
Abstract
Self-efficacy plays a major role in improving health behaviors. The purpose of this study was to examine the effects of a physical activity program that utilized four self-efficacy resources in older family caregivers of persons with dementia. Quasi-experimental pretest-posttest design with control group was used. Study participants were 64 family caregivers aged 60 years or older. The intervention included a 60-minute group session per week for 8 weeks along with individual counseling and text messages. The experimental group showed significantly higher self-efficacy than the control group. In addition, physical function, quality of life related to health, caregiving burden, and depressive symptoms were significantly improved in the experimental group in comparison with those of control group. These findings suggest that a physical activity program with a focus on the resources of self-efficacy may be not only feasible but also effective for older family caregivers of persons with dementia.
Significance Statement
- Self-efficacy has a significant relationship with physical activity initiation and performance. - Detailed strategies which utilize the four components of self-efficacy resources need to be developed and implemented both at group and individualized activities of a physical activity program. - Physical activity program focusing on the utilization of self-efficacy resources may be effective to increase physical function, improve quality of life related to health, lower caregiving burden, and decrease depressive symptoms among older family caregivers of persons with dementia.
Introduction
Nearly 40% of the family caregivers of persons with dementia suffer from severe physical and psychological strain. 1 Approximately 15% of the family caregivers experience moderate to severe depression. 2 Hypertension, low immunity and higher death rates are frequently reported in this group.3–5 Their quality of life related to health deteriorates because of their stress related to caregiving roles and responsibilities.
The number of persons with dementia worldwide is increasing along with the trend of rapid expansion of the older adult population. Globally, the number of people suffering from dementia is estimated more than 55 million in 2021 while almost 10 million people are newly diagnosed every year. 6 Dementia is one of the major causes of disability and dependency among the older population. Family Being a caregiver of persons with dementia can be highly stressful and continued as many as 15 years. 7 They are at risk of becoming ‘secondary or hidden patients’. Because the health of family caregivers and persons with dementia are intertwined, it is critical to provide an intervention for family caregivers’ health that can help both groups. 8
Evidence has shown that regular physical activity reduces stress, depressive and anxiety symptoms while converting an unstable emotional state to stable.9,10 Moreover, physical activities help not only prevent and manage chronic diseases such as cardiovascular disease, diabetes, and osteoporosis but also lower mortality rate.11–16 Self-efficacy is a significant predictor of physical activity initiation and performance. 17 A person’s perception of their ability to complete a scheduled physical activity is referred to as exercise self-efficacy. Literature has repeatedly shown a significant correlation between physical activity and self-efficacy. 18
However, little is known about the effects of physical activity interventions that utilize theory-based self-efficacy resources among older family caregivers of persons with dementia have been found. Because the primary family caregivers of persons with dementia are often their spouses, 19 they may have not only caregiving burden but also at risk of physical inactivity as they are old. According to WHO’s global status report on physical activity 2022, physical activity decreases significantly as age increases. 20 Because of the unfeasibility of leaving persons with dementia alone at home, limited physical activity programs for family caregivers were offered at home or over the telephone in previous studies.19–21 In particular, little is known about the effects of interventions that use theory-based self-efficacy resources in this population.
Therefore, the purpose of this study was to examine the effects of an 8-week physical activity program with content mapping based on theory-based self-efficacy resources among older family caregivers of persons with dementia.
Method
Design
This study used a pretest-posttest design with both experimental and control groups. The effects of an 8-week physical activity intervention were measured in terms of self-efficacy (self-care, exercise), physical function, caregiving burden, depressive symptoms, perceived stress, and quality of life related to health.
Study Participants
Study participants were recruited from three dementia care centers in xxx. Staff (a registered nurse or a social worker) at the centers helped identify potential participations. In order to participate in the study, participants had to satisfy the following eligibility criteria: (1) being a family caregiver who lived with the individual diagnosed as having Alzheimer’s disease or other forms of dementia, (2) aged 60 years or older, (3) enrolled in a dementia care center, and (4) not engaged in regular physical activity (i.e. for 30 minutes more than twice a week) in the previous three months. Participants were excluded if they had the limitation in walking due to any medical condition.
Initially, a total of 74 participants were volunteered and gave their written consent in order to participate in the study. Upon the completion of consent, they were assigned to one of two groups which were either experimental or control. The group allocation was conveniently done because their caregiving schedules for persons with dementia often varied and were not flexible to change in order to attend the intervention. The control group received usual care.
In experimental group, two participants dropped out because of their hospitalization while four were eliminated due to the incompletion of the entire intervention. In addition, there was one withdrawal because of increased caregiving responsibilities as the health of person with dementia got deteriorated. In control group, three participants dropped out because of the incompletion of survey questionnaire. Finally, 64 study participants in total completed the study while 34 in experimental group and 30 in control group.
Intervention
This study provided an 8-week physical activity program which focused on the utilization of self-efficacy resources. In-group physical exercise sessions were held once a week for 60 minutes over 8 weeks. The designated exercise areas at the dementia care centers were used for the intervention. The sessions were scheduled during family caregivers’ waiting time while persons with dementia attended in their own cognitive program. In addition, an individual telephone counseling and text message was provided before and after the in-group physical exercise sessions. The participants in experimental group participated in all the sessions of the intervention.
The intervention of Physical Activity utilizing Self-Efficacy Resources (PA-SER) program was designed for family caregivers who were the age of 60 years or older and did not exercise consistently. Prior to the implementation of the intervention, the content of the program was reviewed and confirmed by a specialist who was certified in strength and conditioning of physical activity.
Program Description: Physical Exercise using the Self-Efficacy Resources.
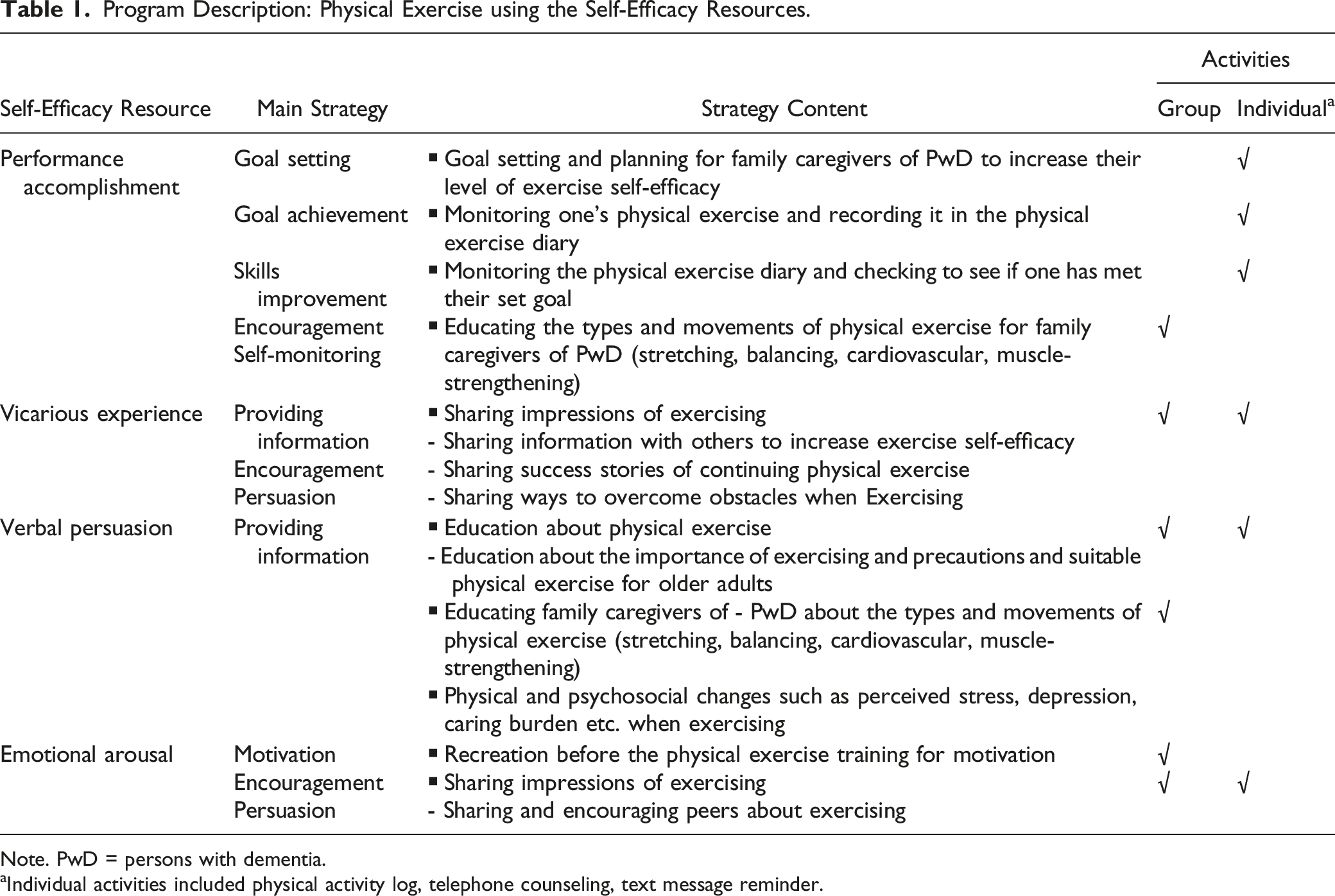
Note. PwD = persons with dementia.
aIndividual activities included physical activity log, telephone counseling, text message reminder.
In-group Activities
In-group physical exercise was carried out in the groups of 11-12 family caregivers. Each physical exercise session was lasted for 60 minutes and divided into four parts. First, before the physical activity, the participants began with recreation activities for relaxation and the feeling of safety (10 minutes). The activities help them feel at ease, safe and inspired to perform physical activity. Initial games, nonsense games and quizzes were utilized with the themes of physical activity, self-efficacy and caregiving for persons with dementia.
Then, the participants engaged in physical movement and exercise (30 minutes). Using a clip video, they completed a popular physical movement routine for 5 minutes (“gook-min chae-jo”) which all the participants were familiar with. The routine consisted of 12 movements performed to music and commands. The movements included preparation (walking in place), breathing (arms forward and down sideways), legs (knee push-ups), arms (arms swinging and swinging back and forth), neck (neck swinging), chest (chest bending), flanks (side-to-side push-ups), back (bend forward and lean back), torso (turn the torso sideways), whole body (roaming or netting), legs (jumping), limbs and legs (waving arms, bending knees and lifting one foot), and breathing (raising arms to breathe).
After the physical movement routine, additional stretching (palm grasp/finger grasp, neck stretch, raising shoulders, turning shoulders, body twist, leg stretches), balance (leg open, narrow walking, wide walking, walking in line), aerobic (marching in place/running in place, hip march, rowing, elbow to knee cross, jumping jack) and muscle-strengthening exercise (shoulder movement, chest movement, leg movement, squat, knee bends, trunk bending, shoulder raise/arm raise/leg raise) were incorporated for 20 minutes. The participants ended the physical exercise with final stretching movements for 5 minutes. If participants experienced fatigue during the exercise, they were instructed to sit and relax as needed. During the eight sessions, each of the balancing, aerobics, and muscle-strengthening were educated in detail in sessions 1 to 3. In sessions 4-8, all three physical activities were performed per day, helping each activity to be incorporated and carried out within 30 minutes.
After physical exercise, education about physical activity was given and followed by their sharing experience and feelings of exercising (15 minutes). Each education session was presented as a lecture, lasted 10 minutes and featured particular instructional topics. PowerPoint lecture slides and clip videos were used. Participants were invited to ask questions after the sessions. They were encouraged to express their feeling and experiences about performing physical activity. The discussions focused on increasing their knowledge, sharing success stories, and exchanging ideas on how to overcome challenges in order to improve their exercise self-efficacy. After the education, family caregivers took turns presenting their ideas and thoughts. Lastly, the participants had a time to create a goal for the following session and keep a physical activity log(5 minutes).
Individualized Activities
Study participants who participated in the in-group exercise were instructed to keep track of their physical activity log and to create a weekly goal. An individual meeting with the research team was scheduled before or after the exercise sessions in order to review physical activity logs and check if participants had achieved the target goal they had set the week before. The participants were encouraged with positive feedback so that they could maintain and keep continuing their exercise if they had achieved their goal. If the participants were unable to record or had fallen short of their target goal, they were given individual problem-solving assistance and motivation to exercise. The importance of self-monitoring was repeatedly emphasized. In addition, an individual telephone counseling along with text message reminder was provided between in-group exercise sessions. During the counseling, participants discussed any pain or discomfort they experienced as a result of the physical activity intervention or any physical activity they did at home, and any obstacle they encountered in exercising or keeping a record of physical activity logs. On average, they engaged in minimum 4 times per week except the first week of the intervention. In general, an individual meeting or counseling lasted for 5-10 minutes.
Measurements
Demographic information of study participants was collected. The characteristics of family caregivers included age, gender, marital status, educational level, religion, job status, perceived health status.
Caregiving-related information were obtained such as family relationship between caregivers and persons with dementia, living situation (living together or separately), length of caregiving (hours per day), availability of other caregivers, cost of caregiving per month, and type of dementia. In addition, in order to assess the extent of behavioral and psychological symptoms of persons with dementia, the modified Memory and Behavior Problems Checklist was used. 25 It has 24 items with a 4-point Likert scale.26,27 The total score ranges from 12 to 36, with higher scores suggesting higher frequency of problematic behaviors. 27
The effects of the intervention were measured in terms of self-efficacy (self-care, exercise), physical function, caregiving burden, depressive symptoms, perceived stress, and quality of life related to health.
Self-care self-efficacy was measured using the Self-Rated Abilities for Health Practices (SRAHP) which focuses on the particular self-efficacy of health-related behaviors. The 28-item questionnaire uses a 4-point Likert scale with the total score range of 28 to 112 points. Higher levels of self-care self-efficacy was indicated by higher scores. 28
Exercise self-efficacy was assessed using the Exercise Self-Efficacy Scale (ESES) which was an 18-item measure developed by Bandura.29,30 The measurement used a 10-point scale while the overall score ranged from 0 “cannot perform” to 100 “certainly can perform”. Higher scores indicated higher exercise self-efficacy, implying that participants can exercise on a regular basis regardless of their circumstances.
Physical function was measured using the Short Physical Performance Battery (SPPB). It consists of four m walking speed, balance and standing from a chair. 31 Scores of all three sections were added for a final score which ranged from 0 to 12 points. The final score was used to determine not only present physical condition but also relative risk of decline in daily living activities over the following four years. Higher scores indicated better physical function. 31
Caregiving burden was assessed using the Zarit Burden Interview (ZBI).32,33 The ZBI is a 22-item measurement with a 5-point Likert scale ranging from 0 “never” to 4 “always”. The total score ranged from 0 to 88, with higher scores indicating greater burden of caregiving. Its validity and reliability has been reported. 33
Depressive symptom was measured using the Geriatric Depression Scale Short Form (GDSSF).34,35 It is 15-item questionnaire and its validity has been reported. 35 Based on their feelings in the previous week, participants were instructed to reply either 0 “yes” or 1 “no” while the total score varied from 0 to 15. Higher scores indicating greater levels of depression. 34
Perceived stress was assessed using the 10-item Perceived Stress Scale (PSS). 36 The instrument used a five-point Likert scale with a total scare ranging from 0 to 40. Higher perceived stress level is reflected by higher scores.
The level of quality of life related to health was measured using World Health Organization Quality of Life-BREF (WHOQOL-BREF) which was a condensed version. 37 The 26-item measurement used with a five-point Likert scale that ranges from 26-130. Higher scores imply better quality of life related to health.
Procedure
Data was collected by the research assistant who did not participate in intervention and was unaware of which group participants belonged to. Prior to data collection, the research assistant received the training related to data collection, procedure and ethical consideration. Study participants were asked to complete survey questionnaires at baseline (pretest) and upon the completion of the 8-week intervention (posttest). The questions of the survey were read if they needed help.
Ethical Considerations
After the university’s IRB approved this study, data was collected. Written agreement was acquired from the three dementia care centers, and all the participants provided their written consent. To protect participants’ confidentiality, all of the data was coded by the researcher herself and stored in a lockable cabinet.
Data Analysis
Descriptive statistics (mean, standard deviation, frequency and percentage) were used to describe general characteristics and continuous research variables. Shapiro-Wilk test was employed to test the normality of study variables. Baseline characteristics between experimental and control groups were compared using independent t test, chi-square test, or Mann-Whitney U test. Then, the linear mixed effect model was used in order to examine the effects of the intervention on outcome variables. SPSS 23.0. was utilized for data analysis with a two-sided statistical significance level of P < .05.
Results
Participants’ Characteristics
General Characteristics of Participants.

Note. Exp. = Experimental group, Con. = Control group,
aFisher’s exact test done, *P < .05.
Caring-related Characteristics.

Note. Exp. = Experimental group, Con. = Control group.
MBPC = Memory and Behavior Problems Checklist.
aFisher’s exact test done.
bIndependent t test.
cMann-Whitney U test.
Intervention Outcomes
Results of Linear Mixed Morel for Outcome Variables.

***P < .001.
Discussion
The findings of this study indicate that the strategies to utilize self-efficacy resources may be critical to improve health outcomes in older family caregivers of persons with dementia. The results are consisted with the evidence of the significant relationship between self-efficacy and physical activity in previous studies.17,18,38,39 Thus, self-efficacy is an important component to be considered when a physical activity program is designed. That is, a physical exercise program for older family caregivers of persons with dementia needs to emphasize on caregivers' self-efficacy in order to be effective in improving health-related outcomes. The PA-SER program was designed to increase self-efficacy, promote behavioral changes, and sustain physical activity performance. In particular, this study shows not only that it is feasible to provide a theory-based physical activity intervention for family caregivers with persons with dementia but also that the strategies of utilizing self-efficacy resources may be effective to increase physical function, improve quality of life related to health, lower caregiving burden, and decrease depressive symptoms.
According to Bandura’s self-efficacy theory, 21 four main resources influence in the improvement of self-efficacy: performance accomplishment, vicarious experiences, verbal persuasion, and emotional arousal. Regarding performance accomplishment, successful accomplishment in one physical activity such as 30-minute exercise on bicycle machine may increase one’s confidence and expand to other tasks such as one-mile walk. However, failure in completing a task can lead to discouragement and decrease in efficacy. Thus, the content of PA-SER program was designed to be appropriate for the cognitive and physical abilities of family caregivers who were older adults, participants were encouraged to reach their goals and continue their physical activities through a review of physical activity logs. Vicarious experiences or observing others perform a physical activity can also help increase one’s self-efficacy. The participants in experimental group might feel more confident in their abilities in physical activity as the study participants witnessed others who were similar to themselves and completing physical movement and exercise in in-group sessions of the intervention. Verbal persuasion involves providing education of the importance of exercising, precautions when exercising, and suitable physical exercise for older adults. Education was provided each session in group and individually by telephone during the intervention. Emotional arousal such as anxiety and stress related to physical activity and exercise can negatively impact self-efficacy. The participants who participated in the intervention had the opportunities to express their feeling and experiences about performing physical activity. During the in-group and individual activities, they discussed any discomfort they experienced during exercise and exchanged tips on how to overcome difficulties to initiate or maintain physical activity.
The PA-SER program was carried out with one or two instructors depending on the size of group. If a designated exercise area can be reserved, the program can be delivered to family caregivers without requiring a lot of materials and preparation which gardening, music therapy and art therapy often need. Given that family caregivers of persons with dementia experience the difficulty in participating in physical activity due to time, place and expense, it is critical that a physical activity program like the PA-SER can be easily available and readily accessible to them in various settings.
Despite the intervention period in this study was shorter than previous research,19,40 it was effective to improve health outcomes in the participants of experimental group. Family caregivers often have the difficulty in scheduling for a regular class due to their caregiving situation. A shorter period of interventions may decrease drop outs and help family caregivers complete them. Because persons with dementia could not be left alone at home, exercise programs for family caregivers were offered at home, over the telephone or in a dyad with persons with dementia in previous studies.19–21 The PA-SER program was, however, delivered in person as a group as well as individually. The group sessions were arranged during the period when persons with dementia were in the cognitive therapy sessions in the dementia care centers. Thus, the family caregivers could spend the time to participate in the sessions and take care of their own health without worrying about their patients.
During the group exercise sessions, the family caregivers were motivated through others who were similar to themselves. In addition, they shared their feeling and experience about performing physical activity. Individually, they wrote physical activity logs about and received feedback regarding their goals, performance and progress through counseling and text messages. Previous research has shown that self-monitoring is useful to keep an individual on track of physical activity.41,42 Feedback on goals and progress help initiate and maintain exercise. 42
In this study, the level of perceived stress was not decreased significantly in the participants of the PA-SER program. The finding was inconsistent with those of previous studies.5,40,43,44 Family caregivers’ obligations and roles can be overwhelming and stressful. 40 Evidence shows that gradual decline in cognition, problematic behaviors and functional impairment of an individual suffering from dementia cause chronic daily stress in family caregivers.5,40,44,45 It is speculated that perceived stress was not decreased significantly because the PA-SER was not designed to address the sources of the stress.
The clinical implication of this study includes the strategies of making accessible a physical activity program for family caregivers of persons with dementia. In this study, the physical exercise sessions were scheduled during family caregivers’ waiting time while persons with dementia attend in their own cognitive program while an individualized telephone counseling and text message was used. Because the family caregivers are often unable to leave persons with dementia alone at home,19–21 it is critical to respect their schedule and make the programs accessible and person-centered. Furthermore, the PA-SER program have the potential to be utilized for those with limited opportunities in physical activities in not only dementia care centers but also various community centers.
Limitation
The findings may be limited in generalization because the study included only the participants who were able to attend in all the intervention sessions. In addition, the participants were recruited from three government-operated dementia care centers in two different geographical locations. Further resesearch is necessary to examine the effects of the intervention in various settings. In addition, there was the possible inaccuarcy of written self-report records due to old age, busy schedule and low literacy. It is necessary to use additional instruments including an assessment of participant’s fatigue during physical exercise in a future study. There was also the possibility of interactions among study participants although the participants in control group were asked to visit the center when there was no schedule of the PA-SER program so that they would not be able to make contact with those in intervention group. Because of the exploratory nature of this study, further research is needed to access long-term effects of the intervention through repeated measurement over a protracted period, such as six months or a year.
Conclusion
The findings of this study demonstrate that an 8-week physical activity program can improve exercise self-efficacy, self-care self-efficacy, physical function and quality of life related to health while reducing caregiving burden and depressive symptoms among older family caregivers of persons with dementia. Theory-based strategies for utilizing self-efficacy resources may be critical to improve health outcomes. The study findings suggest that increased self-efficacy needs to be included as a significant and measurable outcome when a physical activity program is implemented for the population. It is important to make an effective physical activity program easily accessible to them with dementia because it may benefit not only family caregivers but also persons with dementia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors declare to disclose any conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.