
Abstract
This work extends research suggesting a link between indicators of distress among informal caregivers (CG) (e.g., depression and burden), and potentially harmful behaviors (PHB), including feeling like yelling or screaming at the care recipient (CR). We tested three hypotheses regarding the role of a novel predictor, CG preparedness for caregiving, which were: 1) a direct effect between CG preparedness and PHB, 2) CG distress mediates the relationship between the direct effect of CG preparedness on PHB, and finally, 3) CG preparedness is only related to PHB through their shared associations with indicators of caregiver distress, an indirect effects model. Examining two indicators of PHB and CG depression and CG burden, results supported the indirect effects model. Higher CG preparedness was associated with lower CG distress, which in turn was associated with lower risk of PHB. These findings highlight the importance of CG preparedness as a target for caregiver intervention research.
Significance Statement
Caregiver preparedness for the caregiving role was demonstrated to be a protective factor against potentially harmful behaviors committed by a caregiver taking care of someone with Alzheimer’s disease and related dementias. Greater caregiver preparedness was associated with lower levels of caregiver depression and burden, which in turn were associated with lower levels of potentially harmful behaviors such as yelling or screaming at the care recipient.
Introduction
More than 11 million people currently serve as informal caregivers (CG) for individuals with Alzheimer’s disease and related dementias (ADRD). 1 The adverse impact of caregiving on the psychological and physical well-being of caregivers has been widely documented, 2 but less is known about the potential effect of caregiving distress on elder mistreatment and neglect. 3 Mistreatment can take many forms including physical, emotional, and sexual abuse as well as financial exploitation, neglect, or abandonment. 4 Although the prevalence of these behaviors is thought to be low, 3 potentially harmful caregiving behaviors (PHB), thought to be precursors of abuse, can be as high 25 percent 5 As suggested in the literature, PHB “may be thought of as an ‘early warning sign’ or precursor to full-blown elder abuse or neglect”, and can include behaviors or cognitions such as yelling and screaming at the CR, threatening to withhold food, and stopping oneself from hitting or slapping the CR. 5 In line with the theory of planned behavior, 6 an extensive body of research supports the claim that PHB, including abusive ideations or behavioral intentions, are precursors to elder abuse and neglect.7-10
Based on stress process models of caregiving, 11 prior research has often pointed to caregiver stress as a potential cause of elder mistreatment.12,13 CG depression and CG burden, typical components of stress process models 14 are related to PHB. Research that has examined the role of CG depression and PHB and found that higher levels of CG depression are linked to a greater risk of PHB.5,7,9,10,15,16
One of the important drivers of CG depression and burden is caregiver preparedness for the caregiving role,17-19 defined as the degree to which an individual reports being prepared for the emotional and pragmatic demands of caregiving. Preparedness has also been shown to be associated with greater caregiving rewards and more positive CG mental health, 20 less role strain and more positive caregiving/work balance. 21 Thus, overall, findings indicate a relationship between CG preparedness and CG mental health outcomes (e.g., depression, anxiety, burden) such that better caregiver preparedness is associated with better mental health outcomes. The goal of this study is to explore the relationship between preparedness, CG depression and CG burden, and PHBs in caregivers of persons with ADRD.
Present Study
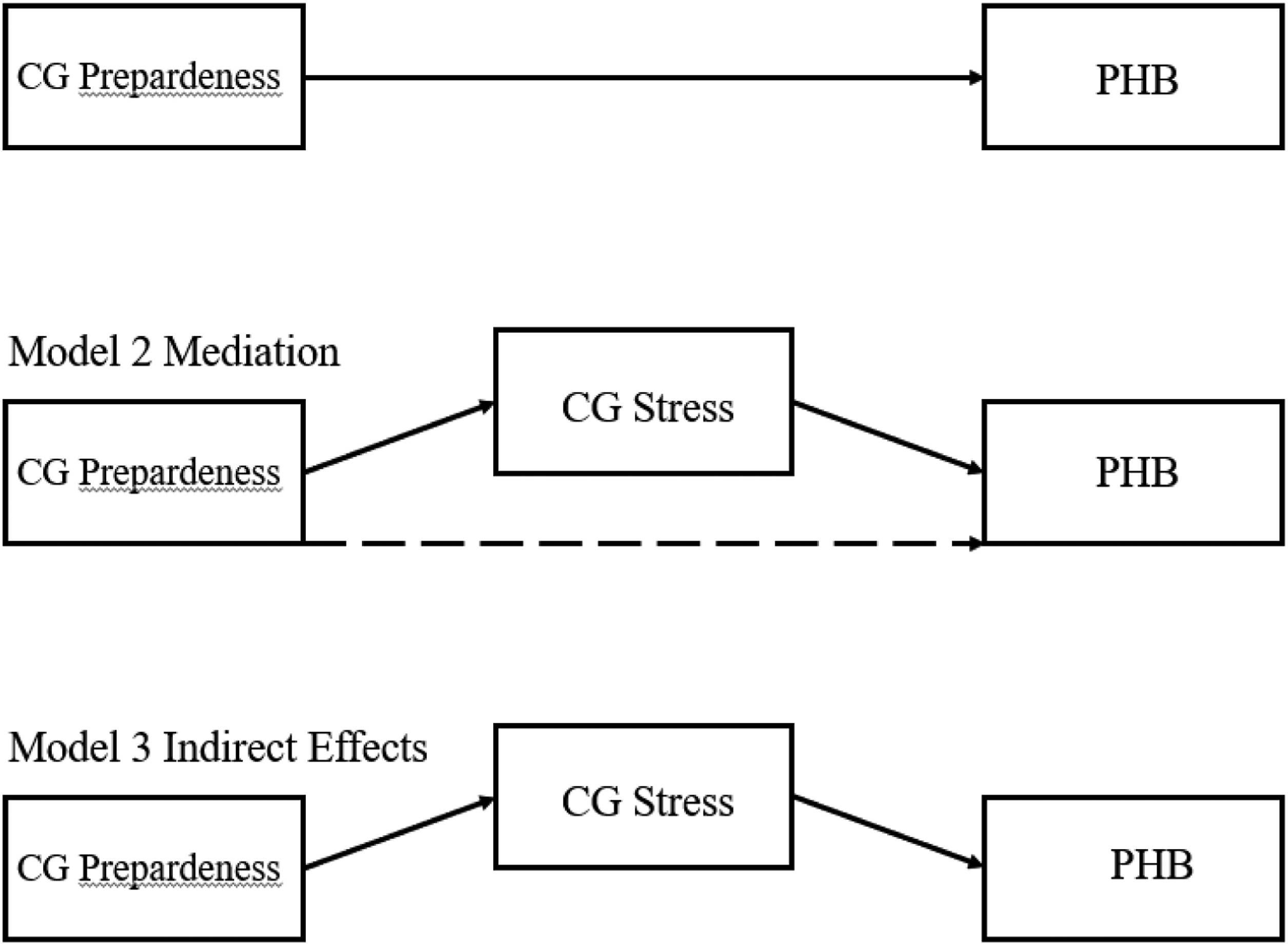
In this paper we take a two-stage approach to testing the association between preparedness, caregiver distress (depression and burden) and PHB (see Figure 1). Given the lack of information on the relationship between CG preparedness and PHB, we first test for direct effects between CG preparedness and PHB, wherein those who are more prepared will be less likely to engage in PHB. Based on the results of this direct effects model, we then test either a mediational model in which the effects of preparedness are hypothesized to be mediated through depression and burden to affect PHB, or an indirect effects model recommended in the literature which posits that CG preparedness is associated with PHB through CG depression and CG burden, in the absence of a significant direct association between preparedness and PHB (see Figure 2).22,23 Thus, the mediation model predicts a significant association between preparedness and PHDs, which is reduced when the depression and burden are added to the model as mediators of the relation between preparedness and PHDs. An indirect effects model is supported if the association between preparedness and PHDs is not significant, and preparedness is significantly associated with psychological distress (depression and burden) which in turn is significantly associated with PHDs. Analysis flow chart. Proposed Direct, Mediational, and Indirect Effects Models. Note: Dashed line represents non-significant effect for full mediation.
Methods
Participants
Analyses were based on data from a study examining the feasibility and efficacy of a multi-component psycho-social technology-based intervention for dementia family caregivers. The aim of the intervention was to improve CG quality of life. Participants were recruited via advertisements, presentations at support groups, and snowball sampling. The study population included 244 White, Hispanic, and Black/African American caregiver dyads that were randomly assigned to one of two groups: 1) The Intervention Condition 2) A Nutrition Attention Control Condition (NAC). The intervention was designed to address known areas of caregiver risk and to foster the ability of caregivers to leverage the type of supports they need for themselves and the AD patient. The intervention builds on the evidenced-based Resources for Enhancing Alzheimer’s Caregiver Health (REACH II) program. 24 The intervention was home-based and delivered in Spanish or English over 6 months using computer tablet technology and consisted of multimedia (text, voice and video clips, real time interactions) features that were placed within a customized website. The components included: skill-building sessions and modules; an annotated resource guide; an annotated reading list; information and tips, expert educational seminars (video), and structured support group sessions. The skill building sessions support groups occurred via a conferencing feature. The attention control group helped to ensure that these participants had access to the study technology and therapeutic contact but without the specific content of provided to the intervention condition. Assessments occurred at baseline, 6 months after completion of the intervention, and at 12 months after completion of the intervention. Measures included in these analyses are described below. All research was conducted with approval of the institutions IRB.
Measures
Caregiver Preparedness
CG preparedness was measured using the 8-item Preparedness for Caregiving Scale, 25 which provides self-report of how prepared CG felt for the CG role. Items were scored from 0 (not at all prepared) to 4 (very well prepared). All items were summed to create single summary score (range = 1-16, α = .86). Sample items include, “How well prepared do you think you are to take care of your family member’s physical needs?” and “How well prepared do you think you are to find about and set up services for your family member?”
Caregiver Depression
CG depression was measured using the short version of the Center for Epidemiological Studies – Depression scale (CES-D,26-28 which is a 10-item scale with response options ranging from 0 (rarely or none of the time) to 3 (all of the time). Scores were summed across the items, with higher scores indicating greater levels of depression (range = 0-30, α = .62). Questions asked about how the participant felt in the past week. Sample items include, “I felt depressed” and “I felt fearful.”
Caregiver Burden
CG burden was measured with the short-form Zarit Burden Interview, 29 which contains 12 questions, with response options ranging from 0 (never) to 4 (nearly always). Scores were summed across the items to create a single summary score, with higher scores indicative of greater burden (range = 0-43, α = .85). Sample items include, “Do you feel angry when you are around (CR)?” and “Do you feel that you have lost control of your life since (CR)’s illness?”
Potentially Harmful Informal Caregiving Behaviors
PHB were measured with a subset of items from the Risk Appraisal Measure (RAM). 30 Recalling that harmful ideations or behavioral intentions are classified as PHB, 7 two items were used to assess PHB related to yelling/screaming, an indicator of emotional/psychological PHB, and hitting/slapping, an indicator of physical PHB. Score options were 0 (never), 1 (sometimes), 2 (often), and 3 (always). For having to stop self from hitting or slapping the CR, 11.5% selected an option other than “never”, compared to 62.6% who selected an option other than “never” for felt like yelling or screaming at CR. Specific questions for these outcomes were, “How often in the past 6 months, have you felt like screaming or yelling at (CR) because of the way he/she behaved” and “How often in the past 6 months, have you had to keep yourself from hitting or slapping (CR) because of the way he/she behaved.”
Demographic Covariates
Multiple demographic variables were added to the models to help rule out alternative explanations and control for factors known to be associated with the variables of interest. CG covariates included age, gender, education, and ethnicity, as well as the CG-CR relationship. CR functional status (combined ADL/IADl), 31 was also included as a covariate, with higher scores indicating greater functional independence, or lower care needs.
Data Analytic Plan
Descriptive statistics for all variables were initially examined. All models were run in MPLUS.
32
Since all variables in the models, except for demographic covariates, were measured at all time points (baseline, 6 month follow up, 12 month follow up), a 1-1-1 multilevel structural equation mediation model, with time points nested within individuals, with fixed slopes was run to reduce model complexity, as random slopes models did not converge (see Figure 3).
33
Syntax for the model followed example I. 1-1-1 model with fixed slopes (MSEM) in the supplemental material provided by Preacher and colleagues.
33
All demographic variables were entered as level 2 covariates, as they were only measured at baseline and assumed to be constant, except for CR functional status, which was measured at each time point and thus entered as a level 1 covariate. Intervention condition was added as a level 2 covariate to control for possible effects of the intervention on the models of interest. All models were run with feeling like screaming/yelling and stopping from hitting/slapping as separate outcomes/models. Markov-Chain Monte Carlo (MCMC) methods were used to handle missing data. The first model tested a direct effect between CG preparedness and PHB. If the direct effect was significant, the second model tested whether the addition of burden or depression (in separate models) as mediators would result in a significant indirect effect between CG preparedness and PHB through depression and burden, separately. If the direct effect was non-significant in the first model, the mediation model was rejected and an alternative model was run examining whether there was a significant association between depression and burden which in turn were significantly associated with PHBs. Although both models are mathematically similar, we believe the distinction between models is important as the mediation model requires a direct effect between CG preparedness and PHB, whereas the indirect effect model does not. As suggested by Preacher and colleagues,
33
the mediated effect was computed as the product of the a and b paths. Multi-level structural model (1-1-1, MSEM).
Results
Sample Descriptives
Sample Descriptive Statistics (N = 244).

Note: May not equal 100% due to missing data or rounding. HS = High school, CG-CR Rel = Caregiver-Care recipient relationship
Model Testing
Model 1 -- Direct effect of CG preparedness on felt like yelling/screaming.

Model 3 -- Indirect effects model output with felt like yelling/screaming as the outcome.

Discussion
Overall, our findings indicate that among a sample of diverse caregivers of persons with dementia, CG preparedness was indirectly related to one of the two PHBs examined, namely, feeling like you want to scream or yell at the CR, which is the most frequently reported PHB. 5 More specifically, greater CG preparedness was associated with lower CG depression and lower CG burden, which in turn, were associated with lower risk of the CG feeling like yelling or screaming at the CR. The pattern of results for stopping self from hitting/slapping were similar, although not significant, likely because of the low frequency of this outcome (only 11.2% endorsed this item at any level other than “never”, compared to 62.6% for screaming/yelling). Overall, these findings are in line with prior research which demonstrates a relationship between CG preparedness and CG depression and CG burden,19,34,35 and CG depression and CG burden and PHB.5,9,10,15,16,36 Our findings extend prior work by simultaneously modeling the relationships among the CG preparedness, CG depression and CG burden, and PHB. CG preparedness was associated with fewer PHBs to the extent that it reduced CG depression and burden. Reversing CG preparedness and CG burden/depression variables in the indirect effects model resulted in non-significant models, providing further evidence of the path model from CG preparedness through CG depression/burden to PHB.
Our findings indicate that better CG preparedness is associated with lower depression and CG burden, which in turn is related to reductions in engagement in PHB. This is an important finding with respect to the development of future caregiver interventions as it underscores the importance of providing CG with education and training to help CG be better prepared for their caregiving role. Given the indirect effect through depression and burden, future work should also target CG depression and CG burden directly, as an alternative means to potentially reduce PHBs. For example, counseling interventions that target sources of CG depression or strategies such as engaging in pleasant activities might mitigate depression. Further, access to respite or other support services may help to alleviate CG burden.”
Examining the preparedness items individually, CG reported they were least prepared to deal with the stress of caregiving, making activities for the CR satisfying, and taking care of the CR’s emotional needs. These findings indicate the importance of educating CGs onstress management strategies. They also indicate that strategies that help the CGs create enjoyable activities that engage the CR, and strategies that help manage the emotional needs of the CR are important intervention targets. Reducing PHB may not only improve the quality of life for the CR but also for CG. For example, some CG may feel guilty because of thinking about or committing PHB, which may be negated if they are more prepared and do not engage in PHB which may in turn also help to reduce their distress. 37
Limitations and Future Directions
The findings in this paper are based exclusively on reports from the CG, future research should also include assessment from CRs when possible. Further, this study was conducted among a sample of dementia family caregivers and may not generalize to other types of caregivers or older adults in general. Finally, the study used two single items, adapted from a different measure of PHB as is traditionally used (the RAM instead of the Conflict Tactics Scale), though we consider this a strength, as it replicates prior work on PHB 5 using different methods. Nevertheless, future work should refine the measurement of PHB and elder mistreatment across a spectrum of severity and types.
Notwithstanding these limitations, the current study was able to demonstrate a consistent relationship between CG preparedness and CG depression and CG burden, and between CG depression and CG burden and PHB. The findings were consistent across a diverse set of caregivers (White, Hispanic, Black/African American). Moreover, the order of the variables was consistent, suggesting an indirect effect between preparedness and PHB. Future studies of caregiver interventions should include treatments that better prepare the caregiver for their role along with measures that assess these constructs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Nursing Research (5R01NR014434-05).