
Abstract
Objectives
To examine the relationship between hearing impairment and cognitive function and the mediating role of social isolation and depression.
Significance Statement
• Older adults with self-reported mild or severe hearing impairment are at high risk for decreased cognitive function. • Social isolation is a mediator linking self-reported hearing impairment to cognitive function. • No mediating effect of depression on the relationship between self-reported hearing impairment and cognitive function.
Introduction
Cognitive function is crucial for maintaining the independence of older adults. 1 With the global population aging, the number of cognitive impairment among older adults is increasing. According to a national epidemiological study, the prevalence of dementia was reported to be 6.0% and mild cognitive impairment was 15.5% among Chinese older adults aged 60 years and above. 2 Dementia has not only decreased the quality of life for older adults but has also imposed a significant burden on families and society as a whole. A multicenter survey conducted in China, involving 3098 individuals diagnosed with dementia, revealed that the average annual cost of care per person amounted to $19,144. 3 It also indicated that the annual total costs would reach $1.89 trillion by 2050.
Hearing impairment, a common sensory disorder in older adults, is now ranked as the fourth leading contributor of disability-related years lived, posing a significant public health problem. 4 It is estimated that 157 billion people experienced hearing impairment in 2019 globally, 62.1% of whom were over 50 years old. 5 For Chinese older adults, the prevalence of hearing impairment was 44% or higher in different provinces. 6 These discrepancies could be due to several factors, such as sex, age, region, and different criteria that could be used to define hearing loss. Due to population growth and aging, the prevalence of hearing impairment will continue to be on the rise. Hearing impairment could lead to increased physical disability and the risk of adverse mental and psychological outcomes. 4 Growing evidence has suggested that hearing impairment and cognitive function appear to be linked and that individuals with hearing impairment suffer from accelerated cognitive decline.7,8 However, the underlying mechanism needs further clarification.
Research suggests 1 potential mechanism between hearing impairment and cognitive function may be through psychosocial factors, in which social isolation and depression might be involved.9,10 Social isolation represents objective social relationships, which consist of social network size, communication frequency, and relationship quality. 11 In contrast, depression, characterized by low mood and low self-worth, is prevalent and disabling in late life. Previous studies indicated that social isolation predicted depression and cognitive impairment in older adults.12,13 Jiang and colleagues revealed that social isolation partially explained the link between hearing loss and depression. 6 In addition, research also showed that there was a significant association between depression and cognitive function. 14 Hearing impairment can make communication more challenging for older adults, increasing the possibility of social withdrawal, social isolation, depression, and consequent cognitive decline.15,16 From the neural perspective, hearing impairment involves a series of complex pathological changes that induce atrophy in brain regions and may thus provoke depression and cognitive dysfunction. 17 So far, social isolation and depression have often been examined individually in their relationship with cognitive function. However, evidence for the psychosocial mechanisms underlying hearing impairment and cognitive function remains limited.
Therefore, the main objective of this study was to examine the relationship between self-reported hearing impairment and cognitive function among older Chinese community dwellers. We also aimed to explore the role of both social isolation and depression in the relationship in the hope of preventing and alleviating cognitive decline among older adults.
Material and Methods
Participants
The baseline survey of CHARLS includes people aged 45 years or older and living in communities, 17708 individuals in total. 18 This study involved community-dwelling older adults aged 60 and above from the 2018 wave of the CHARLS. Harmonized Cognitive and Dementia Assessment (HCAP) was first added in the 2018 wave of CHARLS. The CHARLS HCAP is the first nationally representative sample in China that could support the assessment of cognitive function for respondents aged 60 and over. The 2018 wave of CHARLS national follow-up data (including CHARLS HCAP) was officially released publicly on September 23, 2020 and is the most recent public data available from CHARLS. Ethics board approval for the CHARLS waves was granted from the Institutional Review Board of the University (No. IRB00001052-11015). Informed consent was obtained from all participants and the privacy rights were ensured. The 2018 wave of CHARLS has sufficient information to support the assessment of hearing impairment, social isolation, depression, and cognitive function. We used the STROBE cross sectional checklist when writing our report. 19
Measures
Self-Reported Hearing Impairment
To assess hearing impairment, participants were asked to rate their hearing as very good, good, fair, poor, or very poor by a single item. We classified participants into 3 categories (no hearing impairment = ‘very good’ or ‘good,’ mild hearing impairment = ‘fair,’ severe hearing impairment = ‘poor’ or ‘very poor’).
Cognitive Function
Cognitive function was measured by a popular and valid neurocognitive screening instrument: the Mini-Mental State Exam (MMSE). 20 MMSE was selected as 1 of the tests of the HCAP. MMSE is a set of 11 questions, and the score ranges between 0 and 30. A cut-off point of 24 was used to identify cognitive impaired individuals. A higher score indicated better cognitive function.
Social Isolation
One point was assigned to each participant if they were not in a marriage or not living with a partner, less than monthly contact was made with children, other family members, and friends (each scored 1), or non-participation in any social activity (played Ma-jong, played chess, played cards, or went to community club, or went to a sport, social, or other kind of club, et al). A higher score on a scale of 0 to 5 indicated greater social isolation. 21
Depression
Depression was measured by the Center for Epidemiological Studies Depression Scale (CESD-10). This shorter version contained 10 items on a four-point scale (0-3) that indicate the frequency of each depressive symptom in the past week from “rarely or none” to “most or all the time.” The item 5 and item 8 were reversely scored. The cut-off point was 10. A higher score implied greater depression. In Chinese older adults, the CESD-10 demonstrated acceptable validity and reliability. 22
Potential Covariates
A sociodemographic profile, including age, sex, education, and diseases (hypertension, dyslipidemia, diabetes, heart diseases, stroke), was obtained as potential confounding factors. The diseases were self-reported by answering the questions “Have you been diagnosed with hypertension/dyslipidemia (elevated of low density lipoprotein, triglycerides, and total cholesterol, or a low high density lipoprotein level)/diabetes (or high blood sugar)/heart disease (heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems)/stroke by a doctor?.” Education was classified as a dichotomous variable (less than lower secondary, upper secondary and vocational training).
Statistical Analysis
Data processing and analysis were performed using SPSS for Windows (Version 26) and the Process add-on for SPSS (Version 4.1). Missing values were imputed using predictive mean matching with numeric variables, binary variables by logistic regression, and factor variables by polytomous logistic regression. Continuous and categorical variables were presented as means (SDs) or medians (interquartile ranges) and frequencies and proportions, respectively. A mediation model with a multi-category independent variable, as defined by Hayes and Preacher, was developed and verified. 23 Relative mediation effect, relative direct effect, and relative total effect were used to illustrate and understand the process of mediation analysis for multi-category independent variables. The 95% confidence interval (CI) was generated from 5000 bootstrap samples. Adjustments were made for covariates if they demonstrated statistical significance at a threshold of P < .05.
Results
Characteristics of Eligible Participants From CHARLS (n = 6799).
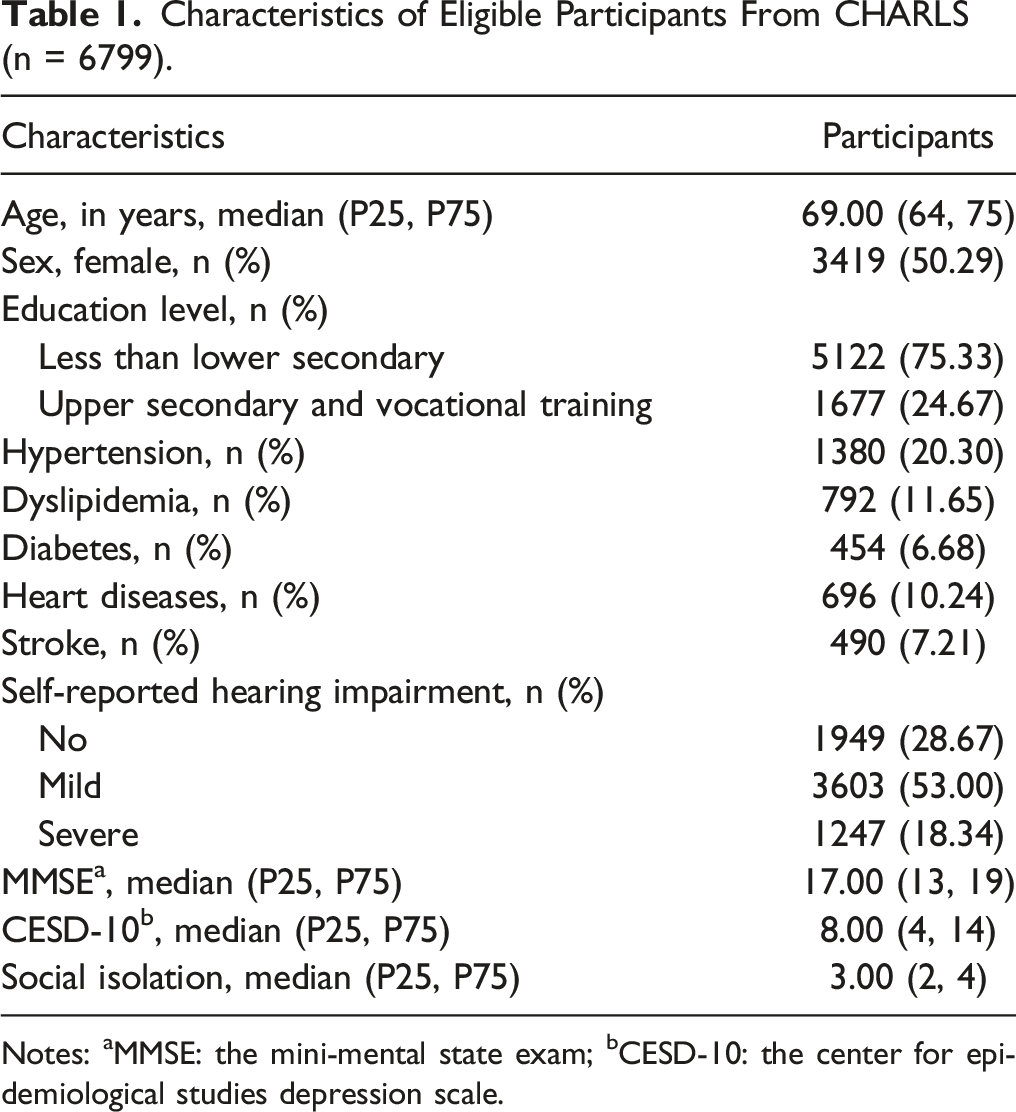
Notes: aMMSE: the mini-mental state exam; bCESD-10: the center for epidemiological studies depression scale.
Participant’s Characteristics and Differences in Variables by Hearing Impairment (n = 6799).
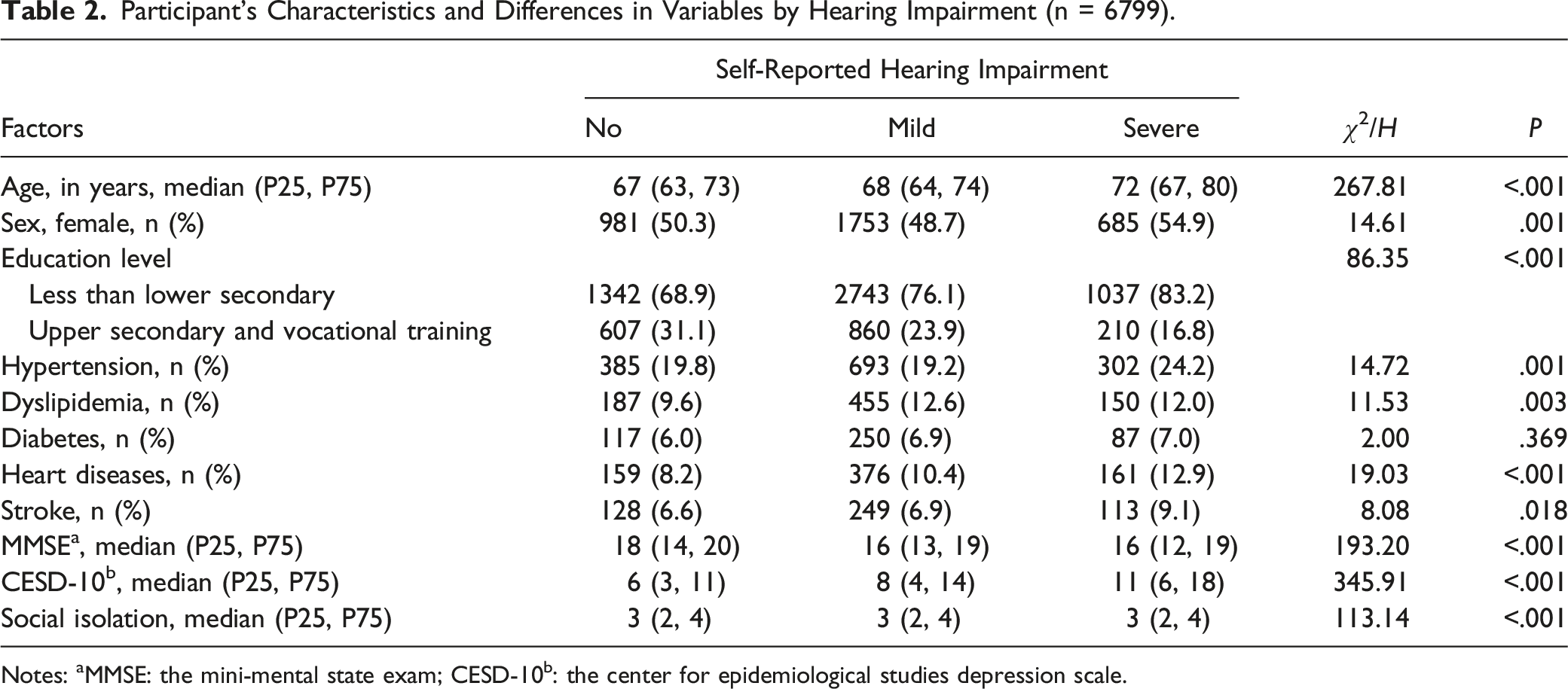
Notes: aMMSE: the mini-mental state exam; CESD-10b: the center for epidemiological studies depression scale.
Regression Results of the Chain Effects Models (n = 6799).
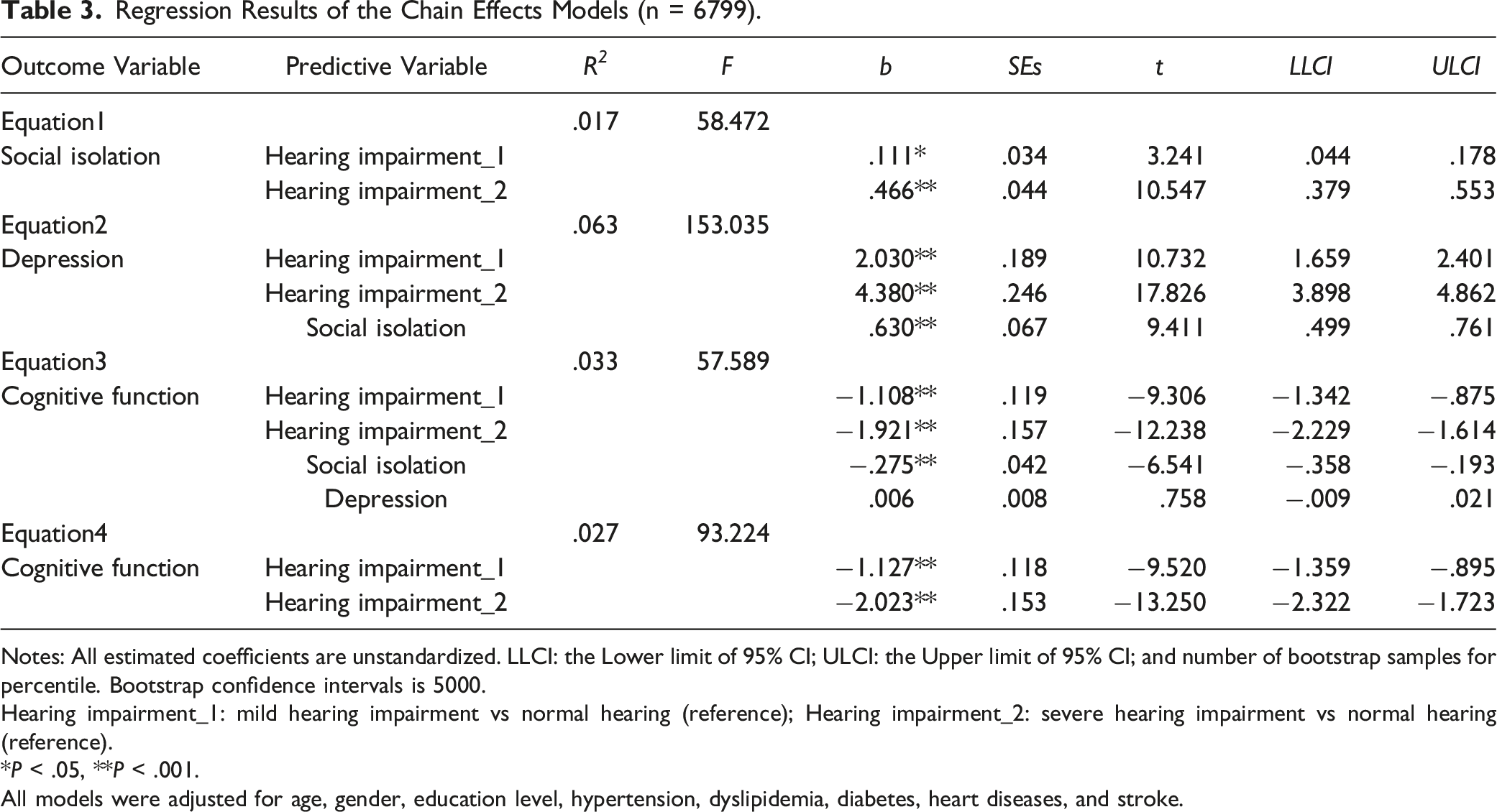
Notes: All estimated coefficients are unstandardized. LLCI: the Lower limit of 95% CI; ULCI: the Upper limit of 95% CI; and number of bootstrap samples for percentile. Bootstrap confidence intervals is 5000.
Hearing impairment_1: mild hearing impairment vs normal hearing (reference); Hearing impairment_2: severe hearing impairment vs normal hearing (reference).
*P < .05, **P < .001.
All models were adjusted for age, gender, education level, hypertension, dyslipidemia, diabetes, heart diseases, and stroke.
Results and Comparison of Chain Mediating Effect (n = 6799).
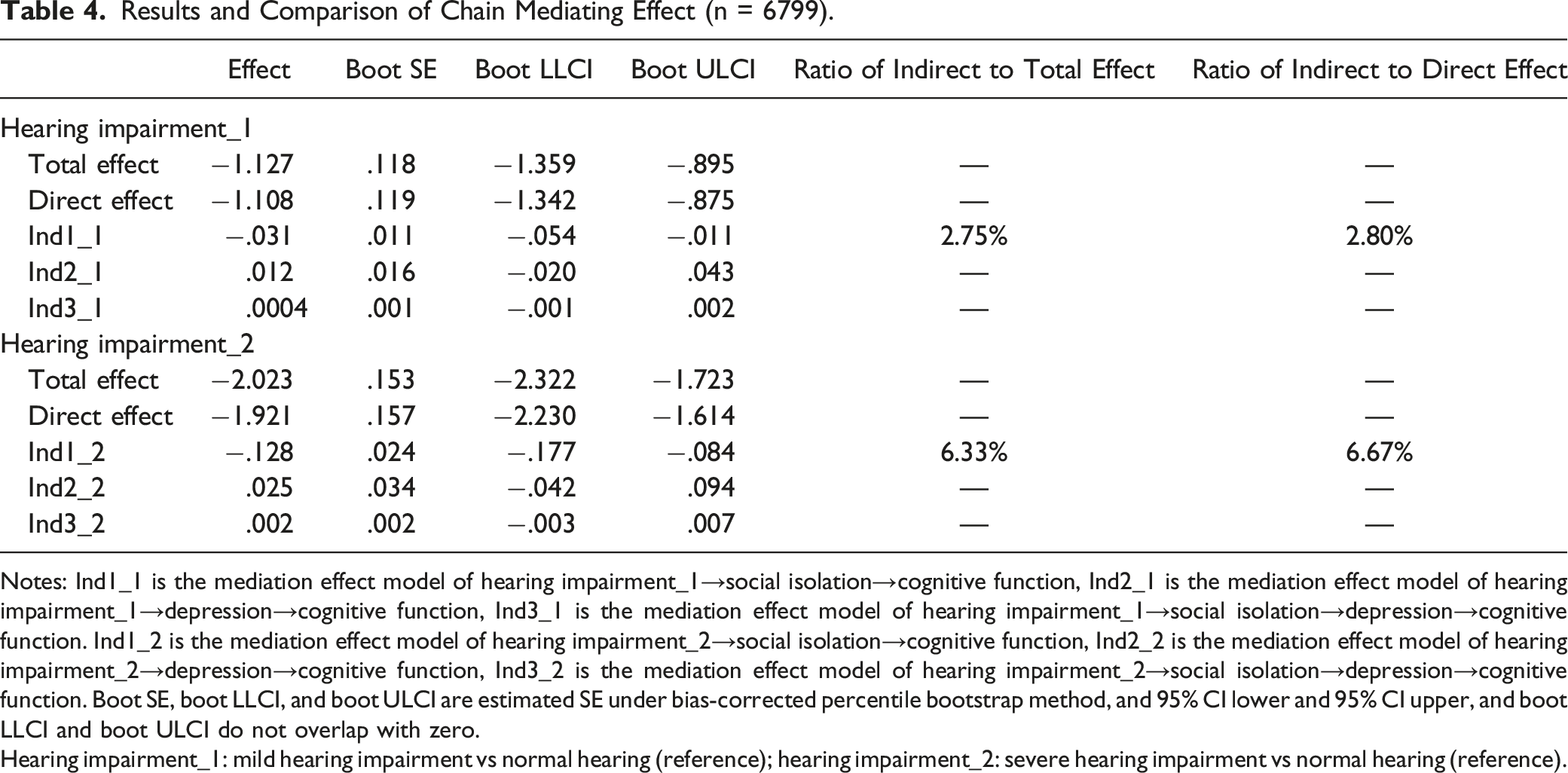
Notes: Ind1_1 is the mediation effect model of hearing impairment_1→social isolation→cognitive function, Ind2_1 is the mediation effect model of hearing impairment_1→depression→cognitive function, Ind3_1 is the mediation effect model of hearing impairment_1→social isolation→depression→cognitive function. Ind1_2 is the mediation effect model of hearing impairment_2→social isolation→cognitive function, Ind2_2 is the mediation effect model of hearing impairment_2→depression→cognitive function, Ind3_2 is the mediation effect model of hearing impairment_2→social isolation→depression→cognitive function. Boot SE, boot LLCI, and boot ULCI are estimated SE under bias-corrected percentile bootstrap method, and 95% CI lower and 95% CI upper, and boot LLCI and boot ULCI do not overlap with zero.
Hearing impairment_1: mild hearing impairment vs normal hearing (reference); hearing impairment_2: severe hearing impairment vs normal hearing (reference).
Discussion
This study primarily suggested the link between self-reported hearing impairment and cognitive function, as well as a possible psychosocial pathway. This study suggests that self-reported mild and severe hearing impairment are directly and negatively related to cognitive function. Social isolation, rather than depression, is an individual mediator linking self-reported mild and severe hearing impairment to decreased cognitive function in Chinese older adults.
The magnitude of the direct relationship between self-reported hearing impairment and cognitive function is large regardless of the positive mediating effect, consistent with prior studies. According to a longitudinal study using English Longitudinal Study on Ageing (ELSA), loneliness and social isolation did not counteract the direct relationship between hearing impairment and episodic memory. 24 Through a meta-analysis, Loughery and colleagues found a significant correlation between age-related hearing impairment and all areas of cognitive function, including global cognition, episodic memory, and visuospatial ability. 25 Researchers have hypothesized that the direct association between hearing impairment and cognitive function could be attributed to that hearing impairment may alter brain structure and function directly by reducing auditory input. The audibility and purity of sound are impacted by hearing loss, which weakens and deprives high-quality sensory information the brain receives, ultimately leading to changes in the structure and function of the central auditory and cognitive systems. 26 Over a 6 years follow-up, 1 study discovered MRI evidence of brain atrophy and volume decline in the right temporal lobe in people with hearing impairment in comparison to people with normal hearing, indicating the independent relationship between hearing impairment and cognitive function-related brain atrophy. 27 Studies on hearing interventions have also shown that hearing treatment has a beneficial impact on general or specific cognitive function, which may potentially point to the connection.28-31 The ACHIEVE study suggested that hearing intervention in older adults at higher risk for cognitive decline might significantly reduce cognitive changes over 3 years, whereas it might not have notable effects in those at lower risk for cognitive decline. 32 Two other potential explanations for the association are the resource allocation hypothesis, which suggests that more cognitive processing resources may be allocated to deal with degraded auditory signals, and the common cause hypothesis, which proposes that age-related changes in both hearing and cognitive function result from widespread neurodegeneration, implying a common underlying mechanism. While these hypotheses provide plausible explanation, further studies are needed to validate the mechanisms linking hearing loss and cognitive decline.33,34
This study shows a small but significant mediating effect of social isolation linking self-reported mild and severe hearing impairment to decreased cognitive function, thus supporting an indirect pathway, and enhancing the multifactorial explanation for hearing impairment and cognitive decline. The indirect association between hearing impairment and cognitive function through social isolation has been also indicated by several sizable cohort studies.24,35 As suggested, the impaired auditory processing of hearing impairment may hamper the ability to understand auditory information and to interact in social contexts. Barker and colleagues have concluded that people with hearing impairment might feel embarrassed or distressed about communication, leading them to retreat from once-enjoyable social interactions and resulting in subsequent social isolation. 36 Besides, poor auditory processing could directly limit cognitive reserve for social interactions along with the rising cognitive load. 37 Furthermore, reduced social engagement, as revealed by accumulating literature, can decrease cognitive function in late life by diminishing protective factors such as cognitive stimulation, cognitive reserve, and physical activities.38,39
An unexpected finding from the study is the absence of a mediating role of depression in the relationship between self-reported hearing impairment and cognitive function. More specifically, the link between depression and cognitive function is not significant in the mediation analysis. Few studies have examined the association of hearing impairment, social isolation, depression, and cognitive function as a full model. Existing evidence partly suggested the association of hearing impairment, social isolation and depression or depression and cognitive function, 40 with little direct evidence supporting depression as a mediator between hearing impairment and cognitive function in older adults. Maharani et al, for instance, looked at the mediation of social isolation and depression connecting hearing impairment and cognitive function individually. 24 One explanation for our findings could be that, when hearing impairment, social isolation, and depression were included in the mediation model, the pathway was adjusted by the former 2, which accounted for the majority of decreased cognitive function. Alternatively, rather than a diagnosis of depression, our measure of depressive symptoms as a continuous variable may have contributed to this insignificant association. To provide further clarity, additional empirical research is necessary to support this finding.
The strengths of this study are the large national random sample of older adults in China and the quantitative mediation analysis concerning both social isolation and depression. Nonetheless, several limitations should be noticed. First, the relatively low prevalence of severe hearing impairment may indicate existing stigma about hearing impairment or other social and psychological factors that prevent older adults from self-labeling as having hearing impairment with a self-reported measure. The measurement of hearing impairment in this study relied on self-reported data, given the lack of available objective auditory measures in CHARLS, which may introduce underestimation or overestimation of the association. Nevertheless, self-reported measures of hearing impairment are widely used in the literature as a cost-effective and accessible tool for studying older adults. Second, the CHARLS enrolled community-dwelling older adults in households, limiting the applicability of our findings to institutionalized older adults, who may suffer from worse status in terms of hearing, social engagement, depression, and cognitive decline. Third, The absence of information regarding hearing aid usage restricts the ability to fully explore the potential effects of hearing aid usage on social isolation, depression, or cognitive function. Future research should consider incorporation the assessment of hearing aid usage to further elucidate the relationships between hearing impairment and the mentioned measures. Finally, the cross-sectional design provides current associations rather than causality between self-reported hearing impairment and cognitive function. To validate the underlying causal relationships and effective strategies for mitigating cognitive decline in older persons, prospective and experimental studies regarding the effects of hearing on social functioning, depression, and cognitive function in different settings are highly encouraged.
Conclusions
This study has shown that self-reported mild and severe hearing impairment is negatively associated with cognitive function, and social isolation, rather than depression, is a mediator linking self-reported mild and severe hearing impairment to decreased cognitive function in Chinese older adults. Given that hearing impairment, even mild hearing impairment as self-reported, represents a risk factor for cognitive decline, early detection of hearing impairment should be emphasized for older adults. Significantly, social isolation related to hearing impairment may be reversible through non-pharmacological interventions and thus, together with hearing enhancement, represent candidate efforts to maximize cognitive function and reduce late-life burden in older adults.
Supplemental Material
Supplemental Material - Hearing Impairment and Cognitive Function: Mediating Role of Social Isolation and Depression
Supplemental Material for Hearing Impairment and Cognitive Function: Mediating Role of Social Isolation and Depression by Fan Wu and Chenxi Zhou in American Journal of Alzheimer’s Disease & Other Dementias®.
Footnotes
Acknowledgments
We are grateful for the generosity of the CHARLS team as well as all the participants for the time and efforts that they have devoted to this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Education Department of Hubei Province under the Science and Technology Research Project [number Q20211607]; Research and Innovation Initiatives of Wuhan Polytechnic University [number 2021Y62]; The 2023 Nursing Research Fund (General Project) of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology [number 2023D49]. The funders had no role in the study design, data analysis, or decision to publish.
Data Availability Statement
The data supporting this study’s findings are available on request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.