
Abstract
Introduction
Multimodal non-pharmacological interventions (MNPI) have been determined as effective in delaying cognitive deterioration. The effectiveness of timing of such interventions in elderly is less discussed. We compared the different effectiveness of MNPI in cognitive preservation in elderly subjects with and without dementia.
Methods
We enrolled volunteer the elderly subjects. Subjects were classified as dementia group and non-dementia group by instrument of ascertainment of dementia 8. All were assigned to attend 3 hours of MNPI (physical fitness training, Chinese capillary, and Chinese drawings and paintings) twice a week over a 16-week period. Neuropsychiatric tests, including Mini-Mental State Examination (MMSE), Cognitive Assessment Screening Instrument (CASI), clinical dementia rating (CDR), and neuropsychiatric inventory (NPI), were administered before and 1 year after MNPI. We demonstrated the changes of cognition and behavioral and psychological symptoms of dementia (BPSD) before and after MNPI. We compared the different effectiveness of cognition preservation between two groups.
Results
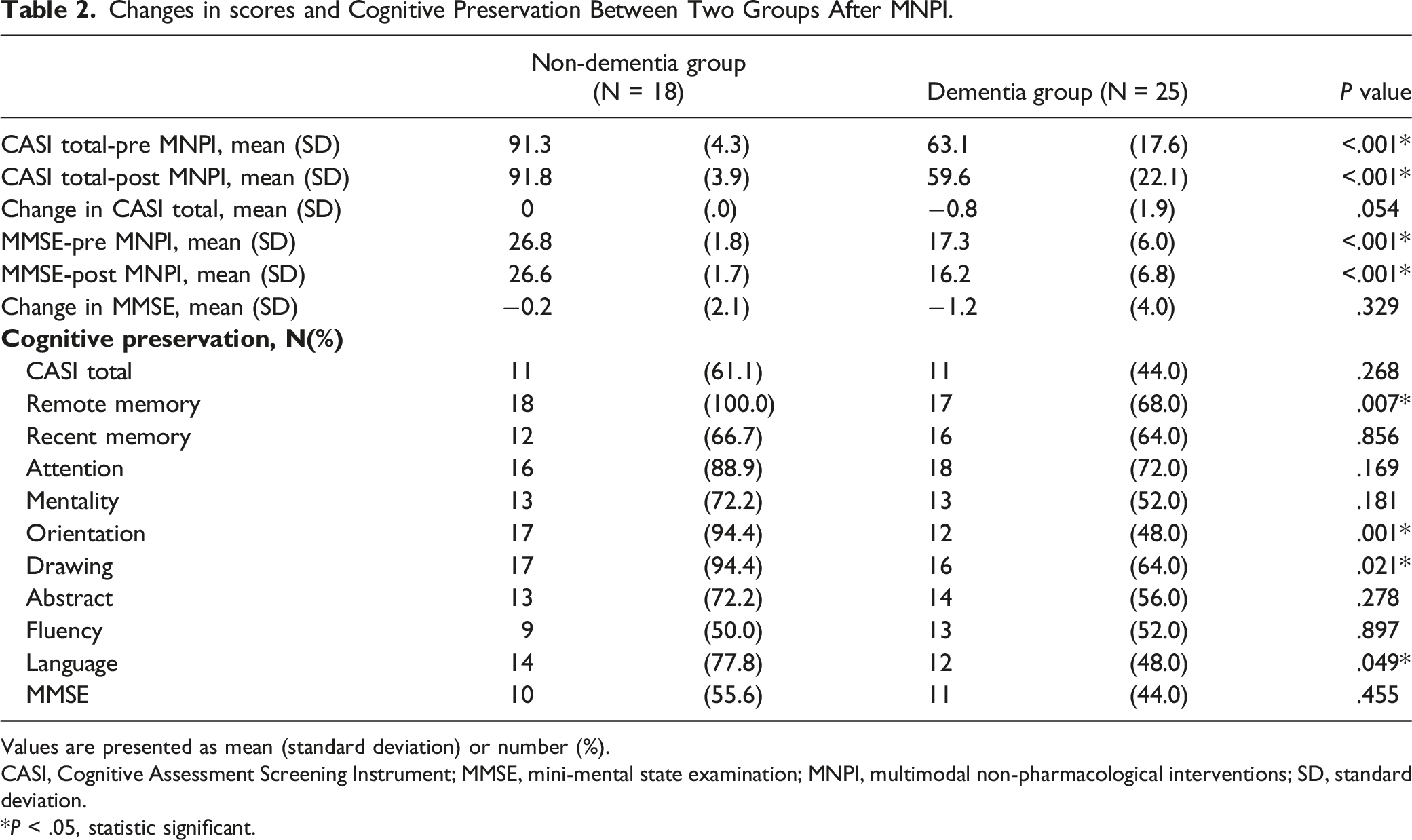
In total, there were 43 participants in our study, including 18 with non-dementia and 25 with dementia. The non-dementia group had a significantly higher proportion of cognitive preservation in remote memory (100.0% vs 68.0%, P = .007), orientation (94.4% vs 48.0%, P = .001), drawing (94.4% vs 64.0%, P = .021) and language (77.8% vs 48.0%, P = .049) than the dementia group. The highest proportion of preserved cognition after MNPI was remote memory (100%), followed by orientation (94.4%) and drawing (94.4%) in the non-dementia group. The highest proportion of preserved cognition after MNPI was attention (72%) followed by remote memory (68%), recent memory (64%) and drawing (64%) in the dementia group. Overall, their improved rate in behavioral and psychological symptoms was 55.6%.
Conclusion
Our study concluded the benefits of early MNPI in cognition preservation in the elderly, especially in the field of remote memory, orientation, drawing and language.
Keywords
Significance Statement
1. Multimodal non-pharmacological interventions (MNPI) have been determined as effective in delaying cognitive deterioration, but the timing of MNPI in the elderly is less discussed. 2. Our study concluded the benefits of early MNPI in cognition preservation in the elderly, especially in the field of remote memory, orientation, drawing and language. 3. The highest proportion of preserved cognition after MNPI was attention (72%) followed by remote memory (68%), recent memory (64%) and drawing (64%) in the dementia group.
Introduction
Dementia is cognitive decline significantly interfering with independence and daily functioning, and has emerged as a major global public health concern due to the rapid expansion of the elderly demographic. 1 Several management protocols have treated dementia with pharmacological or non-pharmacological interventions in improving cognitive, neuropsychiatric symptoms and overall quality of life for patients and families,2,3 and although pharmacological interventions appear to delay progression of cognitive impairment in dementia patients, the benefits are often non-sustained; accordingly, non-pharmacological interventions are now considered for additional therapies in dementia.
Non-pharmacological interventions have been recommended as first-line treatment for behavioral and psychological symptoms of dementia (BPSD). 4 Several non-pharmacological interventions including functional analysis-based interventions (behavior management), 5 caregiver interventions, 6 reminiscence therapy, 7 music therapy, 8 aromatherapy, 9 cognitive stimulation, 10 exercise programs 11 and psychological therapy 12 have all been determined as effective in relieving BPSD with low to moderate grade evidence. 3 In addition to relieving BPSD, non-pharmacological interventions with physical activity training or cognitive training have shown benefits in the cognition function of patients with dementia,13,14 although present findings do not support strong evidence for the use of cognitive training for people with early-stage Alzheimer’s Disease AD) or vascular dementia. 15 Some other art practices have been proposed to deal with dementia, but evidence remains insufficient. Calligraphy, one of the traditional Chinese leisure activities, has been applied in mental nursing programs although as to whether Chinese calligraphy therapy exerts a curative effect to reduce neuropsychiatric symptoms remains inconclusive. 16 Drawings and paintings have been practiced as useful therapeutic interventions by psychiatric and psychological specialties, 17 and while such arts-based therapies might help delay cognitive deterioration, relieve psycho-socio-behavioral problems and improve quality of life in dementia, 18 there is still a lack of pragmatic evidence of real efficacy of art therapy for people with dementia. 19
Currently, multimodal non-pharmacological interventions (MNPI) have been employed. Combinations of exercise, cognitive training and activities of daily living are recommended for improving the global, executive function and memory of dementia patients in nursing homes. 20 Such multicomponent cognitive stimulation therapy interventions have had positive effects on daily life activities, cognitive and behavioral functions in people with mild stage dementia while delaying progression for at least two years. 21 MNPI are considered to have the potential to replenish single therapeutic practice by adjusting multiple modifiable risk factors contributing to cognitive decline. 22 Previous research has included existing diversities of design methods, interventions, case numbers, comparison conditions and outcome measurements that have comparisons in direct cross-studies difficult and inconsistent in real efficacy.15,23
Subjective memory complaints (SMC) could be present in as many as 60% of middle -aged individuals within the community. 24 In individuals with SMC, the signs and symptoms of the dementia might be subtle and only recent memory impairment is apparent 25 with surveys of cognition being often within normal range. In the trajectory of dementia, SMC was included in early definitions of mild cognitive impairment (MCI), which could be an intermediate stage from normal cognition to pre-dementia. 26 Although there is no consensus concerning pharmacological therapy for SMC or MCI, increasing the cognitive reservation by application of non-pharmacological interventions in MCI or healthy individuals could be considered a strategy to prevent further progression to dementia. Herein, we aimed to investigate the different effectiveness of MNPI in cognitive preservation in the elderly with and without dementia and determine the timing of MNPI in dementia prevention.
Material and Methods
Participants
We enlisted volunteers for our study from Kaohsiung Municipal Ta-Tung Hospital, which is situated in the southern region of Taiwan. The study focused on older adults who were randomly selected from outpatients visiting the neurology clinic. These participants were patients receiving neurology treatment or their relatives or partners. The study’s eligibility criteria required participants to (1) be over 65 years of age, (2) have sufficient mobility of four limbs to perform training programs, and (3) be without musculoskeletal diseases or cerebrovascular diseases. We screened the participants by the Ascertainment of Dementia 8 instrument (AD8) 27 and classified the participants into non-dementia (AD8<2) and dementia (AD8≧2) groups. Our study had specific exclusion criteria, which included the inability to complete the entire training course, refusal to cooperate with neuropsychiatric testing, and any participant who missed any sessions during the 16-week training course or pre/posttest. After invitation to participate and meeting the inclusion and exclusion criteria, written informed consent was obtained from all subjects.
Multimodal non-pharmacological interventions (MNPI)
MNPI comprised three training modalities as follows, (1) physical fitness training, (2) Chinese calligraphy practice, and (3) Chinese drawings and paintings. All participants attended 3 hours of MNPI twice a week over a 16-week period. Physical fitness activities comprised pre-exercise for 10 minutes, main exercise for 40 minutes, and finishing exercise for 10 minutes. The exercise routine included a 5-minute walk and 5-minute stretching session for warm-up, followed by various training courses aimed at improving different aspects of physical fitness. These courses included endurance or aerobic activities like brisk walking or jogging, strength or resistance training involving lifting weights and using resistance bands, balance exercises like standing on one leg, and flexibility exercises such as stretching different limbs. A 10-minute stretching session was done as a finishing exercise. To ensure proper exercise intensity, participants wore heart rate monitors, and a physical fitness instructor with experience led them through different motions, postures, and movement speeds while taking precautions to prevent falls and injuries. In Chinese calligraphy practice, participants randomly selected Chinese characters from a calligraphy writing handbook and used soft-tipped brushes to trace the strokes and structures of the characters, which were displayed in a mix of traditional calligraphic styles. Similarly, in Chinese drawings and paintings, participants imitated the Chinese painting using soft-tipped brushes. The participants attended Chinese calligraphy practice and Chinese drawings and paintings in a quiet room. All the practices of MNPI were guided by a trained assistant and designed for a group practice. All participants were advised to maintain their routine activities.
Measurement Outcomes of Cognition and BPSD
To assess the impact of MNPI, each participant underwent a neuropsychological evaluation at the beginning of the study and one year after undergoing MNPI. The study was designed to assess whether the intervention had any lasting effects beyond the 16-week period. Delaying the post-testing ensured investigation of the long-term effects of the intervention. Additionally, the 8-month follow-up was important for assessing the stability of any cognitive improvements that might have resulted from the intervention. The neuropsychiatric tests included the Traditional Chinese version of the Mini-Mental Status Examination (MMSE) 28 and the Cognitive Assessment Screening Instrument (CASI) 29 to evaluate cognitive function. Additionally, the Clinical Dementia Rating Sum of Boxes (CDR-SB) with CDR 30 was used to assess global function, and the Neuropsychiatric Inventory (NPI) 31 was employed for evaluating behavioral and psychological symptoms of dementia (BPSD) exclusively in the dementia group.
The MMSE is a questionnaire consisting of eight categories, including orientation to time, orientation to place, registration, attention and calculation, recall, language, repetition and complex commands. The total score of the MMSE is the sum of the scores in each category. The CASI evaluates cognition using nine subscales: remote memory, recent memory, attention, mentality, orientation, drawing, abstract, fluency and language. Scores range from 0 to 100, with higher scores indicating better cognition. The CDR Dementia Staging Instrument was utilized to evaluate six domains of cognitive and functional performance, including memory, orientation, judgment and problem-solving, community affairs, home and hobbies, and personal care. Each domain has a 5-point scale, with 0 indicating normal and 3 indicating severe dementia. The CDR-SB is the sum of scores in each domain. The CDR Scoring Algorithm was created to interpret the scores of each domain and calculate the total CDR. The necessary information to assess each rating is obtained through a semi-structured interview of the patient and a reliable informant or collateral source, such as family members or caregivers, referred to as the CDR assessment protocol.
NPI consists of twelve subscales; namely, delusions, hallucinations, aggression, depression, anxiety, elation, apathy, disinhibition, irritability, aberrant motor, nighttime behavior and eating. There was at least one caregiver living with patients as the informant. Each sub-item is scored by frequency (0 to 4) and severity (0 to 3) with the total score being the sum of each NPI sub-item, obtained by multiplying frequency and severity. Higher NPI score indicates worse BPSD. The caregiver distress is also scored in NPI (0 to 4). All neuropsychiatric tests were conducted by a psychologist blinded to the participants. Information was also collected from a knowledgeable collateral source, usually a spouse.
For determination of cognition and global function preservation, cognitive preservation by MMSE or CASI was defined as the increase of MMSE or CASI scores≧0, global function preservation by CDR or CDR-SB was defined as the decrease of CDR or CDR-SB scores≧0, while improvement of BPSD was defined as decrease of total NPI scores≧0.
Ethical Considerations
All the participants were voluntary and were informed about the study purpose. A written informed consent, including research title, purpose, explanation of research, and study procedures, was obtained from each eligible participant. We explained the risks and benefits clearly to the participants. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Kaohsiung Medical University Chung-Ho Memorial Hospital (KMUHIRB-SV(I)-20170034).
Statistical Analysis
We analyzed the data by using SPSS for Windows 17.0 (SPSS Inc., Chicago, IL, USA) and demonstrated sample characteristics and variables by descriptive statistics. Frequency distributions were calculated for nominal variable (ie, gender), and mean and standard deviation were calculated for continuous variables (ie, age, educational level, and neuropsychiatric assessments). Comparisons of differences between pre- and post-MNPI used paired t test analysis, differences of neuropsychiatric assessments between dementia and non-dementia groups by independent t test analysis, and difference of proportion of cognitive preservation between the two groups by chi-square test. Total numbers and improved numbers of BPSD in participants were demonstrated by dementia and caregivers. P < .05 was considered statistically significant.
Results
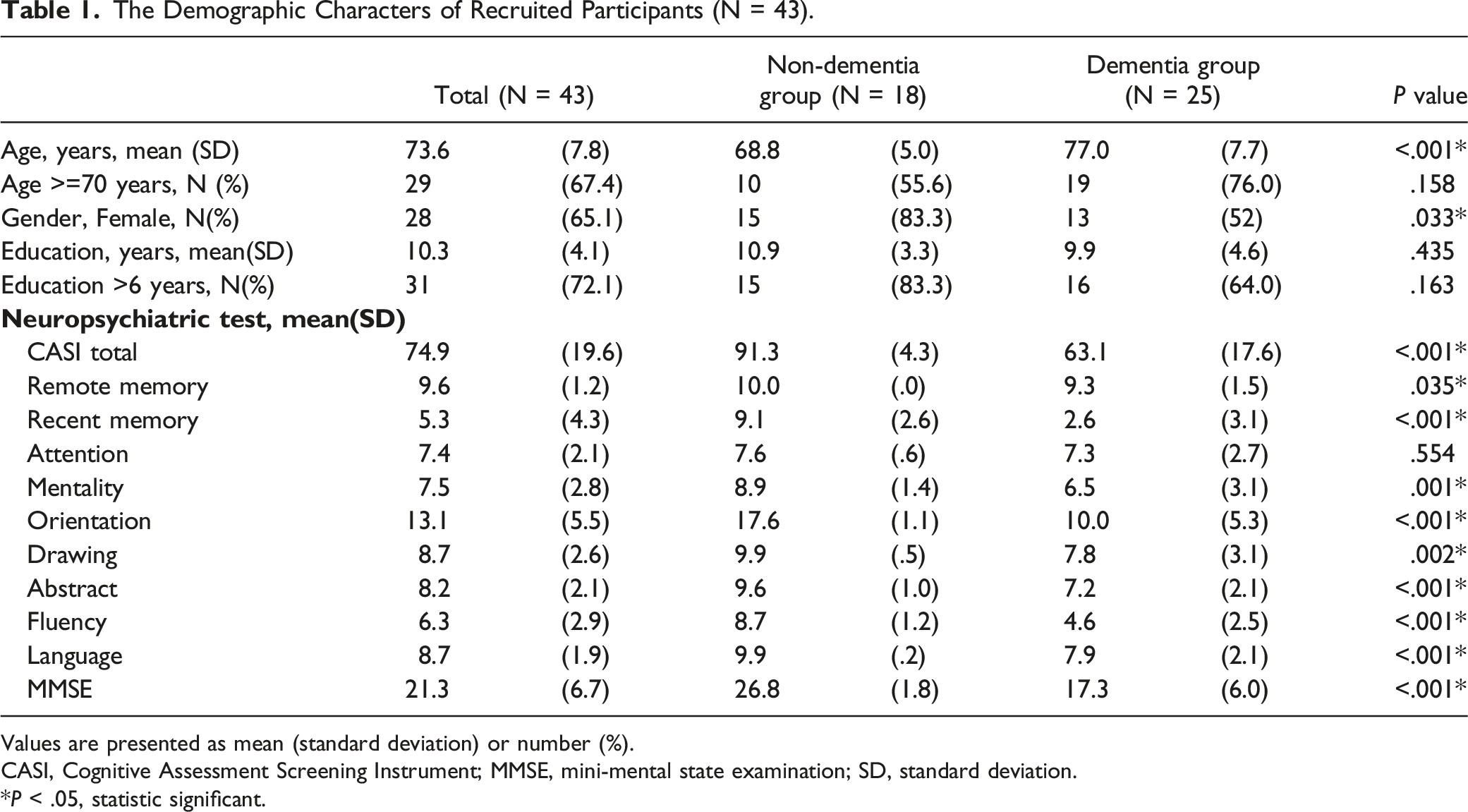
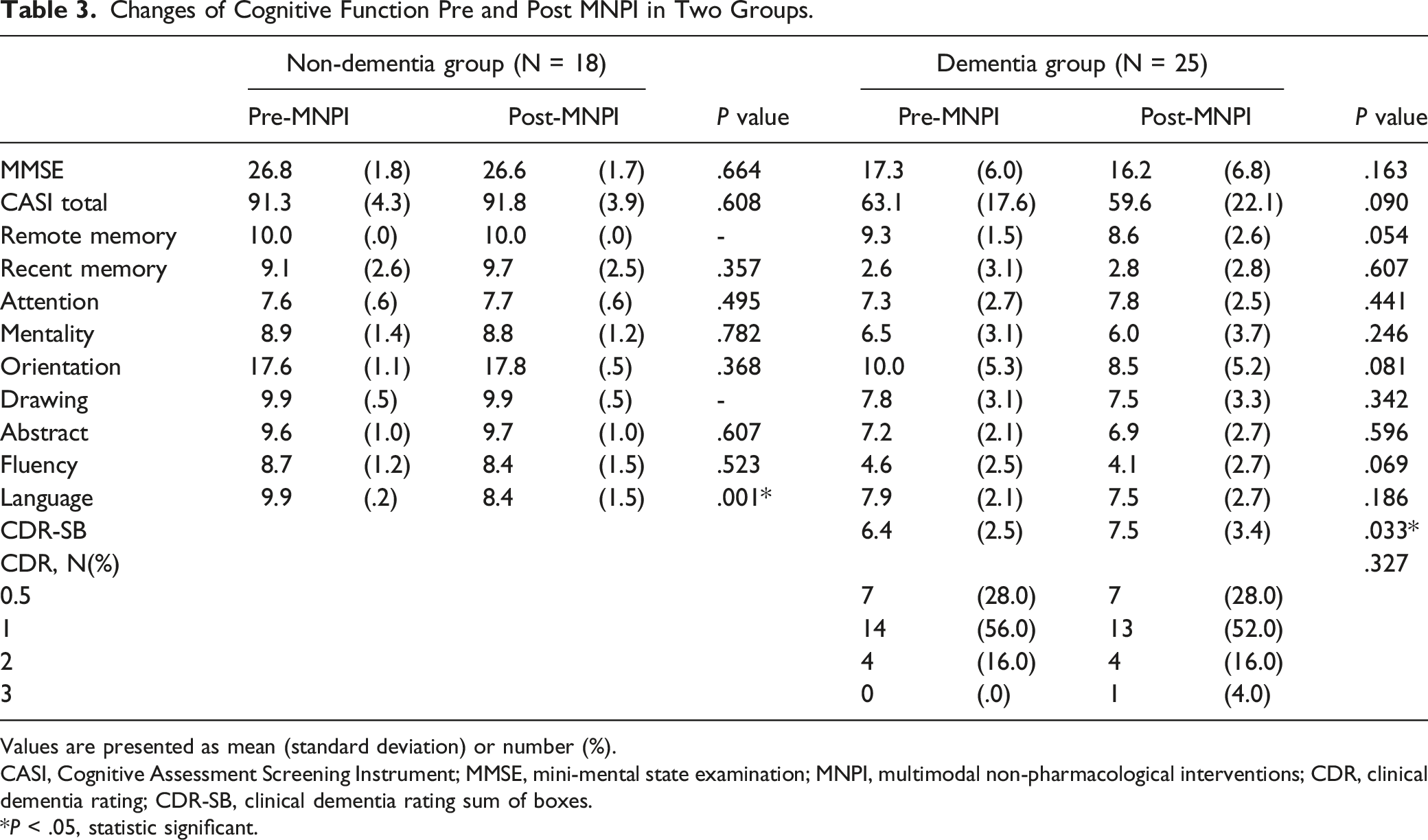
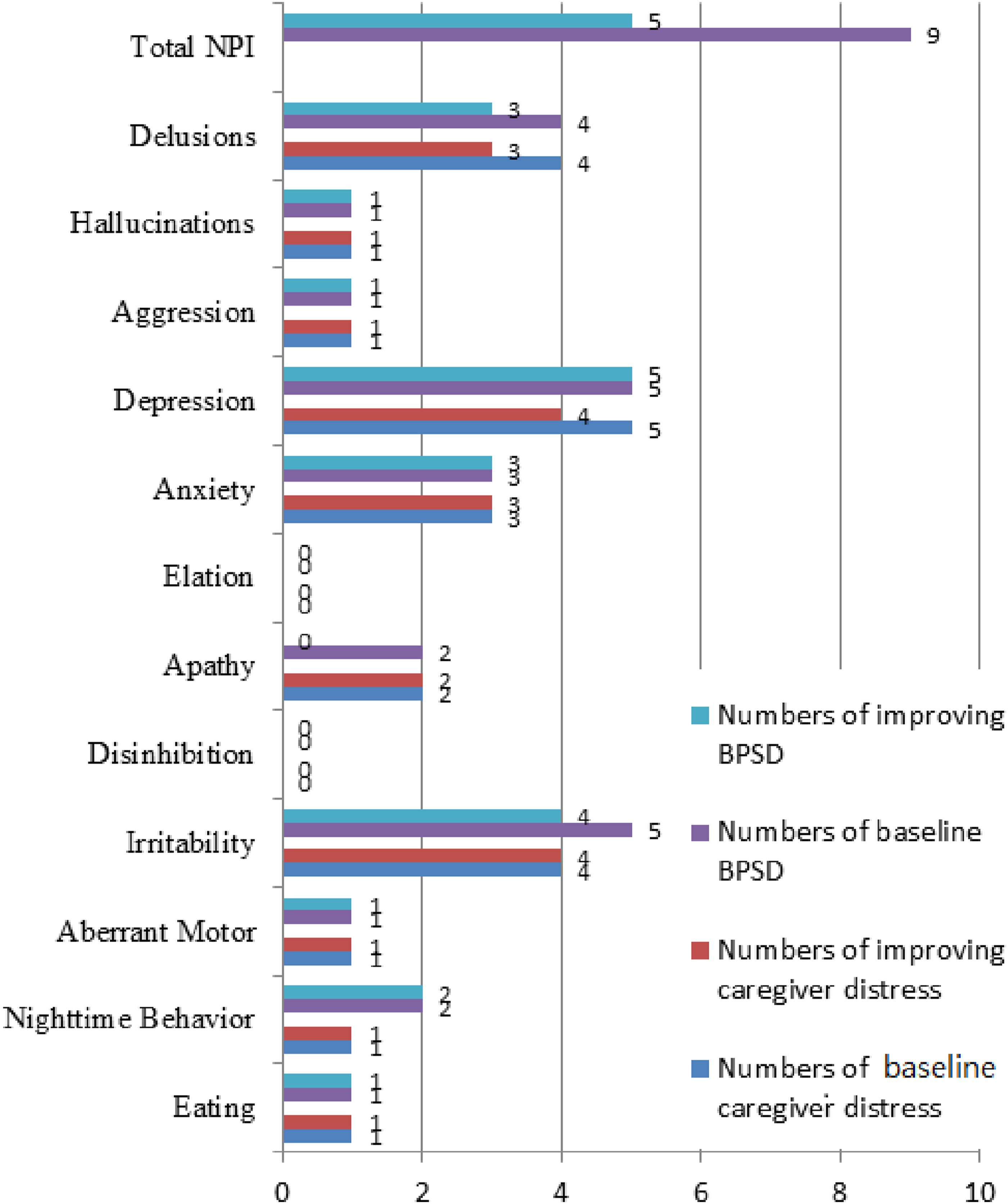
There were 52 participants enrolled in our study, including 24 with non-dementia and 28 with dementia. During the 16-week practice of MNPI, 9 participants were dropped due to withdrawal or incomplete survey, leaving 18 with non-dementia and 25 with dementia into analysis (Figure 1). Table 1 shows the demographic characteristics of the participants as average age being 73.6 ± 7.8 years, 28 (65.1%) were females, and average education level being 10.3 ± 4.1years. Significant differences in age, CASI total scores, most of the CASI subscales (except attention) and MMSE between non-dementia and dementia groups were found. Table 2 demonstrates the difference of changes in scores and cognitive preservation in MMSE, CASI and CASI subscales between the two groups. No significant difference of changes in MMSE and CASI scores between the two groups were found. In the non-dementia group, the highest proportion of preserved cognition of CASI subscales after MNPI was remote memory (100%), followed by orientation (94.4%) and drawing (94.4%). In the dementia group, the highest proportion of preserved cognition of CASI subscales after MNPI was attention (72%), followed by remote memory (68%), recent memory (64%) and drawing (64%). It indicated participants in the non-dementia group had a significantly higher proportion of cognitive preservation in remote memory (100.0% vs 68.0%, P = .007), orientation (94.4% vs 48.0%, P = .001), drawing (94.4% vs 64.0%, P = .021) and language (77.8% vs 48.0%, P = .049) CASI sub-scales than those in the dementia group. Table 3 shows the difference of neuro-psychiatric assessments pre- and post-MNPI in the two groups. In the non-dementia group, the CASI total scores, recent memory, attention, orientation and abstract subscales of CASI had a trend to increase after MNPI, but did not reach statistical significance. Language subscale of CASI significantly decreased in the non-dementia group (9.9 ± .2 vs 8.4 ± 1.5, P = .001) after MNPI. In the dementia group, recent memory and attention subscales of CASI had a trend to increase after MNPI, but not with significance. Progression of CDR-SB was observed (6.4 ± 2.5 vs 7.5 ± 3.4, P = .033) after MNPI in the dementia group. Figure 2 demonstrates the numbers of BPSD in participants and care-giver distress in the dementia group. Overall, 9 had BPSD and 5 (55.6%) showed improvement in BPSD after MNPI. The findings concluded most subscales of NPI were fully improved, while partial relief in delusions (75%) and irritability (80%) was noted although there was no improvement in apathy. In caregiver distress relief, the most frequent BPSD that caused caregiver distress was depression, followed by delusions and irritability. Most NPI subscales of caregiver distress were improved, while partial relief in delusions (75%) and depression (80%) was observed. Flow of enrollment of the study. The Demographic Characters of Recruited Participants (N = 43). Values are presented as mean (standard deviation) or number (%). CASI, Cognitive Assessment Screening Instrument; MMSE, mini-mental state examination; SD, standard deviation. *P < .05, statistic significant. Changes in scores and Cognitive Preservation Between Two Groups After MNPI. Values are presented as mean (standard deviation) or number (%). CASI, Cognitive Assessment Screening Instrument; MMSE, mini-mental state examination; MNPI, multimodal non-pharmacological interventions; SD, standard deviation. *P < .05, statistic significant. Changes of Cognitive Function Pre and Post MNPI in Two Groups. Values are presented as mean (standard deviation) or number (%). CASI, Cognitive Assessment Screening Instrument; MMSE, mini-mental state examination; MNPI, multimodal non-pharmacological interventions; CDR, clinical dementia rating; CDR-SB, clinical dementia rating sum of boxes. *P < .05, statistic significant. Numbers of baseline and improving BPSD in participants and caregiver distress.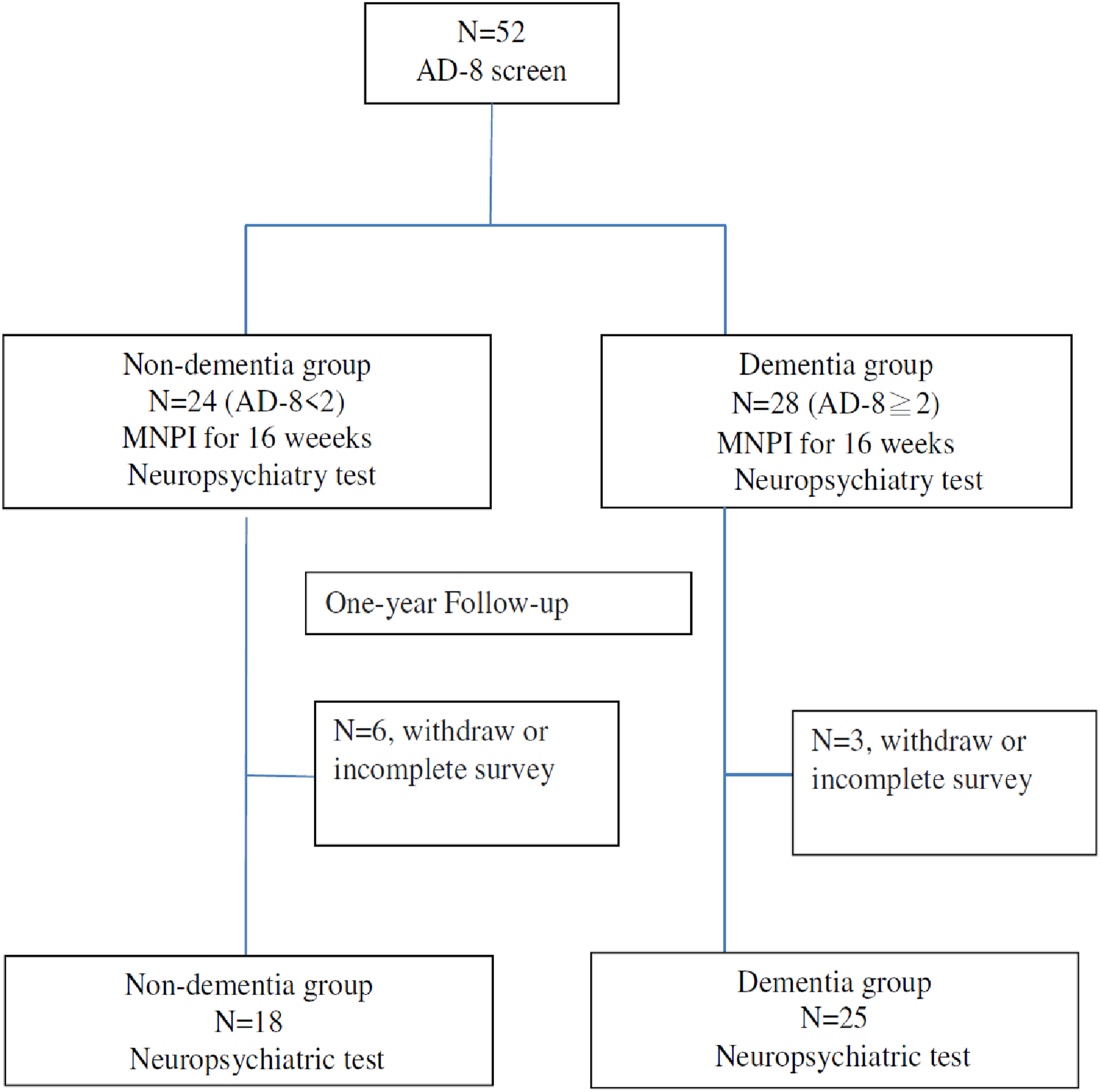
Discussion
Our study concluded MNPI, including physical fitness training and art practices, produced more benefits in preservation of remote memory, orientation, drawing and language in the non-dementia group compared to the dementia group. This confirmed the role of early interventions in cognitive preservation in elderly. Moreover, MNPI contributed to remarkable outcomes of cognitive preservation in attention in the dementia group. Overall, their improvement rate in BPSD was 55.6%.
While previous studies have shown that MNPI is effective in delaying cognitive deterioration, it is unclear whether MNPI is equally effective in individuals with and without dementia. The significance of this study lies in its potential to inform the development of intervention programs for elderly individuals with different cognitive statuses. Specifically, the study’s findings suggest that MNPI with physical training and art practices could be more beneficial in preserving cognitive function in elderly individuals without dementia than those with dementia. Furthermore, the study’s results highlight the importance of early intervention and prevention efforts for cognitive decline, particularly in individuals at risk for dementia. Identifying effective interventions that can slow down cognitive decline could have significant implications for improving the quality of life for elderly individuals and reducing healthcare costs associated with dementia care. Overall, this study’s findings contribute to the growing body of research on the effectiveness of non-pharmacological interventions in cognitive preservation while providing insights into the differential effectiveness of these interventions in elderly individuals with and without dementia.
We selected the duration and amount of MNPI based on the previous research for non-pharmacological interventions to delay cognitive decline in the elderly.32,33 The study enrolled participants for 16 weeks, which is a reasonable timeframe for cognitive interventions to produce measurable effects. We also selected specific interventions based on their potential to address cognitive and functional deficits commonly observed in the elderly. The study utilized a multimodal approach, including physical fitness training, Chinese calligraphy, and Chinese drawings and paintings. The amount of MNPI was set at 3 hours, twice a week, which is a reasonable amount of time for older adults to participate in such interventions without causing excessive fatigue or discomfort. We carefully selected the duration and amount of MNPI based on current research and guidelines, as well as the specific needs and abilities of the elderly participants.
Dementia is a neurodegenerative disease. Clinical trials concluded limited efficacy for the treatment of dementia, accordingly focusing on strategies to prevent cognitive decline in early life during preclinical or asymptomatic stages of dementia is crucial. Our study enrolled 43 participants (18 non-dementia and 25 dementia), and non-demented participants were younger (68.8 ± 5.0 vs 77.0 ± 7.7 years) than the demented participants. Non-demented participants had better cognitive function before MNPI than demented participants. The scenario is consistent with the real-world practice for early intervention implying younger age possessing better cognition before dementia progression; thus, the better cognitive effectiveness of MNPI in the non-dementia group might result from both underlying better cognition and younger age. Education could also be a factor influencing the effect of MNPI, and while the average education level was 10.3 ± 4.1 years in our study, there was no significant difference of education level found between the two groups.
Researchers have used non-pharmacological interventions in dementia prevention, but findings are inconclusive, which are related to randomized, controlled trials, outcome measurements, interventions, long-term effects and limited case numbers. MNPI complements single therapeutic practice and enhances therapeutic efficacy by modifying the risks of cognitive decline. In our study, we adopted physical fitness training and art-based practices in a group practice design. Group practice is a socialization skill, proven to enhance the effects of non-pharmacological interventions in dementia with physical and intellectual activities. 34 Besides, effective non-pharmacological interventions involve fewer side effects than pharmacological interventions and lessen the functional impact of dementia. In this study, we emphasize the potential benefits of group activities such as increased social interaction and engagement, which might have contributed to the overall effectiveness of the MNPI intervention. Additionally, it could be further helpful to examine the impact of group activities on participant satisfaction and adherence to the intervention, which could also have implications for the feasibility and scalability of the intervention in real-world settings.
Numerous studies have demonstrated that physical activity and exercise can positively impact cognitive performance in older adults.35,36 Research has also shown that aerobic exercise can increase volume growth in the anterior hippocampal regions and enhance cognitive and neural plasticity in older individuals.37,38 Additionally, aerobic exercise training can improve cardiovascular fitness, 39 which could help to control cardiovascular risk and prevent vascular dementia. Chinese calligraphy and drawing/painting are two unique traditional art forms in Chinese culture, where Chinese calligraphy involves a dynamic integration of mind and body as characters are written, while Chinese drawings and paintings use various instruments to create visual art on a two-dimensional medium. Both these art-based practices involve visuospatial functioning including visual perception and spatial structuring of the characters, cognitive planning and maneuvering of a soft-tipped brush to follow specific character configurations. Studies have found calligraphy practice in later life might delay cognitive deterioration, 40 as researchers have concluded drawing disorders are very common in AD and other forms of dementia. 41 The drawing process is multi-componential and impaired by various kinds of brain lesions. The clock drawing test is one of the most used cognitive screening tools for early diagnosis of dementia. 42 By practicing the Chinese art-based training modalities, we aimed to spare the visuospatial ability and other cognition modalities. The baseline drawing ability was determined as being worse in the dementia group than in the non-dementia group (7.8 ± 3.1 vs 9.9 ± .5, P = .002). As for the results of our study, 94.4% of drawing preservation rate was significantly noted in the non-dementia group, and 64.0% in the dementia group. The other notably cognitive preservation areas between the two groups included remote memory, orientation and language. The mechanism of action of calligraphy as an intervention is thought to involve a dynamic integration of mind and body as characters are written where calligraphy practice requires concentration, attention and fine motor skills, which tend to stimulate the brain and promote neural plasticity. Regular calligraphy practice can improve cognitive functioning including attention, memory and executive function in older adults while also promoting relaxation and reducing stress, which can have additional cognitive and health benefits. Additionally, calligraphy is a form of art, and engaging in creative activities has been shown to promote cognitive, emotional and social well-being. Overall, calligraphy practice could improve cognitive function through a combination of physical, cognitive and emotional mechanisms.
We evaluated the numbers of BPSD and caregiver distress from BPSD in the dementia group overall, finding 9 subjects with BPSD in the dementia group and 5 (55.6%) with improvement in BPSD after MNPI. Most caregiver distress from BPSD was relieved, with partial relief in delusions and depression. Non-pharmacological interventions were recommended as first-line treatment for BPSD. 4 Physical exercise contributed to the beneficial effects of ameliorating BPSD in AD by both psychological and neurobiological mechanisms, including improved sleep, stress reduction, change in neuro-transmitter concentrations, increased synthesis of neurotrophins and immune activation. 43 The Chinese art-based practices helped to stabilize and improve both the mind and body. Clinical research has revealed calligraphic writing improves attention span, concentration, relaxation and emotional stabilization44,45; thus, the combination of physical fitness training and Chinese art-based practice in our study offered notable benefits in management of BPSD in the dementia-afflicted participants and their caregivers.
Our study revealed MNPI contributed to benefits in cognitive preservation in the elderly with or without dementia and highlighting early intervention of MNPI in non-demented individuals produced better effects in remote memory, orientation, drawing and language function. Current studies have proposed new treatment strategies against cognitive decline from the aspect of neuropathology in non-demented individuals 46 with non-pharmacological interventions on cognitive function in the elderly with MCI being encouraged. Physical activity and cognitive exercise could improve memory and executive functions in the elderly with MCI, but systemized efficient protocols need to be established. 47 Evidence suggests healthy elderly and AD patients retain the potential for neuroplasticity, as non-pharmacological interventions involving cognitive training and physical exercise helped healthy elderly and cognitively impaired subjects modulate neural activity and structural brain integrity. 48
Although the findings of the study are remarkable, there are some limitations. Firstly, the limited sample size and high dropout rate indicated further studies with larger sample size and control group are needed to confirm the effects of the intervention. Secondly, both demographic data (socioeconomic status or family history) and certain medical information (co-medication or medical past history) were unavailable. Thirdly, ceiling effects might be observed in the assessments. Fourthly, regarding the classification of dementia, it was purely based on the AD8 result in our study. We used CDR to access the severity of dementia. There was no clinical ascertainment and determination if there is secondary cause, such as depression. There are some concerns about the study. For the non-dementia group, it includes individuals with and without MCI in our study. We compared the cognition preservation of non-dementia group with dementia groups. Further studies with large case numbers might help to clarify the effectiveness of cognition preservation for individuals with and without MCI in the non-dementia group. The non-dementia group were significantly younger than the dementia group in our study. This can have contributed to the outcome of the study. It’s a valid concern that the non-dementia group in our study may represent individuals who naturally maintain their cognitive abilities over time, without the intervention. It requires a comprehensive approach that includes rigorous study design, longitudinal assessment for the cognitive trajectory, appropriate statistical analysis, subgroup analysis, and qualitative assessment. Large case numbers and standardized protocols are needed to investigate the effectiveness of MNPI. In future dementia prevention trials, using multi-modal, multi-factor, multi-level and community/individually-tailored approaches should be recommended. 49 Furthermore, the impact of the intervention on daily life and other activities outside of the intervention is not well-described in our study, so to ensure that any observed changes are not due to confounding variables, future studies should control for such variables.
Overall, the effectiveness of early MNPI in slowing down cognitive decline is prominent in the field of remote memory, orientation, drawing and language. These findings have important implications for future research and healthcare guidance. Firstly, future research should focus on identifying specific components of MNPI that are most effective in preserving cognitive function in elderly individuals, particularly those with dementia. This will help in developing tailored interventions to meet individual needs and improve overall outcomes. Secondly, healthcare providers and policymakers should consider implementing MNPI as a preventive measure for cognitive decline in the elderly population. This could involve developing programs that incorporate physical fitness training, Chinese calligraphy, and Chinese drawings and paintings as part of routine care for elderly individuals. Thirdly, it is crucial to determine the lasting effects of MNPI practiced in individuals with and without dementia. Finally, there is a need for increased awareness among the general public about the importance of non-pharmacological interventions in maintaining cognitive function in the elderly. Currently, application of virtual reality for dementia management has been developed.50,51 This can be achieved through public education campaigns and community-based programs that promote healthy aging practices and encourage participation in activities that promote cognitive function.
Footnotes
Acknowledgments
We acknowledge Mentality Protection Center, Fo Guang Shan Compassion Foundation, Fo Guang Shan Nan Ping Temple, and Chinese Mentality Protection Association.
Author Contributions
Research concept and study design, YHY; literature review and data collection, SFH, LJL; data analysis and interpretation, LCH; writing-original draft preparation, SWH; writing-review and editing, all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Health Research Institutes, Taiwan (PH-106-SP-17), Kaohsiung Medical University Research Center Grant (KMU-TC112B02), Department of Neurology, Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung, Tainwan (KMTTH-DK(C)11203), and Kaohsiung Municipal Siaogang Hospital, Kaohsiung, Taiwan (Kmhk-108-033, S-108-009, S-109-01 and S-111-01).
Ethical Statement
Data Availability Statement
Data is not available due to ethical reasons. Further enquiries can be directed to the corresponding author