
Abstract
Childhood stress affects physical and mental health, making its proper assessment crucial. While several stress questionnaires for youth are available, their psychometric quality is questionable. Our aim was to develop a brief, age-appropriate questionnaire to measure current stress. Two-hundred thirty German children (6–17 years) completed the Stress Questionnaire for Children (SQC) and measures of stress symptoms, anxiety, depression, and quality of life via an online survey. The SQC consists of 17 items assessing current stress in school, social life, and leisure. An exploratory factor analysis indicated a three-factor solution (school stress, time stress, social stress) with a good model fit. The reliability of the total score (α = .90) and the subscales is good. Convergent validity was confirmed through correlations with stress-related symptoms, anxiety, depression, and quality of life. Total, school, and time stress increased with age, and girls endorsed higher stress than boys. Ratings on perceived difficulty, comprehensibility, and age-appropriateness indicated good acceptance. The SQC is a reliable and valid tool for assessing current stress in children and adolescents. It is child-friendly and suitable for a wide age range, making it suitable for research, clinical, and school settings. Further studies should confirm its factorial structure and its applicability across different cultural contexts.
Keywords
Stress in children and adolescents significantly affects health outcomes, increasing the risk of long-term physical and psychological effects on social, emotional, and cognitive development. Acute physical stress symptoms like headaches or insomnia can affect the immune, cardiovascular, and the digestive system if stress becomes chronic (Torsheim & Wold, 2001). Cognitive-emotional and behavioral stress symptoms are restlessness, altered social behavior, or nervousness (Seiffge-Krenke & Lohaus, 2007). Prolonged stress levels are a risk factor for mental and somatic disorders (Lindholdt et al., 2022).
Stress measurement is often based on Lazarus’ theoretical framework, including stressor exposure, cognitive appraisals, emotional stress reactions, and coping mechanisms (Lazarus & Folkman, 1984), each of which varies across the lifespan. Moreover, these components of stress require different foci for assessment. Combining them in a single questionnaire further complicates interpretation (Byrne et al., 2011). According to Byrne et al. (2007), measuring emotional stress reactions or cognitive appraisals is methodologically and conceptually challenging, as it is difficult to disentangle the causes and consequences of stress, with overlaps with certain dispositions, such as trait anxiety, or psychopathological symptoms, such as depressive symptoms. This explains why most questionnaires focus on stressor exposure.
Notably, the nature of perceived stressors differs between adults and children or adolescents. To capture age-related differences and enable broad applicability, it is essential to include the full age range from early reading age (approximately 6 years) to late adolescence (18 years). In children, aside from developmental requirements (e.g., school entry, puberty onset) and critical life events (e.g., parents’ divorce), everyday stressors particularly contribute to the perceived stress (Warghoff et al., 2020). Recurrent and difficult-to-avoid stressors are related to school, social, and leisure activities (Hemming, 2015).
School-related stressors are highly relevant for students of all age groups (Anda et al., 1997). These stressors include performance and time pressure, difficulties understanding the curriculum, excessive homework, test anxiety, and inappropriate teacher behavior (Brobeck et al., 2007; Seiffge-Krenke & Lohaus, 2007; Warghoff et al., 2020). Social networks can buffer stress, but they can also be a source of stress, particularly through conflicts or bullying (Hansson et al., 2020; Warghoff et al., 2020). Social exclusion and perceived lack of friendships increase stress and are associated with elevated cortisol levels (Peters et al., 2011). Recurrent family conflicts and high parental expectations contribute significantly to stress. Neglect and lack of attention from parents can disrupt a supportive family system and impact well-being (Lau, 2002). Leisure activities (e.g., sports or playing an instrument) can help balance academic and social stress, but they may also become stressors when high performance expectations, time demands, or limited access are present (Gerber & Pühse, 2008). Generally, the quantity rather than the type of leisure activities seems to affect stress levels (Brown et al., 2011). Importantly, individual stress is shaped by sociocultural factors, including experiences of racial or ethnic marginalization, discrimination, and trauma (Berger & Sarnyai, 2015; Carter, 2007; Everett et al., 2016). These contextual factors can significantly impact both the type and intensity of stressors experienced, especially in racially and culturally diverse youth populations (Priest et al., 2013).
Several stress measures for children and adolescents have been developed. Most focus on stressor exposure (e.g., Stress in Children Questionnaire; Osika et al., 2007). Stressor exposure is primarily assessed through stressor lists, where children indicate whether they have experienced specific situations (e.g., Children’s Daily Stress Inventory; Torres et al., 2009). A major concern with this approach arises from inferring stress burden without directly measuring it, relying on stressors from an adult perspective, and thus possibly omitting stress domains relevant for children (Byrne et al., 2007, 2011).
To address these concerns, the Children’s Stress Questionnaire (CSQ; Byrne et al., 2011) for primary school-age children and the Adolescent Stress Questionnaire (ASQ; Byrne et al., 2007) for adolescents ages 13 to 18 years were developed. The ASQ, based on findings from focus groups with adolescents, measures stressor exposure over the past year, with 58 items rated on a 5-point Likert scale from not at all stressful to very stressful. The CSQ measures stressor exposure and self-rated impact with 50 items on a 5-point Likert scale over the past year. Both questionnaires are reliable and validated, yet lengthy. As noted by the authors, the 1-year recall period could be viewed as a potential limitation. This led to the development of the Chronic Stress Questionnaire for Children and Adolescents, for ages 10 to 20 years (CSQ-CA; Bruin et al., 2018). However, the well-validated 17 items mainly focus on emotional responses to stressors (e.g., “I worry too much” or “I easily feel nervous”) over a 3-month period. They do not directly assess the perceived stress burden and do not allow for determining whether the reported emotional states are due to stressor exposure.
The aforementioned questionnaires focus on rather long time intervals, but the current stress level cannot be determined, which, however, is of interest in determining its direct impact on emotional and physical well-being. Moreover, especially in younger children, one can question the validity of recalled stress. White (2014) adapted the adult well-validated Perceived Stress Scale (PSS; Cohen et al., 1983) for children and adolescents ages 5 to 18 years and added new items. The PSS-Child measures stress over the past week (14 items) related to family/peers, school, time pressure, and emotional responses (e.g., anger, lack of happiness). The response is given using a Likert scale with piles of colored balls representing the amount of stress. Discriminant validity comparing small samples of healthy children and children with anxiety disorders was shown (White, 2014). However, a comprehensive psychometric evaluation is lacking.
Richartz et al. (2009) developed the German Scales for Chronic Stress in Childhood (CsiK), entailing nine subscales (e.g., school overload, social isolation, or dissatisfaction) to measure stress during the last week. The factorial structure has been preliminarily tested (Hemming, 2015), yet fit indices were not reported, and factor loadings and subscale reliability were not adequate. A more established measure is the Questionnaire for Stress and Stress Coping in Children (SSKJ 3-8) by Lohaus et al. (2006), which measures stress vulnerability, coping skills, and stress symptoms in children ages 7 to 16 years. However, the stress vulnerability scale measures anticipated stress in hypothetical stress situations and not their actual occurrence.
We developed the Stress Questionnaire for Children (SQC) with the aim to measure current stress levels across a broad age range from reading age to late adolescence using a minimal number of items addressing child-relevant areas of stress. The present study reports its psychometric evaluation in a large sample of healthy children ages 6 to 17 years. In addition to its structural properties, the SQC was validated by testing the relationship with depressiveness, anxiety, and quality of life. We also tested age and gender differences. Importantly, we also assessed children’s acceptance of the SQC.
Method
Participants
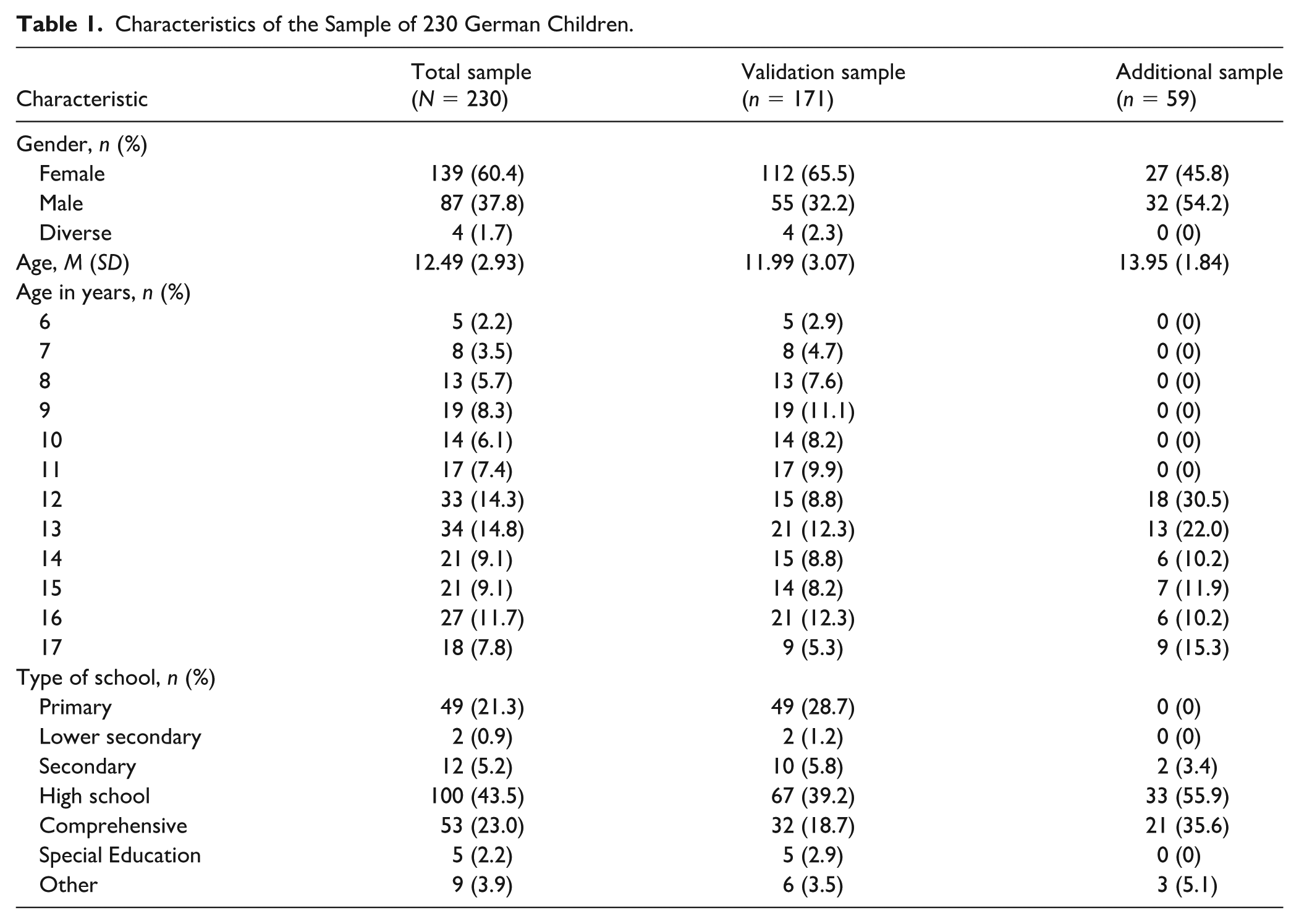
The sample consisted of 230 children and adolescents ages 6 to 17 years (M = 12.49 ± 2.93), of which 139 were females (60.4%, see Table 1). Notably, the age distribution was slightly negatively skewed (Sk = −0.30, SE = 0.16), with very few participants ages 6 and 7 years. Yet, they were included in the analysis for a preliminary assessment of feasibility in this age group. Inclusion criteria were fluency in German language and no current mental or physical illness as reported by parents in the informed consent form. Since no clinical screening was conducted to reduce barriers to participation, parents were explicitly informed during recruitment that only healthy children without diagnosed or suspected conditions were eligible to participate. Informed consent was obtained by both parents and children prior to participation.
Characteristics of the Sample of 230 German Children.
Participants were recruited from two samples: A larger subsample (“validation sample,” n = 171) completed all questionnaires in an online survey package. In April 2021, parent recruitment was initiated via email at a German university, distributing flyers in local schools and recreational facilities, and social media. As incentive, gift vouchers (10 Euro) were raffled. Due to slow online recruitment during COVID and the need to reach an adequate sample size for validation purposes, a convenience sample (“additional sample,” n = 59) was included. These adolescents had already completed the same version of the SQC under comparable conditions as part of an experimental laboratory study on placebo effects (March 2023–November 2023; for a detailed description, see “Procedure”-section). The SQC was assessed prior to the experiment in order to evaluate the impact of stress on responding. The overall sample size was estimated a priori, based on empirical guidelines for minimum sample size for factor analyses (Hair et al., 2019). The study was conducted in accordance with the Declaration of Helsinki and approved by the local ethics committee (#2021-0007).
Development of the German SQC
Initial Item Development and Pilot Study
The SQC was developed by first translating the English PSS-C (White, 2014) into German using a forward-backward translation method within our research group. As the original PSS-C did not sufficiently cover common childhood stressors (e.g., school- or social-related stressors), we added 10 items (e.g., “In the last week, how often did you feel like you couldn’t keep up in class?” or “In the last week, how often was the homework too much for you?”). These items were developed from literature reviews and informal consultations with experts in child development and colleagues. This initial item pool, consisting of the translated PSS-C and the 10 newly developed items, was tested in a preliminary pilot study.
A convenience sample of 40 healthy children (7–14 years, M = 10.63 ± 2.25, 62.5% female) was recruited at a local after-school homework support program. No major exclusion criteria were applied, apart from sufficient German language proficiency. Children completed the initial questionnaire anonymously in an online survey, alongside the Multidimensional Anxiety Inventory for Children and Adolescents (MAI-KJ; Hock et al., 2020) to assess depression and anxiety for construct validity. In addition, 10-minute qualitative interviews were conducted to explore their understanding of stress and identify stressors (“What does stress mean to you?” “What makes you feel stressed?” “What are the three things that stress you the most? [Rank 1–3]” “How do you feel when you’re stressed?” “What helps you when you’re stressed?”) and answers were recorded by the interviewer. €10 vouchers were raffled as compensation. Results indicated poor reliability (Cronbach’s alpha = .62) and low discriminant validity; therefore, several changes were made.
Development of the Final Version of the SQC
The original (piloted) set of 23 items was shortened by the removal of 13 items. Exclusion criteria were item-total correlations below .30 (six items), strong overlap with symptoms of anxiety/depression (three items), or other emotional states rather than stressors (two items), and poor content validity due to wording (two items). The remaining 10 items were either retained in their original form or revised to enhance clarity and readability for children. To better incorporate children’s perspectives, new items were developed based on the qualitative interview data. The most often mentioned stressors (school, social environment, and leisure) were consistent with findings from a more in-depth literature review. Based on this, seven new items were generated to reflect these three stressor domains (e.g., “In the last week, how often did you have to rush to finish something?”). These revisions resulted in the final questionnaire version to be evaluated, which contained 17 items assessing current stress in different domains like school, social environment, and leisure. Children indicate the frequency of stressors during the preceding week on a 4-point Likert scale (0 = never, 1 = rarely, 2 = sometimes, and 3 = always). We developed a child-friendly visual response format using a calendar icon featuring varying numbers of crosses to illustrate stressor frequency in the past week.
Measures
Anxiety and Depression
The MAI-KJ (Hock et al., 2020) is a screening instrument for anxiety and depression in children ages 8 to 19 years. We used the general module containing 27 items to be answered on a 4-point Likert scale (1 = almost never to 4 = almost always). Dispositional anxiety is assessed by items representing agitation and concern (“I am afraid of making mistakes”) and depression by items of sadness and joy (“I feel like crying”). The MAI-KJ has good convergent construct validity (Hock et al., 2020). Both subscales have shown to be temporally stable (rtt = .61–.76 for 2–4 weeks). In our subsample of 171 children completing the online survey, reliability was excellent for both subscales (α = .91–.95).
Stress Symptoms
The Stress and Stress Coping Questionnaire for Children and Adolescents (SSKJ 3-8; Lohaus et al., 2006) evaluates stress vulnerability, stress coping, and physical and psychological stress symptoms in children ages 7 to 16 years through a total of 84 items (Eschenbeck et al., 2006). We used the Stress Symptoms Scale, measuring the frequency in the last week on a 3-point Likert scale (0 = never to 2 = several times). The Psychological Stress Symptoms Scale consists of 12 items describing stress-related emotions such as irritability and nervousness. Physical stress symptoms (e.g., headache) are assessed through six items. The dimensional structure and construct validity were confirmed through extensive psychometric evaluation (Eschenbeck et al., 2006). Internal consistency of both subscales within this sample was high (α = .78–.90).
Quality of Life
The Children’s Quality of Life Questionnaire (KINDL; Ravens-Sieberer & Bullinger, 1998) is a well-established German questionnaire assessing health-related quality of life in children and adolescents. For the current study, the Kid-KINDL was utilized as a self-report version for children ages 7 to 13 years. This questionnaire consists of six subscales (Physical Well-Being, Mental Well-Being, Self-Esteem, Family, Friends, School) with four items per scale. In the present study, Self-Esteem (e.g., “In the past week, I was proud of myself”), Family (“I got along well with my parents”), Friends (“I played with friends”), and School (“I did well on my school assignments”) scales were used. Children indicate the frequency of experienced situations in the past week on a 5-point Likert scale from never to always. Reliability in this sample was high (α = .73–.84).
Additional Measures
Subjective Global Stress Level
This was addressed in the first question of the survey (“How much stress did you experience in the last week?”). Using an 11-point numerical rating scale (NRS), participants indicated the average level of stress they experienced over the past week (0 = never stressed, 10 = always stressed).
Stress Due to COVID-19 Restrictions
As data collection began during the COVID-19 pandemic (04/2021), participants were asked to rate how much they felt affected by the concurrent restrictions due to the pandemic (“How bad is it for you that many things are different now because of COVID-19 compared to before?”), assessed on an 11-point NRS (0 = not bad at all, 10 = very bad).
Acceptance
To assess the usability, participants rated the perceived difficulty (“How difficult did you find it to answer the questions?”), the comprehensibility of the items (“How well did you understand the questions?”), and the age-appropriateness (“How well did the questions fit your age?”) on an 11-point NRS (0 = not at all, 10 = very much). In addition, participants were invited to suggest improvements through an optional open-ended text field.
Procedure
Validation Sample
The subsample of 171 children recruited specifically for this validation study completed the questionnaires anonymously in an online survey, administered using Unipark (Tivian XI GmbH, Cologne). Parents received the survey link via email. Upon detailed participant information and their consent, parents were requested to allow their children to complete the survey independently. Once handed over to the children, the study was explained again appropriately for their age. Participants had the option to withdraw from the survey at any time. First, demographic data were obtained. Next, the subjective global stress level was asked using the NRS, then the SQC was presented, followed by the other measures. Finally, participants indicated their subjective burden due to the COVID-19 pandemic and were asked whether they completed the survey independently or with assistance. After completing the survey, participants could enter a voucher lottery, and winners were notified following data collection.
Additional Sample
The additional sample of 59 adolescents completed the SQC also using Unipark (Tivian XI GmbH, Cologne) as part of a questionnaire package for a laboratory experiment on placebo effects in adolescents between the ages of 12 and 17 years. The SQC was answered at home before the onsite participation in the experiment and therefore unaffected by the subsequent intervention. Participants first provided demographic information, then completed the SQC, and subsequently answered additional experiment-related questionnaires. They received compensation for their participation after completing the laboratory experiment.
Data Analysis
To examine the dimensional structure, an exploratory factorial analysis (EFA) with oblimin rotation was conducted with the total sample of 230 after evaluating Bartlett’s sphericity test and the Kaiser–Meyer–Olkin (KMO) criterion for sample adequacy. To determine the number of extracted factors, we considered only eigenvalues > 1 and assessed goodness-of-fit indices, that is, root-mean-square error of approximation (RMSEA) < .08, comparative fit index (CFI) > .90, Tucker-Lewis index (TLI) > .90, and standard root-mean-square residual (SRMR) < .08 as suggested by Hu and Bentler (1999). Only items with factor loadings > .40 were retained.
Based on the EFA results, a total sum score and sum scores for each subscale (school, time, and social stress) were computed. Internal consistency (Cronbach’s alpha) was calculated for each subscale.
Convergent validity was assessed only in the subsample of 171 children, as the remaining 59 children from the laboratory experiment did not complete the same questionnaires. Correlations between SQC scores and the subjective global stress level (assessed via a Numerical Rating Scale [NRS], 0–10), COVID-19-related stress, and stress symptoms (SSKJ; Stress and Stress Coping Questionnaire for Children and Adolescents; Lohaus et al., 2006) were calculated. Associations between COVID-stress and the SQC are reported separately for participants directly affected by COVID-related restrictions (April 2021 to December 2022, n = 75) and those participating between January 2022 and early 2024 (n = 96). Furthermore, correlations between stress, anxiety, and depression (MAI-KJ; Multidimensional Anxiety Inventory for Children and Adolescents; Hock et al., 2020) and quality of life (KINDL; Children’s Quality of Life Questionnaire; Ravens-Sieberer & Bullinger, 1998) were calculated. To minimize Type-1 error, we employed a conservative significance level of p < .01.
Age and gender differences were analyzed using the total sample of N = 230. Age was assessed with Pearson correlations. In addition, the sample was divided into children ages 6 to 11 years (n = 76) and adolescents ages 12 to 17 years (n = 154), and differences in stress levels were analyzed using t-tests. Reliability and validity indicators were then calculated separately for both age groups. Gender differences between girls and boys were examined using independent t-tests, diverse individuals were excluded due to their extremely small number. Descriptive data on usability are reported regarding comprehensibility, difficulty, and age-appropriateness, each in relation to participants’ age for the subsample of 171.
Data and Code Availability
The data underlying this article are available in the Zenodo repository at https://doi.org/10.5281/zenodo.17159651.
Results
Exploratory Factor Analysis
Significant Bartlett’s sphericity test, χ2(136) = 1547.51, p < .001, a KMO value of .91, inspection of the correlation matrix, and anti-image-correlations of all variables indicated a good adequacy for factorial analysis. According to the Kaiser criterion (eigenvalue > 1), a three-factor solution seemed best, accounting for 54.6% of the variance. All items showed satisfactory factor loadings of at least .40 with no double factor loadings (see Table 2). Item discrimination was good (.42 < rit < .70). Goodness-of-fit indices showed a good fit of the model (RMSEA = .07, SRMR = .06, CFI = .92, TLI = .91).
Items and Factor Loadings of the Exploratory Factor Analysis.
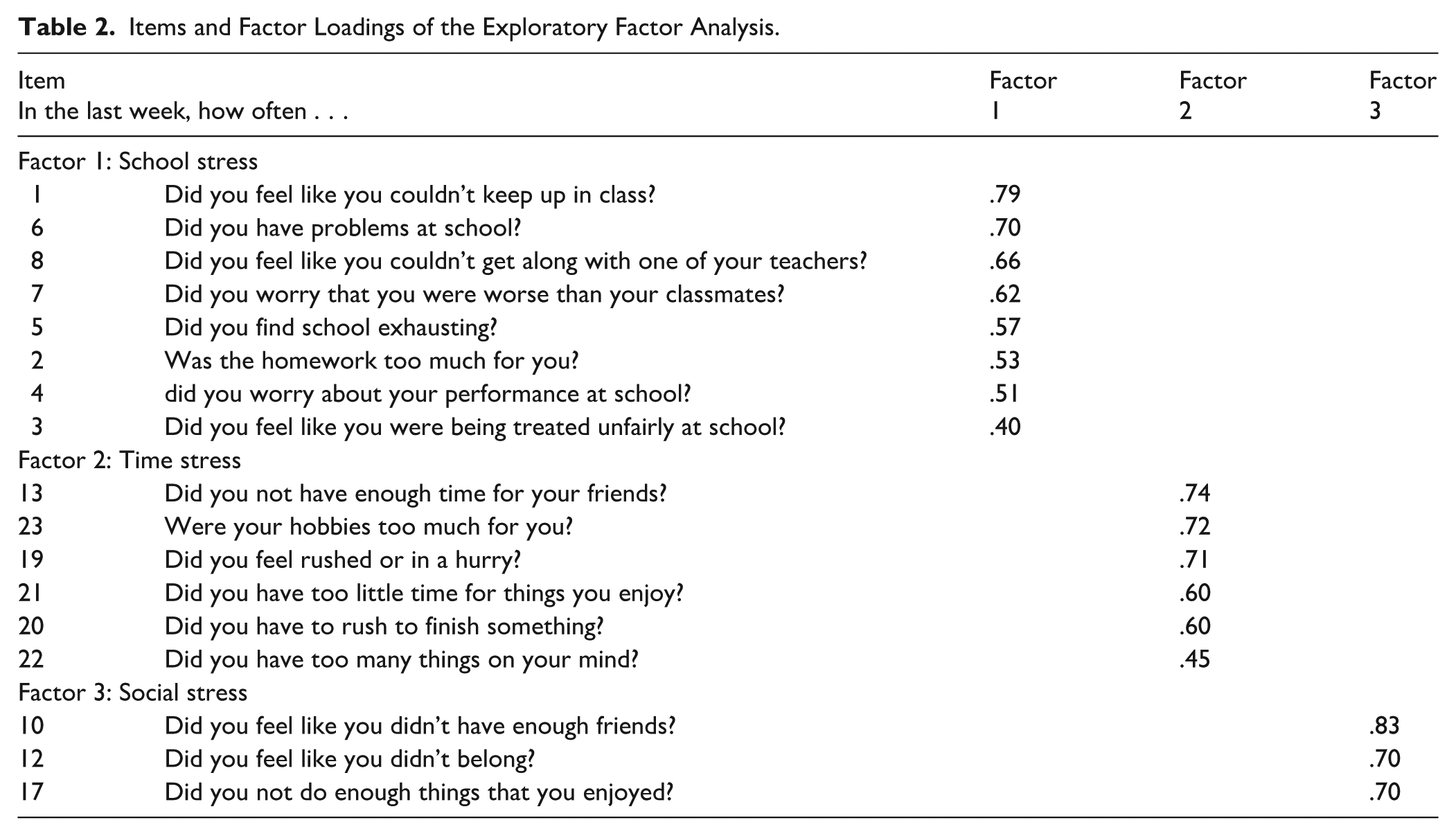
After inspection of the scree plot, a potential one-factor solution was tested as well, which explained 39.6% of variance. Item loadings ranged from .48 to .75. However, fit indices indicated a poorer fit to the data than the three-factor solution (see Table 3).
Fit Indices for the One-Factor and Three-Factor Models.
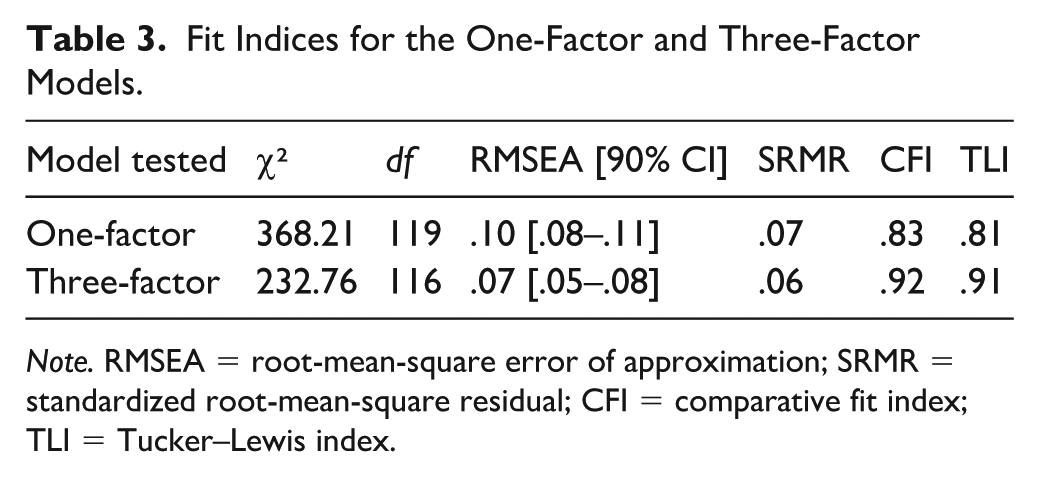
Note. RMSEA = root-mean-square error of approximation; SRMR = standardized root-mean-square residual; CFI = comparative fit index; TLI = Tucker–Lewis index.
Reliability
All subscales demonstrated good internal consistency (school stress: α = .85, time stress: α = .81, social stress: α = .73). Cronbach’s alpha for the total score was excellent (α = .90). As expected, subscales were significantly intercorrelated (r = .54–.66, ps < .001) and highly correlated with the total score (r = .75–.92, ps < .001; see Table 4).
Descriptive Statistics, Internal Consistency, and Correlations for the SQC Total and Subscale Scores.
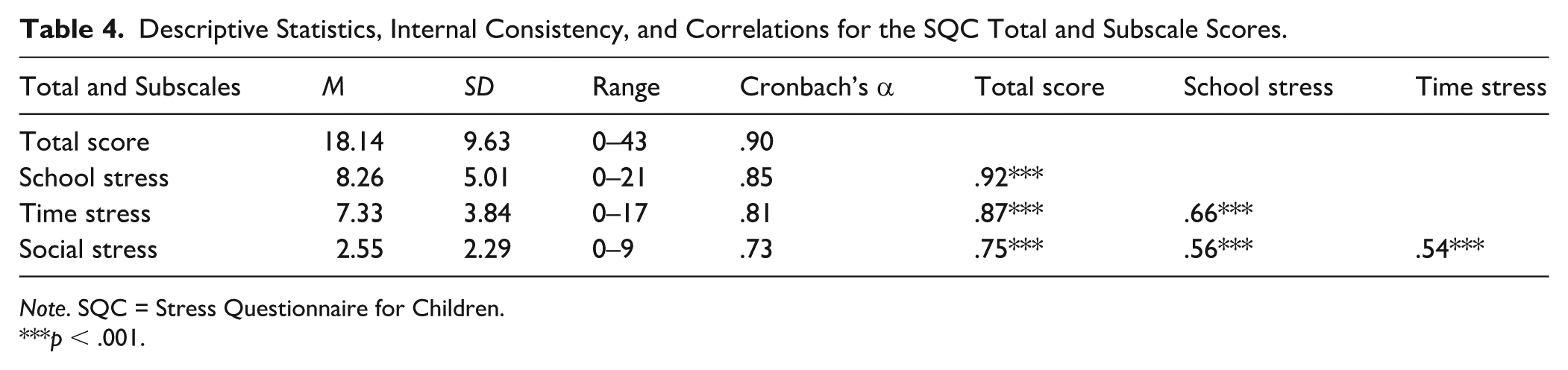
Note. SQC = Stress Questionnaire for Children.
p < .001.
Validity Analyses
Stress-Related Measures
Perceived stress and its subscales were highly correlated with the subjective global stress level (r = .50–.73, ps < .001; see Table 5). In participants directly affected by COVID-related restrictions, COVID-related stress was significantly correlated with total stress (r = .35, p = .002), school stress (r = .32, p = .006), social stress (r = .31, p = .008), and time stress (r = .30, p = .008). These associations were no longer evident in participants who participated from January 2022 onwards (total score: r = .12, p = .249; school stress: r = .17, p = .103; social stress r = .12, p = .249; time stress: r < −.01, p = .980). Perceived stress as measured by the SQC did not significantly differ between participants in those two collection periods, total stress: t(169) = −1.22, p = .223; school stress: t(169) = −1.17, p = .243; social stress: t(169) = −1.44, p = .151; time stress: t(169) = −0.70, p = .485.
Descriptive Statistics, Internal Consistency for Validation Measures, and Correlations with SQC Total and Subscale Scores.
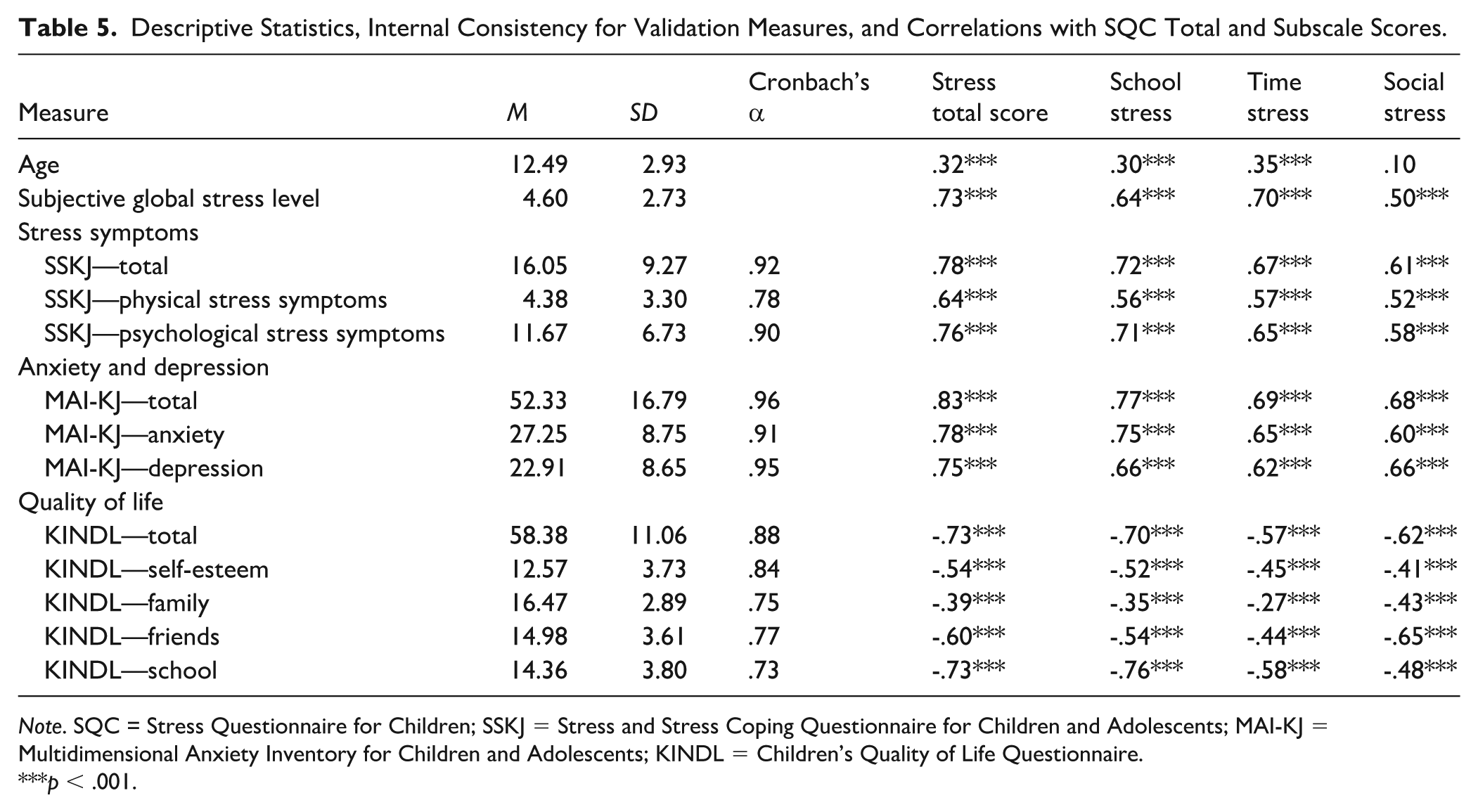
Note. SQC = Stress Questionnaire for Children; SSKJ = Stress and Stress Coping Questionnaire for Children and Adolescents; MAI-KJ = Multidimensional Anxiety Inventory for Children and Adolescents; KINDL = Children’s Quality of Life Questionnaire.
p < .001.
Stress symptoms as assessed with the SSKJ were significantly positively correlated with total stress (r = .78, p < .001) and each subscale (r = .61–.72, ps < .001). Both physical and psychological stress symptoms showed high positive correlations with the total stress score (r = .64–.76, ps < .001) as well as school stress (r = .56–.71, ps < .001), time stress (r = .57–.65, ps < .001), and social stress (r = .52–.58, ps < .001).
Anxiety, depression, and quality of life
Dispositional anxiety (r = .78, p < .001) and depressive symptoms (r = .75, p < .001) were significantly correlated to the SQC total score as well as with the SQC subscales (school stress: r = .66–.75; time stress: r = .62–.65; social stress: r =.60–.66; all ps < .001). Health-related quality of life (i.e., Self-Esteem, Family, Friends, and School) was negatively correlated with stress (r = −.27 to −.76; all ps < .001).
Age and Gender Effects
The level of stress (SQC total score) increased significantly with age (r = .32, p < .001). Similarly, school stress (r = .30, p < .001) and time stress (r = .35, p < .001) increased with age. Social stress was not significantly correlated with age (r = .10, p = .129). Adolescents ages 12 to 17 years (n = 154) reported significantly higher overall stress: t(228) = −3.37, p < .001; school stress: t(228) = −3.09, p = .002; and time stress: t(228) = −3.58, p < .001; compared to children ages 6 to 11 years (n = 76). However, social stress did not differ between the two age groups: t(228) = −1.39, p = .166. The reliability of the SQC was good to very good in both age groups (adolescents: overall stress α = .90, school stress α = .83, time stress α = .80, social stress α = .73; children: overall stress α = .90; school stress α = .87, time stress α = .81, social stress α = .72). Similarly, construct validity analyses were comparable across both age groups (see Table 6).
Validity Analyses for the SQC Total and Subscales for Children and Adolescents (12–17 years, n = 95) from the Validation Sample Who Completed the Online Survey.
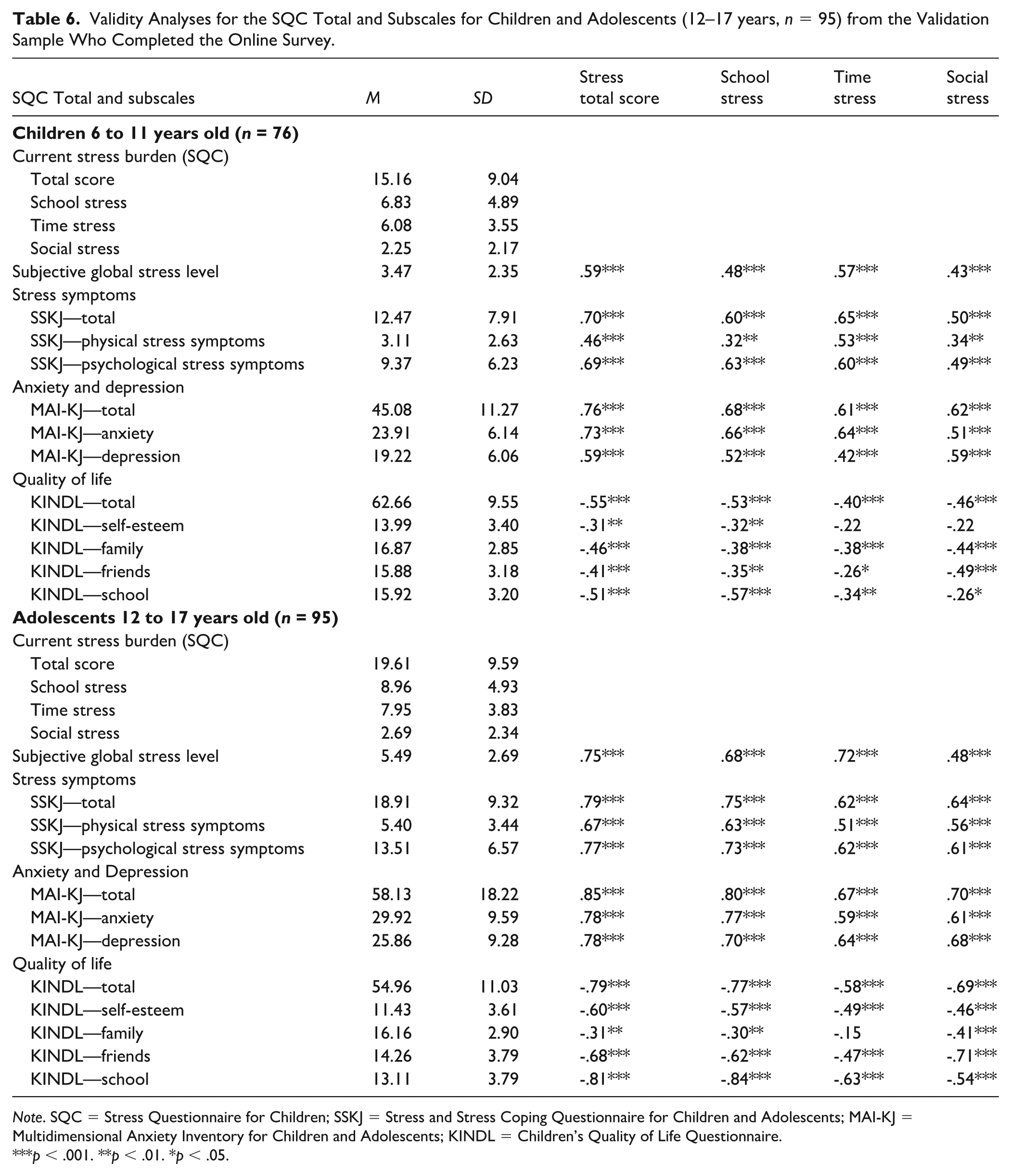
Note. SQC = Stress Questionnaire for Children; SSKJ = Stress and Stress Coping Questionnaire for Children and Adolescents; MAI-KJ = Multidimensional Anxiety Inventory for Children and Adolescents; KINDL = Children’s Quality of Life Questionnaire.
p < .001. **p < .01. *p < .05.
The total stress score was significantly higher in females than in males: t(224) = −3.16, p = .002, ∆ females–males = 4.01. Similarly, females reported significantly more school stress: t(224) = −2.06, p = .040, ∆ females–males = 1.39, time stress: t(224) = −3.26, p = .001, ∆ females–males = 1.66, and social stress: t(224) = −3.18, p = .002, ∆females–males = 0.97.
Usability
On the 0 to 10 NRS, mean perceived difficulty was low (M = 2.32 ± 2.15). Younger participants found the items more difficult (r = −.24, p = .021), especially the youngest participants (ages 6 and 7 years), who rated the difficulty as higher (6-year-olds: M = 5.75 ± 2.87; 7-year-olds: M = 3.00 ± 1.87) compared to older children (8–17 years: M = 2.13 ± 2.00). On average, comprehensibility was high (M = 8.57 ± 2.34), correlating positively with age (r = .20, p = .047). Comprehensibility was also significantly correlated with perceived age-appropriateness (r = .29, p = .004). On average, participants rated age-appropriateness as high (M = 7.28 ± 2.35), independent of age (r = .12, p = .229). However, the youngest children rated age-appropriateness lower (6-year-olds: M = 4.50 ± 4.12; 7-year-olds: M = 6.40 ± 3.91) than older children (8–17 years: M = 7.46 ± 2.09).
Discussion
In a psychometric evaluation of the newly developed stress measure for children (SQC) in 230 children ages 6 to 17 years, a three-dimensional factor structure was identified, showing good reliability for both the overall scale and the subscales (all α’s > .7). Convergent construct validity was confirmed through high correlations with established measures of depression (r = .62–.75), anxiety (r = .60–.78), and quality of life (r = −.27 to −.76). In addition, gender differences and age-related increases in stress levels were observed.
Existing instruments such as the CSQ (Byrne et al., 2011) or ASQ (Byrne et al., 2007) assess stress over extended periods (e.g., the past year) and primarily tap chronic or prolonged stress, which reflects current and retrospective stress (Bruin et al., 2018). Chronic stress reflects accumulated stress over a longer period of time and includes critical life events and everyday stressors (e.g., school-related stressors or stress from social conflicts, etc.). However, in childhood, stress levels often fluctuate due to rapidly changing developmental contexts, which can reduce the accuracy and validity of long-term recall. The SQC addresses this by assessing the current stress burden within the past week. Thus, the SQC allows to detect current stress and its fluctuations over time. It can be used to closely monitor such changes in stress or to determine developmental trajectories of stress. The SQC thus complements existing tools and addresses a gap in stress assessment for children and adolescents.
The three identified factors with an excellent fit, satisfactory item discrimination, and factor loadings were highly intercorrelated, as expected given the oblique method of factor rotation. The first factor (School Stress: eight items; 39.6% accounted variance) addresses typical school problems such as performance pressure, teacher interactions, and too much homework. Previous stress questionnaires such as the ASQ (Byrne et al., 2007) or the CSQ (Byrne et al., 2011) include different school-related subscales (e.g., stress of school performance or stress of teacher interaction). The SQC scale seems to integrate all these aspects. Although the SQC was designed to assess common stressors in school-age children, some items—particularly those addressing perceived unfair treatment (Item 3) or lack of belonging (Item 12)—may be particularly sensitive to differential stress levels among sociocultural groups, due to varying levels of exposure to exclusion, discrimination, or other stress-amplifying contextual factors. School belonging is shaped by ethnic identity (Heikamp et al., 2020; Janke et al., 2024), and experience of discrimination has been linked to elevated stress among ethnic minority youth (Berger & Sarnyai, 2015; Everett et al., 2016). Cultural differences in teacher–student relationships (Roorda et al., 2023), perceptions of teacher authority (Cortina et al., 2017), and systemic variations in instructional pace, academic demands, and support for low-performing students (Castejón & Zancajo, 2015) may further impact how school-related stress is perceived and reported. The SQC could be helpful to determine such differences in stress levels, given that the assessed domains of stress are broadly defined. The second factor (Time Stress: six items; 8.1% accounted variance) measures time pressure related to leisure activities, friendships, or other tasks. Time demands are an important source of stress both in adults and in youth (ASQ: Byrne et al., 2007; CSQ: Byrne et al., 2011; CsiK: Hemming, 2015). The third factor reflects Social Stressors (three items, 7.0% accounted variance) including aspects of social isolation, such as a lack of belonging to a peer group and a lack of positive activities. In light of the role of social media, such social stressors have become increasingly important (Shannon et al., 2022). Despite its brevity, the SQC covers key areas of stress in children and adolescents. Importantly, the factor structure and the intercorrelations between the subscales warrant the use of both the total score as well as the subscale scores.
The reliability of the overall scale and the subscales is very high or even excellent. The SQC reliability surpasses that of other stress questionnaires. Compared to other questionnaires, only the CSQ appears similarly reliable (α = .90; Byrne et al., 2011). No reliability scores are available for the PSS-C (White, 2014). The internal consistency of our 17-item questionnaire is notable when considering that children’s rating scales typically have lower reliability than those for adults (Lohaus, 1989), and other stress questionnaires with similar reliability have more than twice as many items.
Convergent validity of the SQC could also be demonstrated. There was a high positive correlation with a global 0–10 NRS of subjective global stress. Being asked prior to completing the SQC, this rating was not affected by the subsequent stress items. Interestingly, in the sample collected during ongoing COVID-19 restrictions, strong positive associations between perceived stress due to these restrictions and the SQC were observed. This association was no longer found, once the COVID-19 restrictions were lifted. Most notably, the stress levels did not differ between these two periods. This result contrasts with numerous findings indicating increased stress and psychological burden in children and adolescents during COVID-19 (Madigan et al., 2023). A possible explanation might be that our data collection started relatively late in the pandemic when restrictions were not as severe as at the beginning, and adaptation effects to pandemic-related restrictions may have already occurred (Daly & Robinson, 2021).
Moreover, overall stress burden, as well as school, time, and social stress, correlated highly with physical and psychological stress symptoms. The high positive correlations are consistent with previous reports of a close association between current stress and stress symptoms such as abdominal pain or sleep problems (Torsheim & Wold, 2001) as well as psychological stress symptoms like irritability and tension (Seiffge-Krenke & Lohaus, 2007).
As expected, there were also high positive correlations between dispositional anxiety (MAI-KJ; Hock et al., 2020) and current stress, which is consistent with the known neurobiological link between stress and anxiety (Daviu et al., 2019). Anxiety is likely to increase perceived stress, but stress burden is also associated with internalizing problems (March-Llanes et al., 2017) or state-anxiety (Bae et al., 2019). Children with anxiety disorders often experience significant impairments in school, family, and friendships, reporting high stress levels in these contexts (Grover et al., 2005). In White’s pilot study (2014), children with anxiety disorders and other stress-related disorders reported significantly more current stress than healthy children. Significant positive correlations between stress and anxiety have also been reported for stress questionnaires such as the ASQ and CSQ (Byrne et al., 2007, 2011).
Similarly, depressiveness, as assessed with the MAI-KJ (Hock et al., 2020), correlated highly positively with stress, consistent with previous findings. Stress as measured by the ASQ (Byrne et al., 2007) correlated highly positively with a non-validated measure of state-depression. The CSQ-CA (Bruin et al., 2018) showed a strong association between internalizing problems and chronic stress, while the Children’s Daily Stress Inventory (CSDI; Torres et al., 2009) showed a positive correlation with depression. The strong correlations between measures of anxiety and depressiveness and the SQC scores are noteworthy because, unlike measures such as the Chronic Stress Questionnaire for Children and Adolescents (CSQ-QA; Bruin et al., 2018), the SQC assesses current stress levels as opposed to much longer time periods (e.g., 1 year).
In addition, quality of life (KINDL; Ravens-Sieberer & Bullinger, 1998) was reported to be lower with higher current stress levels (SQC total, all subscales). This is consistent with chronic stress during the past year (CSQ-CA; Bruin et al., 2018) correlating negatively with global quality of life (Hwang & Oh, 2024). It is noteworthy that the detrimental effect of current stress on quality of life was observed even though the SQC does not assess stress levels across an extended period of time. Possibly, current stress levels are a good proxy of prolonged levels of elevated stress.
Girls endorsed higher stress levels on all scales than boys. Using the ASQ (Byrne et al., 2007), higher stress levels were also observed in girls across scales closely comparable to ours, including stress of school performance, home life, peer pressure, and school/leisure conflict. Girls show higher stress reactivity due to neurobiological differences in stress-axis function, brain regions, and hormones (Bale & Epperson, 2015; Bangasser et al., 2019; van der Voorn et al., 2017). Higher social stress may arise from gender-specific socialization, including greater social orientation and high expectations tied to social roles (Wiklund et al., 2012). Increased time stress is linked to higher responsibility-taking and multitasking in girls, often resulting in helplessness (Matud, 2004; Wiklund et al., 2010). School stress is further intensified by performance pressure and self-imposed demands commonly experienced by girls (Wiklund et al., 2010, 2012).
Age likely adds to stress burden due to increasing demands as children grow older, for example, academically with more school hours, homework, and exams; leisure activities with higher training loads; or increased household responsibilities (Hemming, 2015). Accordingly, in our sample, stress levels increased with age, particularly school and time stress as well as total stress burden. By contrast, social stress was age-independent. A similar pattern has been reported when (chronic) stress questionnaires have been used (Byrne et al., 2007). Specifically, an age-related increase in stress due to home life, school performance, future uncertainty, financial pressure, and emerging adult responsibility was found. Yet, social stress (e.g., romantic relationships, peer pressure) did not vary depending on age. Using the CSiK (Hemming, 2015), these age differences or lack thereof were also observed. As demonstrated by the reliability and validity analyses conducted separately for both age groups, the SQC effectively captures current stress in both children and adolescents.
Strengths and Limitations
A major strength of the SQC lies in its brevity with only 17 items and a child-friendly response scale. We also assessed usability as perceived by the children and adolescents. Item difficulty was generally rated to be low, although the youngest participants (ages six and seven) reported somewhat greater difficulty compared to older children. The comprehensibility of the items was rated high, with ratings increasing with age. Nonetheless, age-appropriateness was rated as high regardless of age, even though the youngest children tended to rate it somewhat lower. These data clearly support a high level of acceptance and child-friendliness of the SQC from a child’s perspective. The wide age range of 6 to 17 years represents another strength as it allows broad applicability. However, due to the limited number of 6- and 7-year-olds in our study, and some indications of increased item difficulty, further validation is warranted for this age group.
Despite several strengths, this study has some limitations. First, our data were collected through an online survey. This format was chosen because data collection began during COVID times, and in-person testing, or school visits were not possible. The presence of a caregiver might have led to a response behavior influenced by performance expectations or social desirability, especially regarding family stressors. Although we cannot fully rule out this possibility, we explicitly instructed parents that children should answer the questions alone (i.e., in the recruitment email, consent form, and on a separate page in the online survey where parents were explicitly asked to hand over the survey to their child alone). At survey completion, participants indicated if they had answered alone or with partial or full caregiver presence. Only five reported partial caregiver presence. It should also be noted that the results of the validity analyses were highly consistent with previous reports using other questionnaires. Nonetheless, in future studies, context effects should be avoided through in-person testing.
Second, we recruited a school sample but did not screen for mental disorders or other diseases. While we cannot rule out that children with a disorder might have participated, we do not believe that this would affect reliability, factorial validity, or convergent validity. In fact, we believe that our sample is rather representative of a typical school population, which aligns well with the intended use of the questionnaire in school settings.
Third, while the SQC demonstrated good psychometric properties in our German sample, we did not assess race, ethnicity, or trauma histories as potential moderators. Given the known associations between racial discrimination, impaired physical and mental health, and stress (Berger & Sarnyai, 2015; Priest et al., 2013), this represents a limitation in the generalizability of our findings. While the SQC focuses on stressors that we believe occur broadly across cultural contexts, certain items may nonetheless be differentially endorsed depending on a child’s sociocultural background. Yet, this would primarily result in context-related difference in the perceived stress level but would not necessarily limit the validity of the SQC as a measure of current (common) stress. Future studies should examine whether the SQC adequately captures stress experiences in more diverse populations and contexts.
Implications for Practice and Research
Given the link between stress and the development of depression and other psychiatric disorders (Lindholdt et al., 2022), as well as the rising mental health burden among youth following the COVID-19 pandemic (Madigan et al., 2023), the availability of a brief, easy-to-administer tool to quickly assess stress is increasingly important. The SQC has shown associations with measures of depression, anxiety, and physical symptoms that may impair academic performance (Fröjd et al., 2008). Although the SQC has not yet been validated as a screening instrument, it offers educators and school mental health professionals a practical tool for assessing students’ acute stress levels at a given time point. This information contributes to a more comprehensive understanding of students’ well-being and mental health and can inform targeted supportive or preventive interventions for those experiencing acute stress. Future research should evaluate the SQC’s potential as a screening measure in at-risk populations, including the establishment of norms or reference scores in school settings.
The SQC’s focus on stress within the past week distinguishes it from instruments assessing chronic stress, which may be less sensitive to short-term fluctuations. This temporal focus may enable the detection of changes in stress burden over time and could allow the SQC to serve as an outcome measure in evaluating stress-reduction interventions, such as mindfulness-based programs (Phan et al., 2022). Additional studies should examine its sensitivity to change.
In practical terms, the SQC can help school practitioners to efficiently assess student stress burden as an indicator of mental health needs, allowing evidence-based referrals and resource allocation. Although not a clinical diagnostic instrument, future validation studies should focus on discriminant validity by comparing healthy children with those experiencing psychological or somatic conditions. Further research should examine how risk and protective factors such as personality traits, socioeconomic status, and social support influence stress outcomes and evaluate the instrument’s predictive validity regarding long-term health and adjustment.
Notably, cross-cultural validation is another essential step, as the current study’s sample did not address ethnic diversity. Experiences of racism, marginalization, or a trauma history may contribute to stress in ways that differ from those captured in the current item set, especially for children and adolescents from underrepresented or minoritized backgrounds (Everett et al., 2016; Priest et al., 2013). To enhance generalizability, future studies should assess the factor structure in culturally and racially diverse populations. Should differences arise, expanding the item pool through qualitative research with children and adolescents from more diverse backgrounds will be necessary to adequately capture varied stress experiences.
Conclusion
In conclusion, the SQC has been shown to be a reliable and valid questionnaire to measure current stress in children and adolescents across a broad age range. The SQC is user-friendly, tailored for children, and captures relevant aspects of childhood stress. Its psychometric properties are sound and make the SQC a promising and easy-to-use measure for stress in youth.
Footnotes
Acknowledgements
We thank Sarah Platte and Celine Schroeder for their help in data collection.
Author Contributions
Alannah Hahn: Conceptualization; Methodology; Formal analysis; Writing—original draft.
Alexander Winkler: Conceptualization; Methodology; Validation; Writing—review and editing; Supervision.
Christiane Hermann: Conceptualization; Methodology; Validation; Writing—review and editing; Supervision.
Funding
This work was supported by the DYNAMIC center, which is funded by the LOEWE program of the Hessian Ministry of Science and Arts (Grant Number: LOEWE1/16/519/03/09.001[0009]/98).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.