
Abstract
The use of schema therapy to treat personality disorders in older adults is gaining scientific attention. Personality disorders are prevalent in one out of ten older adults and have a detrimental effect on quality of life. Although 24% or more of nursing home residents may have personality disorders, psychotherapeutic treatment options in the case of comorbid cognitive impairment have not yet been studied. This study concerns a 63-year-old care-dependent male nursing home resident with a personality disorder, a substance use disorder, and several cognitive impairments due to cerebrovascular disease, who presented with complaints of loneliness, low self-esteem, sleeping problems and anger outbursts. Schema therapy was delivered based on the schema mode model for a period of 27 months. Post-treatment assessment demonstrated a decrease in early maladaptive schemas and dysfunctional schema modes and improved personality functioning overall. Although situational psychological distress fluctuated throughout treatment, quality of life improved after 7 months and remained stable onwards. Presented complaints either remitted or strongly diminished. Substance use was also addressed and was in remission for the last 20 months of therapy. This case study suggests that schema therapy is a viable treatment for older adults with personality disorders who present with cognitive impairments in nursing homes.
1 Theoretical and Research Basis for Treatment
Mental health guidelines state that therapies proven to be effective for younger adults with mental disorders should also be applied to older people (APA, 2014). Nonetheless, in clinical practice, older adults are less likely to receive psychological interventions than adults of working age due to therapeutic nihilism and ageism (Bryant, 2017; Chaplin et al., 2015; Clark et al., 2018). This is even more the case when treatment focuses on life-long maladaptive patterns as seen in personality disorders. Protection of older people against ageism in mental health care is difficult due to scarcity of empirical research supporting the feasibility and effectiveness of psychotherapy for older adults. As global aging progresses (WHO, 2018), this research gap becomes only more relevant.
It was once thought that personality disorders disappear with age. Yet, according to DSM-criteria, one in ten people in the community aged 65 years and older has a personality disorder (Reynolds et al., 2015; Schuster et al., 2013). Personality disorders in later life have a continuous negative impact on both mental and physical quality of life (Botter et al., 2021; Frías et al., 2017). Despite increasing attention to the issue, a paucity of empirical evidence still exists on the pathogenesis, diagnostic methods, and treatment possibilities of personality disorders in the aging population (Penders et al., 2020; van Alphen et al., 2015). Nevertheless, the need for specialized treatment of personality disorders in older adults is evident (Segal et al., 2006).
Schema therapy is an effective evidence-based psychotherapy for personality disorders (Jacob & Arntz, 2013; Taylor et al., 2017). In adults, effectiveness of schema therapy has been demonstrated for borderline personality disorder (Farrell et al., 2009), avoidant personality disorder (Bamelis et al., 2014), and mixed personality disorder (Skewes et al., 2015). Treatment guidelines are available for the majority of the personality disorders (Jacob & Arntz, 2013). Originated by Jeffrey Young (1990) to target the pervasive and persistent symptoms of borderline personality disorder, schema therapy integrates elements from cognitive behavioral therapy, gestalt therapy, and attachment theory.
Central to schema therapy’s therapeutic model are early maladaptive schemas: core beliefs about oneself, others, and the outside world that are forged when core emotional needs are not met in a person’s childhood. The activation of a schema leads to a corresponding “schema mode,” another core concept of Young’s model. A schema mode is considered to be a momentary emotional state, often the result of coping with the activated schema. The goal of schema therapy is to meet the individual’s unfulfilled emotional needs through “limited reparenting,” with the therapist serving as a temporary attachment figure. Cognitive behavioral and experiential techniques are used to minimalize schema activation and develop healthy alternative schema modes.
Empirical evidence shows that schema therapy is feasible in later life. Observational studies show that schema therapy leads to symptomatic improvement of older patients with a personality disorder (up to remission of the personality disorder diagnosis) by means of individual therapy (Videler et al., 2018) as well as short-term group therapy (Videler et al., 2014). Furthermore, schema therapy can be applied in a nursing home setting, as it has been delivered in the case of cognitively unimpaired residents of very old age who experienced depression (Lapp et al., 2019). Currently, our research group is conducting the first randomized controlled trial evaluating the (cost-)effectiveness of group schema therapy for older adults with mixed personality disorders (van Dijk et al., 2019). Increasing age is inevitably associated with cognitive decline. Present studies on schema therapy in older populations have all been restricted to cognitively well-functioning patients. Neurocognitive disorders are a heterogeneous collection of types of acquired brain injury but are generally viewed as a contra-indication for psychotherapy as the primary treatment of chronic psychiatric disorders (Groenewald et al., 2019; Sadavoy, 2007).
An alternative established treatment method that has been used for treating personality disorder at a later age is Dialectical Behavior Therapy (Lynch et al., 2007). However, we deemed schema therapy to be especially beneficial in the case of the current patient, Dennis. The main reasons for this were (1) the apt fit of the long-lasting and warm therapeutic relation (employing “limited reparenting”) with the emotional needs specific to the life phase (loneliness, dealing with loss, etc.) and (2) the emphasis on rescripting the trauma-like origins of early maladaptive schemas by means of emotional reprocessing, which can be done fairly passively by the patient, thus circumventing cognitive dysfunctions.
In the Netherlands, an increasing number of people with a combination of psychiatric, somatic, and cognitive disorders other than dementia are admitted to nursing homes. To this end, gerontopsychiatric wards have been developed with professionals trained in both somatic and psychiatric nursing methods. The prevalence of personality disorders ranges between 24.1% (Collet et al., 2018, sample includes dementia) and 43.7% (van den Brink et al., 2017, sample excludes dementia). Psychotherapeutic treatment options for older adults with personality disorders and cognitive disorders other than dementia are thus of clinical use. The goal of this case study is to explore the feasibility of individual schema therapy for an older adult with a mixed personality disorder and cognitive impairment in the gerontopsychiatric nursing home setting.
2 Case Introduction
“Dennis” was a 63-year-old man admitted to a nursing home for a left-sided hemiplegia and a corresponding unilateral neglect due to an ischemic cerebrovascular accident and subarachnoid hemorrhage in 2013. Due to these physical constraints, Dennis was care dependent for most activities of daily living (ADL). Neuropsychological testing revealed mild impairments in his attention, memory function (storage of new information), and executive functions.
Dennis had received mental health care since his adolescence for substance use disorder (alcohol, cocaine, cannabis, and opioids) and a mixed personality disorder with dependent and borderline traits. He was assigned female at birth, but experienced gender dysphoria. He started a gender transition process around his thirties, which was completed at the age of 40. His childless marriage with his wife was tumultuous and eventually resulted in a divorce. Dennis worked various jobs as a health care professional in a sheltered home and as a road worker.
3 Presenting complaints
After Dennis was admitted to the nursing home, he no longer had access to illegal drugs. This directly resulted in a remission of his cocaine and opioid use disorder. In addition, his use of alcohol and cannabis decreased significantly. Dennis agreed to limit his cannabis and alcohol use to once a week. Restricting his substance use caused Dennis to rely less on his usual coping style of self-soothing, leading him to be progressively confronted with his inner feelings. He presented with feelings of loneliness and failure, and anger management problems. At night, Dennis ruminated about the loss of his social network and about being admitted to the nursing home. Subsequently, his ruminations caused sleeping problems. Furthermore, he often felt unjustly treated and criticized by his care providers. Arguments rapidly escalated into verbal and physical aggression, after which Dennis often expressed regret.
Simultaneously, Dennis’ care providers struggled with his behavior. From their perspective, Dennis was overly demanding about daily matters such as ADL-assistance or food quality, and this easily resulted in outbursts of aggression. His outbursts had a significant impact on fellow residents and care providers. At times, Dennis would become enraged, lie down on the floor and refuse to get up. To get him to calm down, care providers had to remove Dennis, kicking and punching, from communal areas.
4 History
During his childhood, Dennis lived with his father, mother, older brother (+8), and younger sister (−7) in an urban working-class community. The atmosphere at home was constantly tense due to his parents’ marital problems. His father was a market vendor, whom Dennis portrayed as a dominant man who demanded unreasonable order and tidiness from his wife and children. If his standards were not met, he became enraged and verbally abusive, which was frequently the case. Dennis reported that he and his older brother were outgoing and impulsive thrill-seeking children, and that he was often punished without understanding what he had done wrong. His father had once been admitted to a mental health care facility, but specific information about this was never disclosed to the children. His mother was a homemaker who cared for the family’s practical needs. Although Dennis did describe her as a loving mother, he also gave multiple examples of her psychological abuse and emotional neglect of him and his siblings.
Dennis noted that in general learning was difficult; moreover, he often got into trouble at school. Dennis depicted himself as an inattentive and undisciplined schoolgirl at elementary school. He stated that he had attention deficit disorder (ADD), but it remains unclear whether it was ever officially diagnosed. For the most part, his parents reacted dismissively and punitively to his learning difficulties. Due to Dennis’ oppositional behavior and his father’s punitive parenting style, he was eventually appointed a legal guardian, placed in a group home, and referred to a school for special needs education. He finally graduated from a vocational education program and became a health care professional trained to support sheltered-home residents.
During puberty, Dennis’ substance use disorder manifested, culminating in heavy opioid use at age 17. During his adult life, Dennis’ substance use resulted in his inability to hold down a job, financial problems, petty theft, imprisonment, and a tumultuous long-term relationship with a woman who only saw him during periods when he abstained from use. His older brother had comparable learning problems and an opioid use disorder. He died when both brothers were in their 30s. Dennis had been offered several treatment strategies for substance abuse, including individual psychotherapy, group treatment, day treatment, as well as multiple stays at a rehabilitation clinic. Nonetheless, he never achieved a stable, enduring remission.
Although it had been established that Dennis had a personality disorder, he never received any treatment for it. Until she died of cancer, Dennis’ex-wife provided him with emotional support in the years before he was admitted to the nursing home.
5 Assessment
Diagnostics
In this study, psychiatric morbidity was classified according to DSM-criteria applying the LEAD method, which stands for Longitudinal Expert and All Data. This resulted in the confirmation of a personality disorder not otherwise specified with borderline and dependent features, as well as the presence of a substance use disorder (currently for alcohol and cannabis, with sustained remission for cocaine and opioids). It was decided not to repeat the extended neuropsychological testing, as substance and medicine use would hinder accurate interpretation. Instead, a rough estimate of cognitive functioning was obtained by administering the Montreal Cognitive Assessment (MoCA) and the Frontal Assessment Battery (FAB) (Dubois et al., 2000; Nasreddine, 2005).
On the MoCA, Dennis scored 21 out of 30, which is below the 25-point cut-off indicating cognitive decline. Dennis registered low scores on tasks reflecting attentional and visual/executive functions, while successfully completing the memory and orientation tasks. His score of 11 out of 18 on the FAB also points towards clinically relevant frontal dysfunctions (van den Brink et al., 2013; van Loo et al., 2007).
Pretreatment Assessment
A pretreatment assessment was carried out to (1) diagnose early maladaptive schemas and schema modes and determine their origin as part of a case conceptualization that is suitable for schema therapy and (2) establish a baseline measurement for the three outcome parameters quality of life, psychopathological distress, and personality functioning.
Treatment Monitoring
Both pretreatment assessment instruments were re-administered postintervention at 27 months, and the YSQ-L2 (see below) also at 6 months. In addition to the baseline assessment, we measured quality of life and psychopathological distress nine times during treatment, whereas personality functioning was only re-evaluated posttreatment at 27 months.
Pretreatment and Monitoring Instruments
Early maladaptive schemas were assessed with the Young Schema Questionnaire (YSQ) (Young & Brown, 1994). The YSQ-L2 (long form, second version) is a self-report questionnaire consisting of 205 items measuring a total of 16 different schemas. The translated and modified Dutch version of the YSQ-L2 has been studied thoroughly and has shown favorable psychometric properties (Rijkeboer et al., 2005; Rijkeboer & van den Bergh, 2006). A higher score indicates a more severe level for that particular maladaptive early schema. Schema modes were assessed with the short Schema Mode Inventory (SMI), as validated in Dutch by Lobbestael et al., 2010. This short version contains 118 items from the original SMI (Young et al., 2007), and psychometric properties are sufficient for clinical use. Although schema modes are considered momentary states that can be present at certain times and absent at others, the short SMI has a good test-retest reliability (Lobbestael et al., 2010). Scores are computed for 14 different schema modes, with a higher score indicating more frequent activation of the schema mode. Quality of life was evaluated with the Recovering Quality of Life (ReQoL) questionnaire. The ReQoL assesses themes pertaining to concepts of both recovery and quality life relevant for patients with mental health difficulties—namely, activity (meaningful and/or structured), hope, belonging and relationships, self-perception, well-being, and autonomy. The ReQoL was specifically developed for and with the aid of psychiatric patients, appears to be unidimensional in structure, and is validated across a variety of mental health disorders and age-ranges, up to 80 years (Keetharuth et al., 2018). Psychological distress was measured with the Brief Symptom Inventory (BSI-53) (Derogatis, 1975), an abbreviated version of the 90-item Symptom Checklist (SCL-90). The total sum score is considered as an overall level of psychological distress. Personality functioning was measured with the Severity Indices of Personality Problems Short Form (SIPP-SF) (Verheul et al., 2008). The SIPP-SF measures five domains of personality functioning: Identity Integration, Self-Control, Relational Functioning, Social Concordance, and Responsibility, corresponding with the DSM-5 alternative model of personality disorders.
Based on the norm-values of the ReQoL, Dennis’ score was at the border of a clinically relevant impairment in recovery-related quality of life. The sum scores of the BSI-53 confirmed a high level of distress at baseline, classified as above average compared to an age- and sex-matched norm population. The scores of the SIPP-SF were extremely low for self-control, responsibility, and relational capacities, low for social concordance, and average for identity integration.
6 Case Conceptualization
Considering the personality disorder diagnosis and Dennis’ current symptoms, behavior, and biographical information, schema therapy was deemed an appropriate therapy. According to the schema therapy model, the case conceptualization was based on the initial scores on the YSQ-L2 and SMI. Both instruments are commonly used as a starting point for case conceptualization (Young et al., 2003): the YSQ-L2 for a comprehensive conceptualization connecting current problems with their potential origin and the SMI for an explanatory model of the mood swings and most common emotional states of the patient. Although both conceptualizations can be discussed with the patient, particularly the latter was used in the sessions.
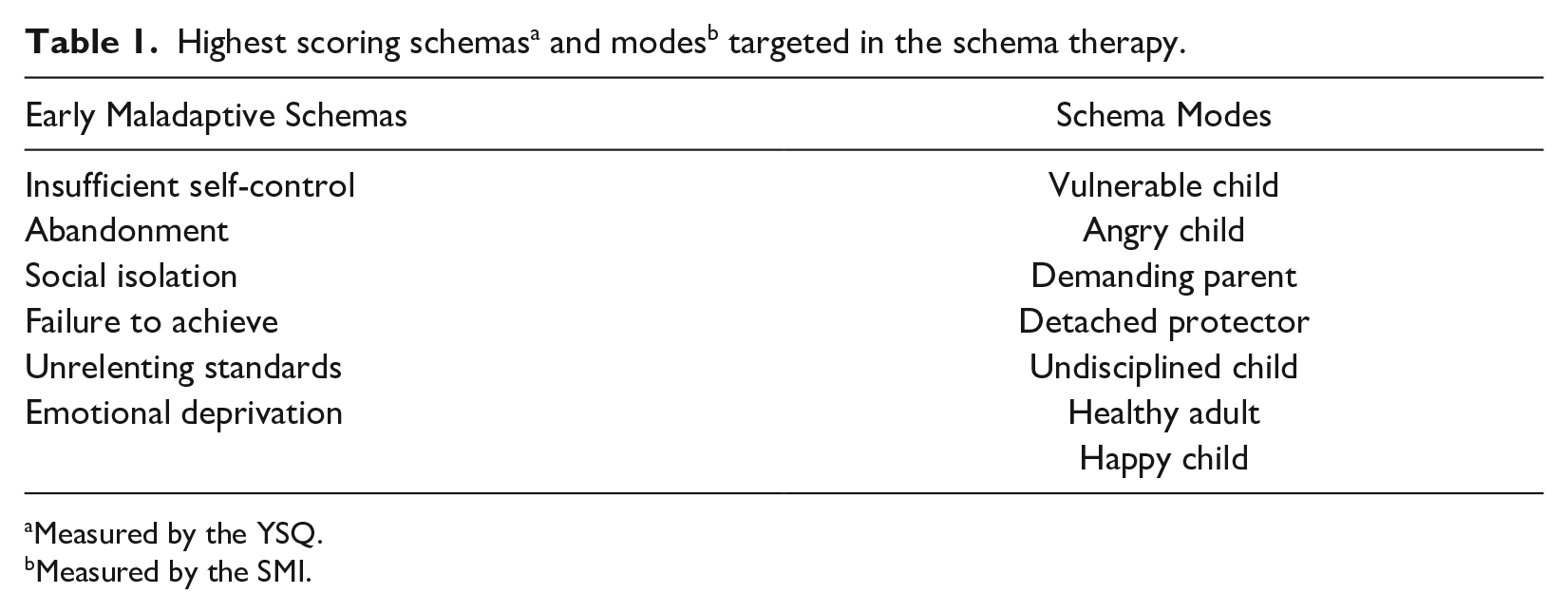
The YSQ-L2 schema scores cannot be classified, as norm groups are not available. The six schemas with the highest scores were used in a subsequent diagnostic interview to verify whether these scores indeed indicated the existence of early maladaptive schemas, which has been linked to personality disorders (Carr & Francis, 2010). Dennis had the highest scores on the following schemas (in order of decreasing severity): insufficient self-control, abandonment, social isolation, failure to achieve, unrelenting standards, and finally, emotional deprivation (see Table 1). Of these six schemas, the first four appeared to be connected to his biography and were consequently used in the case conceptualization. Figure 1 presents the visualization of this case conceptualization connecting Dennis’ early maladaptive schemas with their origins, the three general coping mechanisms (surrendering, avoiding, and overcompensating), and current problems.
Measured by the YSQ.
Measured by the SMI.
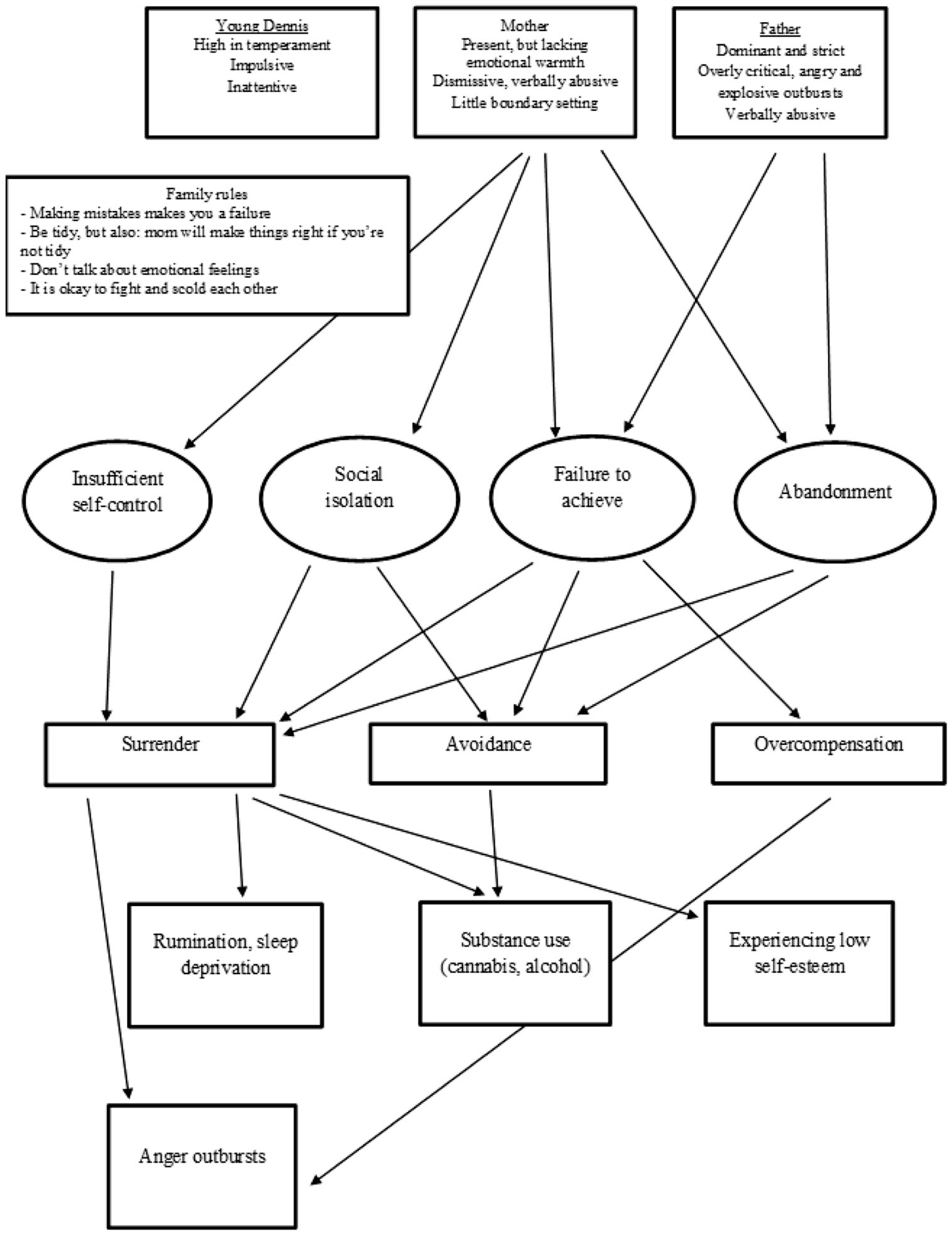
Case conceptualization of the top-4 early maladaptive schemas, their origin, and how the present coping styles led to the presented complaints.
Considering the description of his traits as a child, it is likely that Dennis was genetically vulnerable to develop impulsiveness and high temperament as main personality traits. His childhood environment was evidently unsafe, abusive, lacking in warmth and love, and moreover, devoid of healthy boundaries for his impulsive behavior. Dennis could easily provide examples of childhood experiences related to his most prominent schemas. The schema “failure to achieve,” for example, led him to remember as a child showing his mother his subpar primary school grades. Subsequently, she became very angry with him, calling him a failure and telling him he could do nothing right.
As represented in Figure 1, the therapist hypothesized that Dennis’ low self-esteem manifests when his schemas “failure to achieve,” “abandonment,” and “social isolation” are triggered and he subsequently surrenders to their emotional and cognitive content. On some occasions, his response was to overcompensate these schemas, resulting in outbursts of aggression. An alternative trigger of his aggressive behavior stems from surrendering to his impatience when the schema “insufficient self-control” is activated. According to Dennis, this schema originates from both his father’s lack of self-restraint displayed in his aggressive behavior and his mother’s failure to hold Dennis accountable when he did not do his chores around the house.
The therapist hypothesized that Dennis’ night time ruminations appear when he is confronted with his schema “abandonment.” Dennis felt abandoned on several occasions in his childhood when his parents distanced themselves from him as his problems with school and addiction arose and, ultimately, when Dennis was placed in a group home. It was also postulated that Dennis’ tendency to use psychoactive substances reflects an avoidant coping style when the schemas “social isolation,” “abandonment,” and “failure to achieve” are activated. Furthermore, Dennis’ substance use was also hypothesized to rise from Dennis succumbing to his schema “insufficient self-control.”
Although his gender transition took place in a time period characterized by less social acceptance of gender issues, Dennis felt supported by his family and his peers. In his current life, he has not experienced social exclusion or discrimination. Dennis was satisfied with his current gender and bodily characteristics. Therefore, it was concluded that no relation existed between his gender identity issues and the complaints with which he presented, or his underlying early schemas.
Regarding the SMI, Dennis scored highest on the following modes (in order of decreasing severity): undisciplined child, vulnerable child, healthy adult, detached protector, happy child, angry child, and demanding parent (see Table 1). Figure 2 graphically presents this model, personalized for Dennis by including his most important coping strategies and emotions. As is customary in schema therapy, some of the mode names were personalized to make them more tangible for the patient. The mode model is a supposition of how the activation of Dennis’ schemas leads to a dynamic interchange of momentary emotional states that are reflected in the schema modes.
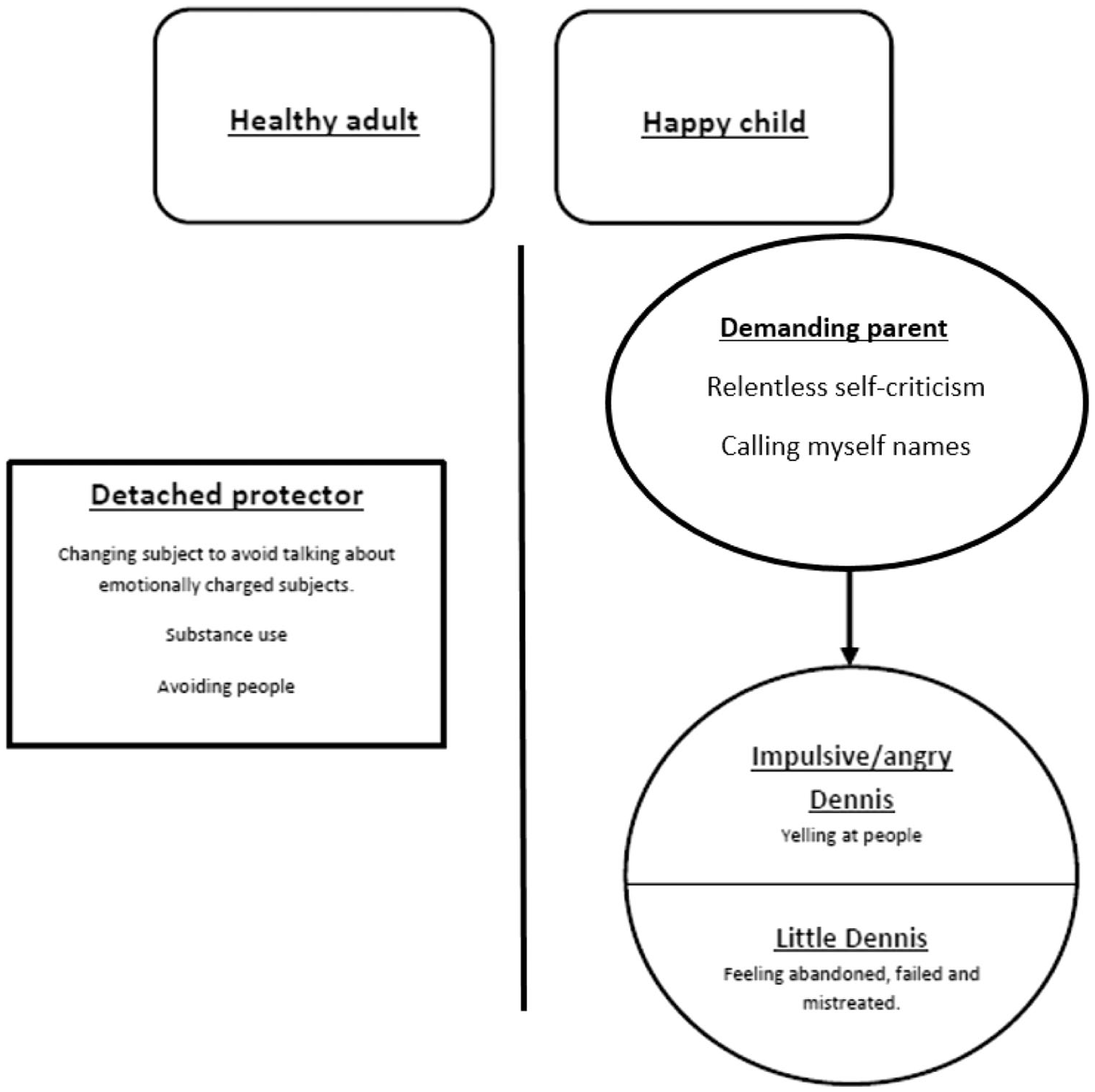
Case conceptualization based on the schema modes, as used in therapy.
A common sequence for Dennis starts with the activation of his demanding parent mode as a result of surrendering to a certain schema. For instance, when Dennis was unable to perform self-care due to his left-sided hemiplegia, his schema “failure to achieve” tended to get provoked. His “demanding parent mode” manifests itself through harsh self-criticism, as if it were criticizing “little Dennis” or his “vulnerable child mode.” As a consequence, the mode “little Dennis” is triggered, making Dennis feel very vulnerable and like a failed person in general. These feelings eventually became too taxing, leading Dennis to exercise a more avoidant coping strategy, thus activating his “detached self-protector” mode, which leads him to use alcohol or cannabis. This mode can be considered an important survival strategy, as it helped Dennis to endure the harmful circumstances of his childhood.
His “impulsive or angry child mode” usually became activated when Dennis felt mistreated by the care team, resulting in his aggressive outbursts and subsequently triggering the above-described sequence from the “demanding parent” to “little Dennis” and the “detached self-protector.” The “healthy adult” and “happy child” modes represent adequate, healthy modes that Dennis is assumed to underutilize in dealing with his schemas. This particular schema mode model fully fits with the schema modes model used for borderline personality pathology (van Vreeswijk et al., 2008). Previously diagnosed dependent personality traits were not observed and are thus not a part of the case conceptualization.
7 Course of Treatment and Assessment of Progress
As no studies have been performed on the feasibility of schema therapy in the case of cognitive impairments, three adjustments were made to best fit Dennis’ cognitive limitations. First, the schema mode model was used in treatment and presented to Dennis, as it is more parsimonious than the conceptualization of the early maladaptive schemas of Figure 1. Second, experiential techniques were emphasized over cognitive techniques, in order to focus the therapy more on emotional reprocessing. This is in line with advice from previous research on schema therapy for older adults (Videler et al., 2018). Moreover, recent insights indicate that a stronger focus on schema mode interventions instead of interventions directly targeting early maladaptive schemas may be most effective (Yakın et al., 2020). Third, to compensate for possible verbal memory problems, a visual representation of the schema mode model was present at every session and positioned within Dennis’ intact attentional visual field.
As is customary in schema therapy, the first part of therapy was devoted to presenting and discussing the schema mode model (see Figure 2). The goal is to reach agreement about the model with the patient. Dennis received psycho education about the schema modes in the first two sessions, after which he recognized all of the schema modes as his typical behavioral responses in daily life. To personalize and familiarize patients with their schema mode conceptualization, all modes were given a name. For example, in our case, the name “little Dennis” was assigned to the vulnerable child mode.
In total, Dennis received 76 individual schema therapy sessions, each lasting 45 minutes. Therapy took place over a period of 27 months. This length is not uncommon, as treatment duration can vary greatly in schema therapy (Taylor et al., 2017). For the first ten weeks, the sessions were held twice weekly to gain momentum. Subsequently, the sessions were held on a weekly basis. The last four sessions were held monthly. The therapist, a non-registered schema therapist with five years of schema therapy experience, is the first author of the present case study. Supervision was provided by a registered schema therapy supervisor who had no role in this study. Therapy sessions were given in a neutral room at the nursing home in which Dennis resided. Dennis displayed a compliant and motivated attitude. In the first months of therapy, Dennis tended to forget his appointment due to memory problems. Therefore, care providers cued him before his sessions until he was able to successfully remind himself. Therapy ended after 76 sessions, when the therapist and patient jointly decided that the treatment goals had been met.
Experiential Techniques
Two frequently used schema therapy techniques are imagery rescripting and chair work dialogues. During imagery rescripting, the patient explores a schema-triggering event and connects it to a childhood experience that was supposedly formative in the development of the early maladaptive schema. By means of imagination, the patient relives the childhood experience. The experience, however, is rescripted by the therapist, who enters the imagery, protects the child, and meets his or her emotional needs. Chair work dialogues are exercises in which the different schema modes, or sides of the patient, are disentangled by assigning them to corresponding chairs. The patient thus learns to differentiate the schema modes, so as to recognize them in daily life and cope with them accordingly. The aims of chair work dialogues are to stop and send away the overly self-criticizing parent mode, to persuade the detached self-protector mode to stop avoiding inner feelings, and to validate and support the vulnerable child mode. In the beginning, the dialogues are directed by the therapist, but eventually they are assumed by the emboldened healthy adult mode of the patient.
Imagery rescripting was used to give Dennis insight into the association between events in his present life that lead to schema activation and underlying childhood experiences. In the first sessions, Dennis had trouble closing his eyes, as doing so triggered an undetermined feeling of fear labelled as the protector mode. Therefore, chair work dialogues were used to let him get acquainted with his detached protector mode. It was only after thorough validation of and negotiation with this schema mode that Dennis surrendered himself to the imagery rescripting exercises. He imagined various traumatizing childhood memories as he connected to his vulnerable child mode. This enabled the therapist to rescript those episodes and thus provide limited reparenting. An additional effect of the imagery rescripting was that Dennis reappraised the course of his childhood. Prior to therapy, Dennis placed all of the blame for his childhood mishaps—the bad school performances, the fights with his parents, and the substance use—on himself. Halfway through therapy, Dennis started to acknowledge that the bad parenting he had received played a major role in those situations.
Chair work dialogues were repeatedly utilized with the aims of stopping and ousting Dennis’ demanding parent mode, diminishing the role of his detached protector mode, setting boundaries for his enraged child mode, and validating and supporting his vulnerable child mode, after which he gradually became able to take responsibility for his current behavior. By constantly identifying and addressing his detached protector mode, Dennis learned that his cannabis and alcohol use had an avoidant function. Prefacing therapy, Dennis had rejected the idea of quitting substance use. Problematizing his avoidant coping styles motivated Dennis to successfully quit using cannabis and alcohol, and to stop smoking. When his parent and protector modes were more absent, Dennis was increasingly able to share his emotions and vulnerability, and he showed more leniency and understanding towards himself. This also enabled him to process suppressed grief over the loss of his brother and ex-wife. In the second half of the therapy, chair work dialogues focused on the healthy adult mode by letting Dennis practice employing this mode as much as possible in therapy sessions to deal with his own dysfunctional schema modes.
Limit Setting
Limit setting is technique used in schema therapy to empathically confront patients with dysfunctional and boundary crossing behavior. At six months (22 sessions), Dennis experienced a relapse and used cocaine when a fellow resident offered the drug to him. Dennis did not report the relapse in therapy. The therapist confronted Dennis about his secretive attitude and connected this with his pattern of behavior during his addiction in the past. After a second relapse, which Dennis frankly disclosed, the therapist proposed limit-setting agreements. Substance use became the sole topic during sessions, with the goal of helping Dennis quit, until progress was made. Dennis agreed and did not use cocaine or any other substance again for the remaining 20 months of therapy.
Psychotropic Drug Use
In the first month of therapy, it became apparent that Dennis was also using a second-generation antipsychotic drug (olanzapine) to suppress his emotions. Olanzapine was prescribed prior to his nursing home admission to facilitate substance withdrawal but evaluation had never taken place. Dennis had displayed neither psychotic symptoms nor cognitive-perceptual symptoms related to his personality problems, and he was clearly sedated by the drug. Therefore, the use of olanzapine was considered inappropriate. After two months (session 11), Dennis agreed to discontinue the olanzapine. As a result, his mental clarity improved and he experienced more emotional arousal, including both positive and negative emotions.
Coping with Somatic Health Events
During the first year of schema therapy, Dennis struggled repeatedly with painful urinary retention and needed bladder catheterization. A surgical procedure was unavoidable to solve his physical discomfort. Although waiting for surgery, numerous negative interactions occurred between Dennis and his caretaking team. Dennis required frequent assistance to empty his catheter bags, and his impatience led to outbursts of aggression when a care provider was not immediately available. In therapy, we focused on the angry child mode so Dennis could practice with self-restriction. Although Dennis was motivated to restrict himself and demonstrate adequate assertive behavior, the caretaking team found it increasingly difficult to remain patient and empathetic towards him. As a result, his “failure to achieve” schema was continuously triggered.
The team was educated about Dennis’ early maladaptive schemas and how these schemas could be triggered by the care providers’ attitudes and responses to him. After this, the team expressed more understanding of Dennis behavior. Upon noticing the change in the team’s attitude, Dennis’ aggressive outbursts stopped, and he made it his priority to thank all the care providers for their efforts.
Clinical Outcomes
A favorable outcome of schema therapy is assumed to be mediated by decreased impact of early maladaptive schemas and (inappropriate) schema modes on current functioning. Figure 3 presents the severity of Dennis’ six most prominent schemas. After six months of schema therapy, five of the six designated schemas remarkably showed higher YSQ-scores upon visual inspection. Two explanations are likely for this. First, during the initial phase of schema therapy awareness and recognition of early maladaptive schemas increase and can feel unpleasant, as adequate coping styles are lacking. Second, discontinuation of the olanzapine could have increased Dennis’ emotional awareness, as reported by Dennis himself and reflected in the scores. Atypical antipsychotic medication such as olanzapine does indeed have mood-suppressing effects (Yatham, 2002). At 27 months, YSQ-scores for all targeted schemas were improved compared to the scores at six months. The scores of the schemas “insufficient self-control” and “abandonment” also showed a clear improvement compared to the baseline scores. Post-treatment improvement of “emotional deprivation” and “unrelenting standards” were minor compared to baseline, while “social isolation” and “failure to achieve” remained more or less stable.
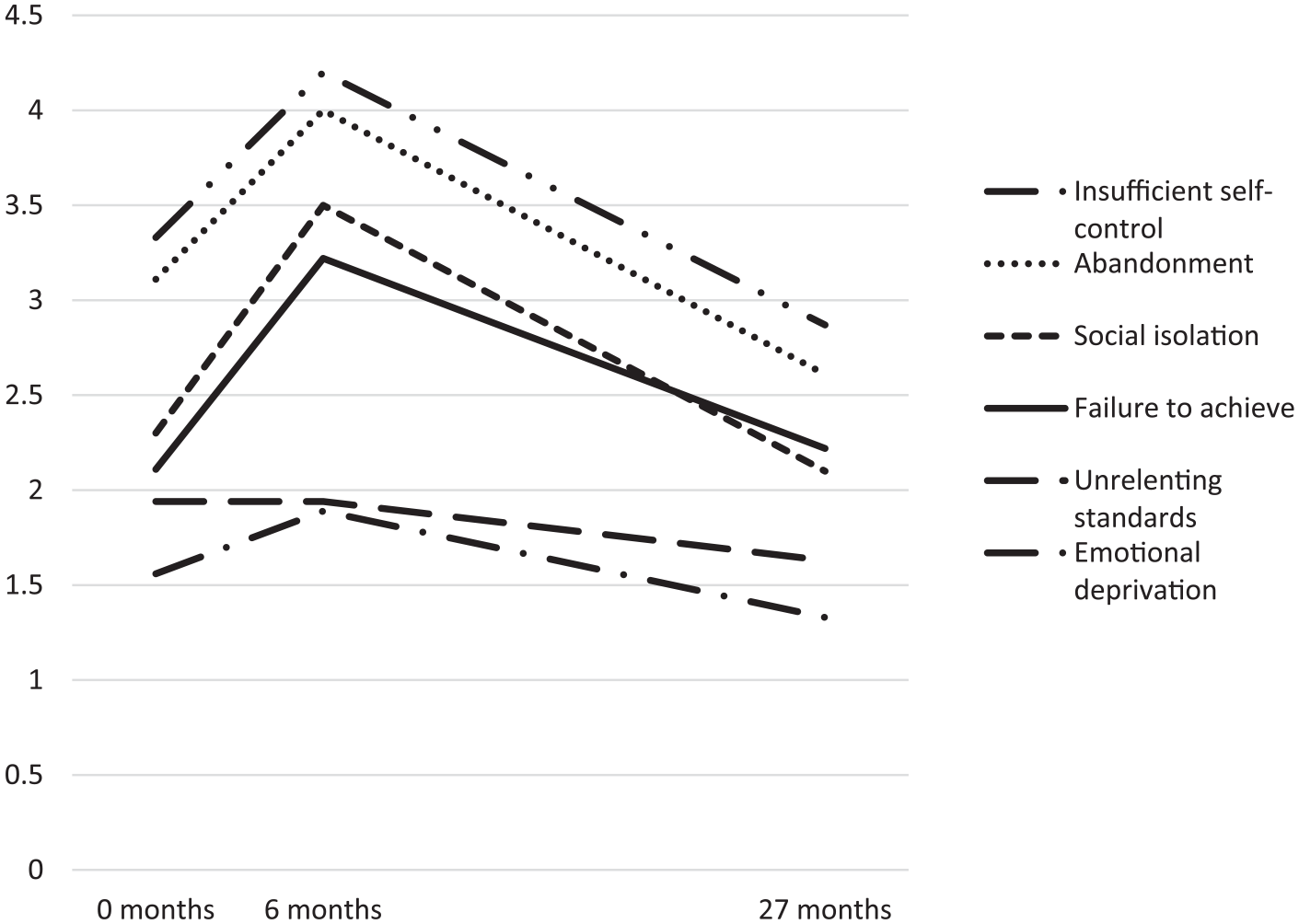
Early maladaptive schemas scores measured by the YSQ at 0 months, 6 months, and 27 months.
Schema mode (SMI) scores improved from pre-through post-treatment (see Figure 4), as multiple dysfunctional mode scores (undisciplined child, angry child, vulnerable child, detached protector, and demanding parent) were diminished. Furthermore, the functional and favored mode scores were either stable (healthy adult) or higher (happy child) posttreatment. These improvements are important as high vulnerable child mode scores are related to high psychopathology in older adults (Phillips et al., 2020). A limitation is the lack of SMI scores at 6 months, as a course resembling the YSQ-scores might have been visible.

Schema mode scores measured by the SMI pre- and posttreatment.
Early maladaptive schemas and schema modes are directly targeted in therapy and changes in these domains are considered as a mediator for clinically relevant changes in quality of life, psychological distress, and last but not least, personality functioning.
Recovery-related quality of life improved after seven months of therapy and this improvement sustained throughout the rest of therapy. In our opinion, this is the most important outcome measure. Traditionally, mental health measures have tended to be based on the patient’s symptoms rather than on recovery of his or her quality of life. There are increasing calls to reformulate the concept of “health” as the ability to adapt and self-manage in the face of social, physical and emotional challenges (Huber et al., 2011). For patients, the essence of recovery is not the absence of the illness, but the ability to “rise above the diagnostic label” (Boevink, 2012), as measured with the ReQoL.
The clinical relevance of studying recovery-related quality of life is actually demonstrated by the fluctuating course of psychological distress during therapy. Although Dennis’ distress increased after 7 months of therapy, it decreased profoundly after 10 months. Subsequently, coinciding with the exacerbation of somatic problems and corresponding negative interactions with the care team, Dennis’ level of psychological distress was high between 12 and 16 months, after which it again decreased until the posttreatment assessment. That recovery-related quality of life remained stable despite fluctuating situational psychological distress could be indicative of a robust therapeutic effect (see Figure 5).
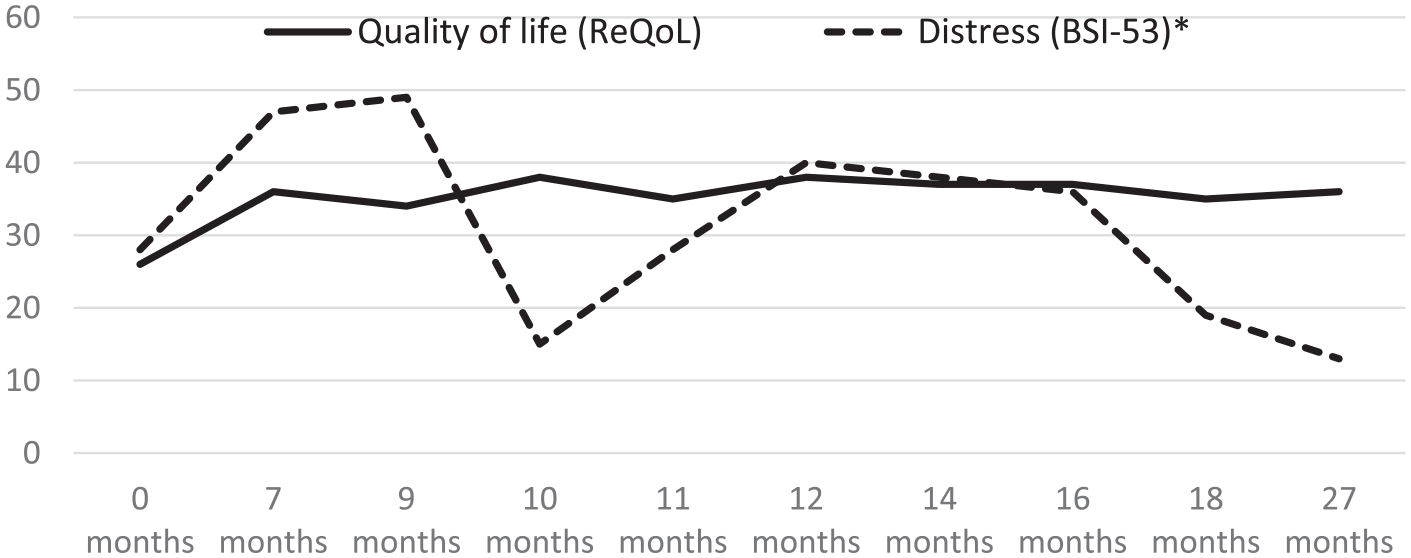
Scores on measures of quality of life (measured by the ReQoL) and psychological distress (measured by the BSI-53). *Total scores multiplied by 10.
Finally, improvement of personality functioning was reflected in several SIPP-SF domain scores (see Table 2). Improvement was visible for the domains “responsibility” and “relational capacities,” as the scores increased from extremely low at pretreatment to an average level posttreatment. A slight increase in the scores for “identity integration,” “self-control,” and “social concordance” was found posttreatment, while remaining in the same norm group classifications.
Personality functioning measured by the Severity Indices of Personality Problems Short Form (SIPP-SF).
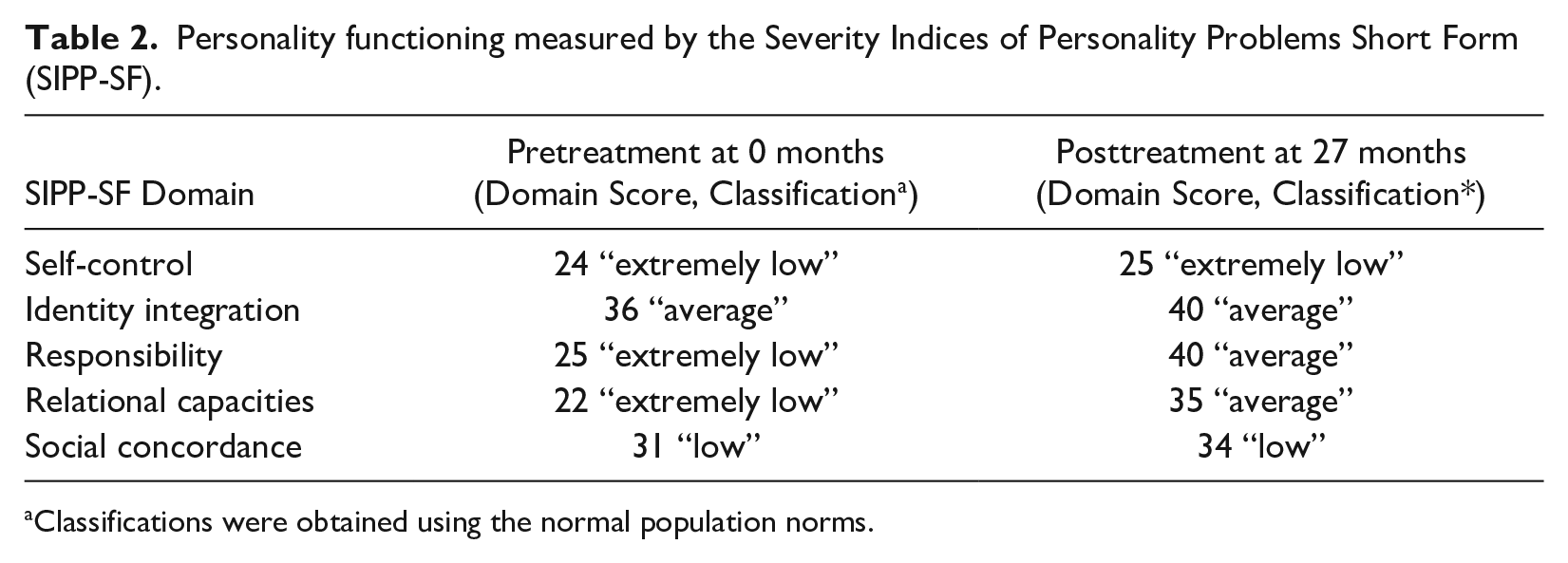
Classifications were obtained using the normal population norms.
Overall, while not psychometrically substantiated, Dennis expressed his satisfaction with the results of his therapy. He said that some of his presenting complaints were completely absent at the conclusion of therapy. For example, he no longer experienced sleeping problems or low self-esteem. Furthermore, he indicated that other complaints were profoundly diminished. Despite fluctuating feelings of anger, he was able to prevent physically aggressive outbursts. He still experienced some degree of loneliness but not feelings of total abandonment. He was able to feel and tell himself that several people in his life had cared and/or still do care about him.
8 Complicating Factors
Schema therapists usually give the patient exercises or assignments to do outside of the therapeutic sessions. However, due to his left-sided hemiplegia resulting from cerebrovascular accidents, Dennis could not write or fill out any forms. This element of therapy was therefore not offered.
After Dennis had completed 1 year of schema therapy, the COVID-19 pandemic reached the Netherlands. In the first COVID wave, Dennis’ nursing home ward was locked down for most professionals other than primary care providers. As a result, Dennis received eight online video sessions, of which one had to be cancelled due to technical difficulties. Although video conference calls had their difficulties, such as finding out how to employ chair work dialogue exercises via video call, Dennis nevertheless appreciated the contact as he struggled to cope with the pandemic. Offering help and support at that time fit the goal of limited reparenting. Although no empirical studies on the efficacy of online schema therapy have been publicized, the first guidelines for online chair work have been presented (Pugh & Bell, 2020).
9 Access and Barriers to Care
In the Netherlands, nursing home facilities are available for all residents who are unable to live independently due to physical and/or cognitive restraints. Nursing homes are well equipped with health care professionals, including elderly care physicians specifically trained for this setting, psychologists, and paramedics (Koopmans et al., 2017). Staff always include psychologists trained in neuropsychological testing as well as psychological treatment. Psychological treatment can be given individually, as well as through the care team (mediative therapy). Traditionally, Dutch nursing home psychologists use mediative therapy more frequently than they do individual psychotherapy. In mediative therapy, the goal is to reduce challenging behavior such as aggression, apathy, or extremely dependent behavior. The psychologist provides the care team with guidelines for their own behavior to elicit positive behavior from the residents, often using principles of operant conditioning (Leontjevas et al., 2013).
A barrier for providing individual schema therapy in the nursing home may be the lack of psychologists trained in psychotherapy in general and schema therapy in particular. Moreover, time restraints often prevent psychologists from giving individual psychotherapy alongside mediative therapy. Furthermore, although specialized psychotherapy for personality disorders can be cost-effective (Wetzelaer et al., 2017), reimbursement policies from health service and insurance companies often favor short-term and complaint-focused therapy (Lazar, 2014). This could pose a barrier for delivering schema therapy, depending on the country in which the patient lives.
10 Follow-up
No follow-up measurements were conducted post-treatment, as Dennis remained clinically stable. Dennis did, however, request a session with the therapist six months after the end of treatment. In this session, Dennis verbally confirmed that his level of complaint and functioning was comparable to the last in-treatment measurement. Nevertheless, he wanted to discuss how to get along with new, inexperienced members of the care team who, in his view, did not take him seriously. Dennis stressed that his aggressive outbursts were still in remission but not feeling taken seriously by new members of the care team really bothered him. Eventually, Dennis concluded that his aim for the extra session was to vent his frustrations. Afterwards, he expressed satisfaction. In the six months that followed, Dennis did not request any further sessions.
11 Treatment Implications of the case
This case study is a first step in gathering empirical evidence to support psychotherapeutic treatment of personality disorders in cognitively impaired older adults—an interesting prospect, as demand for therapeutic options in this demographic might rise in conjunction with increased life expectancy and its accompanying prevalence of (mild) cognitive impairment and frailty (de Roeck et al., 2020). Dennis’ overall satisfaction with the therapy suggests that schema therapy in this population is at least feasible. His improvement in traditionally considered “trait” characteristics (early maladaptive schemas and personality functioning) suggests that personality change is still possible in old age and in cases of cognitive decline. Furthermore, schema therapy offered room for age-specific therapy themes such as grief processing or dealing with the fear of death.
A comorbid substance use disorder did not prove to be an obstacle for therapeutic change in this case, which is advantageous considering the significant overlap between personality disorders and substance use. On the contrary, the schema therapy was probably instrumental in Dennis’ recovery from substance abuse and also enabled him to stop using mood regulating psychiatric medication. Schema therapy has in fact been proposed as a suitable option for dual treatment of personality and substance use disorders, and there is tentative empirical support for its effectiveness (Boog et al., 2019; Kersten, 2012).
Furthermore, the schema model appeared to be useful for team education, giving insight into how behavioral problems can be caused by personality disorders. A subsequent step for future research could be enhancing mediative therapy by incorporating schema model-based interventions.
12 Recommendations to Clinicians and Students
When using schema therapy to treat cognitively impaired older adults, we recommend that the therapist places strong emphasis on using experiential techniques. First, targeting feelings rather than cognitions decreases reliance on cognitive learning mechanisms that might be impaired in a patient. Second, experiential techniques may be better equipped to circumvent the long-standing avoidance mechanisms that older adults possess. The uncomplicated yet insightful standard schema mode model can be used as the main working model for therapist and patient during sessions. However, we want to emphasize that to ensure that core elements of the therapy were administered, we did not make profound adjustments to schema therapy. Our experience was that the therapeutic processes we encountered with Dennis were more similar than dissimilar to schema therapy in cognitively intact younger adults. Further research should examine whether additional adaptation is needed to improve employment and effectiveness of schema therapy for cognitively impaired older adults.
Schema therapy is a demanding form of psychotherapy, and patients will be emotionally disrupted in the early phases of a long-term therapeutic process. The therapeutic process requires a basic level of self-reflection, motivation to stay committed to self-change, and a certain level of cognitive ability. Therefore, cognitive decline is generally considered a hard contraindication for schema therapy. This generalizing approach, however, does not hold true, as patients with cognitive impairment may have an intact self-identity and may be able to distinguish between the present and the past, which is sufficient to receive schema therapy.
We suggest that psychological treatment should never be withheld from people solely on the basis of age, setting, or the presence of a cognitive disorder (Woods, 2003). Individual assessment should take place to obtain a person-centered, tailored treatment advice. Prior to his admission to the nursing home, Dennis’ life was hardly ever stable, structured, or safe. Despite initially triggering schema-activation, Dennis’ care team members were able to change their attitudes towards Dennis and thus provide a safe learning environment. The holding of a nursing home setting can thus provide a good context for schema therapy. Storm damage is best repaired when the ship is in calm waters, so to speak.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding is entirely provided by University Medical Center Groningen and Atlant Nursing Home Care. No grants were requested for this study.