
Abstract
Social anxiety disorder (SAD) is characterized by marked and persistent fear in social situations in which one may be exposed and/or anticipates being exposed to external evaluation and in which embarrassment/humiliation may occur. Acceptance and Commitment Therapy (ACT) has been showing promising results in several disorders, including adult SAD. Considering this evidence and given that adolescence is typically the age of onset for SAD, we developed the ACT@TeenSAD, which is a manualized approach to adolescent SAD delivered via videoconference. It encompasses 10 weekly, 90-minute sessions targeting core pathological processes and fostering higher levels of psychological flexibility; it also includes two booster sessions. The current work illustrates the case conceptualization and therapeutic trajectory of a 17-year-old adolescent (Josie; pseudonym) with a 5-year history of SAD that underwent the ACT@TeenSAD. During the course of the intervention, Josie found purpose and learned life skills to cope with adversity, especially in socially relevant situations. This aligns with the pre- to post-intervention progress shown by Josie (using the Reliable Change Index), particularly in measures assessing acceptance, psychological inflexibility, and self-reported social anxiety. Josie’s case study gives preliminary evidence of the acceptability and feasibility of the ACT@TeenSAD, making it a helpful tool for therapists to become familiarized with. The current work also discusses the limitations of the intervention and presents practical challenges and suggestions thought to be useful for therapists.
1 Theoretical Background and Basis for Treatment
Social anxiety disorder (SAD) is characterized by a marked and persistent fear or discomfort felt in anticipation, during, and after engaging in social situations (i.e., social performance, social interactions, and being observed by others) in which one may be exposed and/or anticipates being exposed to external evaluation that may result in embarrassment or humiliation to the self. Hence, those social events are avoided or faced with intense discomfort, having a significant impact on the daily functioning of those suffering from SAD (American Psychiatric Association, 2013). The experience of social anxiety is intrinsically linked to the evolution of the human species. The human mind has evolved for survival (i.e., the greater the ability to anticipate and avoid danger, the more likely one is to survive and continue the species; Buss, 2015). This also applies to social hazards that constitute potential threats that can happen in any social situation and, therefore, may represent a source of suffering. Despite the current modern and overall safe world, the human mind still functions in quite a primitive way, always alert (i.e., evaluating, judging, and criticizing) to possible social dangers (e.g., being excluded from a group; Oliver & Bennett, 2020). So, the social anxiety response is universal, necessary, and predominantly adaptive. However, when social fears are constant and pervasive, difficulties can arise, leading to maladaptive trajectories and possible psychopathological outcomes. This is the case for SAD that lies at extreme end of the social anxiety continuum (Kashdan et al., 2014).
From an Acceptance and Commitment Therapy (ACT; Hayes et al., 1999; Hayes et al., 2006) stance, the difference between normative social anxiety and SAD has to do with the reaction and relationship the individual establishes with experiencing social anxiety symptoms, rather than the intensity or frequency of the experience of social anxiety in itself. Acceptance and Commitment Therapy is unified model of behavior change that intends to create a valued, engaged, and meaningful life, by developing a healthier relationship with difficult private experiences (i.e., thoughts, emotions, and memories). Ultimately, ACT aims to provide the individual with useful strategies so that they can deal with difficult experiences in a more flexible way, thus promoting value-based choice over one’s behavior. Alternatively, ACT proposes that being inflexible in trying to avoid those difficult inevitable experiences is not functional or useful to a meaningful life. That psychological inflexibility (PI) is proposed as the primary source of psychopathology. According to Hayes et al. (1999, 2006), PI relates the following core pathological processes: • Cognitive fusion (i.e., entanglement/attachment with thoughts so that they dominate one’s awareness and influence one’s behavior); • Experiential avoidance (i.e., attempts to control the appearance, frequency, or intensity of unpleasant private experiences); • Lack of contact with the present moment (i.e., moment-to-moment experience is dominated by a conceptualized past and future—actions are more motivated by the cognitive products of the mind rather than by the reality experienced in the here and now); • Conceptualized self (i.e., the self-description made of all descriptions, evaluations, and judgments that oneself becomes attached with); • Inaction, impulsivity, or avoidant persistence (i.e., behavior repertoire that moves one away from a valued meaningful life—uncommitted action can be described as impulsive, reactive, or automatic, often motivated by experiential avoidance); • Unclear, compliant, or avoidant values (i.e., disconnection from one’s own values, and a neglect of what is truly important in one’s life—absence of guidance/motivation for more useful/effective actions).
From this point of view, when adolescents with SAD avoid social events, they are not avoiding events per se but rather the internal experience associated with those events. Accordingly, PI has been found to relate to social anxiety in non-clinical adult samples (Tillfors et al., 2015) and in clinical adult samples (Fergus et al., 2012). Some PI processes have also been linked to social anxiety difficulties in non-clinical adolescent samples (Cheng et al., 2022; Kashdan et al., 2014; Shimoda et al., 2018) and in clinical adolescent samples (Venta et al., 2012).
Based in those ACT premises and the processes underlying PI (e.g., Hayes et al., 2006), adolescent SAD can be conceptualized as social contexts fostering high levels of cognitive fusion, resulting in a behavior repertoire that is often guided by inflexible linguistic representations rather than by the contingencies of the environment. Individuals with SAD have been found to systematically resort to emotional regulation strategies that rely on experiential avoidance (Kashdan et al., 2014), which, in turn, seems to increase social anxiety (Epkins, 2016; Kashdan et al., 2013). Experiential avoidance has been correlated with social anxiety in adolescents (Kashdan et al., 2014; Shimoda et al., 2018). Previous works have found that this experiential avoidance, when unyieldingly used, becomes both a product and a cause of exacerbated anxiety, being unhelpful, harmful, and counterproductive (Asher et al., 2021). Moreover, contact with the present moment decreases as individuals resort more and more to experiential avoidance. The conceptualized self, based on the past and future, crystallizes as primary emotion regulation strategy, further promoting PI (Hayes et al., 2006). This culminates in adolescents with SAD being unable to act in a way that is consistent with what is valued by them.
Alternatively, ACT, as an intervention approach, aims to foster psychological flexibility (PF; Hayes et al., 2006). PF is the ability to be in the present moment with full awareness and willingness to be with the internal experience non-judgmentally and to act in a way that is congruent with one’s core values. Higher levels of PF translate into more useful and effective action, more vitality, and more purpose (Hayes et al., 2012). Acceptance and Commitment Therapy relies on 6 core principles to develop PF, which refer to the other end of the continuum of the processes defined for PI (see above). The triflex model groups these PF processes into 3 main pillars (be present, open up, and do what matters; Harris, 2009). One pillar—be present—comprises the observing self and contact with the present moment, both revolving around living the here-and-now experience non-judgmentally and in a detached way. Another pillar—open up—regards defusion and acceptance, both about holding a distant and allowing/willingly relationship with thoughts and feelings, seeing them for what they truly are (i.e., transitory products of the mind). The last pillar—do what matters—refers to value definition and committed action, taking into consideration life-enhancing and meaningful action, irrespective of discomfort or unpleasant private events.
Acceptance and Commitment Therapy has been proposed as an increasingly appealing evidence-based approach for the treatment of diverse mental and physical health problems (A-Tjak et al., 2015), improvement of engaged living, and attenuation of the impact of experiential avoidance (Spencer et al., 2022). The acceptability and efficacy of ACT interventions for adolescents with various mental disorders, though not specifically with adolescent SAD, has also been proposed recently, with decreased levels of PI and increased life satisfaction (Moreno & Blasco, 2019). Recent reviews provided empirical evidence for the efficacy of ACT in the treatment of SAD (Caletti et al., 2022; García-Pérez & Valdivia-Salas, 2018). However, only one work that met inclusion criteria for those reviews considered adolescent samples: Azadeh et al. (2015) worked with adolescent girls diagnosed with SAD and found that ACT performed better than a waitlist control group in diminishing self-reported interpersonal problems and in increasing PF.
So, there is an evident need to further explore the usefulness of ACT-based interventions for adolescent SAD. A case study approach might be useful in this regard, providing for an in-depth understanding of the way ACT theoretical premises may be put into practice for ameliorating adolescent SAD. Case studies are optimal tools to provide initial evidence on theoretical assumptions, which may then be used to inform theoretical and practical applications of psychological counseling and psychotherapy to specific phenomenon (Stiles, 2007), such as SAD. As such, the current work intends to present a clinical case study detailing the trajectory of an adolescent girl diagnosed with SAD throughout an online manualized ACT intervention program (i.e., ACT@TeenSAD). Specifically, we will be assessing preliminary feasibility and acceptability, based on the detailed qualitative description of the adherence to the intervention sessions and their specific dynamics, and individual outcomes indicators based on pre- to post-intervention self-reported social anxiety, psychological inflexibility and acceptance and action.
The ACT@TeenSAD Intervention
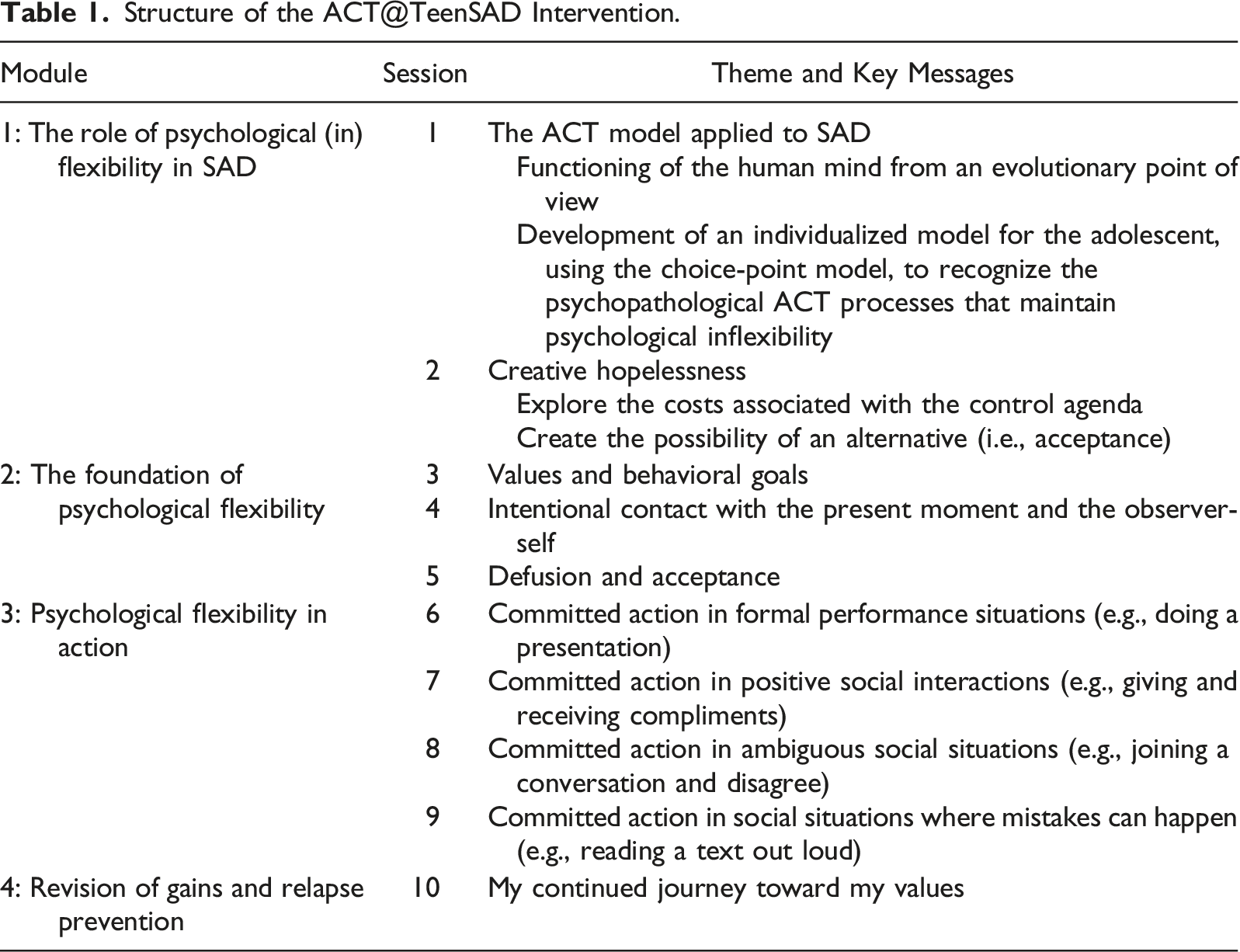
The ACT@TeenSAD was developed within the research project TeenSAD: Changing the Course of Social Anxiety in Adolescence (ClinicalTrials.gov Identifier: NCT04979676). It is a manualized and structured intervention approach based on the PF model proposed by ACT (Hayes et al., 1999), specifically on the triflex model (Harris, 2009), and further resulted from extensive research on ACT, ACT for SAD, and ACT for adolescents. It is designed to be an entirely online intervention, making it necessary to consider specific aspects so that the therapeutic relationship is well established, and the therapeutic outcomes can be as productive as possible (cf. Recommendations).
Structure of the ACT@TeenSAD Intervention.
2 Case Introduction
Josie (J.; pseudonym) was recruited within the procedures defined for the research project TeenSAD: Changing the Course of Social Anxiety in Adolescence (ClinicalTrials.gov Identifier: NCT04979676). These include (1) screening phase where adolescents attending the 10th and 11th grades of collaborating schools filled in the Social Anxiety Scale for Adolescents (SAS-A; La Greca & Lopez, 1998); (2) clinical diagnostic individual interview applied to all willing adolescents who scored one standard deviation above the mean for the Portuguese adolescent sample on the SAS-A (Cunha et al., 2004); and (3) random attribution of adolescents to one intervention condition or to a waitlist condition based on having a primary diagnosis of SAD and on not having psychotic symptoms, not being included in the special education system, and not being currently receiving psychological interventions. All procedures were carried out only after having obtained informed consent from parents/legal guardians and oral consent from the adolescents themselves.
J. is a 17-year-old girl that was allocated and participated in ACT@TeenSAD following those recruitment procedures J.’s case was selected as an instrumental case, meaning that she was considered to portray a typical SAD presentation (including being female) and that her progression through the therapy occurred as expected (i.e., J. actively engaged all sessions of the program and did all the in-session and in-between session challenges; see below).
Josie’s Scores From Baseline to Post-Treatment and Clinical Improvement.
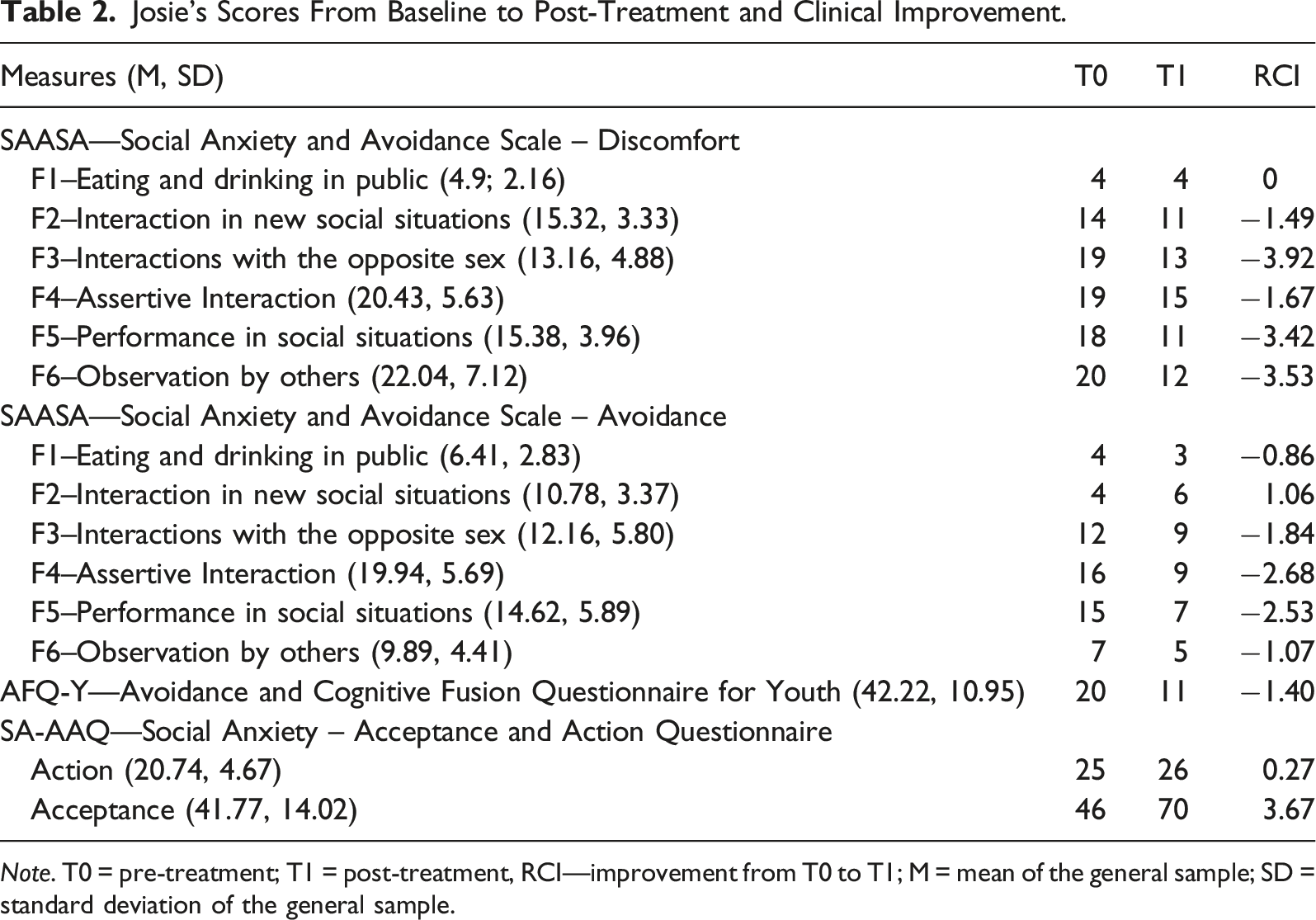
Note. T0 = pre-treatment; T1 = post-treatment, RCI—improvement from T0 to T1; M = mean of the general sample; SD = standard deviation of the general sample.
3 Presenting Complaints
At the start of the program, J. was attending her penultimate year of high school and presented a 5-year history of SAD. She portrayed marked fear of social and performance situations such as presentations in class, asking and answering questions in class, speaking to unfamiliar people, exposing herself, or giving her opinion due to concerns of being negatively evaluated by others and being rejected. Her main fears were that “people can judge me,” “they can laugh at me,” “they are always observing” and “they will not accept me as I am.” In addition to her thoughts about negative evaluation, when facing challenging social situations, J. described experiencing physiological symptoms, such as being very nervous, tense, trembly, always blushing, and with racing heartbeat and breath. To cope with her discomfort, J. would usually avoid social interactions (“get away from the situation,” “stare at my phone,” “I stopped speaking”), reduce her interventions to a minimum (“stay in my corner”), or think/plan before speaking (“what I can say, in which tone, the way I will say it”).
4 History
J.’s personal history was collected from the pre-treatment assessment MINI-KID (Sheehan et al., 2010; Portuguese Authorized Version by Rijo et al., 2016) and from a second interview conducted after treatment, by the psychologist that delivered the intervention.
J.’s father is Portuguese and her mother is German, and until the age of 12, J. lived in Germany with them and her younger brother. J. recounts her childhood as lovely and fulfilled, having enjoyed the German lifestyle, social life, school schedule, and, especially, the language. She details her favorite activities were spending time in the local village, going to local parties, having sleepovers with friends, and overall living a socially active life. Importantly, J. felt a sense of belonging and of being herself (i.e., authentic), without the need to adapt to others. Also, despite mentioning some teachers saw her as a reserved person, she depicted herself as not shy, but rather interactive and proactive, stating that anxiety didn’t negatively influence her life. The German school regime (i.e., finishing classes always before 2 p.m.) allowed more freedom to better enjoy her days with more free time.
J, moved to Portugal in the 7th grade, and that change constitutes a pivotal turning point in J.’s relationship with social anxiety. She described the transition as a very psychologically demanding period, especially since she didn’t know how to speak Portuguese. J. recalls the first day of the 7th grade as a moment of great acknowledgment and insight of how she did not know how to communicate with peers, generating feelings of loneliness and exclusion. Her accent was something she feared people would judge, leading to feelings of being observed and uncomfortable. To cope with her discomfort, J. chose to not talk unless it was absolutely required (“it was better not to talk than risking something bad to happen”). Because she was not willing to communicate with other people, making friends turned out to be very difficult and J. increasingly isolated from her classmates (“I constantly wished for a new German girl to enter my class”). Owing to all of this, J. defines the 7th grade as the onset of her difficulties. Also, from the end of the 7th grade to the 8th grade, J. was bullied by 2 classmates for “always being in my corner” and for not speaking, which exacerbated her social fears and discomfort.
In the 9th grade, J. changed school and described a more positive experience. Adding to the fact that her language skills had significantly improved, J. felt more integrated in the new school and was able to connect with 2 girls from her class. Although she spoke more and her comfort zone broadened, J. reports still feeling very shy and uncomfortable in social situations, resorting to avoidance coping strategies. Over time, her major difficulties shifted to speaking in front of the class (e.g., presentations and answering questions) and interacting with people outside of her safety group (i.e., the 2 girls she felt comfortable with).
J. started considering asking for help when some teachers related care and worry, alerting her for possible difficulties she would face in the future (e.g., internship) due to her shyness. Moreover, close friends were encouraging too. J.’s life goals include finishing high school and continuing her studies to become a veterinary nurse. J. dreams of working with animals. Although she keeps in touch with friends and family from Germany, and visits regularly, she is unsure about returning to her birth country, showcasing an understanding of not being “the same German girl” but an evolved multi-culturally influenced person. Before starting the ACT@TeenSAD program J. was seeing her schools’ psychologist for weekly counseling sessions that were focused on developing J.’s social skills. This intervention terminated before J. started ACT@TeenSAD.
5 Assessment
Establishing the Primary Diagnosis with the Mini International Neuropsychiatric Interview for Children and Adolescents
Baseline assessment was conducted by the same psychologist that delivered the intervention using the MINI-KID (Sheehan et al., 2010; Portuguese Authorized Version by Rijo et al., 2016) 3 weeks before the first intervention session. The MINI-KID is a short, structured diagnostic interview that assesses DSM-V (American Psychiatric Association, 2013) Axis I and the ICD-10 (World Health Organization, 2004) diagnoses in children and adolescents, with the duration of approximately 30–90 minutes. It assesses mood disorders, anxiety disorders, substance-related disorders, tic disorders, disruptive disorders, attention-deficit hyperactivity disorder, psychotic disorders, eating disorders, adjustment disorders, and pervasive developmental disorders. Screening questions are presented for the evaluation of each diagnostic criterion and are answered in a yes/no format. In its original version, the inter-rater reliability was excellent across diagnoses except for dysthymia (Sheehan et al., 2010). For the Portuguese version, there is no study observing inter-rater reliability though it has been previously used for determining diagnosis (Rijo et al., 2016). The clinician received specific training, including role-play exercises, and underwent an initial observation phase of experienced evaluators before she conducted interviews autonomously.
During the interview J. revealed a shy and undemonstrative posture, keeping herself in a corner of the screen and maintained little eye contact. Despite being visibly uncomfortable, J. insightfully described her social difficulties, presenting relevant examples of her day-to-day life. Also, probably due to perceiving these difficulties as interfering with her life, she manifested significant motivation to improve her social skills and quality of life. J. received a primary diagnosis of social anxiety disorder; there were no co-morbidities.
Characterization of J.’s Social Anxiety
At pre-treatment, J. completed a set of self-report measures, that are described next. The Social Anxiety and Avoidance Scale for Adolescents (SAASA; Vagos et al., 2013 adapted from Cunha et al., 2008) is a dimensional and a-theoretical self-report measure of social anxiety that used to assess the degree of discomfort and avoidance over a wide range of social situations across six factors for each subscale: F1–Eating and drinking in public; F2–Interaction in new social situations; F3–Interaction with the opposite sex; F4–Assertive Interaction; F5–Performance in social situations; F6–Observation by others. At baseline, J. showed more evident difficulties in how anxious she felt in interacting with the opposite sex (F3), when performing in social situations (F5), and when being observed by others (F6), given that her scores were at least one standard deviation above the mean found for a sample of adolescent community girls (Cunha et al., 2008). She also had a score slightly above the mean for how anxious she felt and how much she avoided interacting assertively (F4 for anxiety and avoidance) and for how much she avoided performing in social situations (F5). For the remaining anxiety (i.e., F1 and F2) and avoidance (i.e., F1, F2, F3, and F6) measures, she surprisingly scored below average. It could be the case that the avoidance scale in specific is not well suited to the difficulties expressed by J., who seems to be present in most social events (rather than avoiding them) but goes through them with intense suffering and resorting to safety behaviors.
The Portuguese version of the Avoidance and Cognitive Fusion Questionnaire for Youth (AFQ-Y; Greco et al., 2008) by Cunha and Santos (2013) was used to evaluate PI measured by cognitive fusion (i.e., perception of thoughts as an absolute literal truth and not as cognitive products of the mind) and experiential avoidance (i.e., unwillingness to experience private events such as thoughts, bodily sensations, emotions or memories, and using different strategies to avoid, change or control them). Considering the mean values for Portuguese community girls (Cunha & Santos, 2013), J.’ score of 20 is surprisingly below average, indicating low levels of experiential avoidance and cognitive fusion, which contrasts with J.’s reports during the interview and the direct observation made by the therapist during the evaluation. Both clearly indicated high levels of experiential avoidance and cognitive fusion associated with significant impairment and suffering that contributed to J.’s exacerbated social anxiety. This can perhaps be explained by J. being able to notice her thoughts and symptoms that elicited anxiety, despite being highly fused and non-acceptant of her own experience, and describing an overidentification (i.e., cognitive fusion) with them.
To evaluate J.’s experiential avoidance (i.e., lack of acceptance of thoughts and feelings) and unworkable action (i.e., actions that are inconsistent with core values), the Social Anxiety – Acceptance and Action Questionnaire (SA-AAQ; MacKenzie & Kocovski, 2010; Portuguese version by Martins et al., 2011) was used. Considering the mean values for community girls (Martins et al., 2011) for the acceptance subscale, J.’s baseline score of 46 is below average, suggesting difficulties in being willing to be with/to be aware of her internal experience without trying to control, change or diminish it. Regarding the action subscale, J.’s baseline score of 26, is within average. As the behavioral repertoire of adolescents with SAD is known to be limited, it may be that, at the time of completing the pre-treatment assessment, J. did not have the perception that she was not doing things that were important to her. Since J. refused to experience difficult emotions (including social anxiety) for about 5 years, her range of actions is expected to be narrowed, but perceived as naturally so.
J. assessment scores per instrument at pre-treatment (T0) can be found in Table 2. Some of these scores—as stated above—are contrasting with what J. reported during the interview (i.e., fears of risking getting involved in new activities). This may be due to several reasons, namely, J. may have underrecognized social anxiety symptoms as a serious mental health issue (Coles et al., 2016); J.’s responses may have been subjected by social desirability, especially since social anxiety has been associated with perceived/societal stigma (Anderson et al., 2015). It is particularly relevant that J. doesn’t report to markedly engage in some processes associated with PI. Still, we decided to provide J. with the ACT@TeenSAD in its entirety (i.e., no adaptations were made based on these self-reports). This decision was made considering that self-report at this stage may have been biased, that the ACT@TeenSAD is proposed to be a manualized and structure approach, and, more importantly, that PI processes are proposed to be interconnected (hence the hexaflex; Hayes et al., 1999, 2006) and so providing for a holistic ACT approach should be the most ethical, useful, and coherent attitude.
6 Case Conceptualization
J. presents a rigid and inflexible relationship with anxious thoughts, that ends up dominating her actions. This process of cognitive fusion contributes to J.’s difficulties, as it encourages the vision of thoughts as literal truths (thought-reality), and not as subjective and transitory events of the mind (i.e., cognitive products). The symptomatology is perpetuated as J.’s entire life is structured around literalized linguistic representations (“they will mock me,” “if I say something wrong, they will judge me”), rigidifying, restricting, and limiting flexible commitment to valued action. J. also denotes non-acceptance of internal experiences and a judgmental and evaluative attitude toward them (“it is not normal”); these, in turn, promote unwillingness and a shaming conceptualized view of oneself. The costs of trying to control and avoid internal experience, not accepting them as they are, maintain J’s difficulties, because the control agenda exacerbates cognitions, emotions, and sensations perceived as negative. These processes are at the root of experiential avoidance: when fused with thoughts such as “they will laugh at me” or “I will blush,” J. tends to avoid social situations (“stay in my corner,” “not interacting with new people,” “not participating in activities,” “not talking,” “I don’t take risks”), or attempts to neutralize or control the content or frequency of difficult thoughts and emotions by limiting or scripting social interactions when in social events (“I stay in my phone, “I think a lot,” “I compare myself with other people to try and act like them,” “I say bad things to myself”).
Due to the control agenda, mostly through distraction and rumination, and due to the constant judgment and evaluative attitude toward her internal experience, J. does not experience the world in a direct and intentional way. The lack of contact with the present moment keeps J. in a conceptualized past or future (“I think so much that then the moment to act already passed”), rigidifying established conceptions she holds about herself (“anxious and worried person”), about others, and about the social world. The rigid and inflexible relationship that J. establishes with these self-related conceptions maintain her difficulties, insofar as she perpetuates a vision of herself that follows from her fusion with beliefs of being shy, wrong, an “anxious and worried person,” strange or “a person that doesn’t know how to speak.” Thus, the conceptualized self leads to a judgmental attitude toward herself, associated with non-acceptance and avoidance of negative emotional reactions and unwanted thoughts, and with rigid behaviors.
The use of the abovementioned strategies has the paradoxical effect of increasing the unwanted internal experience, pathologizing J.’ social anxiety. These self-perpetuating cycles culminate in actions that are unclear, presently avoidant, and serve the experiential avoidance and the control agenda, seldomly leaving space for the consideration and commitment to actions congruent with what matters deeply in her life (i.e., clearly defined values). This is mostly visible in the school context and in J.’s relationships (e.g., not participating in conversations even with close friends, not interacting during school breaks, not answering questions in class); it is also seen overall in a negative impact in her quality of life (e.g., not sleeping well, not enjoying school, decreasing the number of important friendships, and not being involved in important activities). These unworkable actions deprive J. from adopting more effective and adaptive actions, diverting her from the direction of a meaningful life with vitality.
7 Course of Treatment and Assessment of Progress
J’s therapist in the program was a psychologist with training in Acceptance and Commitment Therapy. The 10 core sessions of the ACT@TeenSAD intervention progressed over the course of 11 weeks, given that one session had to be postponed because it collided with a school activity. As described below, J. adhered to all dynamics proposed in all 10 intervention sessions and provided positive feedback on the way she understood and took them to out-of-session social experiences.
Module 1 (Sessions 1 and 2)
From the beginning of treatment, J. demonstrated a collaborative and interested attitude and revealed good insight into her difficulties and how they interfered in her life. The first session served as the foundation of trust in the therapeutic process. The validation and normalization of difficulties and the sharing of the idea that suffering is inherent to the human condition allowed a de-shaming process early on. J. found the psychoeducational contents were easily understood and essential to foster a different relationship with her own mind (“my mind is not against me”) and used them to develop her personalized model of PI, using the choice point approach. The choice point was applied to a recent situation where she had experienced social discomfort (i.e., speaking in public). She was then able to autonomously draft other difficult social situations, following the same rational.
Also during this module, J. was confronted with the unworkability of her control agenda (i.e., creative hopelessness). To get in touch with the costs of her experiential avoidance, J. was taken through a set of metaphors chosen specifically based on what appeared to be her most distressing PI-related processes (i.e., the shark tank polygraph and the hungry tiger; Hayes, 2005). She also went through experiential exercises (i.e., an adaptation of the exercises “Hands as thoughts and feelings” and “Pushing away paper”; Harris, 2009). The latter opened the possibility for an alternative way of relating with the internal experience (i.e., a more acceptance and distant relationship). J. was able to pick up on aspects of the functioning of the mind and apply them to this second session. She was also able to transfer/apply her insights to a socially demanding situation (i.e., presentation given for English class) by noticing “I know my thoughts were there but it’s like they weren’t in front of me, I tidied them up before speaking because I learnt I wasn’t in danger.” By the end of this module, J. had developed a willingness and openness to be in the sessions with her internal experience, which was pivotal for the rest of the intervention.
Module 2 (Sessions 3–5)
This module comprises the foundation of PF, so J. was taken through the comprehension and practice of its core processes (i.e., being present, opening up, and preparing to do what matters). To foster value-guided action in and out of sessions, and to gain motivation for behavioral change, the third session was dedicated to clarifying the importance of values, highlighting how they differ from behavior goals, and identifying J.’s core values. J. selected courage, authenticity, and health as her top-three core values at that moment. She engaged with the task and easily recognized the vitality and purpose that came with valued living, despite (and perhaps with) the discomfort that comes with it. J. was also led in identifying actions that might help her live her life closer to her valued direction; she mentioned asking more for help, do her final high school exam, and participate more in class as relevant and valued-based actions.
The intervention continued with emphasis on intentional contact with the present moment, which was very well received by J. given that she had, from the start of the intervention, demonstrated a particular awareness regarding lack of contact with the present moment (e.g., “I’m missing out on the good things because I’m always thinking”). Contact with the present moment was introduced as a practical tool that, when trained daily, would help J. to do what mattered in each moment, be it neutral and/or emotionally difficult. In the session, psychoeducation regarding intentional contact with the present moment was done using the anchor in a storm metaphor (Harris, 2009). This process was then trained using both the feet and the breath as anchors. To boost and personalize the practice, different options of anchors were explored in J.’s day-to-day life and this skill was further practiced between sessions. Intentional contact with the present moment segued into self-as-context, as this constitutes the flexible viewpoint from which to observe internal experiences. J. picked up on the impermanence of internal experiences and trusted herself as a permanent existence, making room for the work that followed (e.g., seeing negative affect as normative and temporary states). J. described progress in dealing with difficult thoughts by noticing a greater awareness of her internal experience in the present moment, in a non-evaluative and accepting way.
In the fifth session of the program (and final session of this module), defusion and acceptance were explored. To get J. in touch with her painful internal experience, an exercise was carried out to facilitate noticing thoughts, emotions, and physiological sensations triggered by a challenging social situation chosen by J. (i.e., presentation in class). Josie experienced being with her chosen thought “they are expecting me to fail” in a fused way (e.g., telling it to herself as her mind usually tells it) and then experienced adding to the thought: “I am noticing I’m having the thought that the others are expecting me to fail.” She easily understood this strategy and described an alertness to the fact that the thought was simply a thought and not the unquestionable truth that “people are really expecting me to fail,” finding practical usefulness in this technique for the rest of the sessions. In addition, J. named her story (“the story of not being good enough”) and experienced thanking her mind for the protection-intended thought. In the session, J. described this as the “most intense and sticky” thought, recognizing her state of fusion and difficulty in getting distance from it. However, with between-session practice and J.’s commitment to use defusion techniques, she relied that she gradually experienced more and more awareness and distance from her own cognitive experience. Another goal of this session consisted in promoting acceptance of emotions and physiological sensations through experiential practices and exercises. Starting from the social situation that J. identified previously (i.e., presentation in class), J. was taken through two physicalizing exercises directed at her physiological sensations and then her emotional experience. Starting from the most prominent physiological sensation identified by J. (i.e., blushing), both the adolescent and the therapist purposely induced that same physiological sensation (i.e., using the heat of the hands rubbing on the face skin) and experienced being with it. J. described her blushing as a big and horrible sensation and characterized it as circular, red, very hot, and in movement. She outlined that the exercise was helpful because she had never thought of the characteristics of her difficult sensations (“it was good because I wasn´t completely focused on it but I was seeing its characteristics”), which significantly helped in allowing space for that sensation to be part of her experience, without effortfully avoiding it. Regarding emotions, the most prominent emotion identified by J. was fear. J. described it as being focused on her hands and associated it to a sound-system speaker with maximum volume that vibrated through her body. J. concluded she could look at fear in a different and more curious way stating that “this exercise stops us from thinking about our things as terrible and helps us see that this is just a response from our body (…) It’s not so bad; it is normal.” Significant progress was noted by both J. and the therapist in the relationship that J. developed with thoughts, acquiring a more distanced and less literal view of them, as well as with her sensations and emotions, developing a more detached, flexible, and acceptant relationship with them, so that they might come to have less impact on her behavior.
Module 3 (Sessions 6–9)
This module focused on encouraging committed action based on values in relevant social situations. In all four sessions that constitute this module, J. practiced committed action with the help of a plan that considered the following steps: (1) defining relevant and applicable values, (2) defining actions that help J. move toward her values, (3) defining barriers to committed action, and (4) defining helpers to committed action. The main core values that J. moved toward were courage and authenticity. In detail, J. did a presentation in session 6, had a positive social interaction (i.e., giving and receiving compliments to and from her therapist) in the seventh session, had an ambiguous social interaction (i.e., joining a conversation that occurred between her therapists and an external person invited to join the session, and disagreeing with the subject discussed) in session 8, and being involved in a social situation where mistakes would happen (i.e., calling a stranger on the telephone to ask for biology notes) in the last session of this module and penultimate of the program. The exercises were done in the service of the J.'s values, relying on all ACT processes. The principal barriers to committed action identified by J. were “believe in my stories,” “run (from discomfort),” and “losing contact with the present moment.” The helpers she identified as most useful were “listen to my thoughts and understand them as only thoughts,” “let the thought come and then put it aside,” “anchor in the present moment” with her favorite anchors (i.e., the feet and the breath), and “do it even if I’m afraid.” These verbalizations by J. showcase acceptance toward her internal experience and willingness to be involved in meaningful activities. J. was then able to create further plans and implement committed action linked to her own values during between-session challenges. J. acknowledges having learnt to interact with feared stimuli in new ways: practicing and learning that she can engage in meaningful activities, also when they co-exist with difficult thoughts, anxiety, and unpleasant sensations. Of utmost importance was the fact that value-based actions served as positive reinforcement, and in that way will likely promote the maintenance of these actions after the intervention is completed.
Module 4 (Session 10)
This session aimed to review J.’s journey and accomplishments throughout the program, particularly the strategies/techniques/helpers she experienced as most useful throughout the intervention. When assessing her progress during the program, J. realized an impressive evolution had occurred, in the way she experienced her social anxiety and presented herself in the social world, now in a more truthful and accepting way. Using the bull’s eye exercise (Harris, 2008), she found herself deeply committed to her core values in areas such as school, relationships with friends, and relationship with herself; she also aimed to be increasingly more committed to actions that moved her toward her values in relationships with unfamiliar people. J. identified present moment awareness (i.e., anchoring in the present moment and noticing her experience) and values (i.e., “reminding myself of my values to try to live toward them”) as the most helpful and vital helpers.
As challenging social situations (i.e., current and future) are part of life, it seemed important to recognize obstacles to potential committed actions and establish an action plan to deal with them, encouraging the continued practice of the acquired tools to promote PF after the intervention ended. Though J. was more open with her group and was investing in/enjoying social gatherings with close friends, social interactions with unfamiliar people continued to constitute a challenge. In this way, the main barriers to committed action in these situations were assessed, and it was discussed to what extent the main helpers would be beneficial and sufficient for J. to autonomously manage acting in a committed way in these social contexts. J. found the exploration of barriers helpful because it helped her realize that the obstacles were not new; they were same ones as she had previously faced successfully. She was then able to share her concerns and plan committed actions where she might resort to the helpers in which she trusted.
8 Complicating Factors
J. started attended the ACT@TeenSAD during a very busy school period. Thus, finding compatible scheduling where both the therapist and the adolescent could ensure that all the necessary conditions for online sessions were fulfilled was a complicating factor. However, after necessary adjustments to the weekly scheduling, a scheduled time in the week was agreed and the intervention occurred smoothly through an 11-week period. Additionally, a complicating factor worth mentioning might be that J. had been receiving counseling from her school psychologist shortly before starting the ACT@TeenSAD. Even if it became clear during assessment that the J. could benefit and was motivated to participate in an intervention that was tailored specifically to her social fears, we cannot ascertain as to whether that previous intervention was aligned (or incoherent) to the therapeutic approach utilized in the ACT@TeenSAD intervention.
9 Access and Barriers to Care
During the 10 online sessions, J. presented all the needed conditions to access treatment (e.g., high-quality connection, sound column, webcam, and privacy).
10 Follow-up
To calculate J.’s improvement from T0 to T1, the Reliable Change Index (RCI; Jacobson & Truax, 1991) was applied to each measure. Using the standard deviations of the population of reference, the RCI provides a measure of change in standardized units, enabling to report whether the arithmetical change in a particular measure across treatment corresponds to a significant clinical change. For the SAASA (Vagos et al., 2013 adapted from Cunha et al., 2008) and AFQ-Y (Greco et al., 2008; Portuguese version by Cunha & Santos, 2013), because higher scores indicate increased symptoms, negative RCIs correspond to clinical improvement and positive RCIs correspond to clinical deterioration. The threshold for significant improvement at p < .05 lies at the z-score ≤ −1.96. Therefore, RCI z-scores lower than −0.84 indicate significant change, with a confidence interval (CI) of 80%, and z-scores lower than −1.28 indicate a significant change with a CI of 90% (Wise, 2004). In the case of the SA-AAQ (MacKenzie & Kocovski, 2010; Portuguese version by Martins et al., 2011), because higher scores indicate decreased symptoms, negative RCIs correspond to clinical deterioration and positive RCIs correspond to clinical improvement. The threshold for significant improvement at p < .05 lies at the z-score
In SAASA discomfort subscale (Vagos et al., 2013), J. significantly changed/improved across all factors within the 90% CI, except for F1 (i.e., eating and drinking in public) where no change was verified. Particularly remarkable was J.’s improvement regarding her discomfort in interactions with the opposite sex, performance in social situations, and being observed by others, which were the ones where she reported the greatest difficulties. With respect to the avoidance subscale, J.’s improved across all factors from at least within the 80% CI, except for F2 (i.e., interaction in new social situations) where she had scored below average at pre-intervention and had mildly deteriorated at post-intervention, though still scoring below average. T1 happened shortly after the last session, when J. openly discussed her lingering difficulties while interacting in unfamiliar situations. A recency effect may have led J. to overreport her difficulties in this specific area. It is also noteworthy that, while her self-report at T0 might have represented a narrow view of her unworkable actions based on a 5-year history of SAD, her report at T1 may have considered a rise in awareness of how she handled these situations, compared to how she thought she would handle them if acting committed to her values. The same can be said for the clinically unchanged values she achieved for the action subscale of the SA-AAQ (Martins et al., 2011)—J. continues to report below average values for committed action, which does not reflect her journey through the ACT@TeenSAD intervention. It may be case that J. now understands that, while her committed action is gradually improving, there are still changes she would like to put into practice after the core intervention had ended. Alternatively, she seems to have developed the set of skills that might help her continue that change, given that PI overall, as assessed by AFQ-Y decreased within the 90% CI, and the acceptance subscale of the SA-AAQ showed clinical improvement within the 90% CI. Importantly, this illustrates a different and non-judgmental relationship with the painful internal experience, contrasting with how J. presented at the onset of the program, and paving the way for continued flexible, valued, and committed actions.
11 Treatment Implications of the Case
This case study indicated ACT@TeenSAD to be a feasible and acceptable intervention approach for a typical case of a 17-year-old adolescent girl with SAD, in as much as J. adhered to all sessions and their respective dynamics and was explicit in stating how she understood and took the competences she developed to her daily life outside therapy. Moreover, the ACT@TeenSAD was associated with reliable clinical improvement in most symptoms experienced by J. Change was noticeable regarding the quantitative assessment of self-reported anxiety and avoidance of social situations and of PI processes that are proposed to maintain and exacerbate SAD (Cheng et al., 2022)—change was particularly evident in the social events and skills that J. had identified as more distressing. This change was also evident based on the qualitative feedback observed across the program by the therapist and as expressed by the adolescent. Namely, major changes in the way J. relates with her internal painful experience were observed. By the end of the therapeutic process, J. maintained a non-judgmental and aware relationship with her social anxiety (and all its components), guided by curiosity, willingness, and acceptance. Committed action was no longer systematically avoided as a way of avoiding uncomfortable internal experience. Instead, J’s. actions were then guided by important values and encouraged by a personalized set of helpers (i.e., the strategies that promote the processes of PF). Interestingly, by the end of the program, J. reported not only being able to deal and regulate her own emotions and be with her thoughts in a detached way—reflected in evident changes in PI and acceptance—but also described more competence and ability in helping friends going through similar experiences (e.g., anticipatory anxiety when doing an oral presentation at school), showcasing an in-depth understanding of the shared human experience. Altogether, J. was fundamentally directing herself toward her valued self, making moves toward her values and coping in an adaptive way when setbacks were encountered (e.g., recognizing mistakes are intrinsically human, making new commitments when something took a wrong turn). This openness to life as a continuously challenging experience to be approached relying on ones’ helpers may be sustained by her clinically unchanged—though increasing—scores on the committed action measure.
Other than that, the current work also supports videoconferencing as a useful and robust tool for therapeutic change, specifically with adolescents, born in the tech era, who showcase mastery and are very familiar with online conferencing contexts, (Aschbrenner et al., 2019). The current findings add to the evidence supporting online ACT interventions overall (i.e., iACT; Lappalainen et al., 2021) and reinforce promising results on the efficacy of iACT for adult SAD (Kelson et al., 2019).
12 Recommendations to Clinicians and Students
Because ACT@TeenSAD is a manualized online approach to adolescent SAD delivered through videoconferencing, it requires indispensable technical tools, such as high-quality internet connection, webcam, and an adequate headset. To facilitate the viewing of displayed materials (e.g., images and schemes), adolescents should preferably attend sessions through their computer. Also important is that the therapist must ensure that the adolescent has privacy when attending sessions, so that sessions can be a safe and confidential space for the adolescent to share.
This work also adds evidence to the stance that online sessions can guarantee the desirable high quality of the therapeutic alliance, indispensable to successful outcomes (Backhaus et al., 2012). For that to happen, the therapist must be attentive to certain aspects. To build a strong therapeutic alliance when conducting ACT@TeenSAD online, the therapist should take special care to keep good quality eye contact with the adolescent. It is advised that the self-visualization option be deactivated by both the therapist and the adolescent, simulating a face-to-face interaction, and preventing the self-checking that usually occurs when self-visualizing. Body language is key in therapeutic settings, including online interventions. Thus, the therapist should intentionally use facial expressions and body posture as part of the communication (e.g., nearing and moving away from the screen). Additionally, communication must always be validating, authentic, and based on an ACT-consistent approach.
As with any ACT process, it is of the utmost importance that the therapist and the therapeutic relationship serve as a model of PF when implementing the ACT@TeenSAD. Therefore, the therapist should model acceptance and willingness to be with their own difficult emotions, sensations, and thoughts, by using appropriate sessions/exercises to self-disclose in an adaptive, relevant, and therapeutic way. Also, to further promote a humanizing experience, some exercises of the program (e.g., writing down difficult thoughts in session 2 or inducing an uncomfortable physiological sensation in session 5) should be done and shared genuinely and simultaneously by the adolescent and the therapist. In every session, the therapist must keep mindful not to question and/or discuss the content of the products of the mind, and instead aim at fundamentally changing the way the adolescent relates with cognitions by questioning the domain of these linguistic products over unhelpful behavior. This ACT-based therapeutic relationship should also be seen as a way for the adolescent to experience that the psychological processes sustaining PF are transdiagnostic and applicable to everyone’s and all life challenges. That was the case with J., who portrayed a deep understanding of the general usefulness of the skills she developed to her diverse life contexts and to her continued change trajectory. Despite being a structure program, it is crucial that the ACT@TeenSAD is delivered (i.e., the strategies, metaphors, and experiential exercises) in a flexible and adjusted way. Specifically, all sessions must be adapted to the language and experience of each adolescent, avoiding the presentation of contents in a mechanized or excessively expository way. The psychotherapeutic intervention ought to be specific in response to the idiosyncratic needs of each adolescent and suitable to any developmental requirements that the adolescent may face at the time—that was the case with J. who focused on performance events during the initial modules of the intervention because they were the most relevant to her at the time. Importantly, to safeguard the therapeutic relationship and respect each adolescent’s timings, the program can and should be adapted (e.g., modifying, simplifying, or complicating exercises).
Bearing these considerations in mind, as well as the preliminary nature of the current findings, the ACT@TeenSAD intervention seems to be an acceptable and feasible intervention for adolescent SAD, with promising outcome results. Given the scarcity of previous works focusing on ACT applied to adolescent SAD (for reviews, see Caletti et al., 2022; García-Pérez & Valdivia-Salas, 2018), the ACT@TeenSAD may be seen as a potential helpful tool for therapist to become familiarized with, in trying to change social anxiety trajectories when they are more frequent and impairing. SAD’s onset is most frequently reported before the age of 18 (Knappe et al., 2015; Stein et al., 2017), and there is a high probability of chronicity associated with severe functional impairments, especially in the absence of treatment (Bruce et al., 2005). Thus, testing the efficacy of therapeutic interventions specifically targeted for adolescents constitutes an important responsibility, with major clinic implications, namely, in mitigating the negative overall impact of SAD and in improving adolescents overall developmental trajectories. Future studies should expand the current work, specifically though follow-up assessments and by using larger samples and more rigorous research design.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been supported by FEDER—European Social Fund—through the COMPETE 2020—Operational Program for Competitiveness and Internationalization (POCI), and by Portuguese funds through the Portuguese Foundation for Science and Technology (FCT) in the framework of the project POCI-01-0145-FEDER-029445.