
Abstract
Postpartum depression is a highly prevalent mental health problem with harmful consequences for women, babies, and mother–infant relationships. Cognitive–behavioral therapy (CBT) is among the most effective treatment options for postpartum depression. However, a large number of postpartum women do not seek professional help, suggesting the need for new treatment delivery formats. The present article describes the application of Be a Mom Coping with Depression, a blended CBT treatment for postpartum depression, for a 31-year-old postpartum woman. The intervention was provided over a period of 13 weeks, integrating seven biweekly sessions with a psychologist and six sessions within an online program, and it is described in detail. A summary of the patient’s progress and the results obtained throughout treatment is reported. At the end of the intervention, a significant decrease in depressive and anxiety symptoms was observed, as well as increased perceived maternal self-efficacy, higher psychological flexibility, and higher self-compassion. This case study provides encouraging data for the preliminary evidence of the acceptability, feasibility, and efficacy of the Be a Mom Coping with Depression intervention in the reduction of depressive symptoms during the postpartum period. Advantages of this treatment format and implications for clinical practice and future research are discussed.
Keywords
1 Theoretical and Research Basis for Treatment
The transition to motherhood is a demanding period in which women face challenges related to their identity, their interpersonal relationships, and emotional and physical changes (Finlayson et al., 2020), and for these reasons, it may represent a time of increased risk for women to develop mental health problems (Woolhouse et al., 2014). Postpartum depression (PPD) is among the most prevalent mental health conditions after childbirth, with an estimated prevalence of 20% (Gelaye et al., 2016; Yan et al., 2020). PPD is defined as an episode of depression occurring up to 12 months after birth (American Psychiatric Association, 2013; O'Hara & McCabe, 2013) and it poses negative consequences for the woman, the newborn, and the mother–infant relationship (Field, 2010; Śliwerski et al., 2020).
Psychological interventions are effective in the treatment of PPD (Nillni et al., 2018) and are among the preferred options reported by postpartum women (Goodman, 2009). A recent systematic review of systematic reviews and meta-analyses revealed that cognitive–behavioral therapy (CBT) is the most effective evidence-based psychological treatment for PPD (Branquinho et al., 2021b). According to the CBT model, cognitions are the “key” to understanding emotional and behavioral reactions in certain situations (Beck, 1995). Cognitions are based on a person’s previous experiences and held beliefs, and they manifest through automatic thoughts, which in turn influence emotional and behavioral reactions (Wenzel & Kleiman, 2015). CBT-based interventions for PPD are grounded in this principle, which also assumes that previous experiences and factors (e.g., biological and psychological) contribute to the development of vulnerability to certain underlying beliefs (Wenzel & Kleiman, 2015). Wenzel and Kleiman (2015) also hypothesized that these beliefs, which manifest through automatic negative thoughts, are activated during stressful periods that evoke transitions or changes and therefore play a central role in the development and maintenance of PPD. Given the particular and demanding challenges that are inherent to the postpartum period, CBT treatment in this context should focus on specific beliefs about motherhood and include an interpersonal component for greater efficacy (Batt et al., 2020), covering aspects such as the importance of practical and emotional support and dealing with changes within a couple’s relationship (O'Mahen et al., 2012; Finlayson et al., 2020).
Blended Psychological Interventions for PPD
Despite the existence of effective treatment, many women do not seek professional help for their depressive symptoms during the postpartum period (Fonseca et al., 2015) due to lack of knowledge (e.g., where to obtain help) and practical barriers (e.g., lack of time and childcare constraints), as well as stigma perceptions (Button et al., 2017; Goodman, 2009). Recent efforts to develop new formats of psychological interventions have been conducted, such as blended interventions.
Blended interventions combine “traditional” face-to-face psychotherapy with e-mental health tools, such as web-based programs, which complement each other in a sequential and integrated protocol (Erbe et al., 2017). In this format, sessions through online programs can replace some face-to-face sessions with a therapist. It is common to incorporate the time-consuming elements of psychotherapy, such as psychoeducation and exercises, to web-based programs to provide patients the opportunity to practice between sessions and integrate the strategies into daily routines (Ebert et al., 2018). A blended treatment for PPD could therefore present many advantages for postpartum women, such as cost reduction (decreased number of sessions with a therapist, reduction of travel costs), and increased flexibility, accessibility, and intensity, by decreasing the time gap between face-to-face sessions (Erbe et al., 2017; Lal & Adair, 2014; Titzler et al., 2018). In addition, a blended treatment also contributes to increasing women’s autonomy, by allowing them to advance in their own time and at their own pace, to access contents and exercises between sessions with a psychologist (Titzler et al., 2018), and reducing the shame and stigma associated with help-seeking (Ebert et al., 2018).
Be a Mom Coping with Depression is a blended intervention for PPD, combining sessions with a psychologist and online sessions through a web-based program, which is currently being developed in Portugal (Branquinho et al., 2020). The web-based program was previously created and evaluated as a self-guided tool for the prevention of PPD among Portuguese women presenting high risk for PPD (Fonseca et al., 2018b, 2020a). The blended intervention was developed according to CBT principles applied to PPD—it is problem-oriented, educative, structured and time-limited, promotes women’s active collaboration and participation, and is focused on the present (Fonseca et al., 2020b). It also included third-wave CBT contributions applied to the postpartum period, namely, elements of self-compassion and acceptance and commitment therapy (ACT) (Bonacquisti et al., 2017).
General structure of the blended intervention Be a Mom Coping with Depression.
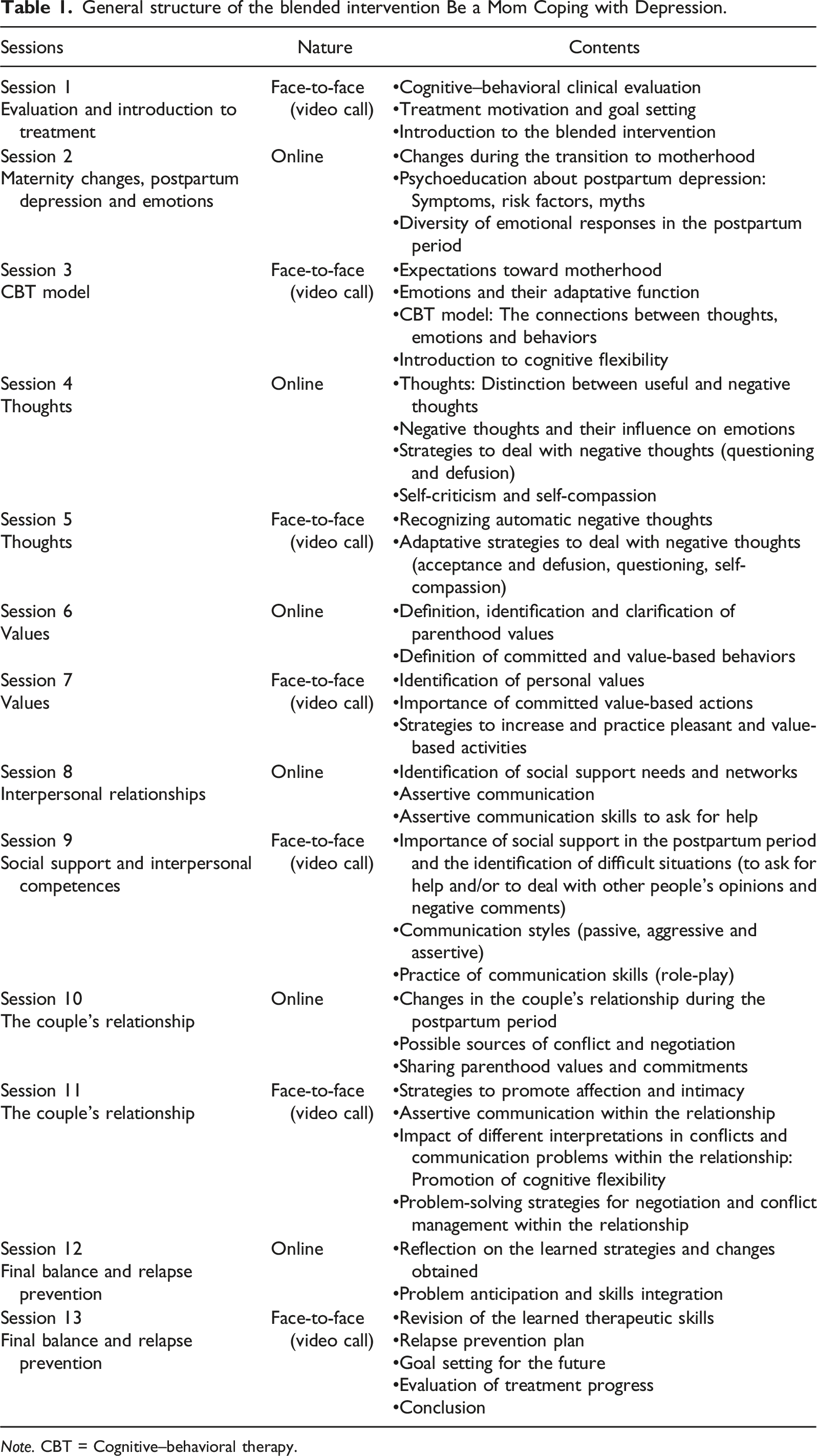
Note. CBT = Cognitive–behavioral therapy.
Online sessions included information and exercises that did not require the therapist’s intervention, and further discussion of the individual’s experience and practice with strategies was incorporated in the sessions with the psychologist. The online program (https://beamomcopingwithdepression.pt/) was organized into five modules that participants accessed between the sessions with the psychologist, according to the instructions given. Each online session took approximately 30–45 minutes to complete and included information and exercises in different formats (e.g., text, video, and audio). The sessions with the psychologist were provided biweekly. Each session lasted approximately 1 hour and included an initial mood check, a review of the experience with the online program and its contents, doubt clarification, and further discussion of each week’s theme and in-session practice of the therapeutic strategies. At the end of the session, the next online module theme and objectives were presented. Email reminders and phone calls between the sessions were delivered to remind the participant of the next week’s module and session appointment, to motivate and to encourage engagement in the online sessions. This blended intervention was developed before COVID-19 pandemic. Given the restrictions imposed in Portugal to activities delivered face-to-face, the intervention was adapted, so that the sessions with the psychologist occurred through video call using videoconference tools (e.g., Zoom).
2 Case Introduction
Sofia (pseudonym) was a 31-year-old Portuguese woman, married for 5 years, with a 10-month-old infant. This was her first child and she did not have any serious medical problems. Sofia had a high education level (master’s degree) and was a health professional. She was employed, had a part-time job, and lived in a rural area. Sofia reported having depression when she made the first contact to get help through this intervention.
3 Presenting complaints
Sofia reported depressed mood, sadness, loss of interest and pleasure in activities, decreased appetite and weight loss, insomnia and sleep deprivation, fatigue, feelings of depreciation and guilt, and decreased concentration during 2 weeks in the previous month to the assessment. She did not present suicidal ideation or suicide attempts. Sofia mentioned feeling more isolated, lack of partner support, and reported difficulties managing daily household tasks and disagreeing with other people’s opinions. In addition, she described that her baby had a difficult temperament (being agitated, crying a lot, having difficulty to settle her down), and manifested worries about financial issues.
4 History
Sofia had a history of depression, reporting a previous episode of depression when she was 20 years old and was studying at university. At that time, she sought professional help and took antidepressant medication prescribed by her general physician. After that episode of depression, Sofia pointed out that she experienced difficulties again in the perinatal period. Sofia said this was a planned pregnancy. She described the last 2 months of pregnancy, which were coincident with the period of lockdown due to the COVID-19 pandemic in Portugal, as “a very difficult time”. During that time, Sofia slept apart from her partner because of fear of possible contamination of herself and the baby, and she expressed the thought “I was totally alone”. The baby was born at 39 weeks of gestation and did not have any medical problems. After childbirth, Sofia mentioned that her partner was afraid of caring for the baby in the first months postpartum (e.g., holding the baby, giving a bath, and feeding the baby) because he was afraid to unintentionally hurt the baby. According to her, this reinforced her feelings of loneliness. Additionally, she mentioned a decrease in marital satisfaction and intimacy. A few months later, Sofia was temporarily separated from her partner and stayed at her parents’ house due to her partner’s lack of comprehension of her difficulties and support in household tasks. The patient referred to the postpartum period as a painful period, reporting hemorrhoid-related problems during the first 3 months after childbirth and feeling pain up to 6 months postpartum. In addition, Sofia described the return to work as a stressful situation. Sofia mentioned having practical support from her mother and mother-in-law when she needed (e.g., to take care of the baby and to cook meals). The current depressive symptoms started, according to the patient, 4 months after childbirth. Sofia mentioned that she had started psychological treatment a few months earlier than the present treatment but dropped out for financial reasons. The patient was not taking any antidepressant medication, had no history of drugs and alcohol use and had no history of depression in her family.
5 Assessment
Before the beginning of the treatment, a clinical interview was conducted by telephone to assess the presence of a major depressive episode through an adapted version of the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013; First et al., 2017). Sofia also completed a set of self-report questionnaires, which included the following:
Edinburgh Postnatal Depression Scale (EPDS; Portuguese version [PV]: Areias et al., 1996). The EPDS is a 10-item instrument (e.g., “I have been able to laugh and see the funny side of things”) that assesses the presence of PPD symptoms, with a 4-point Likert answer scale ranging from 0 to 3. The total score can range between 0 and 30, and higher scores are indicative of more severe depressive symptoms. A score of 10 or higher suggests the presence of clinically relevant depressive symptoms.
Hospital Anxiety and Depression Scale - Anxiety subscale (HADS-A; PV: Pais-Ribeiro et al., 2007). The HADS-A evaluates anxiety symptoms and is composed of seven items (e.g., “Worrying thoughts go through my mind”) answered on a 4-point Likert scale ranging from 0 to 3. The total score for this subscale can range between 0 and 21, and higher scores indicate higher levels of anxiety symptoms. A score of 11 or higher suggests the presence of clinically relevant anxiety symptoms.
Investment Model Scale - Satisfaction subscale (IMS-S; PV: Rodrigues & Lopes, 2013). The IMS-S assesses marital satisfaction through five items (e.g., “My relationship is close to ideal”) rated on a 9-point scale ranging from 0 (do not agree at all) to 8 (completely agree). Higher scores are indicative of higher satisfaction with the relationship.
Perceived Maternal Parenting Self-Efficacy questionnaire (PMP S-E; Barnes and Adamson-Macedo, 2007). The PMPS-E assesses maternal self-efficacy using 20 items (e.g., “I can read my baby’s cues”) answered on a 4-point scale ranging from 1 (strongly disagree) to 4 (strongly agree). The total score can range between 20 and 80, with higher scores indicating higher perceived maternal self-efficacy.
Self-Compassion Scale - Short Form (SCS-SF; PV: Castilho et al., 2015). The SCS-SF evaluates self-compassion and comprises 12 items (e.g., “I’m disapproving and judgmental about my own flaws and inadequacies”) answered on a 5-point response scale ranging from 1 (almost never) to 5 (almost always). The total score can range between 12 and 60, with higher scores revealing higher levels of self-compassion.
Acceptance and Action Questionnaire-II (AAQ-II; PV: Pinto-Gouveia et al., 2012). The AAQ-II is a 7-item instrument (e.g., “I’m afraid of my feelings”) that assesses psychological flexibility. Items are answered on a 7-point Likert scale ranging from 1 (never true) to 7 (always true). The total score can range between 7 and 49, with higher scores suggesting lower psychological flexibility and higher experiential avoidance.
Mood ratings to assess depressed mood were conducted at the beginning of each session with the psychologist through questions developed by the research team (“How do you feel today? How is your mood on a scale of 0 to 10?”), using an 11-point Likert scale ranging from 0 (absence of depressed symptoms) to 10 (maximum of depressed symptoms).
Data concerning usage information (number of logins, average time spent at each login, average number of days between logins, number of completed exercises) were obtained from the website’s system to assess patient compliance and adherence to the online program.
6 Case Conceptualization
Sofia experienced the transition to motherhood as a very difficult time, with perceived losses in several areas, including her social relationships (social isolation, lack of practical support), her marital relationship (decrease in couple’s intimacy, lack of support, difficulties in communication) and personal domains (diminished sense of competence and self-efficacy). Sofia’s previous history of depression, medical complications in the postpartum period, her baby’s difficult temperament and lack of partner’s support are usually reported in the literature as risk factors for PPD (Hutchens & Kearney, 2020). In addition to the context of the COVID-19 pandemic and experiencing the postpartum period with high stress, these factors may have contributed to Sofia’s increased vulnerability to develop depressive symptoms. These events may have contributed to activating dysfunctional cognitions, such as “I am not able to do anything”, “I am not doing enough” and “Nobody understands me” and to internalizing beliefs such as “I am alone” and “I am not a good mother”. These dysfunctional thoughts and beliefs could have contributed to the maintenance of depressive symptoms and were reinforced by her emotional and behavioral reactions. For instance, Sofia reported that she could not do the household chores and the thought “I can’t do anything”, while feeling overwhelmed and guilty, reinforced the behavioral reaction of not performing the tasks.
In line with this, blended treatment was planned to provide Sofia with strategies to deal with motherhood expectations, to understand the function of emotions, to identify negative thoughts and to learn how to cope with them in a more adaptative way, to engage in value-based actions, to develop communication skills and to ask for support, to increase the quality of the couple’s relationship and to create a relapse prevention plan.
7 Course of Treatment and Assessment of Progress
Therapist
The therapist who conducted the intervention was a licensed psychologist with a master’s degree in clinical psychology and was trained in CBT. During the application of the intervention, the psychologist followed a detailed therapist manual and was supervised in biweekly sessions by an experienced postdoctoral-level psychologist.
Course of Treatment
Sofia received 13 sessions of the blended intervention (7 sessions delivered by the psychologist and 6 sessions delivered through the online program) and one follow-up session. The intervention was conducted from April to July 2021.
Session one
The first session aimed to establish the therapeutic relationship with Sofia and to conduct a brief cognitive–behavioral clinical evaluation and a collaborative conceptualization of the patient’s difficulties. The influence of vulnerability factors and stress situations she experienced over the past months on the development of depressive symptoms, as well as the role of negative thoughts and their relationship to emotions and behaviors, was explained. Sofia recognized a pattern of negative thoughts associated with her feelings of guilt, inability to do household tasks, exhaustion and tiredness, and described this mutual influence as a “snowball that keeps increasing.” Afterward, Sofia defined her therapeutic goals for the treatment in several areas, namely, the individual domain (e.g., “to be more flexible with my expectations for myself”), household-related tasks (e.g., “to be able to do the house tasks and cook meals”), her marital relationship (e.g., “going out as a couple once a month”), her interpersonal relationships (e.g., “to have lunch with my friends once a month”), the professional domain (e.g., “get a full-time job”) and engagement in pleasurable activities (e.g., “to read a romance book for 15 minutes a day”). In the final part of the session, Sofia was presented with an overview of the blended intervention and to the online program, including the next week’s module.
Session 2 (online)
The first module elucidated about changes due to motherhood and family reorganization, role idealization and unrealistic expectations toward motherhood, and normalized Sofia’s experience during this period. Then, psychoeducation about PPD was provided, including its prevalence, symptoms, risk factors, associated myths and possible consequences if untreated, followed by psychoeducation about emotions—the diversity of emotional responses, the possible discrepancy between expected emotions and emotions actually felt during the postpartum period, the promotion of their nonjudgmental evaluation, and the links between thoughts, emotions, and behaviors.
Session 3
Concerning her experience with the first module, Sofia mentioned that it was useful “to view little by little” to provide an opportunity to think and reflect about the contents. It was evident that Sofia was motivated to change by her reports that “I want to be well, and for that I have to do my part.” In addition, Sofia reported an improvement in her mood and that during that last week, she was able to cook meals.
The therapist promoted reflection on motherhood changes, social expectations and their impacts on depressive symptomatology. Sofia believed in some myths about PPD that were presented in the module (e.g., “Only weak or bad mothers have postpartum depression”) and realized that her expectations about motherhood were not realistic. The distinctiveness of each maternity experience was discussed, and Sofia said “I understand that but it is very difficult to accept, particularly in my environment, where there are some babies now, and other people are constantly comparing them; it is very frustrating.” and “I feel that my role as a mother is at stake”. Sofia recognized the negative impact of her expectations about motherhood, both external and internal, associated with her perfectionism and self-criticism traits. She referred to the following example of her internal dialogue: “My mother keeps saying that she had three children and that she was able to do everything at home, and I only have one baby and I can’t do anything”. The social pressure to be a “perfect mother” and the stigma associated with revealing emotional difficulties during the postpartum period were discussed to promote its normalization and acceptance.
Regarding the topic of emotions, the therapist normalized the diversity of emotions and the discrepancy between what Sofia expected and what she actually felt during the postpartum period. Sofia mentioned that she did not expect to feel alone and without support from her partner, with the thought “My life has changed and his did not”. Psychoeducation about the adaptative function of emotions was discussed to promote their acceptance and noncritical evaluation. Then, the cognitive–behavioral model was revised, and Sofia was asked to identify a recent situation and links between her thoughts, emotions and behaviors. This exercise also allowed the promotion of cognitive flexibility by asking her to think of possible alternative interpretations for the situation. The patient was asked to keep performing this thought record through the exercise that would be proposed in the next module.
Session 4 (online)
The second module was focused on psychoeducation about thoughts (their automatic nature, the distinction between useful and negative thoughts) and normalizing negative automatic thoughts in the postpartum period. An exercise was proposed to identify negative thoughts and their link to emotions and behaviors. Psychoeducation about the poor effectiveness of thought suppression and cognitive fusion was provided, and more adaptative strategies to deal with negative thoughts were presented—cognitive defusion, acceptance and non-evaluation of thoughts, and thought questioning. The final theme focused on self-criticism and promoted self-compassion as a helpful strategy to deal with private negative and judgmental evaluations.
Session 5
Sofia started by reflecting on the strategies learned in the previous module: “the most important strategy was the way I could deal with the negative thoughts”; “when I was overthinking about something, I asked myself ‘Is this thought useful?’ and it helped me to break that chain of thoughts” and “it has had an impact on my emotions; they are not as strong as before”. The therapist reviewed the thought record exercise that Sofia completed, normalized the existence of negative thoughts during the postpartum period and promoted a reflection on alternative interpretations to increase cognitive flexibility. Then, the ineffectiveness of thought suppression and cognitive fusion (i.e., belief in the thoughts) was discussed, with Sofia mentioning “I can’t control my thoughts, but I can question them”. Afterward, the therapist reviewed and practiced the adaptative strategies to deal with the negative thoughts with the patient—acceptance and cognitive defusion, thought questioning, and self-compassion.
Session 6 (online)
The third module was divided into two different sessions. The first session was dedicated to defining, identifying and clarifying parenthood values and to promoting behavioral activation through value-based actions. An exercise was proposed, and Sofia was directed to reflect on the impact of performing the value-based activities and behaviors on her mood.
Session 7
Sofia mentioned feeling better, with more energy and a better mood. During the last week, she had been practicing thought questioning and revealed increased cognitive flexibility when interpreting her daily situations. In addition, the patient wrote a self-compassionate letter for herself to read when she was facing more difficult moments: “Sofia, I know it has been hard and that you feel unsupported and misunderstood. Be patient and time will help to clarify things. Try to take things slowly without putting too much pressure on yourself. The most important thing is that you and your daughter are well. You have been demanding a lot from yourself, but you have also been giving a lot. Take time for yourself now, to recover and to calmly go back to the battle. You will be happy.”
In this session, Sofia said that it was difficult to identify her values by saying “I know what my values as a mother are, but I am not just a ‘mother’. I am also a woman, a wife…”. The therapist helped Sofia reflecting on her personal values—parenthood-related values (e.g., “to be a present mother”) and individual values (e.g., “to be more connected with myself”)—and how to manage the perception of conflict between values. Then, the importance of doing committed value-based actions was discussed: the impact of not doing value-based actions on depressed mood and strategies to increase and engage in those pleasant and value-based activities (e.g., goal definition, time management, and cognitive defusion to deal with negative thoughts or emotions of guilt).
Session 8 (online)
The second part of the third module aimed to identify Sofia’s social support needs and sources of support among her network and to reduce social isolation. Psychoeducation about assertive communication was given as a helpful communication skill to ask for support and to deal with other people’s comments, and assertive communication techniques were provided.
Session 9
The importance of social support in the postpartum period was reviewed, and Sofia highlighted the importance of the module’s exercise aimed at identifying her needs and sources of support (“I was sad when realized that he [my partner] was not a source of support; it hurts me to know that I cannot count on him”). The therapist and Sofia collaboratively discussed possible solutions to include her partner in practical and emotional support. Then, the importance of assertive communication when asking for support was explained (e.g., using specific requests, showing appreciation, and body posture).
The topic of communication and how to deal with difficult situations was introduced (e.g., dealing with other people’s opinions). The patient reported some changes in her behavior in how she faced these situations by using the strategies for being assertive (“I adopted the ‘broken record’ technique. I assumed my position and I said ‘no’; people kept insisting and saying the same thing, and I kept answering ‘no, thanks’ or ‘no, it is not necessary.’”) and by acting in accordance with her values (“I do what I think is best and what makes sense for me”). The communication styles (passive, aggressive, and assertive) were briefly described in collaboration with the patient. In this context, Sofia revealed some difficulties in communicating with her partner (“I try to communicate, but it is very difficult; sometimes he does not answer, or I talk and he just nods his head”). A role-play exercise was proposed to practice in-session the learned communication skills in a situation of asking her partner for support.
Session 10 (online)
Sofia completed the fourth module about the couple’s relationship, which included three main themes: the changes in the couple’s relationship during the postpartum period and how to promote and increase affection and intimacy; the possible sources of conflict and the promotion of negotiation, assertive communication and problem-solving skills within the relationship; and sharing parenthood values and the normalization and acceptance of differences.
Session 11
Concerning the experience with the module about the couple’s relationship, Sofia considered that this was the most difficult topic for her and reported difficulty in viewing this module with her partner (“I tried to share the module with him [my partner], but he did not want to participate”). The main changes felt by Sofia in her marital relationship during the postpartum period were the presence of distinct expectations about the postpartum period (“He [my partner] thought it was going to be like before”), the rise of communication difficulties and the lack of sexual desire. The therapist normalized these changes and encouraged the patient to find other pleasurable activities for the couple and daily gestures of affection. In this context, Sofia felt that her partner did not perform these gestures toward her (“I got tired of unilateralism and stopped doing it because I also want to receive.”) and that he did not understand her tiredness (“To him, I am not tired because I have a lot of free time”) and lack of sexual desire (“He thinks I am not trying hard enough. However, I actually do not feel like it, but he does not understand.”). Sofia also revealed that it was difficult to overcome the existing communication challenges due to feelings that her partner was not available to change (“I feel ignored”; “His lack of communication is very difficult to deal with.”) and because they had very different perceptions of reality (“His perception is totally different from mine: of the daily routine, how to care for a baby, he does not realize how much work and how exhausting it is.”). Assertive communication tips were reviewed to promote conflict resolution and to encourage Sofia to share her feelings with her partner, and an active listening exercise was proposed for the couple. In addition, cognitive flexibility was promoted concerning the different perceptions mentioned by Sofia. For instance, the thought “My life has changed and his did not” was discussed by examining the evidence that supported and refuted it. The therapist also reviewed the strategies for negotiation and conflict management within the relationship, as presented in the module.
Session 12 (online)
The final module aimed to promote reflection on the learned skills and changes obtained by Sofia during the intervention, as well as to develop a relapse prevention plan, by identifying alert signs and future difficulties and how to use the learned strategies to deal with them. By the end of the module, Sofia was invited to write a testimony of her experience with the intervention: “With this program, I reflected on the changes after the birth of my daughter and learned to accept and recognize them as normal”.
Session 13
Sofia started by sharing her reflection about the relationship with her partner over the last few days, mentioning that she needed to accept the things she could not control, such as her partner’s work schedule and his little availability to be with the baby, and revealed some improvements in their communication and in the support provided by him.
In this last session of the intervention, the therapist reinforced the patient’s therapeutic progress, and Sofia recognized her changes and the importance of the learned strategies (“the management of expectations, the awareness that what I think is not always true, that all emotions are good to help us understand what is good and bad. Now, when I'm feeling down, I question my thoughts a lot to stop that chain of thoughts”). The patient also described to being able to concentrate, to engage in pleasurable activities, such as reading, and to better manage her daily routine. Then, the therapist and the patient collaboratively reviewed the learned skills and the relapse prevention plan developed by Sofia in the online module. The patient identified the increase of a work schedule, her daughter getting sick and getting pregnant again as alert situations that could contribute to increase depressive symptoms, and she recognized that “activating my support network, talking to my partner, to better organize the routine,” dealing with negative thoughts and conducting value-based actions would be helpful strategies. Then, the objectives defined in the first sessions were revisited, and Sofia realized she had achieved most of them, which reinforced her therapeutic progress. She also defined objectives for the future (e.g., “to practice physical exercise, to dedicate more to self-care”). At the end of the session, Sofia was praised for her motivation and dedication to treatment and was encouraged to keep practicing the learned skills to maintain the achieved gains.
Assessment of Progress
The reliable change index (RCI) was calculated to examine the changes obtained by Sofia in the self-report measures. The RCI is obtained by dividing the difference between post- and pretreatment by the measurement error of the instrument (Jacobson & Truax, 1991; Tingey et al., 1996) using the following formula:
Patient’s pre- and post-intervention assessments.
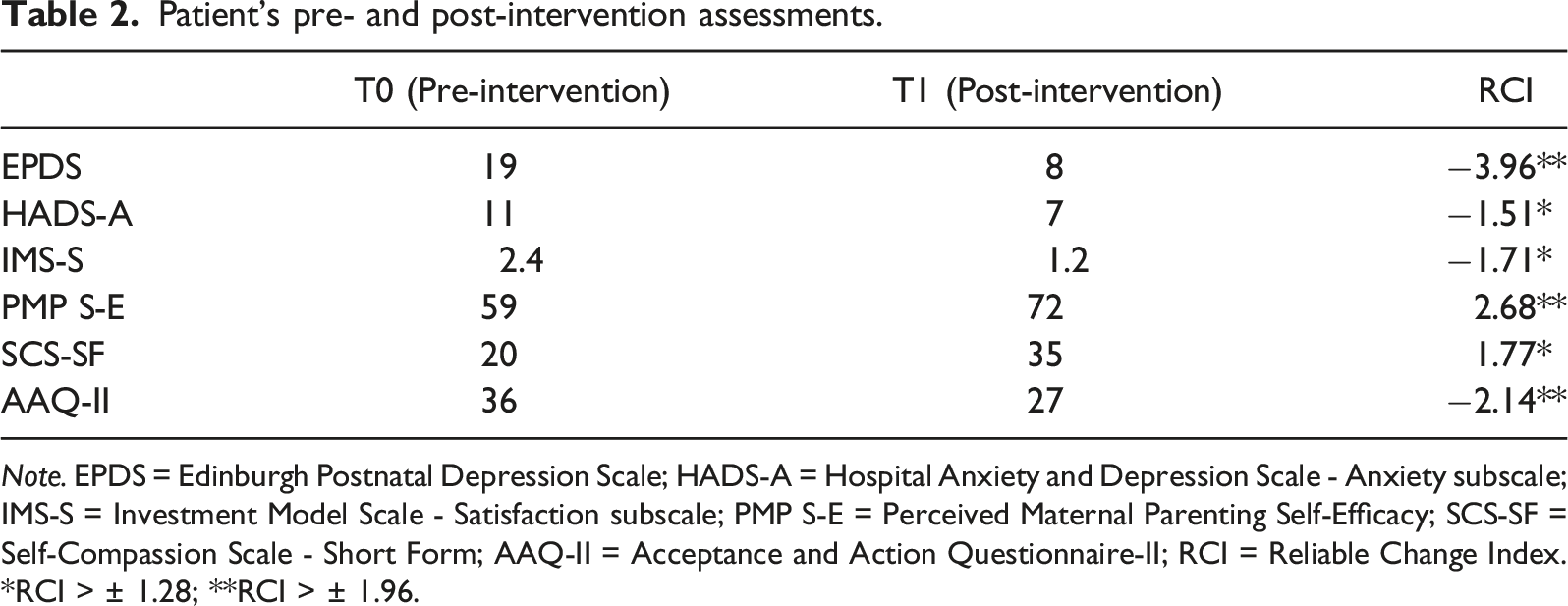
Note. EPDS = Edinburgh Postnatal Depression Scale; HADS-A = Hospital Anxiety and Depression Scale - Anxiety subscale; IMS-S = Investment Model Scale - Satisfaction subscale; PMP S-E = Perceived Maternal Parenting Self-Efficacy; SCS-SF = Self-Compassion Scale - Short Form; AAQ-II = Acceptance and Action Questionnaire-II; RCI = Reliable Change Index. *RCI > ± 1.28; **RCI > ± 1.96.
In Figure 1, a graphic with the mood ratings throughout the sessions is represented. A decrease in self-reported depressed mood was observed, which ranged from 7 (Session 1) to 4 (Session 13) out of a maximum of 10. Depressed mood reporting throughout the sessions.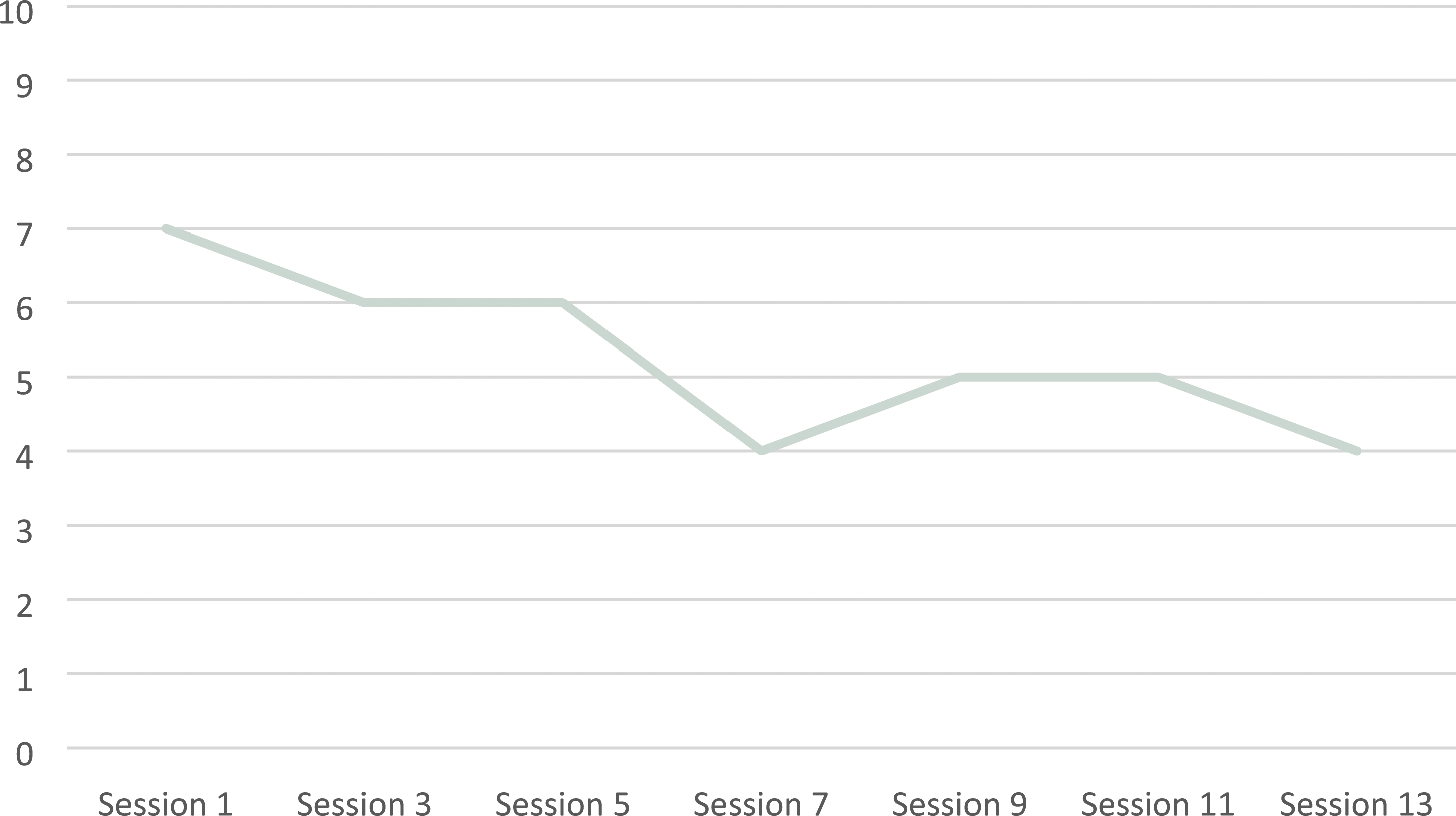
Data concerning usage information revealed a total of 30 logins (average time at each login of 12 minutes) on the website during the intervention period of 13 weeks, with an average of 4 days between logins, and all 13 exercises proposed in the online program were completed.
Patient feedback regarding the treatment was very positive, and Sofia recognized beneficial changes (“it allowed me to gain awareness of my difficulties,” “my problems did not disappear, my way of dealing with them is different now, so I believe I am better”).
8 Complicating Factors
The main complicating factors of Sofia’s progress were the decreased marital satisfaction, the lack of support from her partner and their communication difficulties. In fact, poor marital relationships and low social support are considered important factors in both the development and maintenance of depressive symptoms during the postpartum period by increasing the stress associated with motherhood changes (Hutchens & Kearney, 2020; Wenzel & Kleiman, 2015). Given that this was a structured intervention, including the partner in some sessions was not considered. In Sofia’s case, future sessions with her partner could be particularly beneficial to clarify expectations about their roles, their relationship and parenthood, to promote communication skills and to practice problem-solving strategies to increase partner support.
9 Access and Barriers to Care
There were no evident barriers to care given the online nature of this intervention. Sofia had an internet connection at home and accessed the online modules of the program through her smartphone and computer. Additionally, Sofia was offered the possibility to reschedule any session with the therapist when necessary, and she requested to reschedule one session because her daughter was sick.
10 Follow-up
A follow-up session was provided 1 month after the end of the intervention. Sofia reported feeling “more emotionally stable” and being able to be less reactive in certain situations (e.g., stressful situations). Sofia still reported sleep deprivation but faced it with increased flexibility (“I know this is a transition period”), and also mentioned difficulties managing and sharing household tasks with her partner. In this context, Sofia did not describe any changes and mentioned that her partner still did not understand her point of view regarding the baby’s care and her feelings of tiredness. Despite that, Sofia changed the way she deals with this situation (“Even recognizing this as a difficulty, I think I am dealing better with it. I can see a difference. Now, when I am upset, I will talk to him [my partner] about how I feel; it is better to find a solution.”) and how she deals with her negative thoughts (“I was able to change my way of thinking and to perceive things differently”). Sofia also described a situation in which her partner acted against the value-based action defined by the couple concerning the baby’s feeding, and Sofia was encouraged to keep using the assertive communication style. The patient felt closer to her partner, having created more opportunities to be together and to promote their intimacy. Given the difficulties experienced in the couple’s relationship, the patient was recommended couple’s therapy. Sofia said that she already thought about that option when she was separated from the partner and she agreed that it could be important for them. Regarding the objectives defined in the last session, Sofia has been increasing physical exercise (e.g., walking) and mentioned that she would like to practice meditation and to learn English.
11 Treatment Implications of the case
This clinical case is part of a feasibility study assessing the acceptability of Be a Mom Coping with Depression, and to our knowledge, this is the first blended CBT intervention developed for the treatment of PPD. In this case study, the intervention was effective in reducing anxiety and depressive symptoms. It also seemed to contribute to increasing maternal self-efficacy and to developing psychological competences of psychological flexibility and self-compassion. These findings are quite promising, reflecting the effectiveness of CBT in treating depressive symptoms in the postpartum period (Ammerman et al., 2007; Crespo-Delgado et al., 2020; Nillni et al., 2018), including third-wave CBT strategies. Research interest in ACT and self-compassion therapies applied to the perinatal period has increased in the last years and revealed positive results in this population (e.g., Waters et al., 2020), which reinforces their inclusion in therapeutic protocols for PPD treatment.
This case study indicated that a blended intervention for PPD presents strengths for women during the postpartum period. Sofia perceived the blended intervention for PPD as positive and useful, highlighting time savings in transportation, decreased costs, the possibility to review content in the online program and to progress on her own time, and to better explore online exercises with the psychologist in-session. In fact, a blended treatment format has the benefit of providing patients with psychoeducation through an online program and therapeutic strategies to practice, allowing for better preparation for the session with a therapist, which in turn contributes to increased treatment intensity (Schuster et al., 2018; Titzler et al., 2018). This is in line with our previous research indicating that postpartum women presenting depressive symptoms would be available to receive blended psychological treatment and that this format would be useful (Branquinho et al., 2021a). Therefore, a blended treatment format can contribute to increase postpartum women’s access to effective treatment for PPD by overcoming some help-seeking barriers they often report (Button et al., 2017) and to improve their motivation, self-management and active roles in the treatment (Schuster et al., 2018).
Moreover, this case study also provides insight into therapeutic alliance and adherence to treatment. Throughout the sessions, Sofia described an adequate therapeutic relationship, considering that the online format of the sessions with the psychologist (through video calls) did not compromise it and she engaged positively in both the online and therapist sessions. This can have important implications that are particularly relevant during a pandemic or emergency context. As opposed to what was expected to be a disadvantage of a blended treatment (Branquinho et al., 2021a), the fear of having a “weaker” therapeutic relationship or lack of motivation were not reported by Sofia or observed by the therapist. In addition, using video calls for “face-to-face” sessions may become even more advantageous for women during the postpartum period, since it can reduce stigma associated with seeking professional help during this period or the possibility for the mother to be with her baby during the session. In line with this, clinical guidelines for interventions delivered through information and communication technologies, including interventions through video calls, have been developed for professional practice (e.g., Carvalho et al., 2019) and address specific aspects that need to be followed (e.g., guarantee of confidentiality and obtaining informed consent).
Despite the encouraging results that were found, the conclusions drawn from this clinical case study may not be applicable to all patients receiving blended interventions. The results from the feasibility study will be important to understand the acceptability and preliminary efficacy (not controlled) among a larger sample of women with PPD. Additionally, this case was selected given Sofia’s motivation and adherence to treatment, which allowed us to describe the intervention in detail.
12 Recommendations to Clinicians and Students
Some implications for clinical practice can be drawn from this study. First, we highlight some specificities that should be included in CBT interventions for PPD. As previously exposed, it is particularly important to address motherhood-specific beliefs, discuss expectations and cultural concepts, promote social support, and address couple’s relationships (Crespo-Delgado et al., 2020; O’Mahen et al., 2012). Moreover, we reflected on the potential benefit of including the partner in the intervention, for instance, by assisting in the module about the couple’s relationship or by participating in this session with the psychologist. Previous literature on partner-inclusive interventions indicated that sessions including the partner aim to provide psychoeducation about PPD and to provide strategies such as communication skills, managing household tasks and giving emotional and instrumental support (Alves et al., 2018), which in Sofia’s case, and for other women experiencing marital conflict and dissatisfaction, would be of great relevance.
Second, blended psychological interventions are potentially helpful not only for women experiencing PPD but also for individuals with other mental health problems. In fact, blended interventions are progressively receiving attention from researchers worldwide, with increasing preference for this treatment format among clinicians (Phillips et al., 2021). Recent studies with psychologists revealed a moderate to high acceptance toward blended treatment (Baumeister et al., 2020) and a higher acceptability toward blended interventions when compared to only online or web-based interventions (Mendes-Santos et al., 2020). In fact, previous studies revealed that clinicians recognized several advantages of blended therapy, such as time savings, the possibility of attending more patients by reducing the number of sessions and the gap between sessions that exist in health care systems, and customizing sessions as a function of patients’ needs (Schuster et al., 2018; Titzler et al., 2018). Therefore, blended interventions are also beneficial to clinicians, and more research is warranted to expand the use of this innovative treatment format.
Further studies will be conducted by the research team to assess the clinical efficacy of the intervention within a clinical trial. If proven effective and cost-effective, Be a Mom Coping with Depression can gain acceptance among several stakeholders, such as postpartum women, therapists, and health care services.
Footnotes
Acknowledgments
We would like to thank Sofia (pseudonym) for her permission to share her history in this publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mariana Branquinho was supported by a PhD scholarship from the Portuguese Foundation for Science and Technology (SFRH/BD/145563/2019).