
Abstract
Motor inactivity is typical in the later stages of Alzheimer’s disease although there is evidence that physical exercise can reduce depression and enhance performance of daily activities. The aim of this study was to determine whether a walking program could reduce the functional and cognitive decline of elderly nursing home residents in the later stages of Alzheimer’s disease. A total of 21 patients (84 ± 5 years) were randomly assigned to a walking program (WG) or to a control group (CG). A 6-minute walking test (6WT), the Barthel index of activities of daily living (ADLs), and Mini-Mental State Examination (MMSE) tests were performed before and after 24 weeks of the program. The WG showed significant improvement in the 6WT (20%) and ADLs (23%), while the CG decreased in MMSE (−47%), the WG had a slower decline (−13%). This study indicates that it is possible to stabilize the progressive cognitive dysfunctions in nursing home residents with Alzheimer’s disease through a specific walking program.
Introduction
Today, one of the main purposes of institutional long-term care is to offer complete and combined therapy intervention that can enhance nursing home residents' functional abilities. New integrated clinical approaches concerning physical exercise and Alzheimer’s disease (AD) have recently received attention in the scientific literature. 1 Although physical exercise enhances and maintains benefits on general heath, quality of life, and physical fitness in the older population,2–4 there is also evidence indicating cognitive advantages for older adults 5 with mild cognitive impairment.
Previous randomized control trials have reported that it is possible to get people with mild cognitive impairment6,7 to exercise. Studies on people with moderate dementia have described numerous positive effects of physical exercise and walking programs: improvement in walking endurance, better urinary continence, enhanced communication, reduced depression, and an increase in activities of daily living (ADLs).8–10 Other studies have shown that physical exercise alleviates certain symptoms of early dementia and biomarkers of AD, and improves health and quality of life.2,3,11–13
In a 12-month multicenter, randomized, controlled study, Rolland et al 14 provided evidence that a moderate exercise program carried out twice a week significantly slowed the progressive deterioration in their ability to perform ADLs in people with moderate AD residing in nursing homes; but the authors pointed out the problem of low adherence to the exercise program in this population. On the other hand, Teri et al 15 reported positive adherence to an integrated program (exercise and behavioral management) designed for people with dementia, carried out with the participation of caregivers. The participants increased their physical activity level, decreased their rates of depression, and improved their physical health and functions.
The overall importance of physical exercise in persons with cognitive impairment was recently emphasized in a meta-analysis, 16 which reported the positive effects of different kinds of exercise interventions on individuals with dementia. However, only 13% of the selected studies were done on individuals with severe cognitive impairment. Exercise programs for persons at later stages of AD are very difficult to carry out because their anxiety, sadness, anger, and behavior disturbances are difficult to manage. However, Edwards et al 17 demonstrated the feasibility of an exercise program for individuals with severe dementia and mobility limitations. Despite these encouraging reports, some clinical trials emphasized caution regarding these positive conclusions because physical activity, per se, induces only modest improvement in the cognitive performance of adults with advanced dementia.11,18
Therefore, the aim of this study was to determinate whether an institution-based walking program carried out together with family member caregivers could reduce the functional, cognitive, and physical decline of nursing home residents in the later stages of AD. The walking program was compared with routine care in a randomized controlled clinical trial.
Methods
Eligible individuals were among nursing home residents of an Alzheimer’s care unit (ACU) at the Mons Mazzali geriatric institute. Inclusion criteria were 65 years of age or older, dependent on assistance in 2 or more personal ADLs according to the Barthel index, 19 Mini-Mental State Examination (MMSE) 21 maximum score of 15 and minimum of 5, and absence of mobility limitations, minimum score of 23, according to the Performance Oriented Mobility Assessment (POMA) index, 21 and constant oxygen saturation during walking (SpO2 > 85%). According to the clinical dementia rating scale, 22 all nursing home residents had to be in the later stages (CDR3-CDR4) of AD. 22
Participant Recruitment
Based on the inclusion criteria, 35 participants (5 men and 30 women) were selected from the ACU of the geriatric institute. Caregivers of the ACU residents were relatives who received written and oral information about the study. Three caregivers declined and were excluded from the study; 32 residents and their family caregivers accepted to participate and gave their written informed consent. The University of Verona, Department of Neurological, Neuropsicological, Morphological, and Motor Sciences Institutional Review Board and Mons Mazzali Ethical Committee approved the study.
A multidisciplinary diagnostic evaluation team reviewed the clinical files of the 32 selected residents and excluded 7 (5 men and 2 women) because of severe heart disease, and another 1 due to reduced oxygen saturation during the walking test. The staff team also made a record of anthropometrics, walking abilities, diagnoses, current medication, and clinical characteristics of the participants, as well as of physiotherapy and organized leisure programs that were regularly offered to the nursing home residents (Table 1).
Participants at Baseline Characteristics a
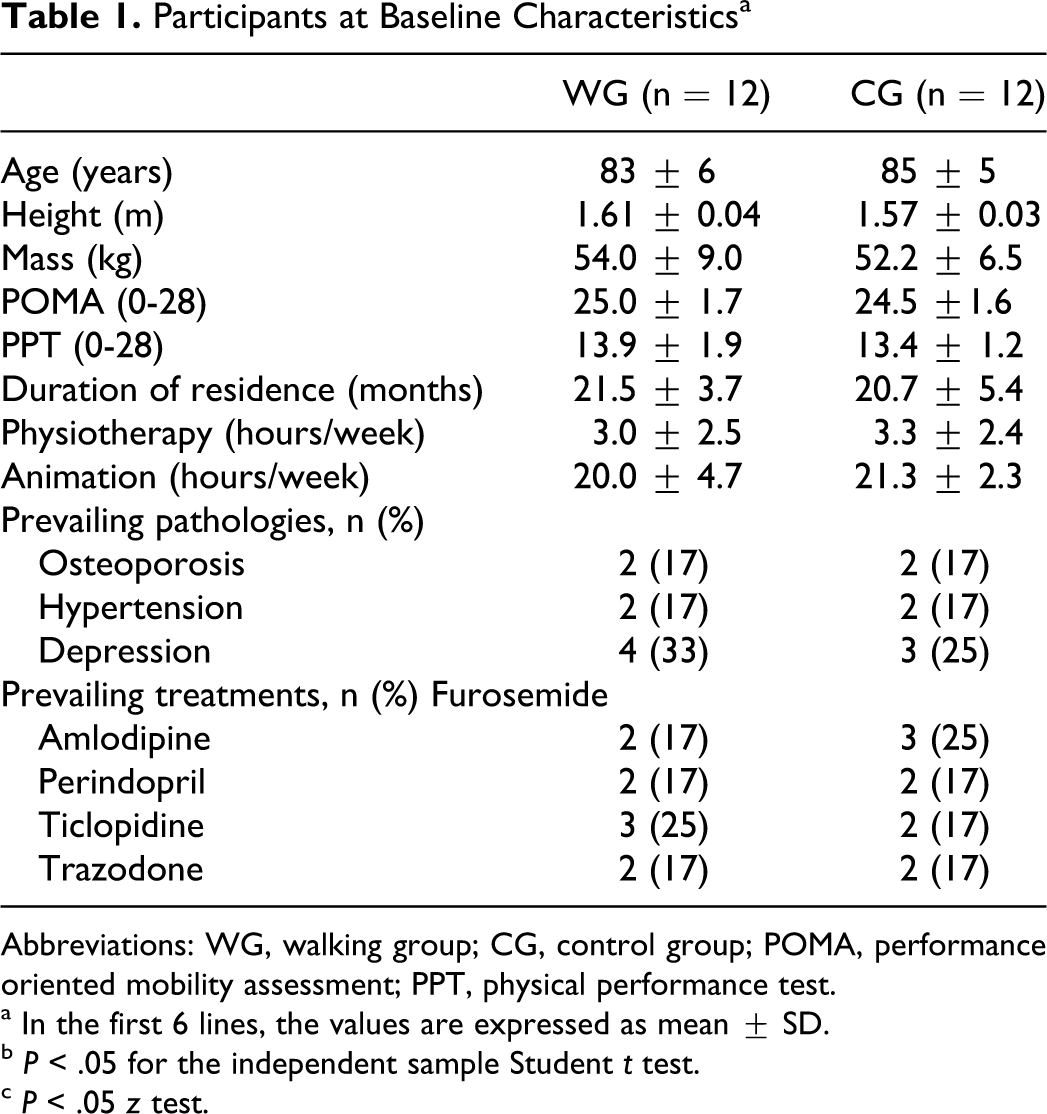
Abbreviations: WG, walking group; CG, control group; POMA, performance oriented mobility assessment; PPT, physical performance test.
a In the first 6 lines, the values are expressed as mean ± SD.
b P < .05 for the independent sample Student t test.
c P < .05 z test.
Measures
The multidisciplinary staff was involved in recording medical measurements: diastolic and systolic blood pressures were measured on 2 different days, using a standard sphygmomanometer device (Heine G7, Germany); the average blood pressure was then recorded, and at the same time fasting glycemia was assessed using a portable glycemic analyzer (Accu-Chek compact plus, Roche, Germany). Anthropometric measures (body mass, height, and weight) were determined using a professional mechanical scale fitted with a stadiometer (Seca mod. 713; III_M; Seca Medical Scales and Measuring Systems, BirminghamUK). The medical staff took these measurements in the rehabilitation unit of the nursing home, in the morning and 24 hours before the residents' last defecation.
A psychologist, specialized in neuropsychology, analyzed global cognitive functions of the participants through the MMSE. 20 This assessment was done in the morning in an appropriate room of the ACU. A physiotherapist evaluated the nursing home residents' gait/balance performance using the POMA test 21 and physical functions using the physical performance test (PPT) 23 ; these assessments were done in the rehabilitation center of the nursing home. An expert nurse (not from the same special care unit) estimated the nursing home residents' ADLs using the Barthel index. 19 The evaluation of the residents' ADLs was done by observing each resident’s daily activities (eating, bathing, grooming, dressing, bodily functions, transfers from bed to chair, mobility on level planes, stairs, and getting on/off the toilet), during the morning activities between 7.00 and 12.00.
An expert kinesiologist, specialized in adapted physical activities for older adults, evaluated the ACU residents' walking performance using the 6-minute walking test (6WT). The test was done according to a standardized protocol 24 using the special care unit hallway of 60 m. The kinesiologist followed the participants during the 6WT, maintaining a minimum distance from the participant of 0.5 m, and encouraging them with standardized statements. An electronic lap counter and timer were used to count the number of laps completed during the 6 minutes; and a handheld pulse oximeter (Vital test, Edan, China) was used to monitor the participants' oxygen saturation.
The collected information was recorded on a spreadsheet; an evaluation was done before and after the experiment period in a blind way and the members of the research team did not know to which group each participant had been assigned. The head nurse of the ACU (not involved in the residents' assessments) did the participants' randomization using StatPlus for Macintosh, version 2009 (AnalystSoft Inc, Alexandria, Virginia). No one on the research team was present during the walking exercise (afternoon); however, the head nurse of the ACU was always present. Before each intervention she checked the participants' health status and their ability to walk that day (exclusion criteria were fever, constipation treatment, low blood pressure, or other serious medical conditions). Caregivers kept a special log where they recorded the daily distance covered during the walking session. All the logs were kept in the ACU and filled out after each visit by the caregivers. Besides distance they recorded how long the walking session lasted and the number of laps.
Caregivers
The eligible caregivers were partners or adult relatives who habitually frequented the ACU a minimum of 4 days a week and spent at least 1 hour with the nursing home resident each time. General characteristics of caregivers assigned to the walking group were age 54 ± 8 years, 8 women, and 4 men. Of the 12 caregivers, 2 were husbands, 1 was a wife, and there were 9 sons and daughters. Of the control group, the main age of the caregivers was 50 ± 12 years, 7 women, and 5 men. Of the 12 caregivers, 1 was a husband, 1 was a wife, and 10 were sons or daughters. The same caregiver followed the same nursing home resident during the 6-month program.
Study Overview
Following the baseline assessments, residents and caregivers were both randomly assigned to either the walking group (WG) or the routine care control group (CG; Figure 1). The exercise program began 1 week after baseline evaluation and ended after 24 weeks. Postwalking session evaluations were done the following week.
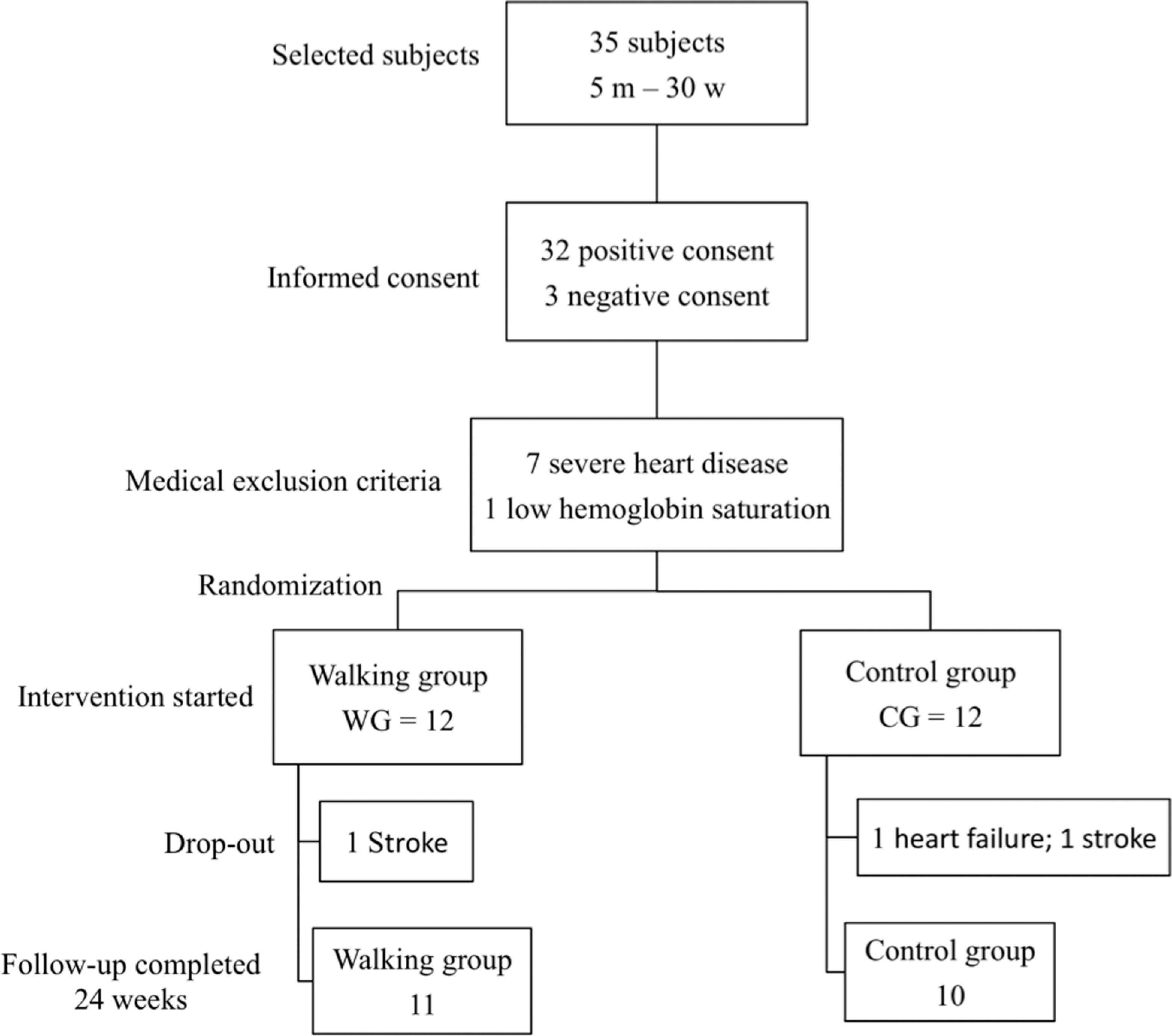
Study overview. m = man; w = women.
Exercise Program
Nursing home residents and caregivers assigned to the walking program received detailed instructions from the research staff; exercise time and the walking modalities were demonstrated and tried before the intervention period in the presence of a physiotherapist. For the residents' safety, caregivers were instructed to maintain a constant walking speed and to avoid accelerating or stopping, but to try, if possible, to understand the participant’s own pace each time. To do this, the walking session times and number of laps were recorded in the log and checked before and after each visit.
The goal of our study was to involve AD nursing home residents in a minimum of 30 minutes of moderate exercise (walking) 4 times a week; the program consisted of a simple aerobic walking activity. When the caregiver arrived at the ACU, he or she met the resident in the adapted living area, usually between 3 and 5
Statistical Analysis
Statistical analysis was done using StatPlus for Macintosh, version 2009 (AnalystSoft Inc). The independent sample t test and z test were used to compare values between the WG and CG groups. Analysis of variance (2-way ANOVA) with a df of 1 for time, 1 for group, 1 for time × group, with a residual of 38, and a total of 41. Tukey all pairwise multiple comparison procedures were used to test the effects of training; a P value below .05 was considered statistically significant.
Results
Characteristics of Participants at Baseline
At baseline, the WG and the CG showed no significant differences in any characteristics such as age (t test P = .9), length of time in the residence ACU (t test P = 0.8), physiotherapy (t test P = .7), and participation in organized activities (t test P = .8; Table 1).
Compliance to the Walking Program
The walking group had a 93.4% ± 3.2% presence at the 96 scheduled training sessions (90 ± 2 training days); individual numbers of visits during the 24 weeks of the program are shown in Figure 2, panel B. The most common reason for not participating in a walking session was constipation treatment. No adverse events related to the exercise program were observed during the experiment period nor did any event influence participation in the sessions. One woman in the walking group left the study after 6 weeks due to a serious medical condition (stroke); 2 people in the control group (reduced from 12 to 10 participants) also left the program because of serious health problems (heart failure and stroke).
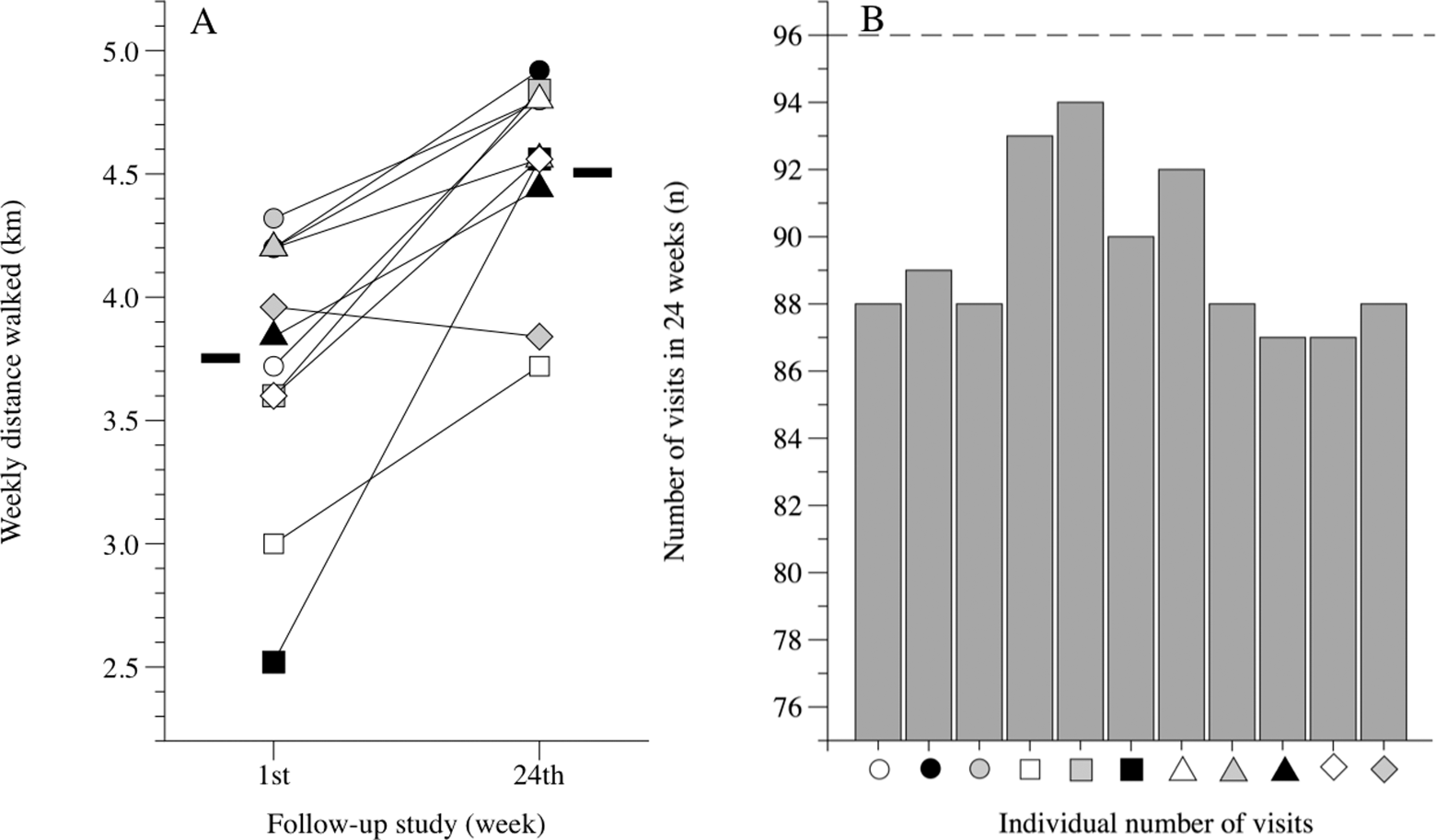
Data from caregivers' logs. Panel A, Individual and group mean (-) weekly distances covered during the 1st and 24th week of the walking program by Alzheimer’s disease (AD) nursing home residents and caregivers. Panel B, Individual number of visits during the program. Dotted line in panel B represents the maximum number of scheduled visits.
Walking Performance
Although the main effects of the walking program cannot be properly interpreted because the size of one factor's effect depends on the level of another factor, our data indicate that there was a statistically significant interaction between groups and time (P < .001): the statistical power performed (α = .05) for groups was 1.00 to 0.05 for time and 0.997 for groups × time. At baseline, the distance measured during the 6-minute walk test was WG 245.4 ± 30.9 m vs CG 238.5 ± 47.1 m. After the activity program, the WG showed a significant improvement in walking performance, whereas performance declined significantly in the control group (Table 2); pre-/postindividual changes are shown in Figure 3, panel A. The weekly distance covered during the 4 sessions of the 30-minute walking program significantly improved for the WG in 24 weeks (1st week 3.7 ± 0.6 km vs 24th week 4.5 ± 0.4 km; t test P < .001). Individual and group mean data are shown in Figure 2, panel A.
Biomedical and Cognitive Results a
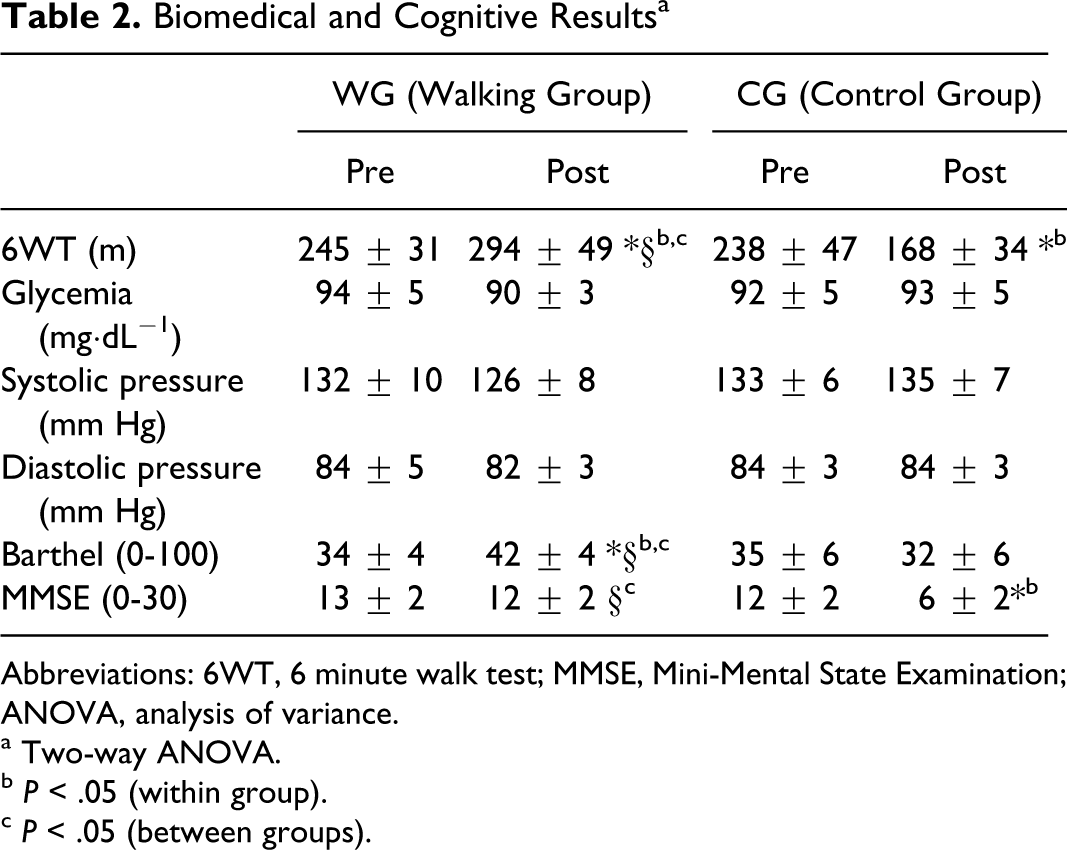
Abbreviations: 6WT, 6 minute walk test; MMSE, Mini-Mental State Examination; ANOVA, analysis of variance.
a Two-way ANOVA.
b P < .05 (within group).
c P < .05 (between groups).
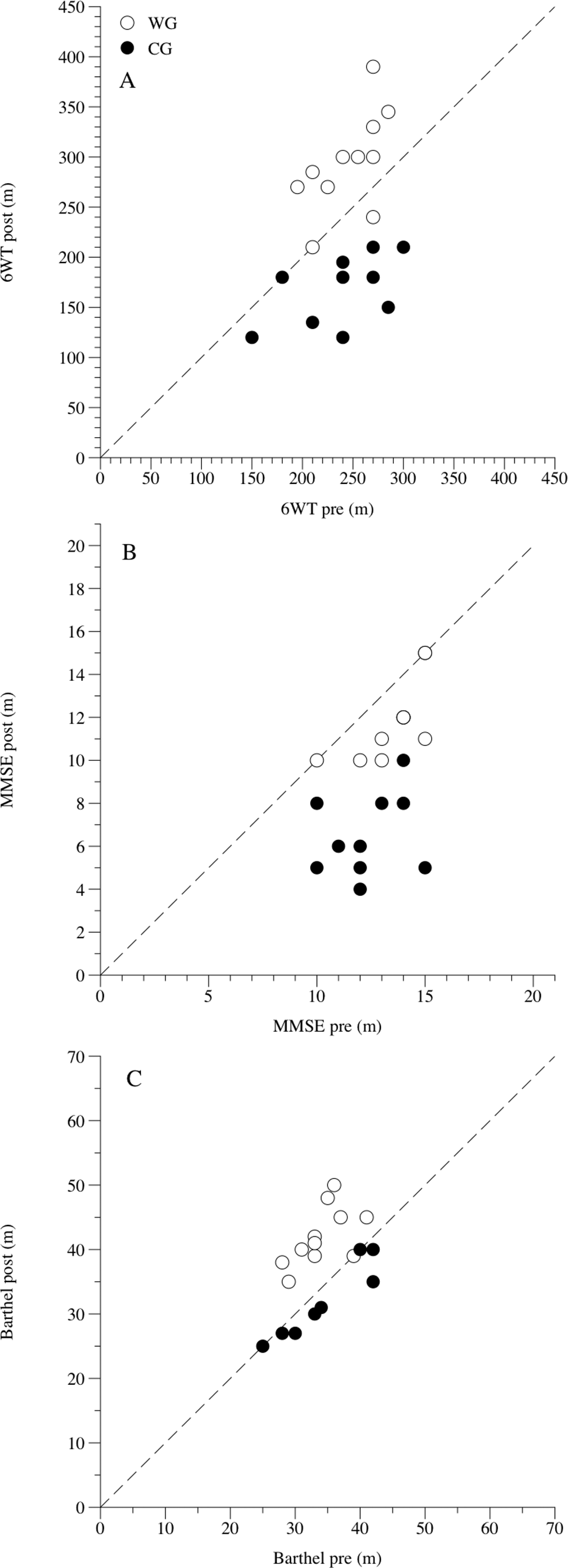
Individual changes after the 6-month walking program. Panel A, Individual changes in the 6-minute walk test (6WT). Panel B, Individual changes in cognitive performance (Mini-Mental State Examination [MMSE]). Panel C, Individual changes in the activities of daily life (Barthel). Open circles represent the walking group (WG) and dark circles the control group (CG).
Biomedical Outcome
The difference in the mean values of fasting glycemia among the different levels of groups and time were not statistically significantly different (P = .784 and P = .345, respectively), and there was no statistically significant interaction between groups and time (P = .143). The statistical power was .05 for both groups: .05 for time and .179 for groups × time. Also mean difference in values of systolic blood pressure among the different levels of groups and time was not great enough to exclude the possibility that the difference was simply due to random sampling variability (P = .054 and P = .368); and there was no statistically significant interaction between groups and time (P = .108), with a statistical power for groups = .37, .05 for time, and .232 for groups × time. Finally, there was also no mean statistically significant (P = .550 and .334) difference in diastolic blood pressure between groups and time (P = .376). The statistical power performed for groups was .05; .05 for time; and .05 for groups × time. Mean biomedical data are presented in Table 2.
Cognitive Function and the Barthel Index for ADLs
Because the size of a factor's effect depends on the level of another factor, the main effects of the walking program on MMSE scores cannot be properly interpreted. However, there was a statistically significant interaction between groups and time (P < .001). The statistical power for the groups was 1.0, 1.0 for time, and .96 for groups × time. The average MMSE score at baseline was 15.5 ± 1.5 for the WG and 12.3 ± 1.7 for the CG. The walking group did not show a significant change in MMSE scores before and after the training period, whereas the CG group showed a decrease in MMSE scores during the same period (Table 2). Pre-/postindividual changes are shown in Figure 3, panel B. The level of other factors, such as the intervention, influenced the main effects on ADLs, but the interaction between groups and time was statistically significant (P = .003), with a statistical power of .73 for groups, .29 for time, and .85 for group × time. Scores of ADL at baseline were 34.1 ± 4.0 and 34.7 ± 6.1 for the WG and CG, respectively. Barthel index items: transfers (bed to chair, pre 4.1 ± 2.0 vs post 7.7 ± 3.4; P = .01), mobility on a level plane (pre 10.0 ± 0.0 vs post 13.2 ± 2.5; P = .002), and stairs (pre 3.2 ± 2.5 vs post 5.5 ± 1.5; P = .01) were positively influenced by the walking program. Thus, the WG showed significant improvement in Barthel index scores after the training period, whereas the control group maintained the same scores (Table 2). Pre-/post-individual changes are shown in Figure 3, panel C.
Discussion
According to the Italian epidemiological study “The ILSA study,” 25 the incidence of dementia in Italy is consistent with the results reported in the majority of population-based studies; however, the Italian population is one of the oldest in the world and the number of individuals with dementia is exponentially increasing. Considering this incipient problem, most Italian nursing homes are offering new therapy proposals that incorporate exercise activities. To demonstrate the feasibility and effects of these programs, we set up a walking program specially designed for patients with AD. Our data indicate that, with the cooperation of a family caregiver, a walking program can be successfully included in the care of nursing home residents with AD. Even considering the limited sample in our study, our preliminary results suggest that these people can increase their levels of physical activity and improve their physical performance and ADLs. While cognitive levels decreased in the control group during the 6-month experimental period, the nursing home residents enrolled in the walking group maintained their previous MMSE assessment values.
The walking program was successfully completed by elderly nursing home residents in the later stages of AD, who resided in a specialized ACU. Compliance to the program in our study (about 93%) appeared to be better than that reported in similar studies involving adults without severe dementia.10,26 Considering the later stage of AD in the population selected for our study, compared to previous studies, our results are highly relevant. This outcome was likely positively influenced by the decision to stroll inside the habitual residence as well as to ask the help of the caregivers. The caregivers appreciated this program because they were actively involved in the care of a family member that was institutionalized at the time of the program. Because the management of people with dementia is difficult in a home situation and the burden is usually on the shoulders of a family member caregiver,27,28 this burden seems to become lighter if the patient is institutionalized in a specific ACU.
Improvement in the 6-minute walk test distance (+20%) was completely different from the range (−2.5%; −20.9%) reported in a previous comparable study. 29 Despite the fact that our participants had greater cognitive limitations, the higher continuous participation in the walking program (90 of 96 training days), the frequency/week of exercise sessions, and the total distance covered during the 6 months of the study could explain this great difference.
The great variability of biomedical data and the small sample in this study surely influenced the biomedical outcomes; our interpretation of these results suggests that the walking program did not modify the most important cardiovascular risk factors (glycemia, systolic and diastolic blood pressure) in this population. The American College of Sport Medicine (ACSM) and American Heart Association (AHA) recommendations for physical activity and public health in older adults 30 state that physical activity plays a substantial therapeutic role in coronary heart disease, hypertension, peripheral vascular disease, diabetes, obesity, and high cholesterol. On the other hand, Eggermont et al 31 pointed out that cardiovascular risk factors could attenuate or reverse the positive effects of exercise on cognitive performance. Our data are partially in contrast with these investigations, but the slow walking speed recorded in our study could possibly influence the outcome.
Our data show that, after the training period, residents in the WG improved their ADLs, particularly in moving from bed to chair, as well as their mobility on level planes and on stairs. Previous studies reported similar improvement in ADLs after a training program,4,10 but those results were obtained in participants with mild cognitive impairment and not in the later stages of AD. Our data strengthen the notion of the positive effects of physical activity on ADLs also in severe AD nursing home residents.
Cognitive levels, evaluated by the MMSE test, remained unchanged during the walking program with no significant differences for the WG, while the control group showed a significant decrease in cognitive functions after 6 months. These results on the CG are partially in agreement with Musicco et al 32 who reported a decrease of 5 points or more in MMSE scores for 31% of participants with severe cognitive impairment. However, the follow-up of our study, 6 months compared with the 2 years reported in the literature suggests that the cognitive decline shown by the control group was greater than what is typical, though other factors and comorbidities could exacerbate this result. On the other hand, the temporary stabilization of progressive cognitive dysfunctions shown in the WG could be attributed to improvements in blood circulation in the brain and changes in neurotransmitter synthesis stimulated by the exercise sessions. 33 Considering that cerebrovascular dysfunction plays a determinant role in cognitive impairment in AD 34 and that neurovascular degeneration amplifies brain dysfunction by incident ischemia, exercise could be considered one approach to counteract dementia by improving cerebrovascular health.
Study Limitations
The main limitation of our study was the relatively small sample size; only 35 residents in the ACU were selectable for the study, and after the preliminary medical exclusion criteria, only 24 people met the criteria. Moreover, the dropout of 3 nursing home residents in the CG and WG reduced the sample size to 21 participants.
Conclusions
The preliminary data show that a walking program involving nursing home residents with advanced Alzheimer and their family member caregivers can stabilize, for a short period of time, the progressive, cognitive dysfunctions shown by MMSE scores and improve performance of ADLs. To our knowledge, this is the first study reporting the positive effects of exercise in patients with advanced AD, residents in special care units. However, future studies are needed that involve larger sample cohorts that can assess whether exercise has differential impacts on different cognitive domains, as has been suggested in research studies on older, healthy adults.
Footnotes
Acknowledgment
The authors wish to acknowledge the contributions of the special care unit head nurse Deborah Bianchi, the psychologist Dr Elena Rubino, and physical therapist Jessica Bertasini.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.