
Abstract
This study examined the association between social distancing measures and Quality of Life (QoL), behavioural problems, and cognition among older adults with severe dementia in residential homes. QoL (Chinese version of the Quality of Life for Late-Stage Dementia), behavioural problems (Chinese version of the Neuropsychiatric Inventory), cognition (Chinese version of the Cognitive Test for Severe Dementia), and clinical variables were evaluated at baseline, 6, and 12 months. Activity involvement was recorded on a monthly basis. Sixty-four participants completed the one-year follow-up. QoL worsened continuously from baseline to month-12; correlated with reduced activity involvement and increased depression level. Behavioural problems increased significantly from baseline to month-12; correlated with reduced activity involvement and deteriorated self-care function. Cognition declined significantly from baseline to month-12; correlated with reduced non-sedentary time. The findings suggest that social restrictions may be negatively related to the QoL, behavioural problems, and cognition of residents with severe dementia.
Introduction
Social distancing measures in long-term care (LTC) facilities have been widely adopted worldwide since the outbreak of coronavirus disease 2019 (COVID-19) in 2020. These measures are aimed to prevent virus transmission in LTC facilities to varying degrees.1,2 Social distancing measures are non-pharmacological strategies to prevent contagious diseases by maintaining physical distance between individuals and reducing interactions. 3
Older adults with dementia in LTC facilities face an increased risk of COVID-19 infection4-7 In Hong Kong, the pandemic swept through nearly all Residential Care Homes for the Elderly (RCHE) units across six waves from 2020 to 2023. The first two waves occurred between May and September 2020, affecting 19 RCHEs. Wave 4 occurred between October 2020 and December 2021, and Wave 5 occurred between December 2021 and May 2022, resulting in record-breaking confirmed cases, with 96% of the RCHE units reporting infections. Wave 6 and post Wave-6 occurred between May and December 2022.8,9
In response to the pandemic, the Centre for Health Protection issued guidelines for RCHEs to prevent the spread of coronavirus in January 2020, and adjusted the measures based on the epidemic conditions until 2023. Staff and residents must follow precautionary measures, including regular testing, disinfection, and physical distancing. 10 Furthermore, the restriction on visitors’ arrangement resulted in the suspension of family and friends’ visits, although residents could meet their families via teleconference or at designated areas with partitions in residential units. The situation worsened during Wave 5 when public hospitals faced the unprecedented challenges for tremendous confirmed cases, and led to infected residents being quarantined on-site in overcrowded conditions in residential units. 11 RCHE staff reported intense stress due to rapid changing condition in pandemic, perceived infection threats, increased workload, and manpower shortages.12,13 Residents needed to adapt to sudden routine changes, including the suspension of non-essential care, activities, and social gatherings, with restricted access to common areas of the facilities.
Recent reviews have revealed that prolonged social distancing measures likely have negative effect on the psychosocial well-being, behavioural problems, and cognition of older adults. The influence may be greater in individuals with dementia than in those without. However, most studies have focused on the early stages of dementia in the community and have employed cross-sectional designs.14-16 Social distancing measures may differ according to the stage of dementia in LTC facilities. Individuals with mild dementia may feel distressed due to pandemic awareness, 17 and stricter restrictions may be needed for those with severe dementia, as they may not understand the infection control measures.18,19 Older adults in the later stages of dementia rely greatly on others for daily care in residential homes. 20 Their main sources of social interaction are staff and co-residents in personal care, activity involvement, and family and friend visits. The implementation of social distancing measures greatly alters the quality and quantity of interactions among residents with severe dementia. Consequently, their physical activity levels are inevitably affected, which may lead to increased behavioural problems. 21
Prolonged social restriction measures conflict with person-centered care (PCC) in dementia care. 22 The lessons learnt from this unprecedented pandemic present an opportunity for a more thorough examination of the influence of social distancing measures in this population. The findings can provide concrete evidence for policymakers and the field to refine LTC policies and improve preparedness for future infectious disease outbreaks. Therefore, this study employed objective measurements of activity involvement and physical activity levels to quantify the changes of social distancing. The aim of this study was to examine the association between social distancing and QoL, behavioural problems, and cognitive function among older adults with severe dementia in LTC.
Methods
Study Design and Participants
This was a one-year longitudinal study. Care and Attention (C&A) homes were recruited through convenience sampling from the RCHE list of the Social Welfare Department. Nine subvented homes and one self-financed residential home were invited to participate in the study. Six subvented homes accepted the invitation, three declined because of the pandemic, and one did not respond. Convenience sampling was used to recruit approximately 15 eligible participants from each home. Data collection for Home A occurred from Wave 1 to the start of Wave 4, between January 2020 and January 2021. The data for Homes B to D were collected from the end of Wave 4 to post Wave 5, between November 2021 and November 2022. Data for Homes E and F were collected from the end of the Wave 5 to Wave 6 and afterwards, between May 2022 and October 2023.
The target participants were older adults with severe dementia living in residential homes. The inclusion criteria were as follows: (1) aged 65 years and over, (2) had a documented medical diagnosis of major neurocognitive disorder (dementia) according to the Diagnostic and Statistical Manual of Mental Disorders 5, 23 and (3) had a rating of 3 on the Clinical Dementia Rating scale. 24 The exclusion criteria were as follows: (1) diagnosis of bipolar disorder or schizophrenia, (2) blindness or deafness, and (3) severely impaired consciousness. Informed consent was obtained from family members or guardians via residential homes, as the participants were mentally incapable.
Data Collection Methods and Tools
Demographic data were retrieved from case files by residential home Occupational Therapist (OT) at baseline. Outcome and clinical variables were collected at baseline, 6, and 12 months, while activity involvement was recorded for five days at monthly intervals over the one-year follow-up. The principal investigator (PI) conducted the assessments of QoL and cognition, while other assessments were collected by residential home OT. Before the study commenced, the PI provided training to the residential staff on the assessment implementation, including wearing actigraph, and staff members could contact the PI for inquiries via email or telephone throughout the study.
Outcome Variables
(a) QoL was measured using the Chinese version of the Quality of Life in Late-Stage Dementia scale (QUALID-C).
25
The original English version was developed by Weiner et al in 2000 and has been translated into different languages with good validity and reliability. It is a proxy-rated scale with 11 items on observable mood and behaviour. Items are categorized into two subscales: expression of comfort (positive emotion) and expression of discomfort (negative emotion). The comfort subscale comprises five items: “smiles”, “enjoys eating”, “appears calm and comfortable”, “enjoys touching/being touched”, and “enjoys interacting with others”. The discomfort subscale comprises six items: “appears sad”, “cries”, “facial expression of discomfort”, “appears physically uncomfortable”, “verbalizations suggest discomfort”, and “irritable or aggressive”. The rating uses a 5-point scale based on occurrences in the prior week. The maximum score is 55, with lower scores indicating better QoL.
26
(b) Behavioural problems were measured using the Chinese version of the Neuropsychiatric Inventory (CNPI).
27
The instrument comprises two parts: CNIP-I and CNIP-II. The CNPI-I measures the severity of neuropsychiatric symptoms, with a maximum score of 144, with higher scores indicating severe symptoms. The CNPI-II measures caregiver stress, with a maximum score of 60, with higher scores indicating higher stress levels. (c) Cognitive function was measured using the Chinese version of the Cognitive Test for Severe Dementia (CTSD-C).
25
The English version was developed by Tanaka et al in 2015, and has been found to reliably capture longitudinal changes in cognition in severe dementia. It is a performance-based assessment tool with 13 items in seven domains: orientation, memory, language, visuospatial ability, frontal function, praxis, and social interaction. The maximum score is 30, with higher scores indicating better cognitive function.28,29
Clinical Variables
(a) Activity involvement was recorded using an activity chart to gather information on the types of activities, time, duration, venue, and manpower required. The categories of activities were based on general practice at residential homes and previous literature,30,31 categories were listening to music/radio, watching television, arts and crafts, art therapy, music therapy, cognition, reminiscence, companion doll/pet, multi-sensory stimulation, exercises, self-care and domestic tasks, visits by friends/family, social, community access, and others. (b) Daytime physical activity level was assessed using an accelerometer (wGT3X-BT Actigraph, Actigraph Corporation, Inc.). It is approximately the shape and size of a smartwatch and a clinically validated objective assessment that provides quantitative information regarding the level of physical activity.
32
The actigraph was worn on the participant’s wrist from approximately 8:30 am to 5:30 pm for five consecutive days and applied to the non-dominant hand if the dominant side was paretic. It could be removed for showering or medical needs. The sedentary time cutoff is 1853 counts per minute.
33
(c) Self-care function was assessed using the Modified Barthel Index (MBI).
34
It comprises ten items covering feeding, grooming, dressing, transfer, toilet, bathing, ambulation, stair climbing, and bladder and bowel control. The maximum score is 100, with higher scores indicating greater independence in self-care tasks. (d) Depression level was assessed using the Chinese version of the Cornell Depression Scale (CCDS).
35
This informant-rated scale assesses mood severity in older adults with dementia. It comprises 19 items covering behavioural, physical, cyclic, and ideational symptoms. The maximum score is 38, with higher scores indicating more severe depression. A score of eight or more indicates a depressive mood.
Statistical Analysis
The IBM Statistical Package for Social Sciences (SPSS) software version 26 was used to analyze the data. All statistical tests were two-tailed, and statistical significance was set at p< 0.050 considered to be significant. Descriptive statistics were used to obtain the general distribution of demographic data, outcome and clinical variables. Spearman’s correlation coefficient was used to examine the bivariate association between two variables. Independent T-test was used to examine the difference between independent groups. Repeated measures of analysis of variance (ANOVA) were used to examine the changes in outcome and clinical variables from baseline to month-12 evaluations, Bonferroni adjustment was applied in multiple comparisons.
Results
A total of 81 participants (female= 70) were recruited with mean age of 89.41 at baseline, and 63% of them received no formal education. Of them, 73 and 64 participants completed the half-year and one-year assessments, respectively (Figure 1). The baseline profile of the sample is presented in Table 1, and the baseline differences between the completers and non-completers are shown in Table 2. Flowchart of participants recruitment Participants Characteristics at Baseline (n = 81) sd = standard deviation. QUALID-C = Chinese Version of Quality of life in Late-stage Dementia; CNPI = Chinese version of Neuropsychiatric Inventory. CTSD-C = Chinese version of Cognitive Test for Severe Dementia; CCDS= Chinese version of Cornell Depression Scale; MBI= Modified Barthel Index. Baseline Comparison Between Completers and Non-Completers QUALID-C = Chinese Version of Quality of life in Late-stage Dementia; CNPI = Chinese version of Neuropsychiatric Inventory; CTSD-C = Chinese version of Cognitive Test for Severe Dementia; CCDS= Chinese version of Cornell Depression Scale; MBI= Modified Barthel index.


The Changes of Outcome Variables Over One-Year
Changes of the QUALID-C Scores Over One-Year (n=64)

*Indicates p-value <0.050, **p-value <0.010 (with Bonferroni Adjustment).
QUALID-C = Chinese Version of Quality of life in Late-stage Dementia, # The lower sores indicate better QoL.
Changes of the CNPI Scores Over One-Year (n=64)
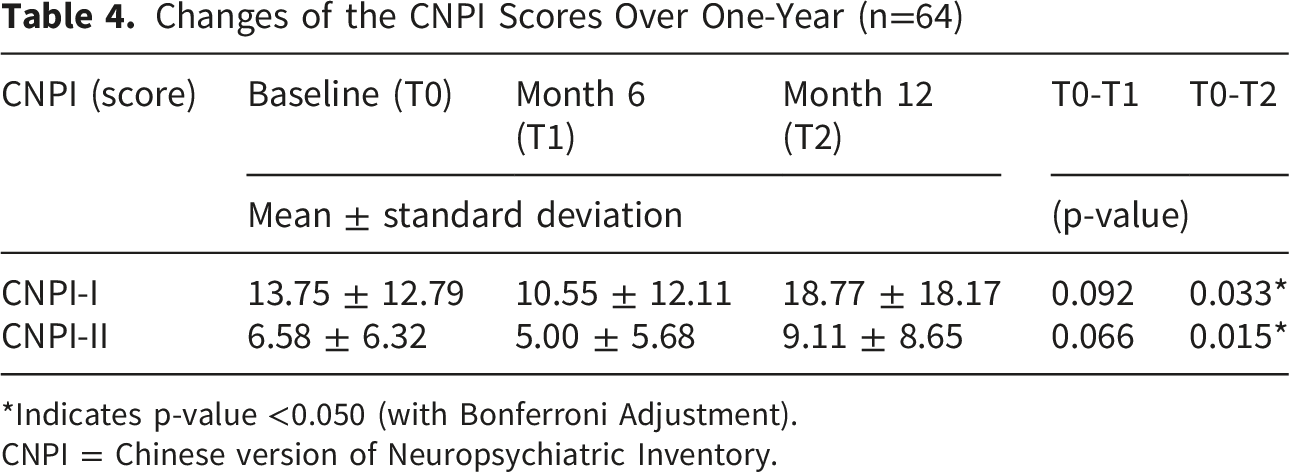
*Indicates p-value <0.050 (with Bonferroni Adjustment).
CNPI = Chinese version of Neuropsychiatric Inventory.
Changes of the CTSD-C Scores Over One-Year (n=64)

*Indicates p-value <0.050; **p-value < 0.010 (with Bonferroni Adjustment).
CTSD-C = Chinese version of Cognitive Test for Severe Dementia.
The Changes of Clinical Variables Over One-Year
Changes of Clinical Variables Over One-Year (n = 64)

*Indicates p-value <0.050, **p-value <0.010 (with Bonferroni Adjustment).
CCDS= Chinese version of Cornell Depression Scale; MBI= modified Barthel Index.
The Number and Duration of Activity Involvement Over One-Year (n=64)


Changes of number of activity involvement at a monthly interval over one year (n=64).

Changes of number of activity involvement at homes where data collection occurred during the same wave (n=64).
Correlation Between Outcomes and Clinical Variables
Correlations Between Outcomes and Clinical Variables
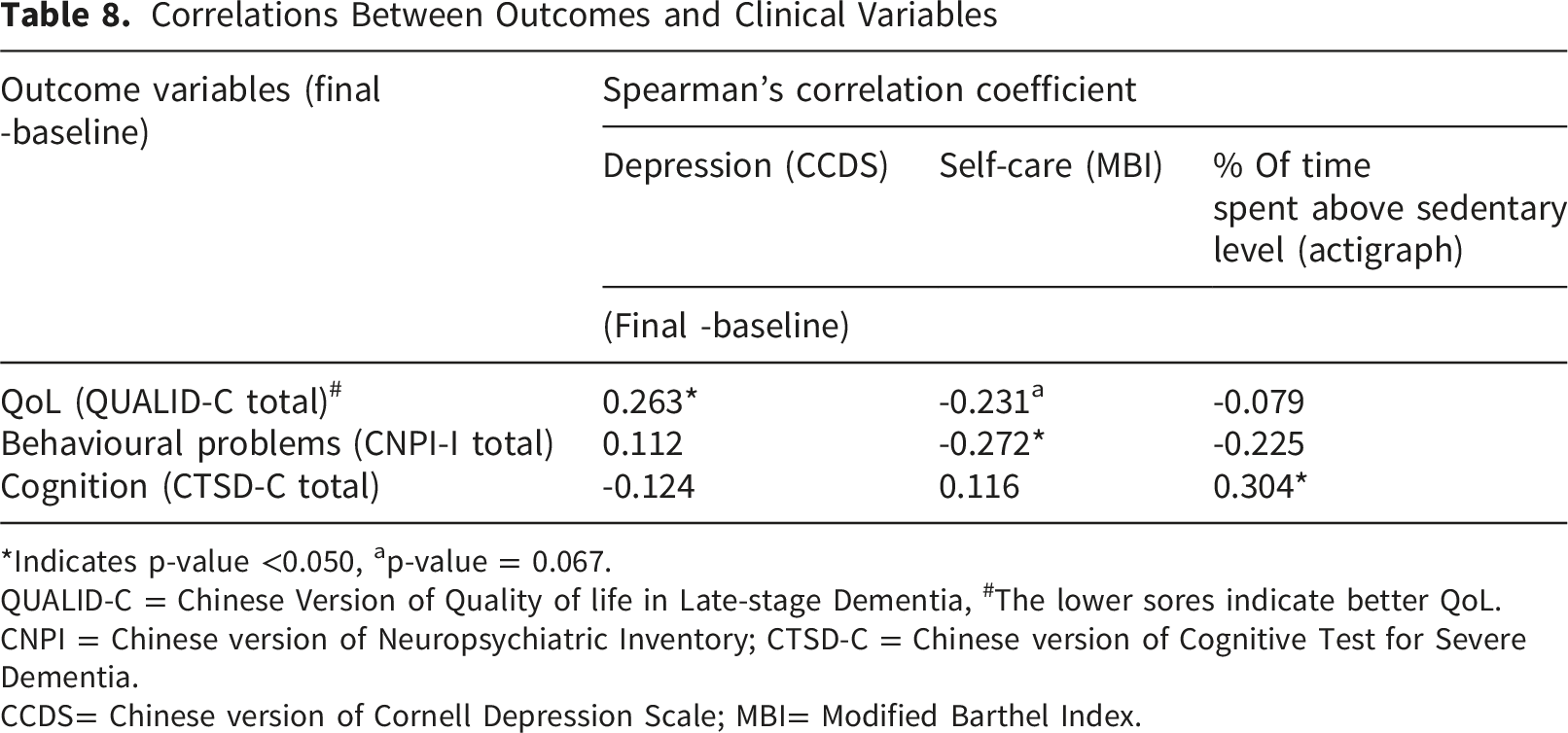
*Indicates p-value <0.050, ap-value = 0.067.
QUALID-C = Chinese Version of Quality of life in Late-stage Dementia, #The lower sores indicate better QoL.
CNPI = Chinese version of Neuropsychiatric Inventory; CTSD-C = Chinese version of Cognitive Test for Severe Dementia.
CCDS= Chinese version of Cornell Depression Scale; MBI= Modified Barthel Index.
Correlations Between Outcomes and Activity Involvement

*Indicates p-value <0.050; **p-value < 0.010.
QUALID-C = Chinese Version of Quality of life in Late-stage Dementia, #The lower sores indicate better QoL.
CNPI = Chinese version of Neuropsychiatric Inventory; CTSD-C = Chinese version of Cognitive Test for Severe Dementia.
Discussion
The aim of this study was to investigate the association between social distancing measures and QoL, behavioural problems, and cognition on residents with severe dementia.
Our sample of 81 participants was recruited from six C&A homes in different districts in Hong Kong. Their mean age was 89.41 years, which was similar to that of previous local report. 36 The baseline QUALID-C (QoL) was 23.28 ± 5.81 which falls within the range (22.74 ± 7.4 and 23.9 ± 6.9) reported in other samples of severe dementia recruited in LTC.26,37-40
The Longitudinal Changes of QoL
The results indicated a decline in overall QoL over the course of a year. The discomfort (negative emotion) and comfort (positive emotion) scales showed a distinct pattern across the three assessments, as QoL is a multifactorial concept encompassing those in the later stages of dementia.41,42
The QoL comfort scale declined from baseline to month-6 and improved slightly in month-12 evaluation. Spearman’s correlation revealed that greater activity involvement was correlated with a better comfort scale. Previous studies have indicated that meaningful activities positively influence QoL in dementia.43-45 In interviews with home staff, residents most frequently expressed positive emotions during meaningful activities or family visits. In Home A, the data collection of the first half-year coincided with the initial two waves, and the baseline activity record was similar to the pre-pandemic, as it was collected just prior to the outbreak. Subsequently, activities were suspended as staff experienced heightened anxiety due to insufficient knowledge and protective equipment availability. With clearer guidelines and a supply of protective equipment for RCHEs in the latter half of the year, individual bedside activities were gradually resumed. According to their staff, they adopted a more stringent approach by requiring both staff and visitors to undergo regular testing to reduce the risk of infection; staff could stay at the residential home if necessary. Additionally, participants resided on three separate floors, enabling the designated rehabilitation staff to continue activities as long as the respective floors were not isolated. The data collection of Homes B to D started when Wave 4 was stable. The first half-year period aligned with the peak of Wave 5, during which nearly all activities came to a halt. In the later half-year period, most residents and staff contracted the infection and/or received at least one vaccine dose, 8 alleviating staff concerns regarding transmission. Rehabilitation staff no longer needed to wear full protective gear when delivering activities, and activities in rehabilitation rooms and in-person family visits gradually resumed. According to the staff of Homes B and C, they had designated rehabilitation staff for residents in different areas, allowing activities to resume if the floor was not isolated. In Home D, an experienced OT initiated the redesign of simple individual activities for residents, even during isolation. These adjustments could resume activities for residents and enhance interaction, and may have contributed to the improvement of the QoL comfort scale. Data collection for Homes E and F took place between the decline of Wave 5 and the stabilization of Wave 6, with the month-6 evaluation coinciding with the peak of Wave 6. Although mandatory infection control measures were relaxed from December 2022 and fully lifted by March 2023, RCHEs required time to adjust their daily operations to prevent a resurgence of cases and gradually restore services. According to their staff, they allocated more resources to individuals with greater rehabilitation potential while adopting a conservative approach for those with late-stage dementia. Activities for residents in the later stages of dementia remained low and only showed slight improvement towards month-12.
The QoL discomfort scale deteriorated continuously, with a significant change in month-12 evaluation. This trend may be explained by several reasons. The marked and rapid disruptions to daily routines negatively affected both physical and psychosocial well-being 46 ; negative emotions were likely elicited as those with severe dementia had greater difficulty understanding and complying with the changes. Manpower resources were prioritized for infection control, potentially delaying responses to residents’ requests and negatively affecting their psychosocial well-being. 47 Residents were isolated if suspected of infection, and their personal care was severely affected. Furthermore, there was a noticeable increase in depressive mood and deterioration in self-care abilities from baseline to month-12, and these factors have been found to related to QoL in severe dementia.48-50
The Longitudinal Changes of Behavioural Problems
The CNPI-I and CNPI-II total scores showed a reduction in behavioural symptoms and caregiver stress from baseline to month-6, followed by an increase in month-12. This observation may be explained by several reasons.
First, the causes of behavioural problems are multifactorial. 51 The patterns of symptoms may result from disease progression and are usually display episodically. 52 Second, these variations could be attributed to changes in care provided over different periods during pandemic.53,54 Individuals with severe dementia may struggle to comprehend infection control measures and find abrupt changes challenging. 19 Third, our findings indicate that behavioural problems worsen with decreased activity involvement but not with non-sedentary time. Meaningful activity is a widely used non-pharmacological approach to manage behavioural problems in dementia, 55 and a lack of activities is suggested to be a contributing factor to these problems. 56 An environment of prolonged under-stimulation during the first half-year might lead to a significant increase in overall behavioural symptoms observed in month-12, 57 along with heightened care related stress among staff, surpassing baseline levels. Furthermore, our finding of an insignificant correlation between behavioural problems and non-sedentary time contrasts with that of a cross-sectional study. 21 This discrepancy may stem from differences in sample sources and study design. Besides, actigraphy was used to measure daytime physical activity levels, and the very low physical activity levels in our sample may have attenuated the association. Finally, our results demonstrated a significant correlation between worsening behavioural problems and deterioration of self-care function. Previous study has suggested a bilateral relationship between these two variables. 58 During the pandemic, residents’ personal care time was greatly reduced, such as only wiping the body instead of taking a shower during Wave 5.
The first half-year data collection in Homes A to D, there was marked reduction in care time, might temporarily decrease behavioural issues in individuals with severe dementia, thus reducing staff stress when addressing these problems. Data collection for the second half-year at Home A took place during Waves 3 and 4, coinciding with the first reported residential COVID-19 case. For Homes B to D, data collection was conducted when the Wave 5 began to stabilize, allowing for the gradual resumption of personal care services. Enforced infection control measures were introduced, such as the requirement of daily rapid antigen tests (RAT) to identify cases earlier. Additional restrictions may be necessary in the later stages of dementia to comply with infection measures, resulting in more distress.1,13,18 In Homes E and F, the participants experienced six pandemic waves and over two years of social distancing. This prolonged isolation may result in a continuous rise in behavioural symptoms and related caregiver stress, as noted in month-12.59,60
In analysing CNPI item changes over time, most items showed fluctuations except for apathy. Apathy is defined as a lack of motivation to engage in activities, and prolonged social restrictions may result in worsening of this symptom. 61
The Longitudinal Changes of Cognition
Similar to previous surveys and retrospective studies conducted during the pandemic,62-64 our participants exhibited a significant decline in the CTSD-C, particularly in the language, frontal, and social areas. According to biopsychosocial and brain plasticity models, dementia care outcomes are influenced by both biological and social factors. 65 First, cognition in individuals with dementia naturally deteriorates as the disease progresses. Second, Hughes et al (2012) suggested that regular social engagement might delay the progression from mild to severe cognitive decline. 66 The quantity and quality of social interactions were substantially affected by the pandemic. Third, our results indicated that cognitive decline was significantly correlated with non-sedentary time but not with the total number of activities involved. Prolonged sedentary time is found to be associated with poor cognitive function. 67 Besides, most recorded activities were not cognitively stimulating, such as passive mobilization exercises, static cycling, watching television, and listening to the radio. Non-sedentary time mainly refers to activities that require participants to be alert and actively engaged, including walking, daily living tasks, and cognitive stimulating activities in this study. The limited prescriptions of cognitive stimulating activities comprised their effectiveness on cognitive function. Finally, approximately 50% of our participants tested positive for COVID-19 through RAT or Polymerase Chain Reaction tests, with approximately 5% experiencing a second infection during data collection. The cognitive deterioration reported could be attributed to post-infection cognitive problems. 68 Despite this, Leung et al (2024) assessed cognitive function in older adults with mild to moderate dementia after a year of social restrictions in RCHEs and found that participants experienced significant cognitive decline compared to pre-pandemic levels, even without infection. 69
Strengths and Limitations
This study addresses the limited evidence on longitudinal changes in QoL, behavioural problems, and cognitive function among residents with severe dementia under extended social restriction. Participants were recruited from six residential homes across districts to enhance sample representativeness. Furthermore, the monthly activity involvement records provided quantitative data on the reduction in social interactions. Actigraphy was used to objectively measure the participants’ physical activity level, a factor that has not been thoroughly examined in previous studies. A performance-based, culturally validated cognitive test was used to evaluate cognitive function rather than employing surveys only.
This study has several limitations. First, convenience sampling affects the generalizability of the results of this study. Second, the monthly activity involvement was recorded over five days, which might not fully represent the picture of the whole month and might have potential reporting and recall biases. Furthermore, the arrangement of activities, such as suspension reasons at individual homes, was based on self-reports and may not accurately reflect the actual circumstances. Third, the deterioration in QoL, behavioural symptoms, and cognition may be attributed to social restrictions, natural dementia progression, and/or post-infection symptoms. However, there are no data on the severity of covid-19 infection which may affect post-infection cognitive function. 70 Fourth, the duration of social isolation varied among participants recruited during the different pandemic waves. Participants from Home A had been under social distancing for one year, Homes B to D had been isolated for two years, and Homes E and F had been isolated for almost three years. Research suggests that isolation duration influences behavioural problems and cognition in different ways. 71 Fifth, the ratings of assessments might be affected by the stress level of responsible staff members, such as pandemic fatigue; however, we did not have related measurements. 72 Finally, without pre-pandemic measurements of outcome variables and a control group, it is not possible to conclude that the effects were solely due to social isolation.
Clinical Implications and Recommendations
The findings of this study highlight the importance of the quality and quantity of care for individuals with later stages of dementia. Willemse et al (2015) suggested that care staff are typically the most engaged with residents and are fundamental to PCC. 47 Balancing infection control measures with ongoing care is crucial for this group of clients.
Designated staff and areas should be assigned for residents to continue rehabilitation and reduce the risk of contamination. Portable equipment and simple activities can use to keep residents active at their bedside. Gerontechnology, such as smart digital windows, can display natural scenes without additional manpower. Reinforced staff training on communication skills, which may take time to develop, is essential to enhancing positive interaction and cooperation in people with severe dementia in daily care. 73 Gavelin et al (2021) found that individuals with cognitive impairments require more intensive cognitive training to achieve improvement than those without such impairments. 74 Existing post-pandemic rehabilitation also mainly focuses on early stages of dementia, with little evidence for later stages. Professionals and care staff should learn from the pandemic experiences to plan for the later stages of dementia care process. 75
Conclusions
In summary, our findings revealed that older adults with severe dementia experienced a marked reduction in activity involvement and non-sedentary time under prolonged social distancing measures in LTC. These may be negatively related to their QoL, behavioural problems, and cognitive function. A longer follow-up period is recommended to assess the post-pandemic conditions. Additional resources are needed to support residential homes in maintaining care under social restrictions and post-pandemic rehabilitation tailored to this specific group.
Footnotes
Acknowledgments
The authors extend their sincere appreciation to the staff members, participants and their family members of all involved residential units for their invaluable collaboration in conducting this research.
Ethical Considerations
This study was approved by the Survey and Behavioral Research Ethics Committee of the Chinese University of Hong Kong (number: SBRE-19-822).
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data will be available from the corresponding author upon reasonable request.