
Abstract
Autistic children are at an increased risk for both (a) exhibiting problematic eating behaviors such as food selectivity and (b) experiencing potentially traumatic events and correlated posttraumatic stress symptoms. Not only could a history of trauma directly influence the development of food selectivity but may also negatively impact the efficacy and social validity of existing evidence-based interventions. There is currently very little published research on interventions for food selectivity that incorporate commitments and strategies of trauma-informed care. In the current study, we sought to apply a trauma-informed approach to address the food selectivity of an autistic adolescent. Via a combination of single-subject experimental designs, we demonstrated that an intervention package inclusive of multiple trauma-informed care strategies directly contributed to increases in consumption of nonpreferred foods. We describe multiple ways in which we recruited and obtained social validation from the adolescent during his participation. Implications for practitioners and future research are discussed.
1 Theoretical and Research Basis for Treatment
Children who have experienced trauma have a high likelihood of exhibiting problematic food-related behaviors (Tarren-Sweeny, 2006). For example, children involved in the welfare system—a population with documented high prevalence rates of all forms of child maltreatment and posttraumatic stress symptoms (Ackerman et al., 1998; McCloskey & Walker, 2000)—are more likely to (a) be selective eaters, (b) engage in compulsive and binge eating, and (c) hoard or steal food compared to children not in government care (Savaglio et al., 2021). Problematic food-related behavior may be more prevalent in these populations due to exposure to acute and chronic stress in these environments in which food and other reinforcers may be inconsistently available or absent.
Despite the severity and estimated likelihood of concerning eating habits as they relate to trauma, evidence-based interventions that consider the impact of trauma are scarce. Although there is a fair amount of research aimed at adolescents and adults diagnosed with anorexia and bulimia who have experienced trauma (i.e., eating disorders; Brewerton, 2007; Shapiro et al., 2007), there is dearth of research for children with trauma backgrounds who exhibit other eating difficulties such as food selectivity, which is characterized by eating a narrow and restrictive range of foods that can pose various concerns to the child and important people in their life (Bachmeyer-Lee et al., 2023). The current paper focuses on profiles commonly referred to as food selectivity. Intellectually and developmentally disabled (IDD) children often live at an intersection of both trauma and eating difficulties. IDD Children are at a greater risk for experiencing traumatic events such as abuse, neglect, and various forms of violence (Reiter et al., 2007) as well as exhibiting feeding and eating difficulties.
Applied behavior analytic (ABA) interventions have been efficacious in addressing food selectivity and refusal of IDD individuals (Williams & Seiverling, 2022). ABA interventions are based on the circumstantial view of behavior that unique, environmental histories of an individual contribute to and maintain eating patterns. To address this problem, interventions such as escape extinction (Piazza et al., 2003), differential reinforcement (de los Santos & Silbaugh, 2020; Tereshko et al., 2023), shaping or stimulus fading (Roth et al., 2010; Tanner and Andreone, 2023), sequential presentation (Kozlowski et al., 2011), and contingency modeling (Flanagan et al., 2021), to name a few, have been employed.
If a child has a history of trauma, however, intervening may pose unique challenges (Finkelhor et al., 2014). Evidence suggests children who have experienced traumatic events and concomitant post-traumatic stress symptoms may be particularly resistant to certain intervention strategies (Grasso et al., 2013). For example, children may be particularly sensitive to physical touch, have increased aggression or oppositional behavior, and have difficulty building rapport with others.
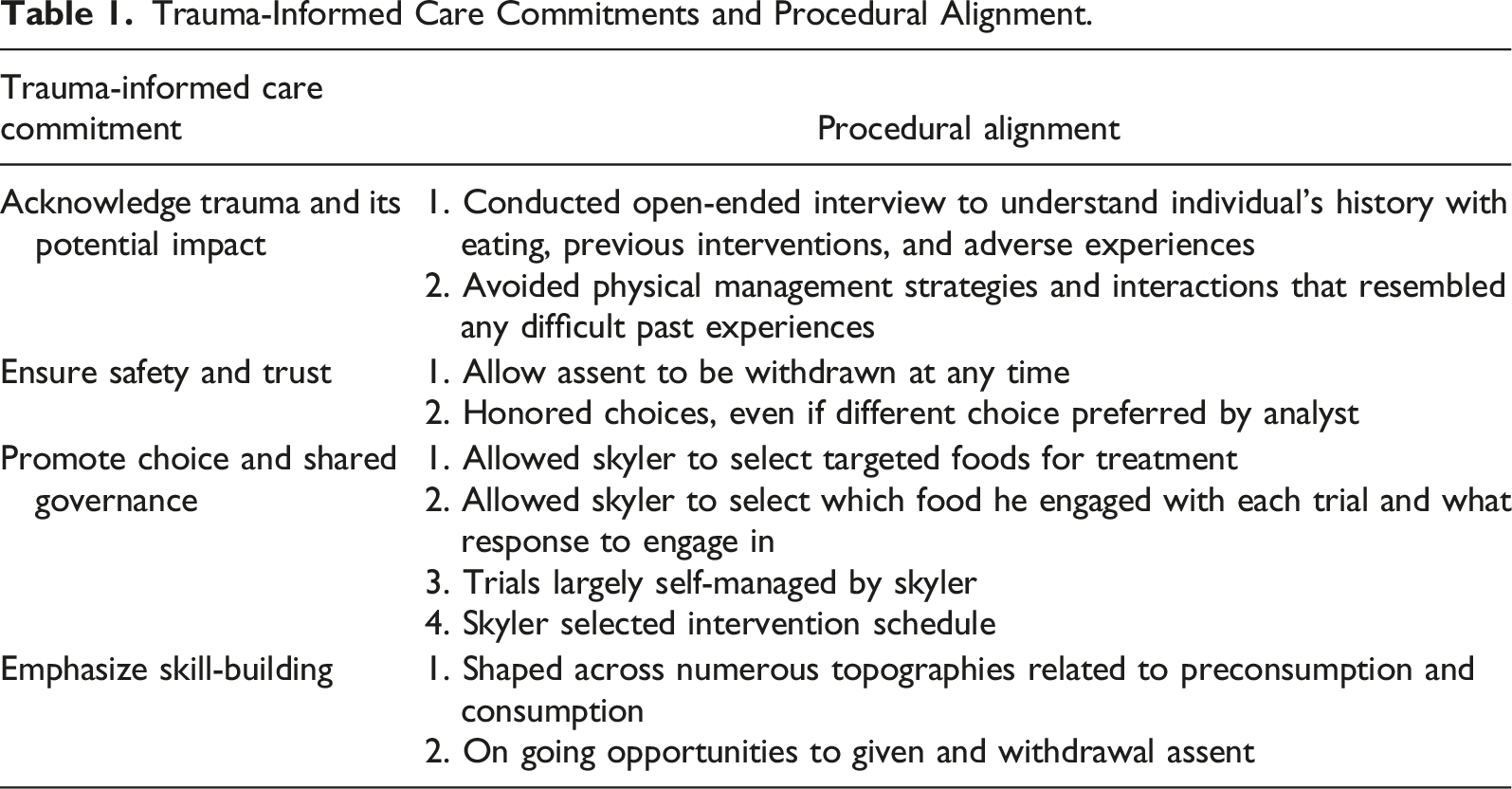
Trauma-informed care (TIC) is a proactive, preventative approach to human services that takes the potential past or present trauma of a client into consideration when designing and providing rehabilitative services (DeCandia et al., 2014). The goal of a TIC approach is to facilitate meaningful, uncoerced participation in one’s care in a manner that does not exacerbate potential trauma (Rajaraman et al., 2022). TIC does not prescribe specific procedures or interventions, nor is it intended to treat specific stress symptoms associated with trauma (see trauma-specific services, e.g., Oren & Solomon, 2012). Key commitments of a TIC framework include, (a) acknowledging trauma and its potential impact, (b) ensuring safety and trust, (c) promoting choice and shared governance, and (d) emphasizing skill-building. Rajaraman et al. (2022) argued in favor of incorporating TIC commitments into ABA research and practice to help protect against potentially exacerbating traumatic experiences. In service of demonstrating how a TIC approach may benefit ABA service recipients, Rajaraman at el. Offered recommendations for researchers to (a) explicitly describe how procedures align with TIC commitments and (b) report additional measures beyond primary dependent variables that provide an indication that traumatic experiences were minimized (e.g., measuring approach and avoidance of sessions, emotional responding during intervention, explicitly asking relevant individuals about perceived harm associated with procedures).
A TIC approach has yet to be integrated into behavioral interventions addressing food selectivity, let alone much of ABA research and practice. Given the prevalence of eating difficulties with IDD children and higher risk factors for experiencing traumatic events, an explicit TIC approach to addressing food selectivity is warranted. Gover et al. (2023) recently evaluated an assessment and intervention process that successfully addressed the food selectivity of three young children. The authors conducted interviews with the children’s caregivers, assessed the children’s food preferences, and conducted functional analyses of the children’s mealtime behavior. During intervention, the authors provided differential reinforcement for increasing levels of engagement with the target foods (e.g., smelling, licking, holding on tongue). The participants also had the option to leave the intervention context at any point and access a hangout area that was free from the expectation to engage with the target foods. Although this study began to address the need for more research on interventions that do not rely on restrictive procedures (e.g., escape extinction, physical management), this study only included young children, it did not articulate explicit links to TIC, and they did not obtain social validity from any shareholders, including the participants themselves.
The purpose of the current study was to replicate and extend Gover et al. (2023) by incorporating TIC strategies into the process for assessing and intervening upon the food selectivity of an autistic adolescent in a school setting. Our aims were to (a) address the restrictive eating of an adolescent in a school setting, (b) describe clear examples of how to incorporate TIC commitments into behavioral interventions for food selectivity, and (c) report several measures that assess whether procedures contributed to perceived trauma, including multiple forms of participant social validity. The current study considered the potential impact of trauma on the conceptualization, delivery, evaluation, and acceptability of procedures addressing food selectivity.
2 Case Introduction
Skyler was an autistic, 12-year-old, white male. At the time of the study, he was 5′ 2″ and 160 lbs. His language skills were developmentally appropriate for his age. He enjoyed creating assignments and quizzes for his teachers as well as working on creating his own complex catalog of fictional characters. Skyler was a student at a specialized school comprised primarily of autistic students who could not be appropriately educated by their home districts.
It is important to note that at the time Skyler’s participation in the study, he had no documented history of prior traumatic experiences (e.g., abuse, neglect, food insecurity) and did not appear to present with common posttraumatic stress symptoms (e.g., hyperarousal, learned helplessness) other than a pervasive unwillingness to try new things (see CDC [2019] and SAMSHA [2014] for information about events and symptoms correlated with trauma). As such, this study does not represent an evaluation of a trauma-specific service aimed to reduce trauma symptoms; rather, it is an evaluation of a preventative TIC approach to behavioral intervention for food selectivity to ensure that the therapeutic context was not traumatizing and maximized voluntary consumer participation.
3 Presenting Complaints
At the time of this study, Skyler’s classroom staff expressed concerns regarding Skyler’s eating habits at school. Skyler inconsistently ate 10–16 different types of food. At school he ate a fewer variety of foods. For lunch, he ate pretzels, Hershey’s chocolate, Twizzlers, and white bread. While at home, Skyler ate a wider variety of foods (e.g., some proteins, french fries, etc.), at school, he ate the same lunch every day. His parents reported he has been a selective eater for most of his life, and they had “given up the battle” several years ago. Given mounting health concerns (e.g., gastric distress), they desired for him to expand his diet, especially at school.
Skyler’s particular issues with eating can be described as exhibiting food selectivity, rather than total food refusal (Williams et al., 2010). He did not have a clinical diagnosis of Avoidant Restrictive Intake Disorder (ARFID). As such, his food selectivity did not pose an immediate health risk, but still posed challenges for his family as health issues were beginning to emerge per parental report. His parents reported no medical issues influencing his food selectivity (e.g., reflux), nor any motor-oral issues related to eating the foods he currently ate. An onsite Speech and Language Pathologist observed lunch sessions with Skyler to note if she observed any oral-motor issues related to eating and reported no concerns.
4 History
Skyler’s caregivers reported that behavior analytic interventions were previously implemented when Skyler was younger in attempts to increase the variety of foods he ate, which were unsuccessful. The school team, at one point in time, would offer Skyler various foods for him to try, but largely did not attempt to address his food selectivity at school. In addition, Skyler had previously gone through a successful behavioral intervention for severe behavior (outside of the mealtime context) of which he maintained zero to low rates of throughout his day. The treatment, specifically a skill-based treatment (Coffey et al., 2021), continued to be in place throughout his school day.
5 Assessment
All assessment (and subsequent intervention) sessions were conducted in a specialized, self-contained school for students with autism and related diagnoses. Sessions were run in Skyler’s classroom which contained materials typical to a classroom: desks, chairs, shelves, TVs, and learning materials. Skyler shared the room with five other students. Procedures took place at his desk where he completed schoolwork and ate lunch. He also used a desk space across the room with a computer for breaks and reinforcement periods. The first author, a doctoral-level board certified behavior analyst, conducted all assessment and intervention procedures (hereafter referred to as analyst). Skyler’s teacher and an educational assistant conducted the naturalistic extensions and the long-term follow-up.
The analyst interviewed Skyler’s caregivers to learn about the challenges their family had with respect to mealtimes, previous strategies attempted with Skyler, previous history with food, what typical mealtimes looked like at home, emotions surrounded meals, and what their goals were for Skyler and the impending therapeutic relationship. They were asked if Skyler engaged in any challenging mealtime behavior and if any specific strategies worked to encourage him to try new foods. They reported that they rarely pushed him to try to new foods and that Skyler was only willing to try new foods if it was “his idea”; that is, he would refuse any foods that were suggested by someone else. The analyst asked Skyler’s parents about adverse experiences related to foods and were asked if there was anything they’d like to share that would be important to conducting a behavioral treatment for food selectivity for their son. They reported that Skyler having control and autonomy was very important to him.
Caregivers were sent a food preference survey to gather information about which foods Skyler did and did not eat from various nutritional categories. The survey was administered via Google forms. The survey contained 10–20 foods per nutritional category (i.e., protein, fruits, vegetables, grains, dairy, and snacks), compiled from various forms available online, and caregivers were asked to indicate which foods from that category they wished Skyler to eat. From the food preference survey, we learned that Skyler ate very few fruits and vegetables, but ate a fair number of grains, proteins, and snacks. Skyler’s parents generated a list of seven foods from the food preference survey they wished Skyler would eat at school, and these foods were analyzed in a preference assessment.
The analyst then conducted a preference assessment of the caregiver selected foods and reported preferred foods with Skyler. She presented foods to Skyler in a single-stimulus format (Hagopian et al., 2004). Reported preferred and nonpreferred foods were offered one at a time; one bite of each food was placed in a small Tupperware container. The analyst showed the food to Skyler and stated what it was. If Skyler indicated he did not want to eat the food (i.e., shaking his head, saying “no”), the food was immediately removed and the next food was presented. If Skyler elected to take the food and consume it, the analyst waited until he was finished before presenting the next bite of food. Skyler ate a lollipop (i.e., small dum-dum lollipop that Skyler ate quickly), chocolate, and Twizzlers, and did not eat the rest of the foods. Skyler’s parents agreed that Skyler could select three foods to target from the list they generated.
The analyst interviewed Skyler using a Likert questionnaire. She asked Skyler how he felt about trying new foods and whether he felt eating a variety of foods was important. Following the preference assessment, the analyst gave the list of nonpreferred foods from the preference assessment to Skyler and had him rank them from “good to bad.” Together, they then selected the top three foods to target for intervention. Skyler selected how he would prefer to have each food prepared (i.e., red apples without the skin, mozzarella cheese, and sweet potato fries instead of tater tots). Skyler also selected the schedule of sessions. The analyst initially slated the sessions to take place five days a week, but Skyler requested a less frequent schedule. He chose Monday, Thursday, and Friday at 10:30 am.
6 Case Conceptualization
The information gleaned from the assessment directly informed the selection and design of the intervention. We learned from the school team, Skyler’s caregivers, and Skyler that he had a long history of selective eating, previous attempts had failed, and that the food selectivity did not appear to be due to any medical reasons. Caregivers reported that he had had an oral-motor evaluation when he was younger and there were no concerns with him being a safe, oral eater, and he currently had no trouble eating the variety of table textured foods he did consume. In other words, Skyler’s food selectivity was likely a behavioral issue rather than a medical or biological issue. In addition, we learned there were certain personal characteristics that could make implementing an intervention for selective eating challenging. For example, we learned that Skyler was highly averse to being controlled and told what to do, especially around food. Thus, we chose to replicate and extend Gover et al. (2023) given the procedures allowed the participants’ ample choice making opportunities and the ability to opt in and out of the intervention. Further, Gover et al. (2023) addressed food selectivity specifically, rather than more severe forms of pediatric feeding disorders such as total food refusal, and the procedures appeared to be feasible for a classroom setting.
Trauma-Informed Care Commitments and Procedural Alignment.
To evaluate the efficacy of the intervention, we opted to combine multiple single-case experimental designs to appraise the impact of the intervention on Skyler’s food-related behavior. The effect of the intervention was evaluated using a concurrent multiple-baseline design across target foods with an embedded changing criterion design for each targeted food item (see Beaulieu & Povinelli, 2018, for an example of this design combination; see Klein et al., 2017 for a review). We obtained baseline measures with each target food until stable responding was observed; following observed stability, the intervention was introduced in a staggered manner across the three foods. We systematically increased the response requirement (e.g., moving from touching to smelling to tasting) for each food in a stepwise fashion. In addition, we reversed to baseline conditions before reinstating intervention conditions for two out of the three target foods. Functional control was considered demonstrated when (a) Skyler’s engagement with the foods began reliably improving only when the differential reinforcement contingency was introduced; (b) changes in food-related behavior corresponded with changes in reinforcement criteria; and (c) performance reverted to baseline levels during the reversal.
7 Course of Treatment and Assessment Progress
Measurement
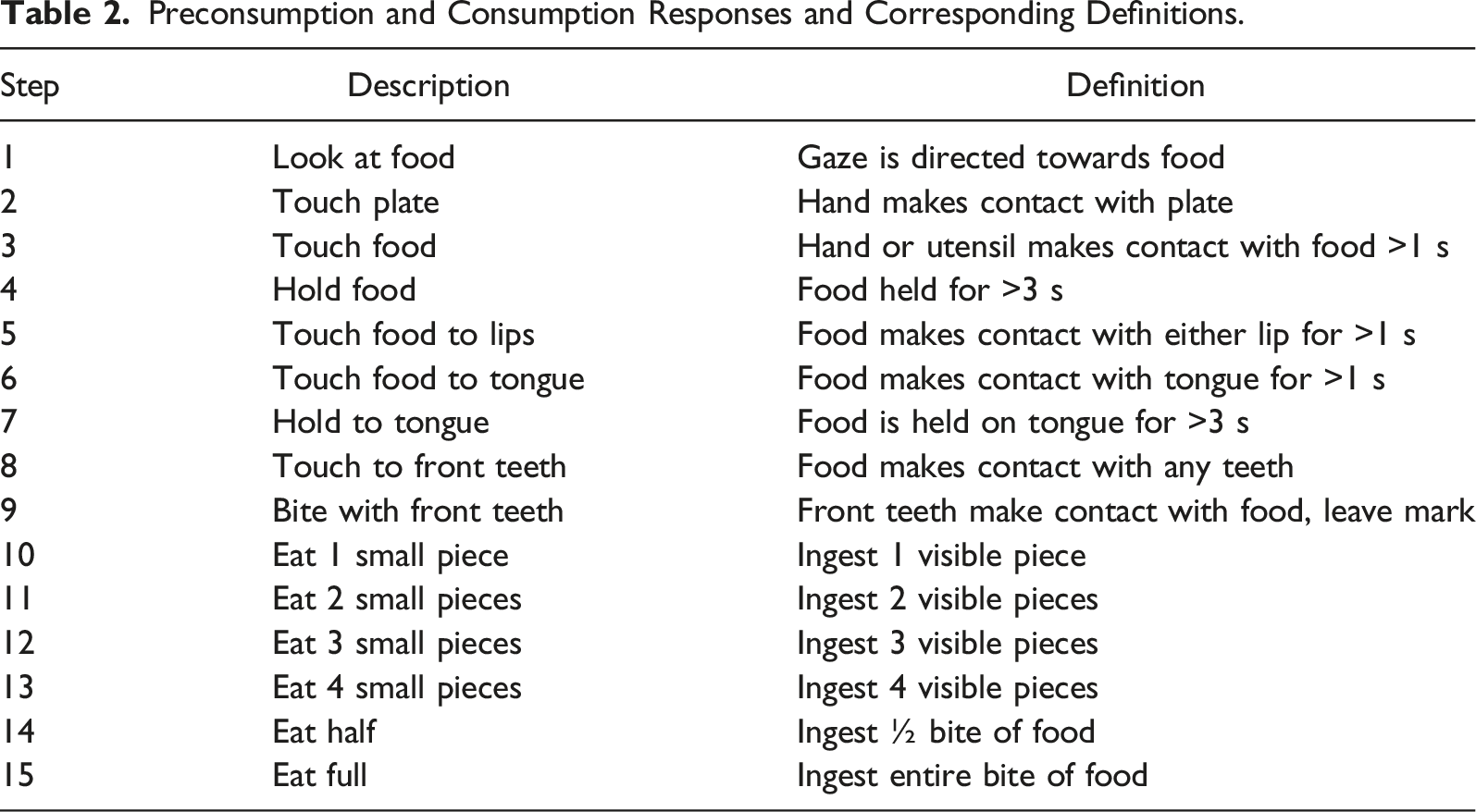
Preconsumption and Consumption Responses and Corresponding Definitions.
Differential Reinforcement Without Extinction Baseline
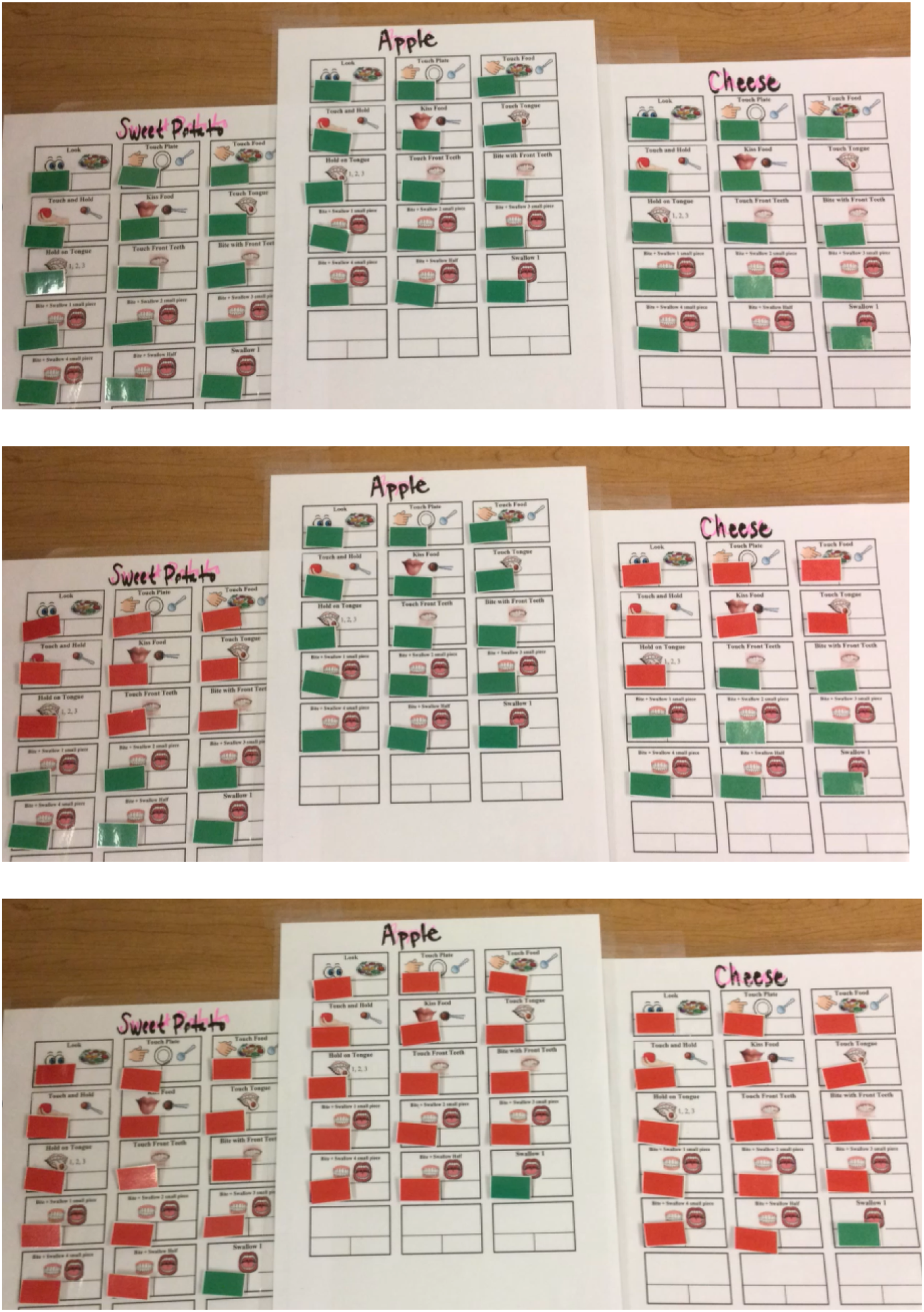
We first conducted a baseline phase to evaluate Skyler’s current level of engagement with the target foods (sweet potato, cheese, apple). Skyler was asked to come to the treatment table. On the table were three identical laminated boards (See Figure 1). At the top of each respective board was a bite-sized piece (2.5 cm x 2.5 cm) of the target food in a small container as well as a fourth container containing pieces of Twizzlers (i.e., a piece of apple was above the first board, a piece of sweet potato of was above the second board, a piece of cheese was above the third board, and pieces of the candy in a fourth container). The three boards each listed responses related to preconsumption and consumption (See Figure 2 for the boards in baseline, top image). See Table 2 for the list of preconsumption and consumption topographies we shaped across. During baseline, next to each response was a green sticker indicating that if Skyler selected and engaged in that response, he would receive access to full synthesized reinforcement. Full synthesized reinforcement included access to a piece of a Twizzler, his computer, and the full attention and cooperation from his teacher for about 2 minutes. As such, we arranged differential reinforcement without extinction in baseline in that all responses resulted in the same reinforcement, but a response was still required. Skyler’s intervention results. Depiction of Skyler’s choice board across baseline (top), mid-treatment (middle), and end of treatment (bottom).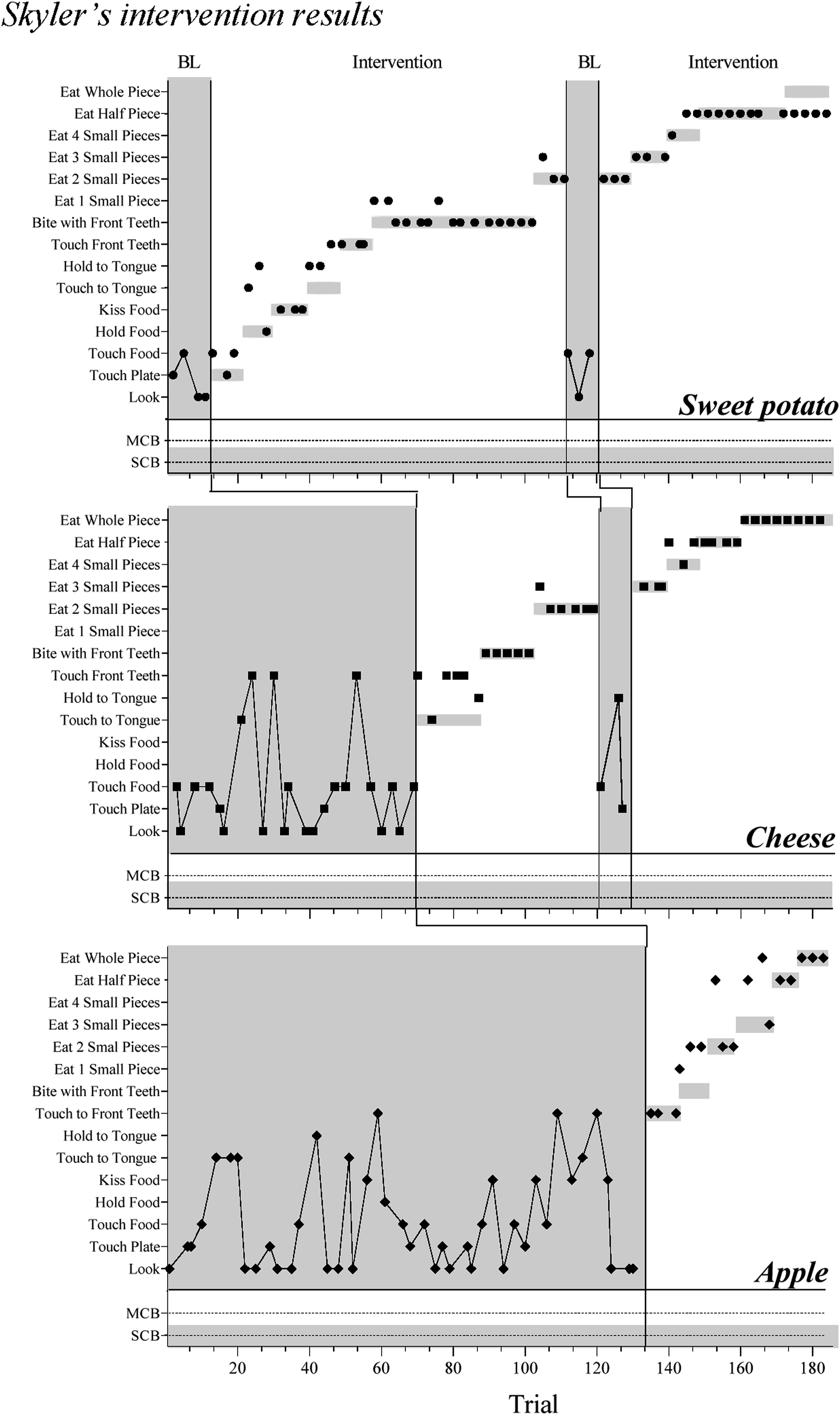
Each trial, each time Skyler came to the treatment table, he would choose one of the foods to engage with (sweet potato, cheese, apple) and select what he wanted to do with it amongst the choices visible on the board. Once Skyler engaged with one of the foods and returned to his reinforcement space, that food was removed for the subsequent trials until all three foods were removed. For example, if Skyle chose to engage with apple on trial 7, when he returned to the table for trial 8, only the boards for sweet potato and cheese were present. After Skyler cycled through the three foods, they were replaced, and the trials began again.
The baseline procedures were explained to Skyler, which was sufficient for him to understand. The first author told Skyler he could let her know if he was uncomfortable with any of the procedures; if so, they could modify them. To promote autonomy, we designed the baseline, and subsequent intervention, such that Skyler conducted each trial mostly independent of the analyst (i.e., he self-managed much of the procedures). At the start of each trial, the analyst would ask Skyler to come to the table. Already present at the table were the laminated boards indicating which responses were available for the full synthesized reinforcement, the target foods, and his preferred food. Skyler would observe the boards, select a food to engage with, take a Twizzler piece, and return to his computer area. The analyst would then remove that food and board from the desk (or would replace all boards on the desk). After stable responding was observed for a given target food, the intervention was introduced for that food only.
Differential Reinforcement Without Escape Extinction Intervention
Intervention was identical to baseline with the addition of a differential reinforcement contingency. In addition to the full synthesized reinforcement contingency, a partial reinforcement contingency was introduced for some responses. The partial reinforcement contingency included access to the computer area and full attention and cooperation from Skyler’s teacher, but for a shorter duration of time (approximately 1 min), and without access to a piece of Twizzler. Thus, partial extinction was in effect for the edible reinforcer portion of the synthesized contingency.
Any responses at or above the criterion would result in full reinforcement; any responses below would result in partial reinforcement. The partial reinforcement contingency was indicated to Skyler with a red sticker (See Figure 2, middle image, for an example). Once Skyler met or exceeded the criterion in place for the full reinforcement contingency across three consecutive trials for that food in the absence of any MCB or SCB, the criterion was increased one level. For example, if Skyler met or exceeded the reinforcement criterion (e.g., touching to lips) for cheese for three consecutive trials without any MCB or SCB, the criterion was increased to the next level (e.g., touch to tongue). The first full and partial reinforcement contingencies of intervention were determined by Skyler’s responding during baseline. Subsequent criteria increases were determined by Skyler’s responding during the previous trials. For example, across four baseline trials for sweet potato, Skyler chose to touch the plate, touch the food, and look at the food; thus, we chose touching the plate as the first full reinforcement criterion in intervention.
We staggered the introduction of the intervention across the three foods. Therefore, in each session, some of the foods may have still been in baseline and some may have been in intervention, depending on the phase. When the full reinforcement criterion was met for a given food, the analyst changed the reinforcement criterion level on the respective board. The analyst continued to change the reinforcement criterion across the preconsumption and consumption reposes as Skyler was successful, all the way up until consuming the entire bite of the target food. Skyler had the opportunity to behave above or below the set criterion for full reinforcement, a key feature of changing criterion designs. The intervention was complete once Skyler reached the terminal criteria (i.e., eating a whole piece of food) across three trial-blocks.
Contingency Reversal
For two of three foods, we reversed to baseline conditions consisting of access to the full reinforcement contingency for any response (i.e., differential reinforcement without extinction). Once responding was observed to revert to baseline levels, we reinstated the intervention procedures, setting the reinforcement contingency at or above the previously met performance criteria.
Reversing to baseline conditions could be undesirable for caregivers given progress may temporarily stalled and the amount of time a practitioner spends in baseline should be carefully considered. The way in which our intervention was designed allowed us to briefly (e.g., three trials) return to baseline for a single food while the other two remained in treatment.
Assessment of Progress
Progress was assessed by entering the data into the line graphs and visually analyzing the results. Attention was paid to whether Skyler was meeting the criteria each session, engaging in any minor or severe behavior, and choosing (or not) to participate.
Overall, Skyler demonstrated success across all target foods in that he increased his consumption of those foods compared to baseline levels and consumed entire bites of two out of three target foods. Skyler’s baseline and intervention data are depicted in Figure 3. The data for sweet potato, cheese, and apple are depicted in the top, middle, and bottom panel, respectively. For sweet potato, during baseline, Skyler elected to touch the plate of food or look at the food. An approximate average for these responses was determined, and the first reinforcement criterion during intervention was set at touching the plate of food. His responding met or exceeded the criterion for the first seven intervention steps. Skyler’s responding decreased to lower levels once baseline conditions were put back in place. Once the intervention was reintroduced, his responding met or exceeded the criterion in four of the five steps. When the criterion was increased to swallowing the entire bite of sweet potato, Skyler elected to only eat half of the bite. Skyler’s naturalistic extension results.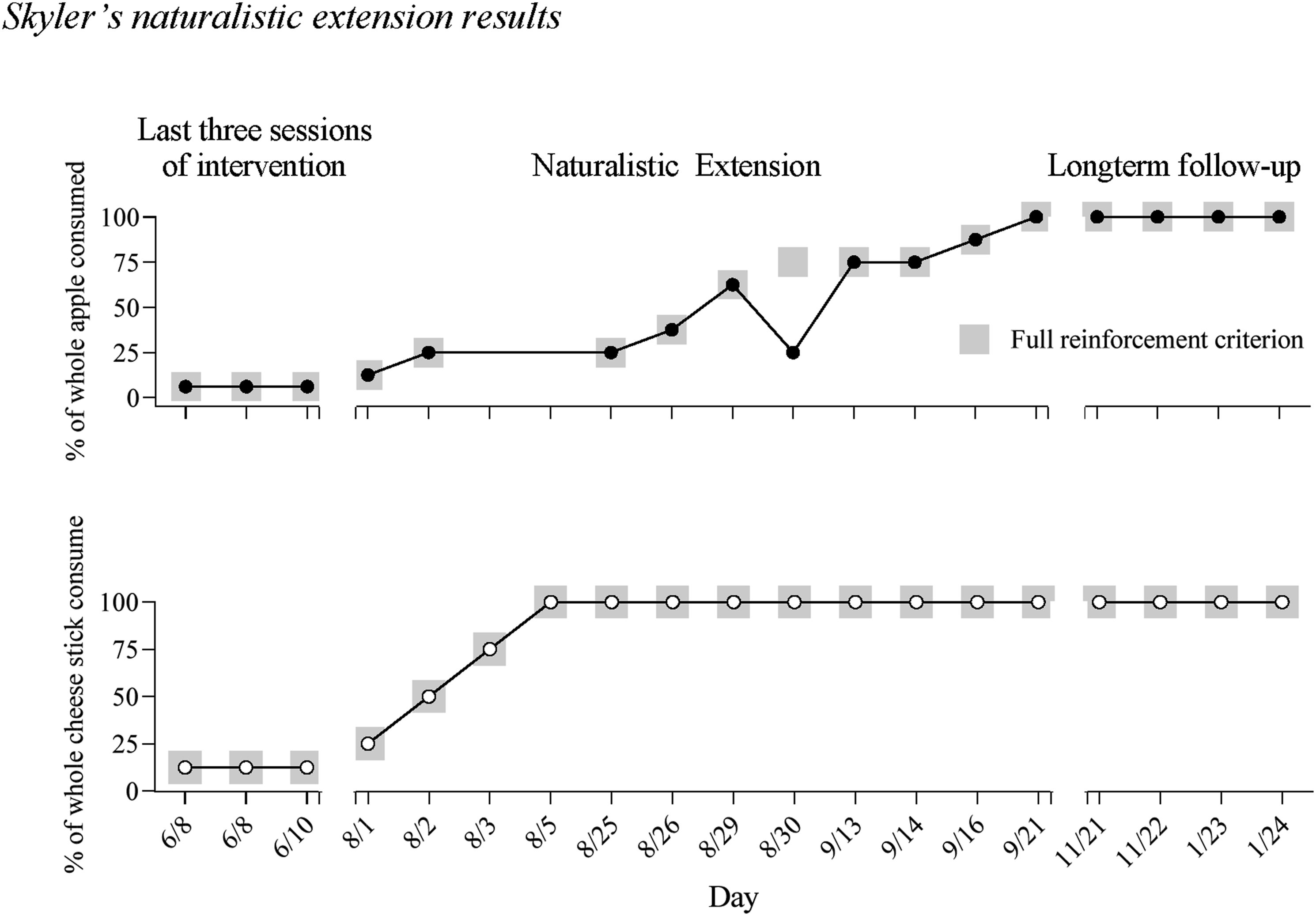
For cheese, Skyler’s responding was more varied during baseline, but he did not elect to interact with the cheese beyond touching it to his teeth. The first full reinforcement level was set to touching it to his tongue, and his responding met or exceeded the criterion in the first three steps, returned to lower levels during baseline conditions, and again met or exceeded the criterion when intervention was reintroduced. Responding was similar for apple in that it was varied during baseline but became more orderly once the intervention was in place. Skyler did elect to consume full bites of both cheese and apple.
The intervention took a total of 17.5 hr across 35 days, over the span of four months. No instances of MCB or SCB were observed, and Skyler chose to participate in the intervention during 100% of scheduled opportunities. However, on several occasions (e.g., a Monday holiday), the analyst asked Skyler if they could make up a session on a non-scheduled day (Tuesday or Wednesday); he sometimes agreed to the schedule change and sometimes said no.
A second independent observer collected data for 100% of the preference analysis, 30% of sessions across baseline and treatment, and 75% of sessions during the extension. Interobserver agreement was calculated by hand. Data were compared on an item-by-item agreement per trial. The number of agreements were divided by the total number of agreements and disagreements and multiplied by 100. An agreement was scored if both observers recorded the same event(s) on a given trial. For example, an agreement would be scored if both observers recorded that Skyler selected “apple” and completed “touched to teeth” in a given trial. Interobserver agreement for the preference assessment was 100%, for baseline and treatment 99%, and for the treatment extension 100%.
8 Complicating Factors
There were several complicating factors associated with conducting an intervention for food selectivity in a school. First, we were beholden to school schedules and activities. Sessions were sometimes disrupted by another student’s needs (e.g., needing the room cleared), fire drills, and school holidays. Second, although we interviewed Skyler’s parents for medical related information and consulted an onsite SLP, we did not have access to a nutritionist to help select target foods nor did we request a formal medical workup from a healthcare professional. Access to a transdisciplinary team may be challenging for practitioners working in applied settings such as homes and schools with limited resources. This didn’t appear to affect the efficacy of our intervention, but components of the intervention may have been improved with additional professional input. In addition, there is very little research on behavior analytic interventions with older children and adolescents. Most research includes children under the age of six. Thus, there were no known clinical guidelines or best practice available when working with a child like Skyler. This highlights an additional benefit of incorporating trauma-informed care strategies that prioritize the physical and emotional safety of participants.
9 Access and Barriers to Care
An important, and we believe necessary, feature of the intervention was to allow Skyler to choose the schedule of and level of participation in the intervention sessions. This allowance represents both an increased access and a barrier to care, in that we believe it was a necessary component for Skyler to voluntarily participate, but also a barrier in that the process took longer. The entire process duration likely could have been reduced by half had we run sessions each day or ran multiple sessions within one day. However, we do not know if we had selected a denser schedule if Skyler would have opted out of the session more often.
Although we were able to influence Skyler’s eating habits at school, a barrier to overall care is that the intervention was only implemented at the school and by school staff. Although the presenting problem persisted across all settings of Skyler’s life, we were only able to intervene at school. The continuity of care across multiple settings (home, school, community) remains a barrier in many human service delivery models.
10 Follow-Up
Social Validity From Skyler.
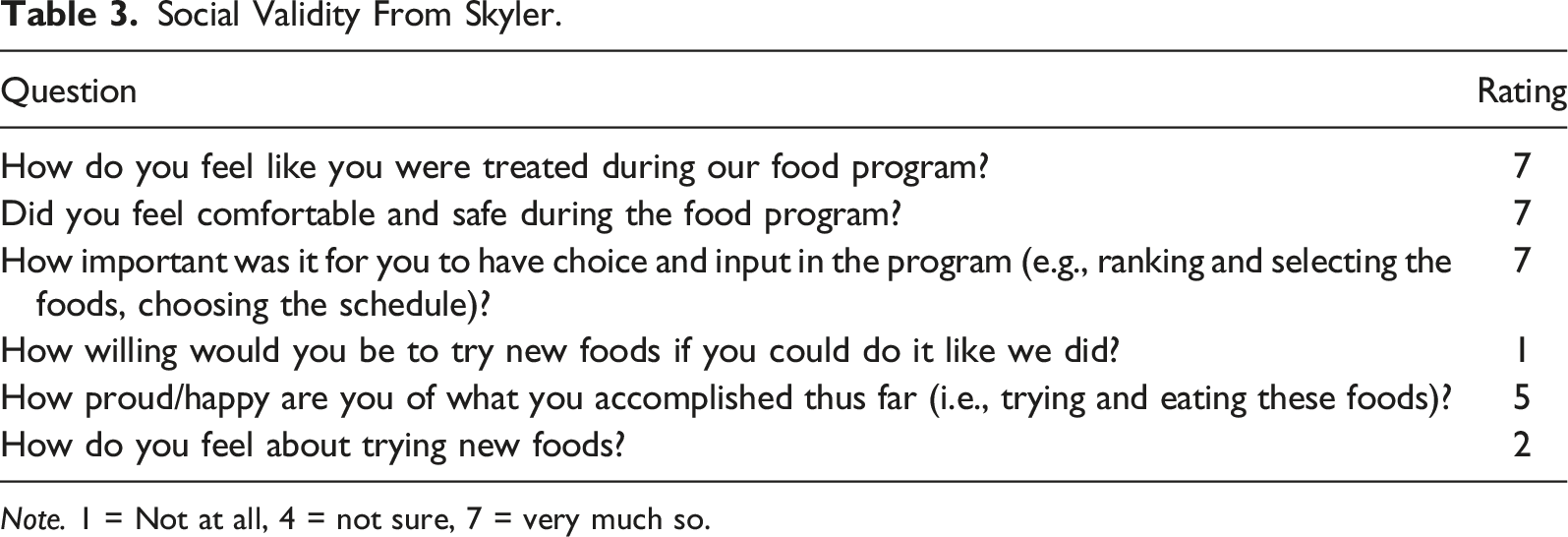
Note. 1 = Not at all, 4 = not sure, 7 = very much so.
Social Validity From Skyler’s Teacher, Who Observed the Intervention and Implemented the Naturalistic Extension.
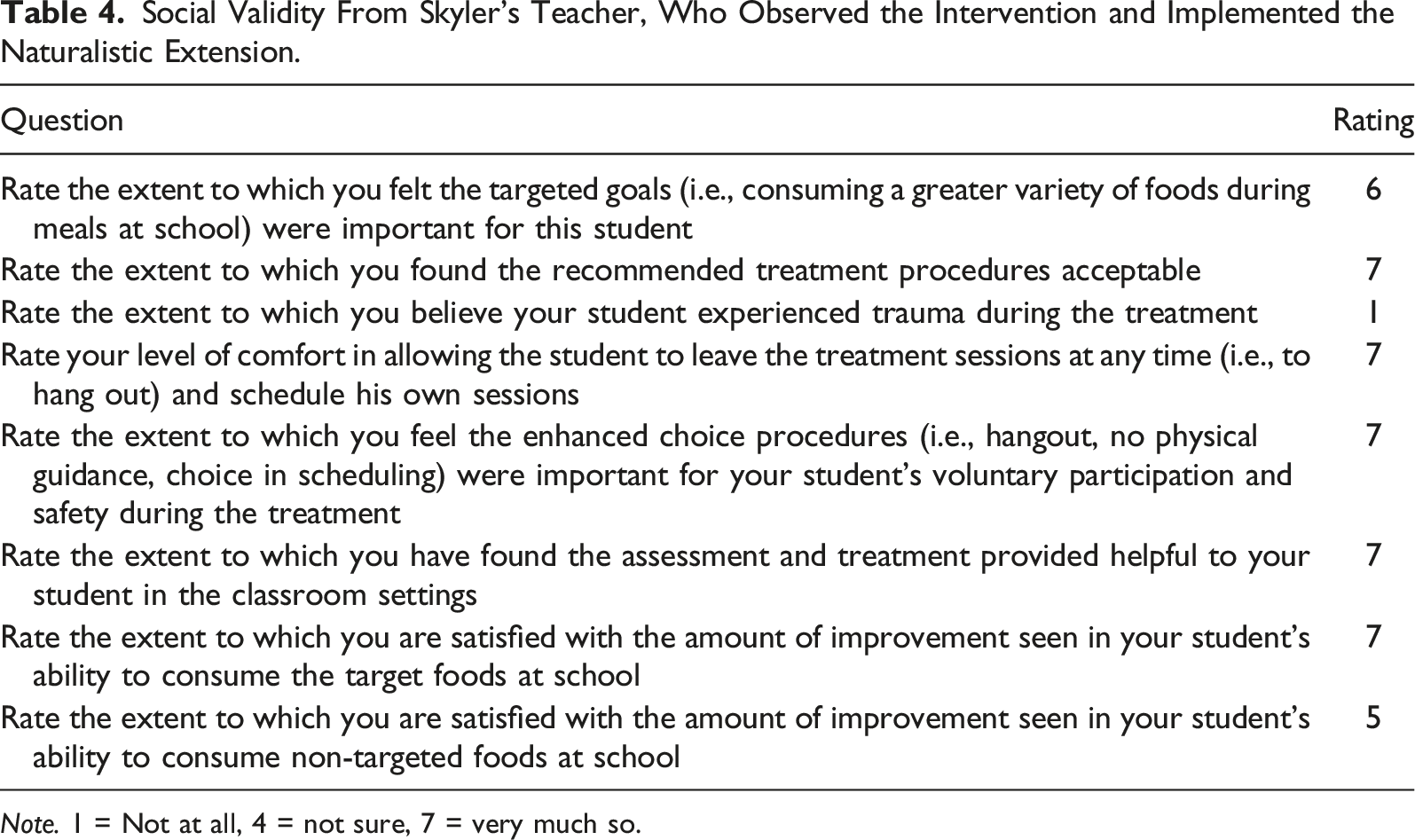
Note. 1 = Not at all, 4 = not sure, 7 = very much so.
The management of the procedures and extension was then transferred to Skyler’s classroom teachers in what we called a naturalistic extension. This extension of the intervention was not a controlled, systematic evaluation. Instead, Skyler’s teachers were encouraged to gradually increase the amount of the target foods he was consuming and to incorporate the procedures into his lunch period. The new expectation was to eat a gradually increasing amount of a cheese stick and apple with his lunch, thereby expanding his regular diet.
These new expectations were expressed to Skyler verbally. The visuals and board were no longer present (e.g., “Today you can eat two bites of apple and two bites of cheese if you’d like the candy in your lunch, but you don’t have to if you don’t want to”); instead, he was told the number of bites of apple and cheese were required each day to receive access to the candy in this lunch. Sweet potato was discontinued following the first phase of the intervention after Skyler expressed his personal distaste for the food. Skyler’s family and school team had no objections to using contingent edibles as he was already consuming candy as part of his lunch prior to the intervention.
Results of this extension and follow-up are in Figure 3. Skyler met the criterion in place for all but one day of the extension. Anecdotally, the apple was deemed too “mealy” that day. Apples were also unavailable for two days on 8/3 and 8/5. Skyler continued to eat an entire cheese stick and apple with his lunch up to two months following the extension in the absence of any minor or challenging behavior.
11 Treatment Implications of the Case
With consistent input throughout intervention from Skyler, an adolescent with autism and a highly restrictive diet, we improved his selective eating during mealtimes at school via a process that incorporated shaping and differential synthesized reinforcement without escape extinction while prioritizing assent and choice making. Taken together, food-related behavior data and Skyler’s verbal reports suggest the intervention was efficacious and did not appear to be correlated with traumatic experiences.
The current study is a preliminary proof of concept of what we argue is trauma-informed, practitioner-oriented ABA research. Further replication and validation are certainly warranted; however, this evaluation presents several novel contributions to the behavior analytic feeding literature and implications for practitioners. First, because Skyler is 12 years old, he falls within an age range that is relatively underrepresented in behavioral feeding research. Thus, if working with older clients, strategies included in this approach may be helpful. Second, although previous studies have incorporated various choice-making procedures (e.g., Fernand et al., 2016; Tereshko et al., 2023), the current study’s procedures are among the first in the behavior analytic feeding literature to explicitly describe procedures wherein the individual could altogether withdraw and reinstate assent during every moment of intervention (see Morris et al., 2021, for a review of assent procedures in ABA research).
While the provision of assent and assent withdrawal presents a novel contribution to the food selectivity literature, it also engenders questions around when we can and cannot honor assent withdrawal from an intervention. Behavior analysts help children and families with a number of activities, such as medical visits, immunizations, and traffic safety, to name just a few, which often need to be completed regardless of assent. Relatedly, our procedures would have likely looked a lot different had Skyler had life threatening or serious medical issues related to his food selectivity. As behavior analysts begin to incorporate more choices into service delivery and research, it should be clear under what circumstances these procedures are being recommended. Families and their care teams should always prioritize the child’s life and wellbeing above all. Certainly, if more restrictive practices were necessary for a child’s wellbeing, practitioners could incorporate strategies included in the current study’s procedures (e.g., multiple choice-making opportunities, synthesized reinforcement, trauma-informed care strategies) when such cases are referred for behavioral services.
As third novel contribution, to our knowledge, this represents the first behavior-analytic food selectivity study in which information regarding the social validity of goals, procedures, and outcomes was solicited from the participant and reported (Ferguson et al., 2019; Hanley, 2010), although other studies have recruited social validity of procedures from participants (e.g. Gregori et al., 2023), Skyler influenced the goals of the intervention by choosing which nonpreferred foods—among a larger list nominated by caregivers and verified to be nonpreferred via preference analysis—should be included and targeted in the intervention. Skyler evaluated the acceptability of the procedures and the meaningfulness of the outcomes in the post-intervention questionnaire, in which he reported being treated well and feeling safe. It is notable, however, that Skyler said he was not interested in trying new foods in the same manner again despite reporting being treated well. Ideally, we wanted to create a therapeutic context that Skyler would not only participate in but want to participate in again; this, however, is a helpful data point for future research. Practitioners should be encouraged to recruit feedback from relevant caregivers and clients throughout our therapeutic relationship.
Taken together, the methods and outcomes reported in the current study appear to be in alignment with procedural commitments of TIC. Unique procedural commitments served to minimize potential trauma experienced during an ABA intervention. Evaluating such an intervention may help engender much needed research to include and support participants with documented trauma histories, post-traumatic stress disorders, and those with ARFID diagnoses.
12 Recommendations to Clinicians and Students
Although this is but one application of a behavior analytic intervention for food selectivity, Skyler’s case elucidates several recommendations for clinicians, specifically behavior analysts, and students of the field. One, the current study underscores the feasibility, acceptability, and the potential necessity of incorporating procedures that promote choice, shared governance, and assent. Although we did not conduct a comparison between an intervention with these components and one without, Skyler and his school team reported they felt these components were important to the success of the intervention. In addition, allowing Skyler to participant in the design process and giving him control over participation did not prevent achieving the intervention goals. Every client is different, however, and practitioners should individualize the intervention to meet their unique needs.
Second, this case includes procedural decision-making that highlights de-emphasizing compliance as a main intervention goal. As an example, towards the end of the intervention, Skyler reported he did not prefer the sweet potato and elected not to meet the criterion when it was increased to consuming the entire bite. Instead of increasing the intensity of the intervention or attempting to modify the procedures to get Skyer to eat the sweet potato, we honored this preference and moved on with the two foods we did observe success with. We made this decision because we observed him taste and eat small bites of the sweet potato through several sessions; that is, he interacted with the food enough to develop an informed opinion, and also, he made progress with the two other foods. The progress with the other foods showcases that there wasn’t an issue with the intervention; the election to not eat the sweet potato was truly a personal preference. It is recommended that practitioners target multiple foods during an intervention. If progress were to stall and only one food was being targeted a time, it would be unknown if the stagnation was due to a personal preference or an issue with the intervention.
There are also several considerations if a practitioner is interested in addressing the food selectivity of a client for the first time. First, they should refer the case to other professionals if the eating issues appear to be more severe than a food selectivity case. This knowledge will come from a comprehensive screening process that ascertains medical information, the child’s current eating repertoire, and previous interventions. If there is any suspicion that the child may have additional medical issues contributing to the food selectivity, the practitioner should recommend a medical evaluation from a professional. In addition, specifically with older, verbal clients, practitioners should consider referring out to other professionals conducting interventions such as cognitive behavioral approaches which have success with similar populations. Second, practitioners should consume relevant content and training on the topic (journal articles, webinars, trainings) and recruit supervision from someone with experience. Third, they should seek out a community in which to practice and not practice on an island, to gain feedback and have a built-in accountability system. This community is ideally made up of colleagues and professionals that they trust, have experience in this realm, and they can easily share data and concerns. And fourth, safety procedures should be incorporated including training on First Aid and CPR, a safety plan if there is an allergic reaction or other medical issue, and the child and their care team (family or school team) should have the ability to end a session at any point if they feel uncomfortable.
Footnotes
Author’s Note
The authors would like to thank Zohaa Awan and Mark Casassa for their assistance in collecting and organizing data for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request. Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Author Biographies