment of ritual abuse-related imagery. The dearth of research and the absence of treatment guidelines for the treatment of mental images of ritual sexual abuse (Hendriks et al., 2023) serve as important barriers to the treatment of patients with these images. The potential for of memory distortion or creation of mental images during treatment with imagery-based techniques (Gezondheidsraad, 2004, p.106; Herndon et al., 2014; Loftus, 1994) has been a concern for clinicians, as it may lead to an exacerbation of symptoms, This hesitation among clinicians to offer imagery-based trauma-focused treatment is driven by the desire to avoid the risk of harming the patient. Given the positive effects of ImRs as a standalone treatment for patients with a history of childhood sexual abuse (Kip et al., 2023; Raabe et al., 2022) and our expectation of few negative effects on the mental images (i.e., no expansion of the adverse images) due to ImRs’ working mechanisms, we expected the treatment to have positive effects in this case. The case study indeed demonstrated reliable reductions in PTSD symptoms from baseline to post-treatment and continued to decrease during the 6-month follow-up period.
The patient’s fantasy and imaginative capacity proved beneficial during ImRs, allowing her to vividly visualize the images and interventions, which may have enhanced the treatment effect. Further research is needed on the role of high versus low fantasy-proneness in ImRs and to what extent fantasy-proneness should be considered as a predictive factor when deciding on the type of trauma-focused treatment (e.g., PE, EMDR, ImRs). Ann’s fantasy and active role in the rescripting may have helped her challenge negative, trauma-related beliefs and increase her sense of mastery. It is known from the literature that ImRs may reduce the believability of encapsulated beliefs, such as negative beliefs about the self, others, and the world, that are activated along with the mental images, such as “I am a burden” or “I am powerless” (Assmann et al., 2024). Consistent with these findings, Ann’s belief “I am guilty” changed significantly over the course of treatment. The reduction of which may have played a role in the reduction in overall symptomatology. This is in line with theoretical models of PTSD, according to which negative trauma-related cognitions or beliefs are central to the onset and maintenance of PTSD (Ehlers & Clark, 2000; Gómez de La Cuesta et al., 2019) and are therefore suggested as one of the core working mechanisms of trauma-focused treatments (Brown et al., 2019).
No negative effects, such as the creation of new adverse images, were observed. Also, despite the patient’s moments of dissociation during treatment, this did not hinder the therapy. These moments of dissociation are believed by some clinicians to impede the effectiveness of trauma-focused treatments and may result in therapist drift. In such cases, both the patient and the therapist may decide to discontinue treatment due to the perceived risks associated with the dissociation and the challenges the treatment may pose. Research has demonstrated that dissociation is not a contraindication to delivering trauma-focused treatment for PTSD and does not determine the treatment outcome (Hoeboer et al., 2020). The current study also demonstrates the efficacy of effective therapy in cases of dissociation. This case of a fantasy-prone PTSD patient with comorbid ASD, supported the hypothesis that ImRs may be effective as a stand-alone treatment in case of mental images of childhood ritual abuse and severe dissociation.
Recommendations to Clinicians and Students
Based on this case study, we formulated four recommendations First, in cases involving mental images of childhood ritualistic with bizarre elements, such as in Ann’s case, ImRs might be a preferred option for trauma-focused treatment. Unlike PE or EMDR, ImRs limits direct exposure to the distressing images and quickly shifts the focus toward empowering patients by helping them protect their younger selves and confront the perpetrators within the imagined situation. This approach reduces the risk of unintentionally validating bizarre elements while addressing the emotional impact of the mental image. Additionally, ImRs can foster a sense of mastery, promote emotional resolution, and encourage the development of more adaptive beliefs. Monitoring these beliefs as was done in the present case, can help to evaluate treatment progress.
Second, there were multiple practical preconditions of the treatment that might have contribute to the treatment success: (1) That is, Ann’s treatment was conducted in a facility that focuses primarily on the treatment of PTSD, so the therapists could easily consult other trauma experts within the facility, and crisis care and daily support were provided (i.e., by others than the therapists). These two aspects helped to maintain focus on PTSD treatment and minimize therapist drift. (2) The treatment was provided by two therapists, which has also been shown to reduce therapist drift, decrease therapist anxiety about providing trauma-focused treatment, and increase therapists’ perceived readiness to treat PTSD (Van Minnen et al., 2018). (3) All sessions were scheduled in beforehand and were offered in a limited time frame, which may have prevented dropout. (4) The treatment was well prepared with preparatory sessions that clearly outlined treatment procedures for the patient, referring therapists, and the patient’s support system. The preparation phase contributes to the patient’s understanding and correct expectations of the treatment. This increases the patient’s motivation and readiness. Theoretically, preparatory sessions help shape positive treatment outcome expectancies, which are associated with better therapeutic engagement and symptom improvement (Matthews et al., 2022; McLane et al., 2019 ). By addressing misconceptions and fostering a collaborative framework, these sessions also reduce dropout risk and enhance treatment credibility (Ahmed & Westra, 2009). (5) As the involvement of social support in the treatment of PTSD has been shown to increase the treatment efficacy (Price et al., 2018), Ann’s partner was actively involved in the preparatory phase was available for support during the treatment. (6) As emphasized by the patient herself, clear agreements on crisis management were made between the health care professionals and the patient were made and recorded in a safety plan, so that the patient knew what to do in moments of emotional stress or crisis. This procedure is supported by research that has shown that such a meaningful safety plan can reduce suicidal ideation and behavior, depression, and hopelessness (Ferguson et al., 2022).
Third, this case also highlights the need for regular intervision and supervision when working with patients with PTSD—especially in cases involving reported ritual abuse. Previous research has also shown that case consultation with a supervisor during trauma-focused treatment increases therapists’ self-efficacy and contributes to improved treatment outcomes (Foa et al., 2007).
Lastly, we would like to highlight some more general recently proposed guidelines for discussing mental images that are reported by patients who claim to have experienced ritual sexual abuse. First, based on findings that beliefs about the way memory works are associated with PTSD and dissociative symptoms (van der Linde et al., 2023), we recommend that therapists provide psychoeducation about how memory works. One should be aware that memory is (re)constructive and that memories are not objective representations of reality. This is not to say that therapists should get into conflict with patients about whether their ‘memories’ really happened or not. Rather, it is recommended that therapists do not tell patients that their mental images, even if very vivid and emotional, must be memories, nor that these mental images must be fantasies. Instead, it is helpful to validate the patient’s emotions and suffering in the here and now. Wessel and Van Minnen provided the following guidelines to avoid inducing false memories: (1) minimize the chance of inducing false memories by asking open-ended (rather than closed-ended suggestive) questions, (2) be aware that intense emotions when remembering or the patient’s firm belief that something happened a certain way, do not mean that the image must therefore refer to a true event, (3) be mindful of the possibility of false memories when the patient reports traumatic memories from their preverbal period (for most before the age of 3), when the memory is “recovered” during treatment, and when the patient continues to report new traumatic memories during treatment that seem increasingly absurd or improbable (personal communication, 2024). Overall, this study demonstrated that ImRs was a viable treatment option for a highly fantasy prone patient reporting mental images about ritual abuse. The effectiveness of ImRs in patients with mental images of ritual abuse could be further elucidated by conducting (randomized) studies in larger samples. We hope that our results and recommendations will provide guidance to fclinicians working with these patients.
Supplemental Material
Supplemental Material - Imagery Rescripting Therapy for Mental Images About Ritual Abuse During Childhood - A Case Study
Supplemental Material for Imagery Rescripting Therapy for Mental Images About Ritual Abuse During Childhood - A Case Study by Marie-Louise J. Kullberg, Bart Verkuil, Rafaele Huntjens, and Maartje Schoorl in Clinical Case Studies
Footnotes
Acknowledgements
We would like to thank Ann (pseudonym) for her permission to share her history and treatment course. All identifying information that was not deemed central to the conceptualization and treatment of this patient was removed to maintain confidentiality. We would also like to thank Loes Marquenie for training and supervising and Eva Bloemers and Monique Vulto for treating Ann.
Ethical Statement
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the sensitive nature of the clinical data, the data supporting this study are not publicly available.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.