
Abstract
Background
A validated instrument for assessing adolescent attitudes toward dementia in Chinese-speaking communities is currently lacking. This study aims to translate the Brief-AADS into Chinese and examine the psychometric properties of the Brief AADS-C.
Methods
The methodological study employed a cross-sectional design with 2 phases. Data was collected in Macao and Shenzhen, China.
Results
The scale demonstrated excellent content validity(S-CVI = 0.99) and good internal consistency (Cronbach’s α = 0.814). Test-retest reliability was acceptable (ICC = 0.647). EFA identified a three-factor solution “Perceptions”, “Acceptance”, and “Engagement” with 11items—accounting for 56.07% of the variance. CFA supported this 3-factor structure with acceptable goodness of fit indices (χ2/df = 3.076, GFI = 0.937, SRMR = 0.0579, RMSEA = 0.077). All factor loadings of the items ranged from 0. 33to 0.82, indicating strong item-factor relationships.
Conclusions
The Brief AADS-C is reliable and valid for assessing adolescent attitudes toward dementia in Chinese-speaking regions.
Introduction
Dementia is a major global health concern, affecting over 55 million people worldwide, with numbers projected to rise to 139 million by 2050. 1 As dementia prevalence continues to rise, many countries, including China, have prioritized dementia awareness and have been developing Dementia-Friendly Communities (DFCs) through public health policies.2,3 In Macao, for instance, the government has implemented a 10-year strategic framework to foster DFCs, aiming to promote social inclusion and reduce stigma.4,5 However, while efforts have focused on improving dementia awareness among healthcare professionals and caregivers,6-8 adolescents remain an underrepresented group in dementia education and research. Given that adolescence is a critical period for shaping long-term social attitudes,9-11 understanding and improving adolescent perceptions of dementia could play a pivotal role in long-term stigma reduction and caregiving behaviors. Evidence suggests that well-designed programs can positively shape youth attitudes toward dementia. For example, Australia’s “Intergenerational Dementia Education” and the UK’s “Dementia Friends” initiatives have successfully improved adolescent awareness and engagement.12,13 Similarly, culturally specific programs in Macao highlight the importance of contextually adaptive interventions, reinforcing the global need for youth-focused dementia education. 14
Assessing adolescents’ attitudes toward dementia is essential for designing effective educational programs. However, most existing dementia attitude scales, such as the Dementia Attitudes Scale (DAS), 15 the Dementia Care Attitude Scale, 16 the Chinese instrument of knowledge, attitude and preventive practice on dementia care, 17 the Scale of Attitudes toward People with Dementia and their Care 18 and the Dementia Public Stigma Scale 19 were developed for adults or healthcare professionals. These scales may demonstrate reduced accuracy or weaker psychometric properties when applied to adolescent populations, primarily due to differences in cognitive maturity and contextual relevance. For example, adolescents typically lack caregiving experience, which may hinder their ability to meaningfully respond to items such as “I cannot imagine taking care of someone with Alzheimer’s disease and related dementias” from the DAS. 15 Similarly, the item “It is rewarding to work with people who have Alzheimer’s disease and related dementias”in DAS 15 may be less applicable or resonant for this age group.
Although some studies have employed self-designed questionnaires to assess adolescent attitudes,20-22 many of these tools lack psychometric validation, raising concerns about their reliability and cross-cultural applicability. The Adolescent Attitudes toward Dementia Scale (A-ADS) was the first validated tool specifically designed for adolescents and has since been refined into a shorter, psychometrically robust version—the Brief Adolescent Attitudes toward Dementia Scale (Brief A-ADS).23-25 Together with the original English version, further cross-cultural validations in Pakistan and Malaysia further affirm its broader applicability.24,26 Recently, the Brief A-ADS was recognized as one of the most reliable tools for assessing dementia-related attitudes in young populations. 27 However, a validated instrument for evaluating adolescent attitudes toward dementia within the Chinese-speaking communities still lacked, leaving a significant research gap.
To address this gap, the study aims to translate and validate the Chinese version of the Brief A-ADS. And it can contribute to: (1) improving the measurement of adolescent dementia attitudes in Chinese-speaking populations, (2) facilitating cross-cultural comparisons of dementia attitudes, and (3) supporting the development of targeted dementia education programs for adolescents in schools and communities. The validated Brief AADS-C will serve as a valuable tool for future research and policy initiatives aimed at enhancing dementia awareness among youth.
Methods
This research employed a cross-sectional methodological design in 2 phases. The first phase aimed to:(1) translate the English-language version of the Brief AADS into Chinese language using a modified Brislin’s translation model, 28 with approval from the original authors; (2) access the content and face validation of the translated scale. The second phase examined the psychometric properties of the Brief AADS-C.
Phase 1: Translation, Content and Face Validation
The translation process was based on the principles of Brislin’s model of forward and backward translation. 28 Forward translation: 2 bilingual experts in nursing with overseas study experience independently translated the original English version into Chinese. The research team and translators reviewed and discussed the translations to reach a consensus on a preliminary Chinese version. Back translation: The preliminary Chinese version was back-translated into English by 2 independent bilingual experts unaware of the original scale. Discrepancies were resolved through comparisons with the original version to ensure equivalence. Consensus meeting: The research team and translators finalized the Chinese version after iterative discussions, ensuring linguistic and cultural relevance.
Content validity was assessed utilizing the Content Validity Index (CVI). A panel of 6 experts in dementia education (including a psychiatrist, a social worker, 2 geriatric nurses, and academic staff in psychology and education) evaluated the relevance of each item on a 4-point Likert scale, where 1 indicated “not relevant” and 4 indicated “highly relevant.” The Item-Level Content Validity Index (I-CVI) was determined by dividing the number of experts who rated an item as either 3 or 4 by the total number of experts. The Scale-Level Content Validity Index, Average (S-CVI/Ave), was calculated by averaging the I-CVI values across all items. The criteria for acceptable content validity were established at I-CVI ≥ 0.78 and S-CVI/Ave ≥ 0.90. 29
The face validity of the Brief AADS-C was evaluated to ensure item comprehensibility and applicability as a self-report tool. A purposive sample of 8-20 potential users were recruited, as literature suggests this range effectively identifies ambiguous items.30,31 Participants assessed item clarity (yes/no) and rephrased items in their own words; interpretability was rated by researchers on a 4-point Likert scale (1 = fully correct, 4 = completely wrong). 32
Phase 2: Psychometric Testing of the Brief AADS-C
The Brief AADS-C’s psychometric properties were assessed using a correlational cross-sectional design to evaluate construct validity, internal consistency and test-retest reliability. To ensure independent evaluation and avoid carry-over effects, phase 1 samples were excluded. The study sample was recruited from high school and university students in Macao and Shenzhen, China. Eligibility criteria mandated that participants (a) aged between 15 and 24 years old, (b) have proficiency in reading and comprehending Chinese, and (c) provide informed consent for participation. Sample size estimation followed the recommendation of 10-20 participants per item for factor analysis. 33 With the Brief A-ADS comprising 13 items, a minimum of 130 to 260 participants was deemed sufficient for Exploratory Factor Analysis (EFA), and the sample size of Confirmatory Factor Analysis (CFA) is normally not less than that of EFA. Thus, to ensure statistical robustness, a target sample size of approximately 700 participants was set, evenly divided for exploratory factor analysis (EFA, n = 350) and confirmatory factor analysis (CFA, n = 350).Students from 5 high schools and 5 universities in the study regions were conveniently recruited. The survey was conducted via an online platform (Wen Juan Xin). A poster containing a QR code linked to the survey was distributed with institutional support. Participants voluntarily completed the survey in September and October 2024, following a pilot test with 50 participants to refine the procedure.
Construct validity was evaluated through Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA). The EFA was performed on a randomly selected subsample comprising 50% of the total participants (n = 353). A scree plot was constructed to determine the optimal number of factors to retain, employing maximum likelihood estimation for normally distributed datasets and principal axis factoring for non-normal distributions. 34 To optimize the factor structure, we implemented Promax rotation with Kaiser normalization, an oblique rotation method particularly suited for identifying correlated latent variables in psychological and behavioral research. Factor retention criteria included eigenvalues greater than 1 and factor loadings of 0.40 or higher. The suitability of the data was confirmed by a Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy of 0.80 or above, and a significant Bartlett’s test of sphericity (P < 0.05). The CFA was conducted on the remaining subsample (n = 354) using maximum likelihood estimation. Model fit was assessed using several indices, including a chi-square to degrees of freedom ratio (χ2/df) of less than 5.0, a Goodness of Fit Index (GFI) of 0.90 or higher, a Comparative Fit Index (CFI) of 0.90 or higher, a Standardized Root Mean Square Residual (SRMR) of 0.08 or lower, and a Root Mean Square Error of Approximation (RMSEA) of 0.05 or lower. 35
Internal consistency was assessed utilizing Cronbach’s alpha coefficient, where values equal to or greater than 0.70 were considered acceptable. 36 Stability was evaluated through test–retest reliability over a two-week interval. The intraclass correlation coefficient (ICC) was calculated to quantify the test–retest reliability, with an ICC value of ≥0.75 considered indicative of good reliability. 37 According to the sample size recommendations proposed by Giraudeau and Mary for reproducibility studies, when the expected ICC exceeds 0.6 and 2 repeated measurements are conducted (P = 2), a minimum total of 60 observations (np = 60) is advised, corresponding to a sample size of at least 30 participants (n = 30). 38
The Brief A-ADS
The Brief A-ADS is a 13-item scale designed to assess adolescent attitudes toward dementia, with 3 dimensions: perceptions of dementia, empathy toward individuals with dementia, and personal sacrifice. Developed from the original 23-item A-ADS, it has demonstrated strong internal consistency (Cronbach’s α = 0.88) and model fit indices (CFI = 0.90).23,25 The Brief A-ADS employs a 5-point Likert scale, with higher scores indicating more positive attitudes. This concise format enhances its applicability in time-limited settings, such as schools. The scale has been validated in various cultural contexts, including Malaysia, and Pakistan, with consistently robust psychometric properties.24,26
Statistical Analysis
Statistical analyses were performed utilizing SPSS version 28.0 and AMOS version 26.0, with the threshold for significance established at P < .05. Descriptive statistics (eg, means, standard deviations and percentages) and inferential statistics (eg, Cronbach’s α, ICC, statistics used in the EFA) were used as described above. AMOS version 26.0 (IBM SPSS Inc) was used for the CFA.
Ethical Considerations
This study was granted ethical approval by the Ethics Committee of Kiang Wu Nursing College of Macau (reference: REC-2023.0701) and the Medical Ethics Committee of Shenzhen University (reference: PN-202400133). Authorization to utilize the study instruments was secured from the original author. Prior to completing the questionnaire, all participants provided informed consent. They were explicitly informed that their participation was voluntary and anonymous, and that their privacy would be rigorously safeguarded. Furthermore, participants were assured that all data collected would be used exclusively for research purposes and would be accessible solely to the research team.
Results
Phase 1: Translation, Content and Face Validation
The Brief A-ADS was translated from English to both traditional Chinese and Simplified Chinese. For content validation, the 6 healthcare and social science experts commented that the scale was satisfactorily relevant, as reflected by a S-CVI of 0.99 and I-CVI of 0.83∼1. For face validation, 12 college students (5 in Macao and 7 in Shenzhen) aged 19∼24 years commented that the Brief AADS-C items were comprehensible, yielding a comprehensibility and interpretability rating of 100%. Additionally, 50 participants in the pilot study completed the questionnaire without difficulty, and no further improvements were suggested.
Phase 2: Psychometric Testing of the Brief AADS-C
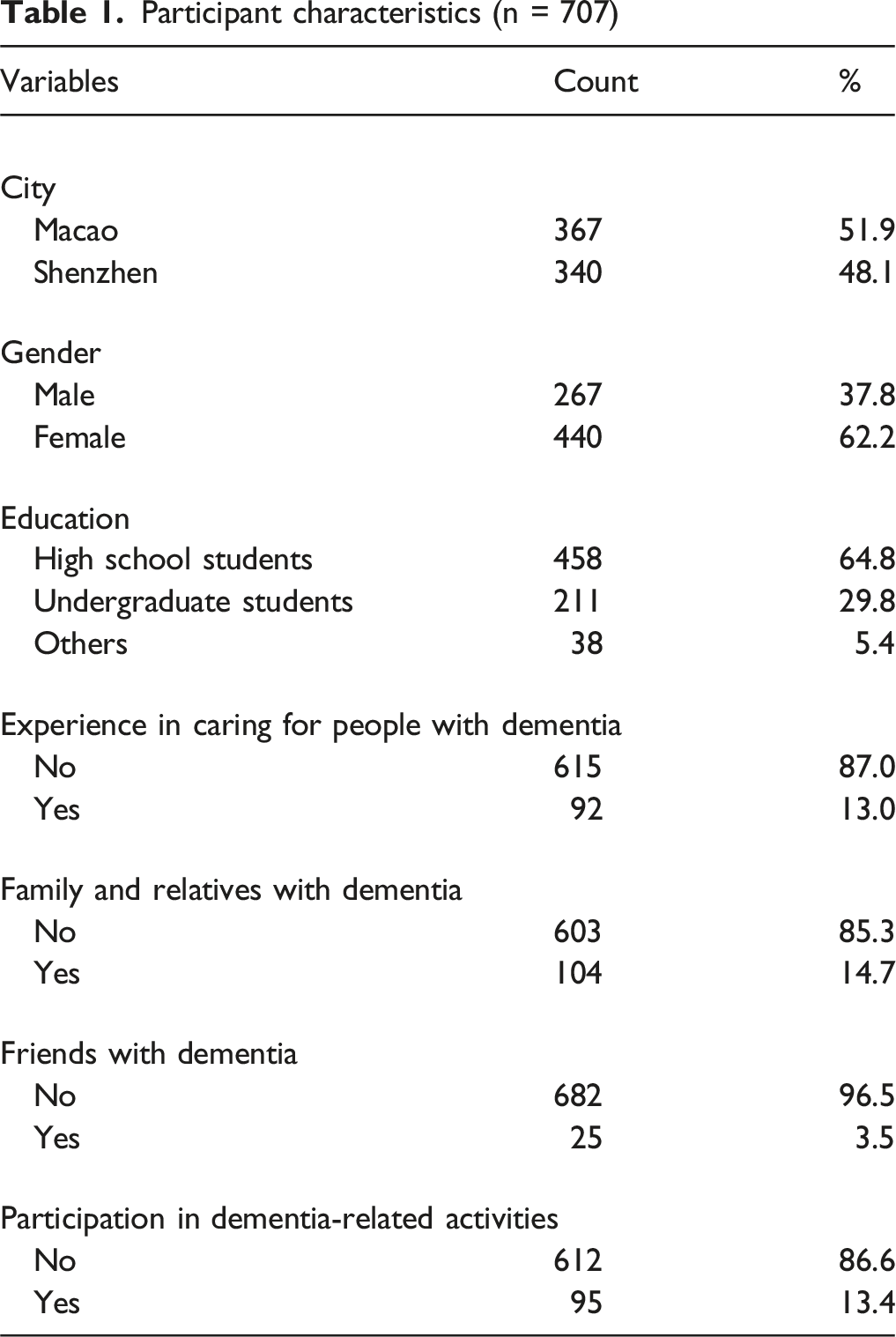
Participant characteristics (n = 707)
Exploratory Factor Analysis of the Brief AADS-C (n = 353)

CFA with the 354 remaining datasets was conducted to assess the validity of the three-factor solution for the Brief AADS-C with 11 items (Figure 1). The three-factor solution demonstrated a good model fit (χ2/df = 3.076, GFI = 0.937, CFI = 0.915, SRMR = 0.0579, RMR = 0.031, RMSEA = 0.077). Most items loaded significantly onto their respective factors (factor loadings ≥0.4), except for 2 items (Item 9 = 0.34, Item 12 = 0.33). Confirmatory Factor Analysis of the Three-Factor Structure of the Brief AADS-C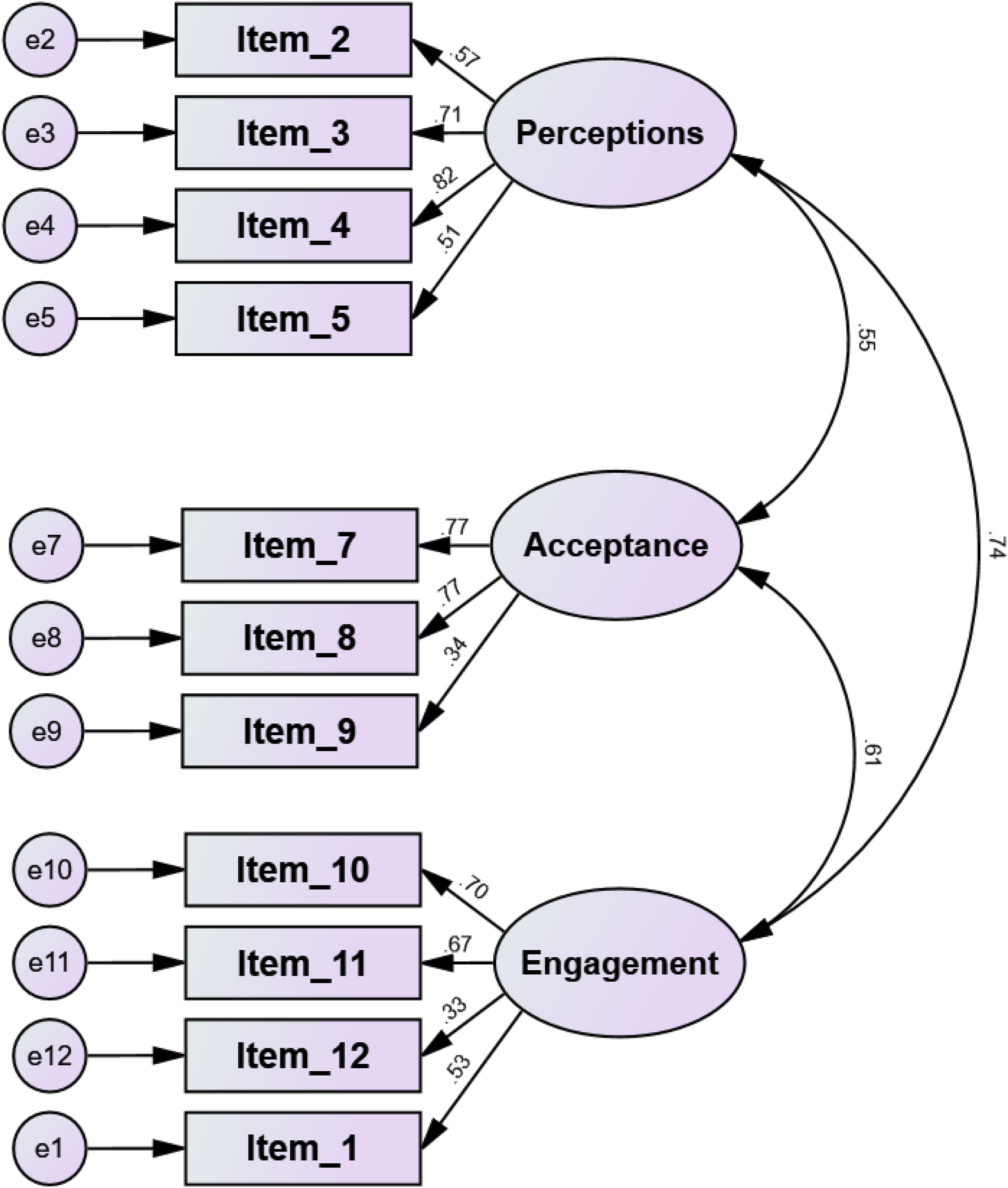
The Brief AADS-C demonstrated good internal consistency, with an overall Cronbach’s α of 0.814. Subscale Cronbach’s α values ranged from 0.653 to 0.775, indicating acceptable reliability. Test-retest reliability was also satisfactory (ICC = 0.647, P < 0.001).
Discussion
This study is the first to translate and validate the Brief AADS in a Chinese context. Following rigorous translation and validation process, the scale demonstrated satisfactory reliability and validity among adolescents aged 15-24. The findings provide robust support for the applicability of the Brief AADS-C as an appropriate instrument for assessing dementia-related attitudes in Chinese-speaking youth populations.4.1 Psychometric properties
The content validity of the Brief AADS-C was excellent, with I-CVI ranging from 0.83 to 1.00 and an S-CVI of 0.99. These findings indicated that the translated items were relevant and culturally appropriate for the target population. 29
EFA identified a three-factor structure—Perceptions, Acceptance, and Engagement—accounting for 56.07% of the total variance. This deviates from the unidimensional structure of the original English version 25 and reflects potential cultural differences in how Chinese youth conceptualize dementia-related attitudes. This multidimensional approach reflects a richer interpretation of adolescent attitudes, capturing not only general perceptions but also emotional openness and willingness to act. Notably, the Engagement dimension, which includes behavioral intentions such as volunteering or helping, is largely absent in other tools (eg, the Scale of Attitudes toward People with Dementia and their Care 18 ). The Brief AADS-C captures adolescents’ potential roles as future advocates or informal supporters, aligning well with dementia-friendly community objectives.2,3 Despite the promising results, Items 6 and 13 exhibited factor loadings below the acceptable threshold (0.31 and 0.29, respectively). Item 6 (“It is rewarding to work with people who have dementia”) may lack relevance for adolescents with limited working exposure. This suggests potential misalignment with the target population’s lived experience. Item 13 (“I would feel uncomfortable being around people with dementia”®) may demonstrate conceptual overlap with Item 4 (“It is possible to enjoy spending time with people with dementia”), creating redundancy. Moreover, the remaining Perception items (Items 2-5) collectively explain 37.13% of variance, indicating comprehensive coverage of this dimension without Item 13.
Furthermore, CFA supported the three-factor solution with acceptable model fit indices (χ2/df = 3.076, GFI = 0.937, CFI = 0.915, SRMR = 0.0579, RMR = 0.031, RMSEA = 0.077). 35 However, items 9 and 12 exhibited factor loadings below 0.40, a common occurrence in scale translation studies due to cultural and demographic diversity.39,40 The low loading of item 9, “I admire how people with dementia deal with things,” may be attributed to cross-cultural differences in the interpretation of the term “admire.” In Chinese cultural contexts, the sentiment may be more accurately captured by the term “respect” rather than “admire,” reflecting a subtler but meaningful distinction in attitudinal expression. In contrast, item 12, which is reverse-scoring and features a relatively long and syntactically complex structure, may have impeded adolescents’ comprehension, thereby diminishing its factor loading. This finding highlights the need for further validation of the Chinese version of the scale across diverse populations to ensure its robustness and applicability.
The reliability of the Brief AADS-C was satisfactory, with an overall Cronbach’s alpha coefficient of0.814 and subscale coefficients ranging from 0.653 to 0.775. These values met the threshold of 0.70 recommended by Streiner 36 and indicated good internal consistency. The test-retest reliability (ICC = 0.647) indicated a moderate level of stability; however, it fell below the commonly accepted threshold of 0.75 for good reliability. 37 This result contrasts with the higher test-retest reliability (r = 0.78) reported for the original Brief A-ADS. 41 Several methodological factors may account for this discrepancy. First, potential conceptual non-equivalence during translation may have compromised item comprehensibility (eg, Item 9: “I admire how people with dementia deal with things”). Second, environmental inconsistency between test administrations—initial assessments conducted at home vs retests in classroom settings—could introduce attention bias. These observations suggest that further studies are needed to work on this issue.
Comparison With Existing Measures
Compared to existing dementia attitude scales, the Brief AADS-C demonstrates superior applicability for adolescents by incorporating age-appropriate language, relevant situational contexts, and a concise format. Traditional scales such as the DAS, 15 and the Dementia Public Stigma Scale 19 were designed primarily for adults or healthcare professionals and tend to emphasize cognitive knowledge or public stigma. While they provide robust psychometric properties in adult populations, their use among adolescents is limited by item complexity and a lack of developmental alignment. In contrast, the Brief AADS-C addresses the unique cognitive and emotional characteristics of adolescents aged 15-24, allowing for more accurate and meaningful assessment of their attitudes in educational and community-based settings. Its brevity (11 items) also improves feasibility in time-restricted contexts such as school programs or public health outreach.
Though the Brief A-ADS has been validated in Malaysia 24 and Pakistan, 26 this study reveals a distinct factor structure in the Chinese context, supporting findings from previous cross-cultural validations that emphasize the influence of sociocultural norms on scale interpretation. 27 . Items within the Brief AADS-C were revised to align with local expressions and tested through the face validity and pilot testing, ensuring semantic and contextual relevance. These adaptations not only enhance construct validity but also facilitate the scale’s integration into school-based health education and national dementia policy assessments in Chinese-speaking regions.
Implications for Practice and Research
The validated Brief AADS-C represents a significant advancement in dementia education and research within Chinese-speaking regions, providing a culturally relevant and adolescent-specific instrument for assessing attitudes and evaluating educational interventions. Adolescents constitute a vital demographic for dementia-friendly initiatives, as their formative and adaptable attitudes have the potential to influence future societal perceptions. 42 However, there is a scarcity of validated instruments specifically tailored for adolescents. Thus, the validated Brief AADS-C can address the research gap.
Additionally, the validated Brief AADS-C can help promote the dementia awareness and friendliness initiatives within Chinese-speaking regions. By enabling the evaluation of educational initiatives, the Brief AADS-C addresses gaps in adolescent-targeted research. 27 Studies have demonstrated that adolescent-focused interventions can significantly reduce stigma and foster empathy and social acceptance. 25 Programs such as the UK’s “Dementia Friends” and Australia’s intergenerational initiatives have shown success in shifting attitudes and provide adaptable models for the Chinese context. 12 Some innovative approaches like Time for Dementia Programme conducted in some western countries demonstrated to be effective across professional training among university students.43,44 However, these kinds of dementia awareness and friendliness initiatives among the youth are relatively scare in China. 14 Thus, the validated adolescent-specific instrument may be specifically applied in dementia awareness and friendliness promotion programs in settings such as schools, in line with the World Health Organization’s Global Action Plan and the National Dementia Strategies for Mainland China and Macau SAR.2,4
Limitation
Despite its significant contributions, this study has several limitations that warrant attention. First, the reliance on convenience sampling from 2 urban regions (Macao and Shenzhen) may restrict the generalizability of the findings to adolescents in rural or less-developed areas. Future studies are needed to employ this instrument in more diverse geographic and socio-economic populations. Second, the three-factor structure identified in this study differs from the unidimensional construct of the original scale, 25 suggesting potential cultural influences and raising questions about its cross-cultural comparability; further investigation into these differences is necessary. Third, items 6 and 13 exhibited low factor loadings, indicating the need for refinement or replacement to enhance the scale’s structural validity. Additionally, although the sample size was sufficient for EFA and CFA, broader and more heterogeneous samples are needed to enhance generalizability. Finally, the moderate test-retest reliability (ICC = 0.647) fell short of the recommended threshold of 0.75, potentially due to adolescents’ psychological variability or item-level limitations, indicating the need for further refinement and validation.
Conclusion
This study validated the Chinese version of the Brief Adolescent Attitudes towards Dementia Scale (Brief AADS-C), establishing it as a reliable and culturally relevant tool for assessing adolescent attitudes toward dementia in Chinese-speaking regions. The three-factor structure (Perceptions, Acceptance, and Engagement) reflects unique cultural interpretations, with robust reliability and structural validity supporting its application in both research and education. The Brief AADS-C addresses a critical gap in dementia education, enabling adolescent-targeted interventions to reduce stigma, enhance empathy, and foster DFCs. While minor limitations in item performance and convergent validity were noted, this tool offers valuable insights into adolescent attitudes and contributes to advancing dementia education strategies in alignment with global and regional health priorities. Future research should focus on refining item content, expanding population diversity, and conducting longitudinal studies to enhance the tool’s applicability and impact.
Footnotes
Acknowledgments
The authors express their sincere gratitude to the Macao Foundation for its financial support. They also wish to extend their appreciation to all respondents and investigators for their invaluable contributions to this research. Special acknowledgment is given to the participating schools for their assistance in promoting and disseminating the study. Additionally, the authors are grateful to the experts involved in translation, cultural adaptation, and content validation.
Ethical Approval
This study was granted ethical approval by the Ethics Committee of Kiang Wu Nursing College of Macau (reference: REC-2023.0701) and the Medical Ethics Committee of Shenzhen University (reference: PN-202400133). Authorization to utilize the study instruments was secured from the original author. Prior to completing the questionnaire, all participants provided informed consent. They were explicitly informed that their participation was voluntary and anonymous, and that their privacy would be rigorously safeguarded. Furthermore, participants were assured that all data collected would be used exclusively for research purposes and would be accessible solely to the research team.
Author Contributions
J. Wu conceptualized the study, prepared the initial proposal, and significantly contributed to the writing of the manuscript. Q. Wang participated in the study design, data collection, and revision of the manuscript. M. Tan, Y. Wen, and X. Gao contributed to the drafting of the manuscript. I. H. Wong, W. I. Lei, N. Liu, and I. K. Van were involved in data collection and manuscript revision. All authors have reviewed and approved the final version of the manuscript for publication.
Funding
The authors received financial support for the research, authorship, and/or publication of this article: This study was funded by Macao Foundation (Grant No.: 0544/DGAF/2024-02).
Declaration of Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All supporting data are incorporated within the manuscript and supplementary materials. Further data can be provided upon reasonable request to the corresponding author.