
Abstract
Dementia is attributable to 12 known risk factors in 40% cases. This study aimed to assess the prevalence of defined risk factors among people living with dementia. 174 patients with dementia and caregivers were interviewed using semi-structured pro forma, risk factors provided by the Lancet Commission on Dementia (2020), and Dementia Severity Rating Scale (DSRS). The prevalence of 11 known risk factors and associations between the risk factors and dementia severity were assessed. The mean age of the participants was 73.9 years (SD = 8.34 years). The education below intermediate level was 83.3%, 17.8% had hearing loss, 37.9% had hypertension, 24.1% had diabetes, 25.9% and 55.2% had alcohol and nicotine harmful use respectively and 8% had a history of traumatic brain injury and obesity each. There is a substantial prevalence of risk factors among people living with dementia in Nepal but no associations between any of the risk factors and dementia severity.
Introduction
Dementia is a general term for the new-onset problem of memory, language, behavior, problem-solving, and other thinking abilities that is severe enough to interfere with daily life. It is a syndrome of a chronic or progressive nature that leads to deterioration in cognitive function beyond what might be expected from the usual consequences of biological aging. 1 Worldwide around 50 million people live with dementia and this number is projected to increase to 152 million by 2050, particularly in low-income and middle-income countries (LMIC). 2 According to the 2001 census of Nepal, there was 6.5% (1.5 million) geriatric population (>60 years) which has increased to 10.2% (2.97 million) in 2021. 3 Dementia affects individuals, their families, and the economy, with global costs estimated to be about US$1 trillion annually 2 and contributes to 4.1% of total disability-adjusted life years (DALYs). 4 On the contrary, dementia is under-recognized, under-disclosed, undertreated, and undermanaged, particularly in LMICs, and considered a part of normal aging rather than requiring medical care. 5
Various risk factors are considered to be associated with an increased incidence of dementia. The 2020 report of the Lancet Commission on Dementia prevention, intervention, and care, has identified 12 modifiable risk factors of dementia, which include less education, hypertension, hearing impairment, smoking, obesity, depression, physical inactivity, diabetes, low social contact, excessive alcohol consumption, traumatic brain injury (TBI), and air pollution. These modifiable risk factors might prevent or delay up to 40% of dementia. 6
Given the expanding geriatric demographic in Nepal, pinpointing modifiable risk factors pertinent to this population may yield critical insights for public health interventions in resource-constrained environments. This research aimed to study the prevalence of modifiable risk factors of dementia among people living with dementia and its association with the severity of dementia. Knowledge about the prevalence of risk factors would help us to lay a baseline understanding for further research on the primary prevention of dementia in our setting. The number of published literature regarding pathways to care and risk factors of dementia in Nepal was scanty, to the best of our knowledge.
Methodology
This was a cross-sectional study conducted at Patan Academy of Health Sciences (PAHS) from April 2022 to March 2023. The main objective of the study was to assess the prevalence of defined risk factors among people living with dementia attending Patan Hospital in 1 year. The out-patient department (OPD) and in-patient cases, diagnosed as dementia by consultant psychiatrist as per ICD 10 criteria were included. The only exclusion criterion was the refusal of written consent by participants or caregivers. Over 1 year, 174 people living with dementia were interviewed and included in the study. Approval of the study was obtained from the Institutional Review Committee (IRC) of PAHS (Ref: PMS2203041595). The participants and their caregivers had the study explained to them in detail before obtaining the informed written consent. For informed written consent, a generic PAHS consent form in Nepali was used. If participants wished, they were allowed to withdraw at any time without any reason. We guaranteed the confidentiality of all the participants. They were interviewed using semi-structured pro forma including the risk factors for dementia as provided by the 2020 report of the Lancet Commission on Dementia, and Dementia Severity Rating Scale (DSRS) was applied. DSRS has 12 items scored 0-3 to 0-6 in different items. The score is categorized as mild (0-18), moderate (19-36), and severe (37-54) dementia. 7 Data was analyzed using SPSS. Categorical data were presented in frequency and percentage while continuous data were summarized in mean and SD for parametric data or median with interquartile range for non-parametric data. The association between risk factors and the severity of dementia was explored and analyzed by using the Chi-square test or Fisher exact test. The P-value less than 0.05 was considered significant.
Result
The mean age of the participants was 73.9 years and most of them (73.6%) were between the age group of 60-80 years. The majority were male (51.7%), married (61.5%), and living in a joint family (77.6%). (Figure 1) Risk Factors Profile in People Living With Dementia Attending Tertiary Care Hospital (n = 174).
Association Between the Risk Factors and Severity of Dementia in People Living With Dementia Attending Tertiary Level Hospital (n = 174).
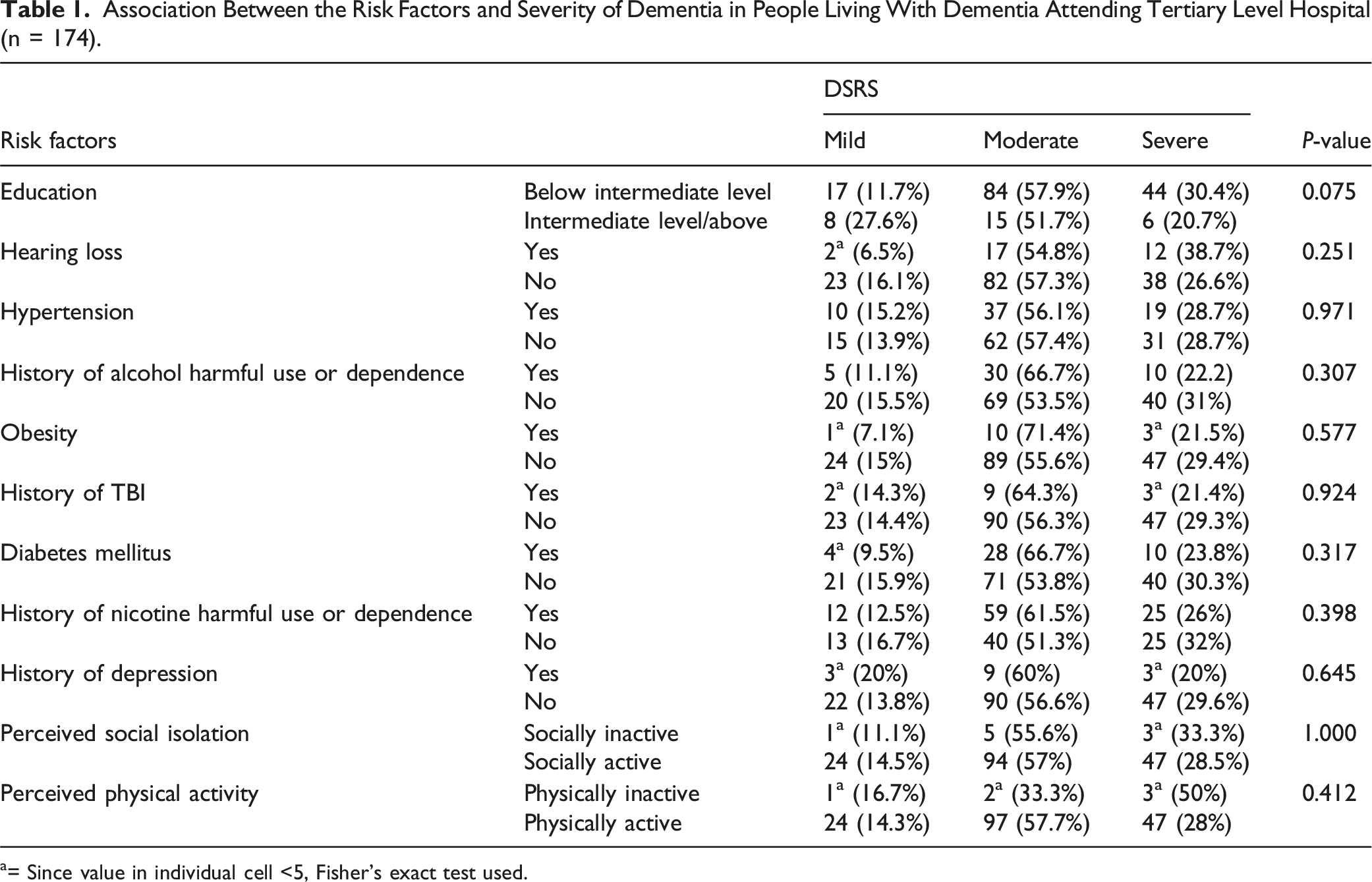
a= Since value in individual cell <5, Fisher’s exact test used.
Discussion
In this hospital-based cross-sectional study, the mean age of the participants was 73.9 years (SD = 8.3 years) which is comparable with other studies in Nepal and India. 8 The comparable age for patients in the Indian population could be because of our similarities in life expectancy and lifestyle.3,9 In a study done in the USA, the mean age was 83.1 years, which is higher than our study. 10 This can be due to the sample selection of advanced dementia, nutritional status, and life-expectancy differences.
The majority of the participants (77.6%) in this study were from a joint family (married couples and their children living in the same household, where all the men in the household are related by blood and the women are their wives, unmarried daughters or widows 11 ) which is per our socio-cultural background of staying in a joint family. In this study, most of the participants were married (61.5%) followed by widow/widower (37.9%) which was similar to other studies done in tertiary hospitals in Nepal and India.12,13
In this study, eleven risk factors were evaluated in the participants. Most of the participants (83.3%) were educated below intermediate (high-school) level. A similar finding was seen in a descriptive cross-sectional study done in an OPD of another tertiary care hospital in Nepal. 14 Most participants did not have formal education or were below intermediate level due to limited educational institutions during that time i.e. almost half a century back and socio-cultural factors like lack of knowledge of the importance of education. The higher the education, the higher the intellectual capacity, occupational complexity, and engagement in intellectually and cognitively stimulating activities, which increases the cognitive reserve and brain plasticity. 15
The prevalence of hearing loss in this study was 17.8%. In a study done in 2020, hearing loss accounted for 8.2% of dementia cases. 6 It is known that even subclinical levels of hearing impairment (below 25 dB) were related to lower cognition. 16 Timely treatment of hearing loss can reduce new dementia cases by 9.1%, the largest reduction among all known modifiable risk factors. 17
It was seen that 37.9% of the participants in our study had hypertension and were under medication, where the duration of hypertension was from 2 years to 43 years. A study done in India and USA showed hypertension prevalence to be 55.3% and 66% respectively.18,19 The difference might be due to help-seeking behavior, socio-economic and lifestyle factors. Midlife and late-life hypertension are associated with an increased risk of late-life dementia. 20 The mechanism is neurovascular damage, focal brain atrophy, β-amyloid, and tau neuropathology. 21 With proper treatment of hypertension, the incidence of cognitive impairment decreases (HR 0·8; 95% CI 0·7-1·0). 22
In this study, 42 out of 174 participants (24.1%) were diabetic for 1 to 39 years. A case-control study done in India showed 33.3% prevalence of diabetes in dementia cases. 19 An American longitudinal study showed the prevalence of diabetes in dementia to be 28%. 18 The variations might be due to eating habits, early recognition, and treatment of diabetes in other countries. The risk of dementia increases with the duration and severity of diabetes. 23 The underlying pathophysiology are vascular mechanisms, toxic effects of hyperglycemia/hypoglycemia, insulin resistance of the brain, formation of advanced glycation end products, and competition for insulin-degrading enzyme resulting in reduced degradation of -amyloid, but none of these has been proven unequivocally. 24
Obesity was seen in 8% of the participants at the time of presentation, which was similar even before the onset of dementia according to the caregivers. This finding is similar to a study from China where the prevalence of obesity was 9.5% in dementia patients. 25 In the English Longitudinal Study of Ageing (ELSA) 29.6% of dementia patients were obese. This difference might be due to eating habits and lifestyle differences. 26 Obesity is associated with brain atrophy, white matter changes, disturbances of blood-brain barrier integrity, and increased incidence of hypertension, diabetes, and coronary artery disease, which increases the risk of all-cause late-onset dementia. 27 Intentional weight loss in obese/overweight people is associated with improvements in performance across various cognitive domains and decreases the risk of dementia. 28
It was seen that 8% of participants in this study had TBI prior to the onset of dementia. A case control study done in India showed the prevalence of TBI in 15% of participants with dementia. 19 Similar to this study, a nationwide cohort study in Sweden showed the prevalence of TBI as a risk factor in 6.3%. 29 TBI increases the risk of dementia by widespread hyperphosphorylated tau pathology in the brain. 30
Among the participants, 25.9% fulfilled the criteria of alcohol harmful use or dependence in this study. In a case-control study in India, the prevalence was 19.3%. 19 In a nationwide retrospective cohort study done in France, the prevalence of alcohol use disorder was 38.9%. 31 The differences might be due to socio-cultural factors and the availability of alcohol. Alcohol is known to cause neurotoxicity, thiamine deficiency, and brain atrophy, leading to cognitive impairment and early abstinence can decrease the risk.32,33
Nicotine consumption was the most common modifiable risk factor, identified in 55.2% of subjects, including nicotine harmful use or dependence. A case-control study in India showed nicotine dependence or harmful use in 33.3% of cases. 19 The number is higher than alcohol consumption due to easy availability, consideration of nicotine as a non-psychoactive substance, and a significant number of females along with males, consuming tobacco. A population-based cohort study conducted in seven LMICs as part of the 10/66 Dementia Research showed no significant association between smoking and the onset of any dementia. 34 Smoking cigarettes causes oxidative stress and systemic inflammation, responsible for dementia in both active and passive smokers. 35 Early cessation of smoking is seen to decrease the risk of dementia in the future. 36
A history of depression diagnosed by health professionals prior to the onset of dementia was seen in 8.6% of the participants. Similar findings were seen in the Longitudinal Ageing Study in India (LASI) Wave 1 (2017-18) including 31 464 participants and in a nationwide study done in Sweden in 41 727 dementia patients.37,38 Depression can be a prodrome of dementia and there can be reverse causation between depression and dementia. 6 The possible mechanisms for depression to be the risk factor for dementia are hippocampal atrophy, increased amyloid plaques, pro-inflammatory changes in the brain, among others. 39 Adequate treatment of depression with SSRI reduces the risk and delay the progression of dementia. 40
Among 174 participants, 9 (5.2%) were identified to be socially isolated as perceived by the care-givers. The isolation was not due to socio-cultural aspects but individual preference. Social contact is accepted as a protective factor against dementia by enhancing cognitive reserve. At times, social isolation might also occur in the prodrome of dementia 6 which should be properly identified.
In this study, 6 participants (3.4%) were physically inactive as perceived by the caregivers. Exercise is associated with a reduced risk of dementia. 17 Aerobic exercise was seen to be better than resistance exercise and 30 minutes per day for 5 days in a week of moderate to vigorous exercise decreases the risk of dementia.41,42 These modifiable risk factors account for about 40% of worldwide dementias, which could theoretically be prevented or delayed. 6 The prevention strategy is more applicable in LMIC as many of the risk factors are more prevalent and dementia cases are ever-increasing in this part of the world.
The final objective of this study was to assess the association between risk factors and severity of dementia, where no statistically significant association was found. The risk factors were known to increase the risk of dementia 6 but as per this study, dementia severity was not associated with the risk factors profile. As such, on a thorough search in PubMed, Google Scholar, and NepJOL we could not find studies assessing the association between risk factors and dementia severity.
Strengths of the Study
This was a unique study in Nepal, as per the search in NepJOL, Google Scholar, and PubMed there have been no studies assessing the aforementioned risk factors profile, and association of risk factors with the severity of dementia, done in Nepal. The participants were diagnosed by consultant psychiatrists using ICD-10 criteria making the diagnosis reliable. The use of DSRS with good psychometric properties and consideration of risk factors as provided by 2020 report of the Lancet Commission on Dementia made the study more objective. The sample size was also adequate as per the prevalence of dementia in a previous study done in Nepal.
Limitations of the Study
There were some limitations in this study. This is a cross-sectional study conducted in a tertiary hospital, so the results of the study cannot be applied to the general population. The sampling method used was convenience sampling, which could have led to selection bias, perhaps failing to represent the wider population of people living with dementia in Nepal. This is neither a cohort nor a case-control study, so attributable risk could not be determined. There could be recall bias in reports of the caregivers regarding past facts, for example, onset, duration, and presence of risk factors (though physician records corroborated most). The risk factors were not analyzed with types of dementia. Similarly, the exploration of risk factors associated with dementia severity was not adjusted for age of the patient or time since diagnosis. Regarding obesity, we had to measure current BMI and ask caregivers if it was similar in the past which could have been different and caused the bias in the results. Physical activity and social isolation were quantified as per the caregivers’ perception which doesn’t have a good validity as compared to the real-time measure. Though the scales used have good psychometric properties, they were not validated in the Nepalese setting. Among 12 risk factors discussed by the 2020 report of the Lancet Commission on Dementia prevention, intervention and care, we included only 11, excluding “air pollution”, as there was no reliable way to quantify air pollution and the residence of the participants would change often.
Conclusion
In this study, we assessed the risk factors profile of people living with dementia who presented to a tertiary care hospital and also assessed the association between risk factors and the severity of dementia. Majority of the participants were male, married, between 60-80 years age group, living in a joint family and taken care by their children. All the studied risk factors were prevalent in our sample. The significant prevalence of modifiable risk factors such as lower education, smoking and hypertension highlights the necessity for targeted public health interventions aimed at early prevention, particularly in resource-constrained environments like Nepal. The majority (56.9%) of the participants had moderate severity of dementia according to the DSRS score. The risk factors were common in the sample, but there was no association between the risk factors and dementia severity.
Recommendation and Future Direction
Early identification and prevention or management of risk factors can prevent dementia significantly and minimize the social and economic burden of care. It is more applicable to the LMIC like ours, as the greying population is ever increasing and treatment gap is high. There should be specific policy from the government to assess the risk factors in mid-life and cognitive impairment in late-life, so that early identification and management of risk factors could be done. To get a better understanding of the risk factors and dementia, we recommend cohort studies/RCTs, multi-centric studies in the general population and in the community, to generalize the result. This study can be a foundation for further research on risk factors in people living with dementia in Nepal and formulation of National dementia care plan.
Footnotes
Acknowledgments
To the entire department of psychiatry of PAHS and all the participants of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
Data will be shared upon reasonable request by the corresponding author.