
Abstract
Foreign accent syndrome (FAS) has historically been attributed to a neurological etiology. However, recent research has identified psychogenic causes of FAS, where patients present to health care services with medically unexplained FAS symptomology. Due to the rare nature of psychogenic FAS, there is currently no evidence-based psychological treatment for this syndrome. Although patients with psychogenic FAS do not meet the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) or the International Classification of Diseases (ICD)-10 diagnostic criteria for a diagnosis of somatization disorder, there are some similarities in presentation between psychogenic FAS and the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria for somatic symptom disorder (SSD). These include the presence of distressing and disruptive symptoms that result in increased health care utilization. Given the emerging evidence for cognitive behavioral therapy (CBT) for SSDs, it is arguable that CBT could help patients with psychogenic FAS to manage the psychological distress they experience. This paper aims to explore the use of CBT in reducing the psychological distress of a patient with no organic explanation for FAS using a single-case (A-B) experimental design. The results suggest that CBT was effective in reducing distress, as measured using the Clinical Outcomes in Routine Evaluation–Outcome Measure (CORE-OM). This paper highlights the value in using an individualized formulation-driven CBT approach for presentations that do not yet have evidence-based guidelines. In this case, cognitive restructuring, activity scheduling, and stress management appear to be key mechanisms of change in reducing psychological distress associated with FAS.
Keywords
1 Theoretical and Research Basis for Treatment
Foreign accent syndrome (FAS) is a rare motor speech disorder (Jonkers et al., 2017), for which the prevalence remains unknown. FAS is characterized by a change in prosody and articulation (Reddy et al., 2016) and is perceived by listeners to be a new accent that differs from an individual’s native language (McWhirter et al., 2019). Until relatively recently, FAS was believed to have a neurological cause, requiring medical and neuro-rehabilitative treatment. Over the past century, there have been 112 published FAS cases, the majority of which are associated with neurological damage that is acquired, congenital, or developmental in nature (Mariën et al., 2019). However, as Mariën et al. identified, in 18 of the 112 cases (16%), FAS developed in the context of psychiatric issues, thus contributing to emerging evidence for a psychogenic etiology.
A FAS taxonomic classification, developed by Verhoeven and Mariën (2010), distinguishes between (a) neurogenic, (b) psychogenic, and (c) mixed FAS, with each variant having unique characteristics (Asogwa et al., 2016). Neurogenic FAS involves an accent change caused by damage to the central nervous system (CNS), which affects the language dominant areas of the brain (Verhoeven et al., 2013). Neurogenic FAS is associated with etiologies including brain trauma, stroke, multiple sclerosis (MS), and vascular dementia (Keulen et al., 2016), with possible comorbid speech and language impairments such as dysarthria, apraxia, and aphasia that might accompany FAS. Psychogenic FAS has no known organic cause but may be preceded by mutism (Jones et al., 2011) and may be characterized by difficulties including, for example, dysphonia (impaired or disordered voice) or aphonia (absent voice), which is believed to be perpetuated by psychological or emotional factors (Butcher et al., 2007). Grammatical anomalies may also be present with psychogenic FAS (Cottingham & Boone, 2010). Meanwhile, mixed FAS is characterized by neurological damage in addition to a loss of identity that results in increased efforts to improve the authenticity of an accent to create a more coherent identity (Verhoeven et al., 2013). Ryalls and Miller (2015) describe a blending of neurogenic and psychogenic determinants, whereby FAS arises as a functional adjustment to an earlier neurological event (Lee et al., 2016).
With growing interest in this field, recent literature has established psychiatric comorbidities with psychogenic FAS (Ashgar & Whitty, 2020; Gurnani & Horwitz, 2017). For example, abnormal emotional regulation has been identified among those with FAS (Berthier et al., 2016). In addition, links have been established between FAS and the withdrawal of medication, specifically high-dose dopamine or anticholinergic agents (Schuh, 2017) and antipsychotic drugs (Keulen et al., 2016). The term psychogenic FAS is considered by some to be problematic, particularly in instances where there is neither a neurogenic cause nor a presence of any psychiatric conditions (Mariën et al., 2019). The alternative term “functional FAS” is gaining support, as it appears to overcome the aforementioned issues (Lee et al., 2016; McWhirter et al., 2019). Butcher et al.’s (2007) comprehensive work on psychogenic voice disorders revealed common etiological features. These include stressful life events and anxiety, and being more prevalent among females. In addition, common features included family and interpersonal difficulties, with particular difficulties expressing views and emotions, a burden of responsibility, over-commitment and helplessness, and near-normal psychological adjustment, while also being vulnerable to anxiety. Butcher et al. exclude low mood, stating it has not yet been possible to determine whether low mood precedes or follows the voice disorder. They further purport that in psychogenic FAS cases, “the voice problem may manifest itself with musculoskeletal tension and hyperkinetic behaviors and these may eventually give rise to laryngeal pathology, these being products or symptoms of the underlying psychological cause” (p.1). The prognosis for recovery from psychogenic FAS is believed to be good (Haley et al., 2010), although there is no clear treatment pathway.
Given that psychogenic disorders are typified by physical symptoms that remain medically unexplained (Harwood et al., 2018), these presentations represent a challenge to health care services. Patients often experience protracted difficulties, frequently presenting to medical services (Rancourt & Darkes, 2019), yet derive limited benefit from treatment (Woolfolk & Allen, 2012). Although there is now greater awareness of psychogenic FAS, as evident in the growth in publications of single FAS case studies (e.g., Ashgar & Whitty, 2020; Asogwa et al., 2016; Reddy et al., 2016; Schuh, 2017), there is no clear guidance on how best to treat individuals with psychogenic FAS. As such, psychogenic FAS remains a syndrome rather than a disorder, and is not included in diagnostic manuals in its own right. In the absence of evidence-based guidelines for the treatment of FAS, it seems logical to consider recommended treatments for related disorders, such as, somatic symptom disorder (SSD), whereby individuals have persistent somatic symptoms that cause significant disruptions to functioning (American Psychiatric Association [APA], 2013). Like FAS, SSD is characterized by distressing, excessive, and disproportionate feelings and behaviors toward symptoms (APA, 2013). A cognitive approach could be helpful in questioning assumptions that contribute toward patients’ judgment of foreignness and in understanding the influence of illness behavior on the chronicity and maintenance of somatoform symptoms (Gurd & Coleman, 2006; Witthoft & Hiller, 2010). This paper aims to establish whether cognitive behavioral therapy (CBT) is effective in reducing the psychological distress of a patient with FAS and aphonia (with no known organic cause). This study employed an (N=1) A-B single-case experimental design (SCED) (Barlow & Hersen, 2008). The extent of the client’s problems was established during a baseline 3-week assessment period (A) prior to 14 weeks of CBT intervention (B) with a clinical psychologist in training.
2 Case Introduction
This study reports the case of “Becky” (pseudonym), a middle-aged British female living with her husband, “Tom,” and children. Becky was referred for psychological therapy following multiple medical investigations that had failed to find any neurological explanation for her FAS.
3 Presenting Complaints
Becky presented with FAS, alternating between two European accents, with difficulties in word-finding and speech fluency. This was accompanied by periods of not being able to talk (aphonia), low mood and motivation, rumination, anxiety in social settings, poor sleep, low self-confidence, and difficulties communicating with others. Medical and neuropsychiatry reports confirmed a diagnosis of FAS, accompanied by migraines, nonepileptic seizures (NES), dystonia, and facial weakness. Becky was prescribed migraine and epilepsy medication to manage her symptoms. Becky’s life was severely impacted by these problems; she was not able to maintain paid employment, could not drive (as a result of the seizures), and she did not feel confident about going anywhere alone. Becky had to rely on others to go anywhere and reported having strained relationships with friends and extended family. Becky described feeling stuck, as though her life had been on hold in recent years, due, in part, to FAS but also because an “overly-involved” family member was dictating how Becky lived her life.
4 History
Becky first encountered difficulties the day a close relative died; she described an experience of not being able to breathe, as if her body had forgotten how to function, and she interpreted this as a transient ischemic attack (TIA). Following this traumatic event, Becky encountered periods of aphonia, sometimes lasting several weeks. When Becky was able to speak, she did so with a foreign accent. She described a tightening of her facial muscles and a migraine preceding each episode of voicelessness. These symptoms confirmed to Becky that the cause must be neurological. Becky consequently spent several years engaging with medical professionals from a variety of local and national services, seeking a medical diagnosis that would explain her symptoms. However, multiple MRI (magnetic resonance imaging) and CT (computerized tomography) scans, neurological and physical tests, and repeated investigations failed to reveal any neurological cause. Neuropsychiatry reports confirmed that Becky did not meet the diagnostic criteria for any major psychiatric disorder, such as psychosis, personality disorder, bipolar disorder, depression or anxiety, although low mood and mild anxiety were reported. Medical assessments indicated that Becky was cognitively oriented, insightful, and good at communicating in written form. However, a neuropsychiatry assessment reported that Becky was easily fatigued despite adequate sleep, she was exhausted from the effort involved in trying to communicate, and her symptoms worsened during periods of stress. When medical professionals advised Becky that there was no more they could do for her, she was referred to a secondary care psychological therapies service. This left Becky feeling frustrated and helpless; first, because she held firm beliefs about the neurological etiology of her difficulties, and, second, because she saw no utility in psychological input as, in her view, there was no perceived psychogenic cause.
Prior to her bereavement, Becky had a medically unremarkable history; neurologically, growth and development were typical and there was no history of developmental disorders or learning difficulties. However, Becky’s close relative had a neurological condition and another relative had FAS for 6 months following a period of stress, with spontaneous recovery and no difficulties since. Becky previously enjoyed paid employment and effectively maintained positive relationships with a wide network of friends. Becky described her former self as outgoing and personable but said she had since lost this aspect of herself. Becky reported being the “go to” person when others needed to offload their worries. Relationships were important to Becky and she described herself as nurturing and caring, having been the sole carer for her relative during the last months of their life. Becky reported not sleeping for 4 nights prior to her relative’s death and had previously experienced a difficult relationship before her current marriage.
5 Assessment
A structured assessment took place over three sessions to elicit the problems Becky was experiencing. Although the referral information suggested FAS was Becky’s main difficulty, Becky identified the key problems as feeling suffocated by interactions with a family member; not knowing how to fill time or how to gain more independence; not speaking (i.e., aphonia); and needing to find a story to explain the foreign accent when meeting new people. The assessment helped Becky to identify the following goals: (a) re-establish old friendships and/or find new friendships; (b) manage the family member who keeps her feeling “stuck” in not living her life; (c) find meaningful and enjoyable activities to create a new life; (d) develop a narrative to manage new social situations; (e) re-connect with family members following the relative’s death; and (f) resolve conflict regarding differences in parenting approaches. The assessment also identified strengths that had helped Becky to manage difficulties in recent years, including, having a supportive husband and children, being psychologically minded, and willing to try techniques that help, such as creative therapeutic activities and meditation. During the assessment process, Becky vacillated between absolute certainty that the cause of her FAS was neurological, to acknowledging the presence of psychological problems related to spiraling mood, and feeling anxious, angry, and frustrated about her situation. The assessment process also included brief socialization to the CBT model and a comprehensive risk assessment.
Risk
The referral information indicated that the neuropsychiatrist had previously assessed risk as very low. Risk was also assessed during the initial assessment sessions via questions about Becky’s mood, any thoughts of harming herself/others and questions pertaining to coping strategies and sources of support. Risk was also monitored as part of the weekly Clinical Outcomes in Routine Evaluation–Outcome Measure (CORE-OM). There was no evidence of any risk to Becky or others during the initial assessment or during the course of therapy. Becky’s mood and perception of coping was also assessed during the weekly check-in part of the session.
Measures
The following self-report measures were used to assess the impact of therapy.
CORE-OM was administered weekly to assess psychological distress, which is a common feature of FAS and psychogenic disorders (Jones et al., 2011). The CORE-OM is a 34-item self-report pan-theoretical measure (Royal College of Psychiatrists [RCP], 2016) that comprises a 5-point Likert-type scale to assess subjective (a) wellbeing, (b) psychological problems (including anxiety, depression, trauma, and physical problems), (c) functioning (including relationships), and (d) risk during the past week. It is considered to have good internal reliability: α > .70 (Barkham et al., 2005) to α = .95 (Evans et al., 2002) and has been validated in primary and secondary care settings (Lyne et al., 2006).
Session Rating Scale (SRS) administered during two assessment sessions and the first four intervention sessions to assess therapeutic alliance, as a positive alliance is widely considered to be one of the best predictors of outcome (Horvath, 2001). The SRS comprises four analog 10-cm scales, exploring (a) relationship, (b) goals, (c) approach, and (d) client’s perception of the session. The maximum score of 40 indicates the highest therapeutic alliance (Wheeler, 2017). The SRS is considered to be a valid and reliable measure of the therapeutic alliance (α = .88, Duncan et al., 2003).
6 Case Conceptualization
CBT was identified as the most suitable intervention as it has received empirical support for somatization (Allen & Woolfolk, 2010), where individuals have no medical explanation for persistent symptoms that significantly impact on daily functioning and wellbeing. Moreover, a meta-analysis of randomized controlled trials (RCTs) indicated that CBT is effective for psychogenic disorders and medically unexplained physical symptoms, with reductions in anxiety, low mood, and physical symptoms (Jing et al., 2019), all of which Becky was experiencing. CBT was deemed to be a good fit as it accommodated Becky’s preference for a mode of therapy that focused on the “here and now,” and met her request for an intervention to help her make sense of her difficulties and a feeling of stuckness. CBT also aligned with the therapist’s skillset. Furthermore, it was believed that a CBT case conceptualization would enable Becky to understand how her thoughts, feelings, bodily sensations, and behavior interrelate with one another (as shown in Figure 1).
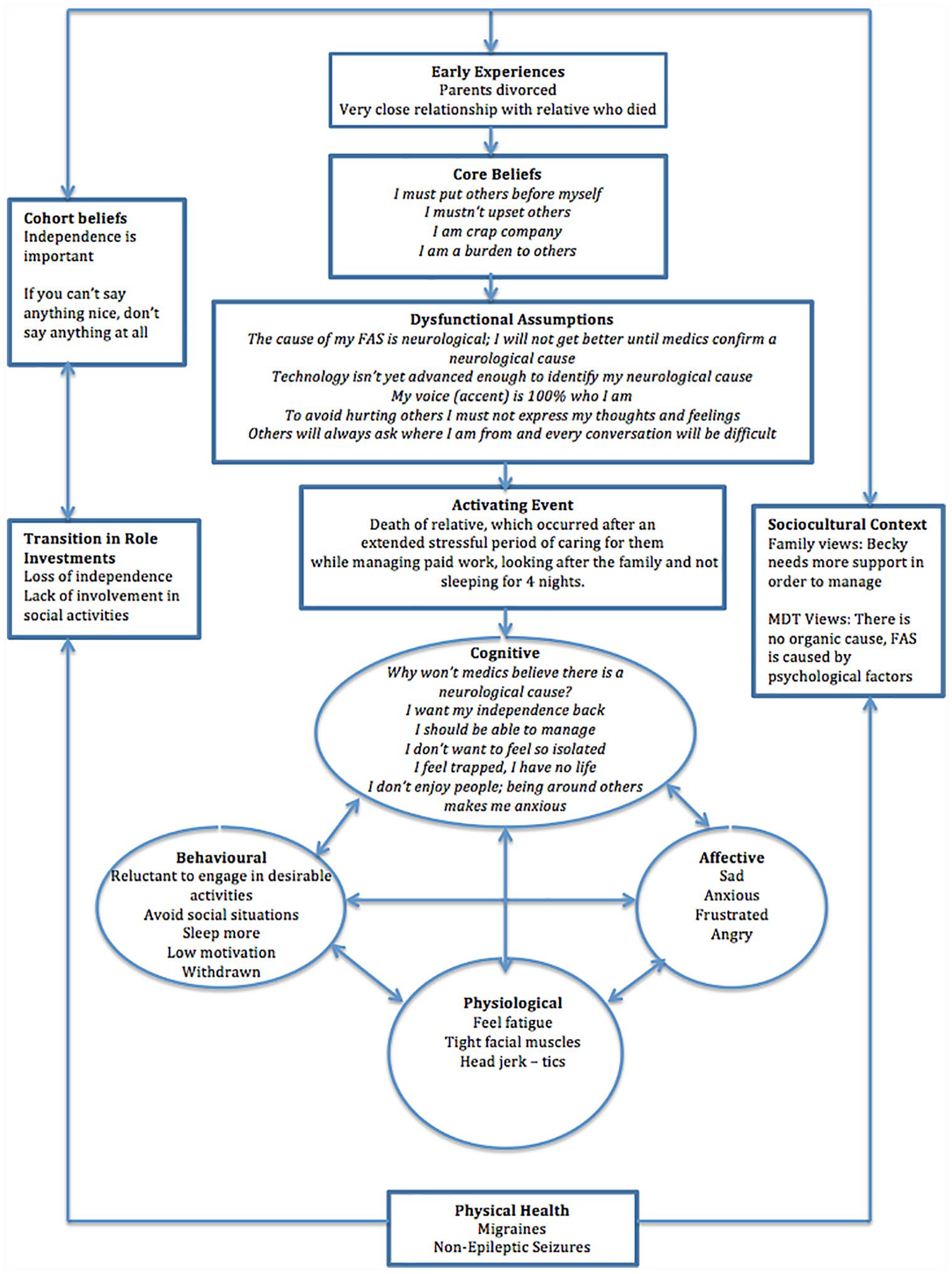
Diagram of longitudinal formulation.
In the absence of any empirically based cognitive behavioral models for FAS, a longitudinal formulation was developed through collaborative discussion to identify idiosyncratic aspects of Becky’s presentation (Manceil et al., 2012). The longitudinal formulation was based on Laidlaw et al.’s (2004) adapted model of Beck et al.’s (1979) longitudinal formulation, to identify (a) Becky’s core beliefs (e.g., “I am a burden to others” and ‘I mustn’t upset others’), (b) her dysfunctional assumptions (e.g., “to avoid hurting others I must not express my thoughts and feelings”), (c) the activating event (i.e., the death of her relative), (d) physical health (i.e., migraines and non-epileptic seizures), and (e) cognitions, feelings and behavior (Figure 1). Although Laidlaw et al. (2004) originally developed their conceptual CBT framework for work with older adults, Becky’s assessment identified that her problems did not exist in isolation. Thus, attending to (f) the socio-cultural context. For example, family beliefs that Becky required more support, and multidisciplinary team [MDT] views that there is no neurological cause. This was considered to be important as social interaction plays a critical role in the development of cognition (Vygotsky, 1978). The importance of gaining and maintaining independence became apparent through Becky’s assessment, which linked to (g) wider cohort beliefs and (h) transition in role investments.
Laidlaw et al.’s (2004) adapted model was believed to be the most appropriate framework. It recognized Becky’s early experiences, including parental divorce and the very close relationship with her deceased relative. In addition, it considered the contribution of these early experiences to Becky’s core beliefs and the subsequent development of dysfunctional assumptions. Thus, evidencing the link between how such beliefs/assumptions can be activated following a critical incident (Fenn & Byrne, 2013), such as the death of Becky’s close relative. The longitudinal formulation helped to maintain the focus on Becky’s current problems and collaboratively agree on goals (Johnstone & Dallos, 2013). This was important to Becky, who wanted to focus on the present and not “dwell on early experiences.” Becky’s formulation was modified as new information was shared in subsequent therapy sessions (Kuyken et al., 2011). This helped Becky to understand the critical role of her underlying beliefs in the interpretation of her current situation. Laidlaw et al.’s (2004) comprehensive framework was helpful in making sense of the “causes, precipitants and maintaining influences” (Eels, 2010, p. 4) of Becky’s main difficulties. However, it failed to fully account for the maintenance of Becky’s aphonia. Charlesworth and Reichelt (2004) recommend that selected mini-formulations can be of benefit when working with family members. Thus, an additional “vicious flower” formulation was collaboratively developed with Becky and Tom. This identified negative feedback loops (Salkovskis et al., 2003). These loops highlighted the strategies that Becky was using to manage her aphonia that had unintentionally become a part of maintaining the problem (Figure 2). This process of formulation fostered collaborative work and enhanced meaning, hope, and agency (British Psychological Society [BPS], 2011).
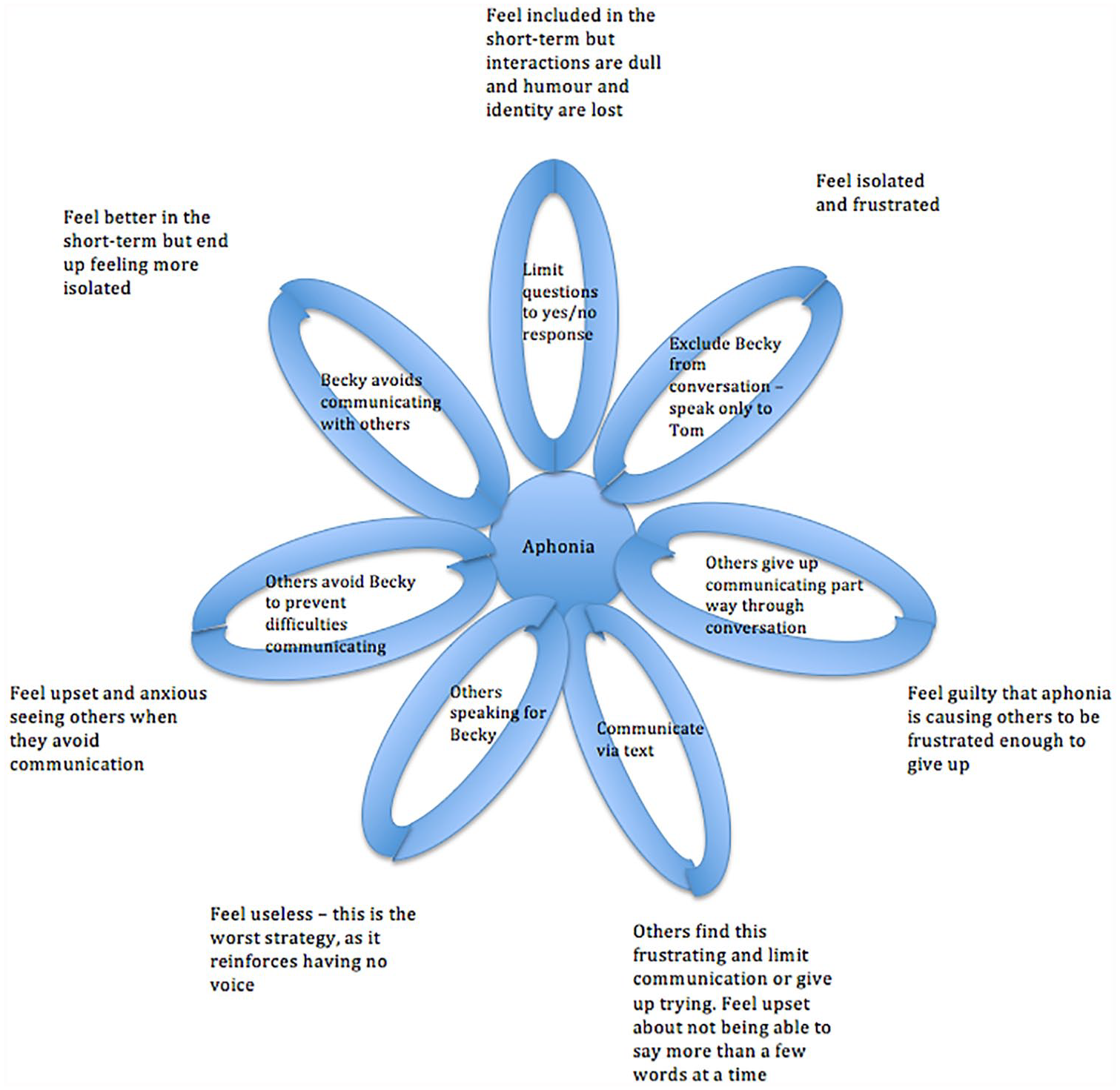
Diagram of vicious flower of strategies used to manage aphonia.
Hypotheses
It was hypothesized that Becky’s dysfunctional assumptions helped to maintain an external locus of control (Rotter, 1990), with the aphonia being maintained by dysfunctional coping strategies that kept her feeling stuck, voiceless, helpless, and unable to manage. It was further hypothesized that CBT treatment focusing on the reappraisal of dysfunctional assumptions and beliefs would help Becky to develop a greater internal locus of control and, subsequently, improve her confidence, mood, and ability to communicate better with others (Ahmad & Zadeh, 2013).
7 Course of Treatment and Assessment of Progress
Becky engaged in 14 1-hr CBT treatment sessions. In the absence of a CBT protocol for FAS, a CBT approach was used to collaboratively map out how Becky’s problems were working. The intervention was informed by the psychological principles and processes (BPS, 2011) identified in Becky’s longitudinal formulation (e.g., scaling beliefs, identifying evidence for and against a neurological cause of FAS, and behavioral experiments to engender greater insight for Tom into life with FAS and aphonia). Following a review of the formulation in Session 4, the vicious flower formulation informed problem-solving, reframing, and cognitive restructuring interventions (Clark, 2014). Further stress management, activity scheduling, narrative development, and self-compassion practice were informed by Becky’s formulation, as outlined below. Homework was also set at every session and served to help Becky and Tom practice and consolidate the skills learned in therapy session (Freeman, 2007). Table 1 provides an overview of the content of each session.
Overview of CBT for FAS Intervention.
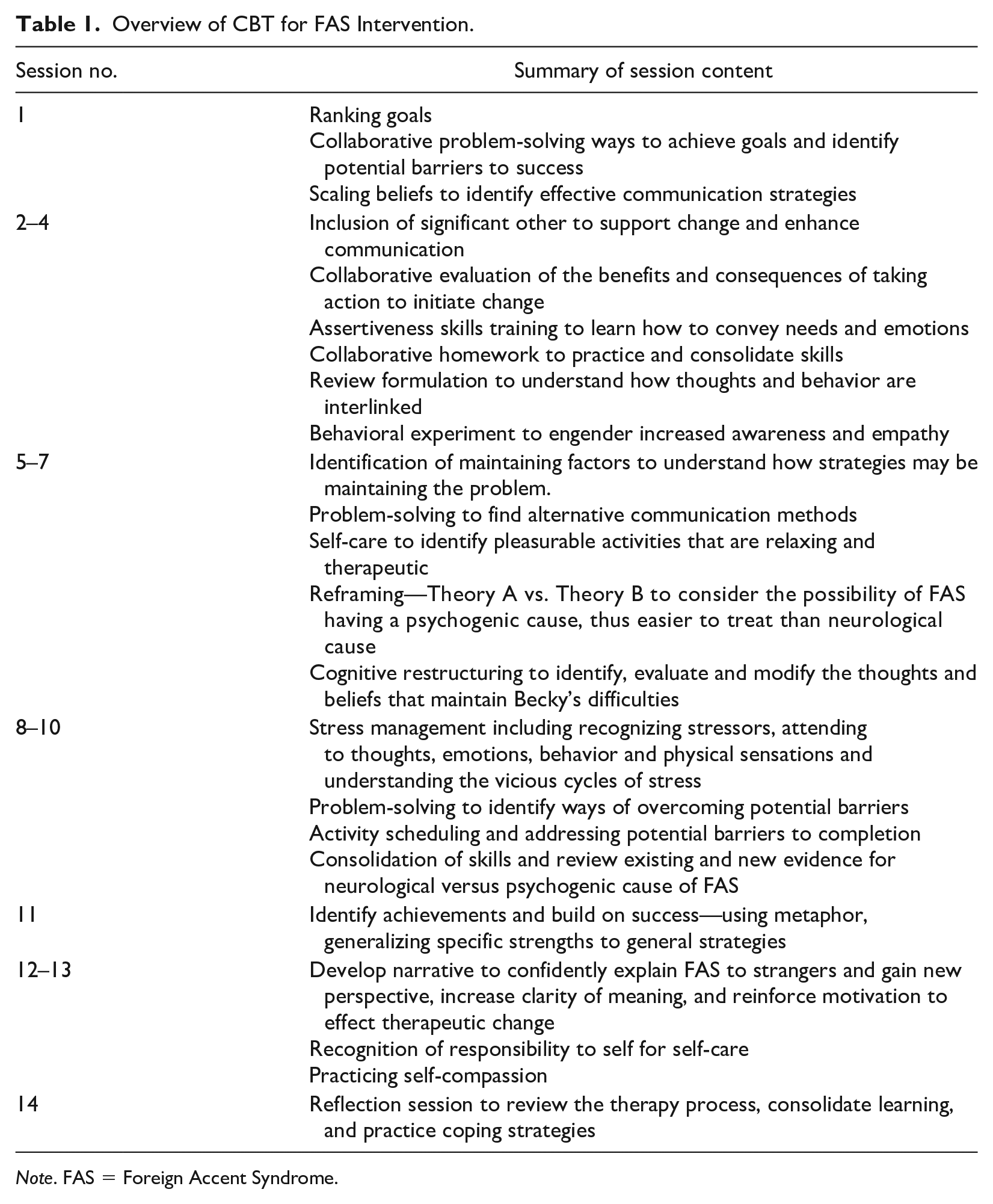
Note. FAS = Foreign Accent Syndrome.
Becky’s psychological distresses, as measured by CORE-OM simple scores, ranged from 11 to 19 during the three assessment sessions and increased to 20, 22, and 25, respectively, during the course of treatment. These increased scores coincided with particularly stressful life events, including a health scare (treatment Session 4) and a traumatic incident with a family member (treatment Session 11, as illustrated in Figure 3). There is a notable decrease in reported distress following each peak in weeks 7 and 14 (scores reducing by 5 and 20 points, respectively). When assessing the CORE-OM sub-scales (Wellbeing, Problem, Functioning, and Risk), there were notable fluctuations throughout the course of therapy (as depicted in Figure 4). In the final treatment sessions, Becky’s CORE-OM simple score reduced to 4, indicating a 71% reduction in psychological distress compared with baseline scores. This also demonstrated a statistically reliable change (CORE Partnership, 2007). Becky demonstrated significant improvements in her functioning and wellbeing, as she reached the clinical cutoff (simple scores <10), with this change being maintained during the final three sessions.
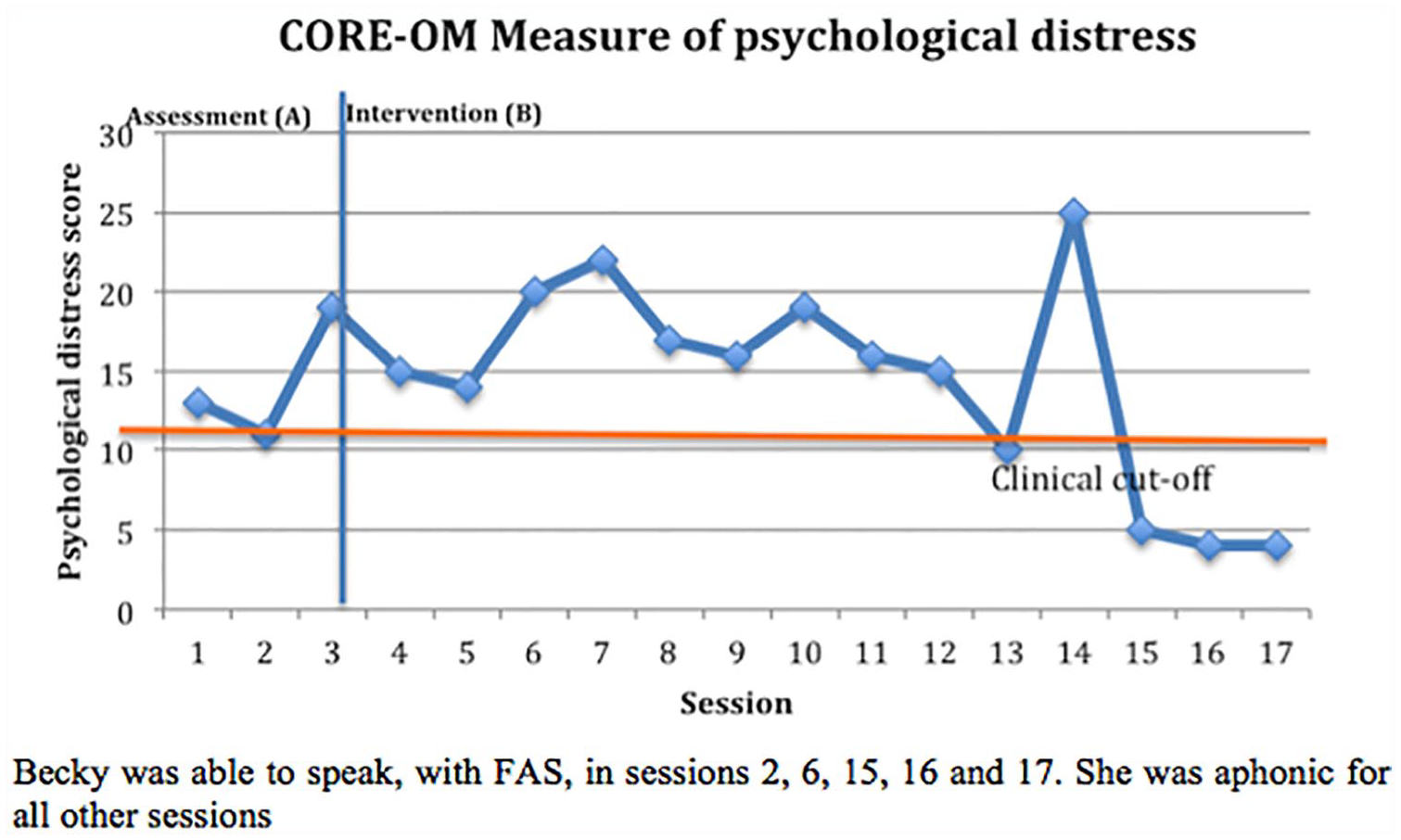
Graph of Becky’s psychological distress as measured by CORE-OM Simple Score.
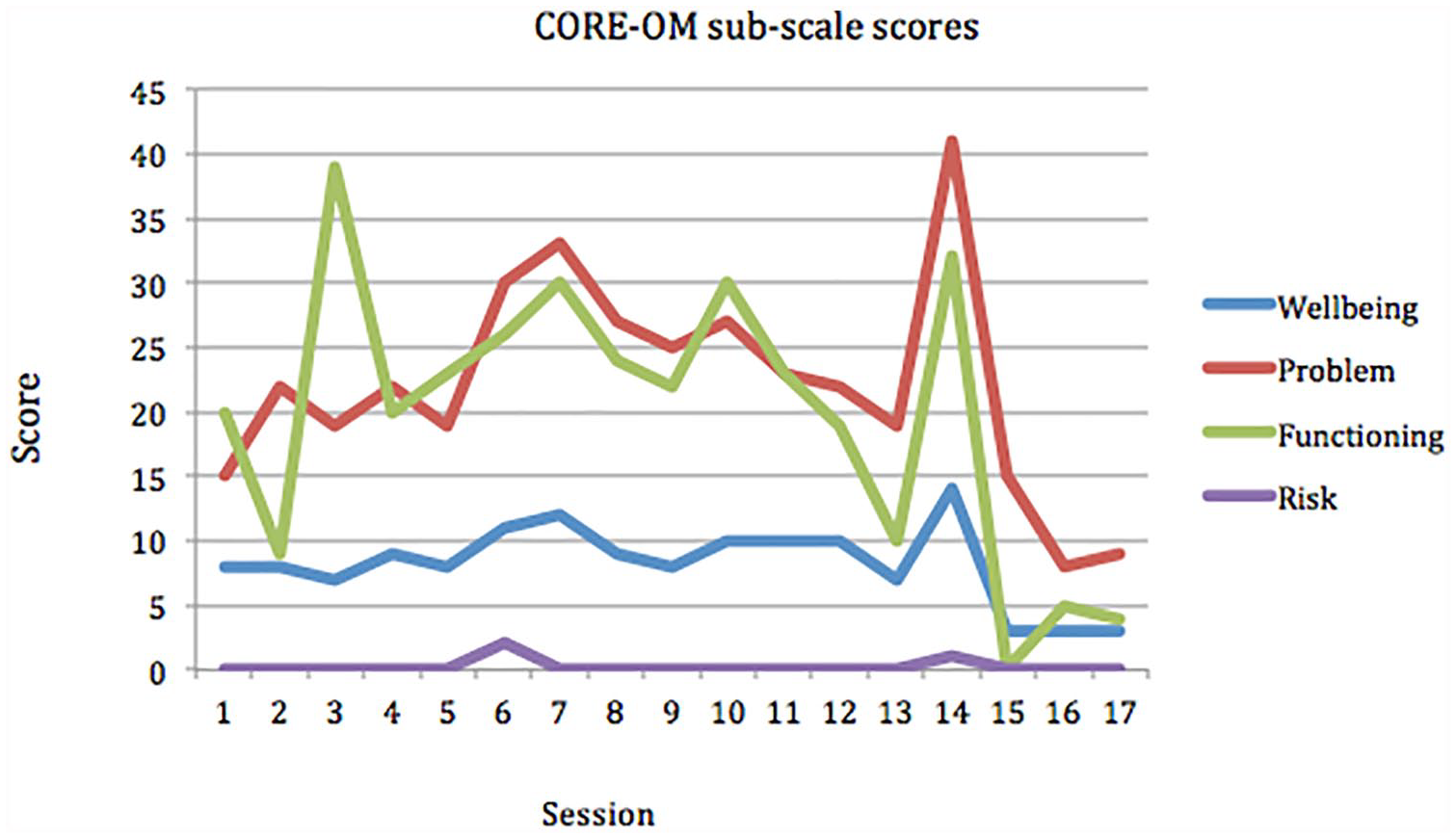
Graph of Becky’s Wellbeing, Problem, Functioning, Risk, and Total CORE-OM scores over time.
Maximum session rating scores (SRS = 10) were given for all aspects of the SRS therapeutic alliance measure (Johnson et al., 2000) in the first four treatment sessions, with the exception of goals (i.e., “we talked about what I wanted to”) for treatment Session 1, when Becky scored 9/10, explaining that she marked lower because she “‘couldn’t physically talk” (see Figure 5).
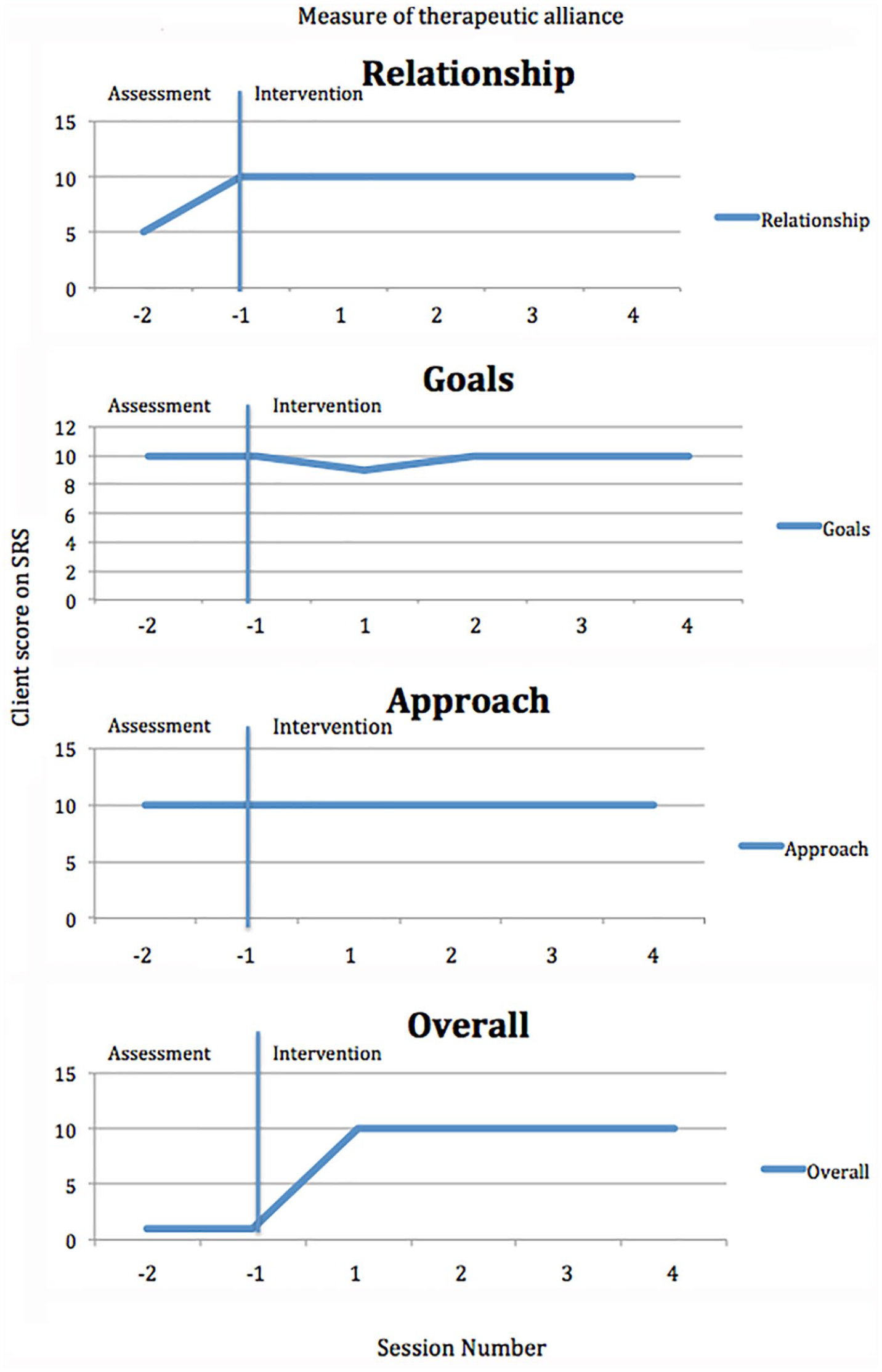
Graph of Becky’s ratings of the therapeutic alliance during two assessment sessions and four intervention sessions.
8 Complicating Factors
The primary complicating factor in this case was communication difficulties during periods of aphonia. In response to this, a mix of creative methods was employed, including drawing/doodling, using an iPad, inviting Tom to sessions, gesturing, and using nonverbal communication to give Becky a voice when she was not physically able to talk. It also required the therapist to consistently check that she had understood what Becky was saying, which Becky was able to confirm.
In relation to the outcome measure used in this case, baseline measures of psychological distress (CORE-OM) were taken at the start of the first three assessment sessions as resource limitations prevented the collection of data prior to assessment sessions. It is possible that these scores may have been impacted by Becky’s attendance at the mental health service. In addition, brief socialization to CBT took place during the assessment period, which coincides with an increase in the third baseline measure. It is possible that an increased awareness of the CBT model conflicted with Becky’s strong initial beliefs regarding her problems having a neurological basis (Blumstein & Kurowski, 2006). To ensure a stable baseline, it would have been optimal to start the collection of outcome measures prior to the assessment sessions.
With regard to the selection of outcome measures for FAS, the CORE-OM (RCP, 2016) was used in this case, as it was routinely used in the psychological therapies service. In addition, to the CORE-OM a self-report measure of depression (i.e., PHQ-9; Kroenke et al., 2001) and anxiety (i.e., GAD-7; Spitzer et al., 2006) would have been useful for monitoring and managing mood and anxiety related to FAS. Moreover, idiosyncratic measures such as conviction belief ratings would have been useful, particularly as Becky initially saw no utility in psychological input, as she did not believe there was a psychogenic cause.
9 Access and Barriers to Care
In this case, access to care was facilitated by the service having a trainee clinical psychologist on placement within the team. Instead of waiting an extended period to access psychological support from a qualified clinical psychologist, Becky was offered the option of a reduced wait if she accepted support from a trainee clinical psychologist. This has implications for other services not affiliated with training institutions. It is not known whether this resulted in other barriers to care but therapeutic alliance did not appear to be impacted by the comparatively limited experience of the trainee clinical psychologist.
Furthermore, neuropsychological testing was not considered and therefore not undertaken in this case. This could be a potential barrier to care and, in hindsight, neuropsychological testing would have been beneficial. Research indicates that individuals with psychogenic disorders exhibit decreased neurocognitive abilities in the domains of attention, memory, information processing, executive functioning, and language (de Vrogue et al., 2020). Given that CBT requires the use of these abilities, the effectiveness of treatment may be impacted if clients experience impairments in any domain. Without neuropsychological testing, it was not known whether Becky experienced any neurocognitive difficulties that would have required adaptations to therapy or indicated the need for an alternative therapeutic approach. As de Vrogue et al. (2020) assert, the evidence base for third-wave therapies, including mindfulness, is growing and may better meet the needs of individuals with psychogenic disorders.
Another potential barrier to care could have arisen when a break in care resulted from a period of staff illness, which occurred between Sessions 14 and 15. However, the break in therapy appeared to have a therapeutic benefit as it permitted space for Becky to autonomously practice her newly acquired communication and assertiveness skills in addition to self-care and coping strategies during this time. Consequently, her voice returned for the remainder of the course of therapy.
10 Follow-Up
Follow-up measures were not taken as both the clinician and the clinical supervisor left the service shortly after Becky completed treatment. It is therefore not possible to report on the longer-term maintenance of gains. Follow-up data would have been beneficial in establishing the stability of change and strengthening study validity (von Allmen et al., 2015).
11 Treatment Implications of the Case
This case study suggests that a formulation-driven CBT approach was effective in reducing self-reported levels of distress from “moderate-severe” to sub-clinical levels (Mellor-Clark, 2007). This improvement was evident in the final three treatment sessions, although in the absence of follow-up data, it is not clear whether these results are representative of longer-term improvements (von Allmen et al., 2015). Prior to a clinically significant reduction in distress, Becky’s scores consistently fluctuated within the moderate–severe range, indicating relatively persistent levels of psychological distress as Becky navigated family difficulties, an ongoing sense of “stuckness” and dissonance between working psychologically while maintaining a firm belief in a neurological cause (Ashgar & Whitty, 2020). Research has shown that unanticipated and undesirable events exert significant effects on levels of distress (Gielkens et al., 2018). It is, therefore, not surprising that patterns of distress mirrored difficult life events.
Becky’s scores peaked following a health scare and traumatic experience but scores then dropped to below baseline after the traumatic experience. This occurred immediately after therapy work evaluating evidence for and against a neurological cause of FAS, activity scheduling to promote engagement with others, and an increase in exercise levels and stress management. Collectively, these aspects of CBT appear to be a mechanism of change (Teachman et al., 2014) and are clinically significant as the sub-clinical score was maintained for the following 2 weeks. Around this time, Becky reported improved mood as she connected with friends to commence exercise classes, spoke to the family member she felt was keeping her stuck, and consequently, felt like a “huge weight had been lifted,” thus accomplishing three goals identified in the assessment. In addition, the sub-clinical scores may have been maintained by the skills developed in the following sessions. For example: the development of a positive narrative [fourth goal] to confidently explain FAS to strangers without divulging the context of its traumatic onset (i.e., her relative’s death); increased focus on self-compassion; and new insight into self-care, which has been found to decrease distress and enhance wellbeing) (Slonim et al., 2015). Interestingly, Becky’s voice returned for the three final treatment sessions, although it is not clear whether distress reduction contributed to her speaking ability or vice versa. During this time, Becky made strides to reconnect with relatives and discuss parenting strategies to reduce conflict at home (i.e., fifth and sixth goals).
Further reductions in distress were observed after treatment sessions that focused on (a) reviewing the formulation to identify how thoughts and behaviors are interlinked, (b) behavioral experiments to engender empathy from family members (reported by McMillan & Lee, 2010 to be effective); (c) identifying cognitive and behavioral maintenance factors that were key in understanding Becky’s reported “stuckness,” (d) problem-solving different communication methods; (e) stress-management (advocated by Woolfolk & Allen, 2012); (f) use of metaphor, found by Shoushtari (2015) to be helpful in reducing depression; and (g) cognitive restructuring (as recommended by National Institute of Clinical Excellence [NICE], 2009). While Becky held firm beliefs regarding a neurological cause of her difficulties, the introduction of reframing (e.g., Theory A vs. Theory B, (Salkovskis, 1996) appeared to be central in initiating change. Further research on the efficacy of reframing and cognitive restructuring in CBT treatment for FAS would therefore be worthwhile.
While it is encouraging that pre-post distress scores decreased, it is not clear what role the therapeutic alliance played in this. Working alliance is considered to be a strong predictor of therapy outcomes (Falkenstrom et al., 2014), and according to Johnson et al.’s (2000) SRS measure of therapeutic alliance, it appeared that a positive therapeutic alliance was evident in the first four treatment sessions. Although Becky demonstrated the ability to question the therapist and report when things were challenging for her, the SRS results were interpreted with potential social desirability effects in mind. However, as Reese et al. (2013) found, SRS alliance scores were not correlated with a measure of social desirability.
This case provides support for the work of Butcher et al. (2007) as Becky documented most of the etiological factors identified in their work, including stressful life events and anxiety, being female, having family and interpersonal difficulties, difficulties expressing views and emotions, a burden of responsibility, over-commitment, and helplessness. Although it is not possible to generalize beyond this single case, it may be worthwhile considering these etiological factors in future FAS research. To date, FAS has been overlooked and future research would benefit from considering CBT specific interventions for FAS. Although the debate regarding neurogenic, psychogenic, or mixed cause continues (Verhoeven & Mariën, 2010), it could be argued that the development of a CBT for FAS treatment model might help reduce strain on health services (Woolfolk & Allen, 2012). In addition, it may help service users to develop greater autonomy and internal locus of control, associated with improved wellbeing. In an area that remains under-explored, further research is certainly needed to identify the most robust intervention for FAS cases.
12 Recommendations to Clinicians and Students
When faced with referrals for unusual conditions like FAS, which do not yet have evidence-based guidelines for recommended treatment, clinicians and students would benefit from considering a formulation-driven approach. This approach facilitates the identification of idiosyncratic aspects of the service user’s presentation and permits the development of mutually agreed goals, which may differ from the goals identified by the referrer. Dissonance between the goals of the service user and those outlined by the referrer are important to think about clinically. It is possible that this intervention may have been less effective had the work been driven by either client goals or referral information alone. It is therefore recommended that an individualized formulation-driven CBT intervention that allows scope for revisiting and including an additional mini (vicious flower) formulation is essential to collaborative working and shaping of the intervention.
It is also recommended that clinicians are open to service users’ requests for significant others to attend therapy, to understand how family relationships recursively support dysfunctional interactions (Nelson et al., 1986). In this case, the use of core therapeutic skills and creative means of communication was essential in developing a positive therapeutic relationship, to ensure the service user felt heard, even when verbal communication was challenging for them.
Clinicians and students who encounter referrals for people with psychogenic FAS may benefit from identifying dysfunctional assumptions that may be maintaining an external locus of control (Rotter, 1990). As with this case, treatment that focused on the reappraisal of dysfunctional assumptions and beliefs helped with the development of a greater internal locus of control and resulted in improved confidence, mood, and increased ability to communicate with others (Ahmad & Zadeh, 2013). Use of cognitive restructuring and reframing, particularly Theory A/Theory B, was instrumental in shifting negative bias toward misinterpretations to more manageable interpretations (Salkovskis & Kirk, 1997, cited in Wilding & Milne, 2013). Cognitive restructuring was certainly a mechanism of change for Becky and is recommended to others working with people with FAS. As Mankiewicz (2019) denotes, recovery can be achieved when formulation-driven cognitive restructuring occurs in the context of a positive therapeutic relationship. As this remains an under-researched area, it is recommended that clinicians and students consider undertaking SCED studies in future and ensure that follow-up data are collected to assess the stability of change over time.
Footnotes
Acknowledgements
The author thanks Becky (pseudonym) for her consent to the publication of this article. Names used in the report have been changed to maintain confidentiality.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All procedures contributing to this work comply with the Ethical Principles of Psychologists and Code of Conduct as set out by the APA.