
Abstract
Introduction
Dementia is an increasing global health concern, particularly with the extending lifespan of human beings. As the most common clinical type of dementia, Alzheimer Disease (AD) accounts for up to 80% of all dementia cases.
1
The prevalence of age-dependent AD increasingly boomed by 146.2% from 2000 to 2018, becoming the fifth cause of death worldwide among people over 65 years of age.1,2 However, there is still a lack of an effective remedy for dementia. Therefore, it is of strategic significance to screen modifiable risk factors/behaviors in adulthood that could decrease the incidence of dementia in elderhood. With the rapid development of industrialization, shift work is increasingly required for numerous careers that offer 24 h of round service or production.
3
Approximately 16% of employees earning wages and salaries were scheduled for shift work in the U.S. in 2020 (https://www.bls.gov). Irrespective of its undetermined definition, shift work is generally defined as an employment practice that employs workers outside of the hours of 7:00
Methods
Data Sources and Literature Search
The present study was conducted following the guidelines of the Meta-analysis on Observational Studies in Epidemiology protocol (MOOSE) and the Preferred Items for Systematic reviews and Meta-Analyses (PRISMA) statement (Supplementary Table S1).33,34 A systematic literature search was conducted using electronic data from 3 databases: PubMed, Cochrane Library, and the Web of Science from their inception to 23 November 2021. Observational studies that provided estimates of the risk of shift work on dementia were extensively searched. The search terms were: “shift work, shiftwork” and “dementia, Alzheimer’s disease, Lewy body disease, primary progressive aphasia, progressive supranuclear palsy, Huntington disease, Creutzfeldt Jakob disease, and Wernicke Korsakoff syndrome.” The search results from the 3 databases are respectively addressed in Supplementary Table S2. Additionally, a hand search was carried out of all of the reference lists to identify all relevant original publications and reviews. No language restrictions were imposed.
Study Selection
Two researchers independently scanned the titles and abstracts. Animal studies, clinical trials, reviews, letters, and commentaries were excluded. A full-text scan was performed to identify potentially eligible studies. The eligibility of the studies was determined using the following 4 inclusion criteria: (1) Designed as an observational study, including a cohort or case–control study design; (2) included a measurement on shift work defined as either night work, evening work, irregular work, rotational work, or a combination of these; (3) provided an estimated risk of dementia based on a reliable diagnosis; (4) omitted shift work as the core cause of dementia with an independent reference group. Disagreement about the study selection was resolved by discussion and consultation to reach a consensus.
Data Extraction
Two authors independently extracted data, including information on the authors, publication year, country of origin, study design, sample size, number of cases, participant characteristics (age and gender), duration of follow-up, definition of shift work, dementia measurements, risk estimates, a corresponding 95%CI, and adjusted covariates in the statistical analysis. When the original studies had several adjustment models, the risk estimates that represented the maximum extent of adjustment for potentially confounding variables were extracted. Disagreements were discussed to reach a consensus.
Statistical Analysis
Meta-regression analyses were conducted the random effects models using DerSimonian and Laird method. During the present estimate of pooled risk ratios, hazard ratios and incidence rate ratios were deemed equivalent to RRs. The statistic I 2 was estimated to assess the heterogeneity of between-study variations: Values between 0 and 30% represented minimal heterogeneity; between 31 and 50%, moderate heterogeneity; exceeding 50%, To identify the source of potential heterogeneity, a subgroup analysis was conducted with baseline age (>50 and <50 years), gender, follow-up duration (>15 and <15 years), sample size (>5000 and <5000), number of dementia cases (≥100 and <100), schedule of shift work (evening shift, night shift, and rotating shift for cross-sectional schedule; evening–evening shift, night–night shift, rotating–rotating shift, and changeable shift for continuous schedule), and occupation (nurse or non-nurse). A statistical test of interaction was conducted to analyze the disparity between the subgroups. 35 All the analyses were performed with Stata version 16.0 (Stata Corp, College Station, TX). All the tests were two-sided, with a significance level of .05.
Quality Assessment
Sensitivity analyses were conducted to assess the impact of “missing” studies by sequentially removing 1 study at 1 time and re-pooling the remaining studies. 36 Publication bias was assessed with the Begg correlation test, 37 and the Egger linear regression method 38 and a visual inspection of the funnel plot. The study quality was assessed using the Newcastle–Ottawa Scale (NOS). 39 A study with at least 7 points was defined as a high-quality study.
Results
Study Selection
A search flow diagram is shown in Figure 1. We retrieved 1991 articles and retained 1786 unique references by removing duplicates. Using PRISMA-based reviewing, we retrieved 13 studies for full-text reviewing after excluding 37 reviews. Four cohorts were finally selected.29-32 During the search, 1 disagreement was that the same cohort was analyzed for 2 different outcomes (dementia incidence/dementia mortality).29,40 A consensus was reached by retaining 12 studies using dementia incidence as the outcome, characterized by a larger sample size and more details. In summary, 4 articles comprising 5 studies were included, addressing 8 risk estimates of dementia with shift work exposure. Search flow diagram for the systematic review on risk of dementia with shift work.
Study Characteristics
Characteristics of the Studies Included in the Meta-Analysis.

CMS, Copenhagen male study; STR, Swedish twin registry; SALT, Screening across the lifespan twin; DNC, Danish nurse cohort; DWECS, Danish work environment cohort study; NOS, Newcastle–Ottawa scale; ICD, International classification of diseases.
All the included studies were prospective cohort studies conducted in northern European countries (Sweden/Demark) and published within the last 5 years (2017-2020). These cohorts presented 3975 dementia cases from 84 492 participants, with an average follow-up duration of 9.8-41.2 years. The average age of the participants at baseline ranged from 37.8 to 60.9 years, indicative of the majority of the shift work exposure experienced in laboring time. Among these cohort studies, 1 study enrolled only occupational nurses
29
; the remaining 4 studies enrolled occupationally mixed populations.30-32 One study only enrolled male workers
32
; 1 study only female workers
29
; the remaining 3 studies included both male and female workers.30,31 For all cohorts, a broad definition of shift work was used and included workers working outside the conventional day time. One study categorized shift work schedules into 3 subtypes: Evening shifts (3:00
Meta-RRs of Dementia With Shift Work Exposure
Twelve reports from 4 cohorts presented a positive association between shift work exposure and the incidence of dementia, while only 2 reports presented a negative 1. The pooled RR of dementia with shift work exposure was 1.15 with 95%CI 1.02∼1.30 (Figure 2). Forest plot of risk estimation of dementia with shift work exposure.
The meta-regressed findings have address high overall heterogeneity (I2 = 52.8%, P = .016), which was category to considerable heterogeneity (greater than 50%). 41 As all the studies were of good quality (NOS scores are shown in Supplementary Table S3), sensitivity analysis was further conducted by leave-one-out analysis to show the consistency of the pooled RR.
Sensitivity Analysis
We obtained the influence of 1 single study by respective new meta-estimated effect using sensitivity analyses (Figure 3, Supplementary Table 4S). An overall symmetric distribution was shown as 7 increased pooled RRs and 5 decreased pooled RR by omitting-one-study-at-a-time. The largest fluctuation was shown by removing 2007 (remaining pooled RR = 1.198, 95%CI 1.075∼1.335) or by removing 2018(STR) (remaining pooled RR = 1.115, 95%CI .982∼1.265), which were close to the overall effect. Therefore, the pooled RR of dementia with shift work exposure was considered stable. New overall meta-analysis effect by removing a single study at a time.
Publication Bias
No evidence of publication bias was shown by using Egger’s test (P = .687) or Begg’s test (P = 1.000) (Supplementary Figure S1). We also visualized the publication bias by the funnel plot (Figure 4). The results indicate that the combined estimate and 95%CI were not influenced by any single report. Funnel plot for the relative risks of dementia with shift work exposure.
The symmetry of the funnel plot indicates no publication bias in the present meta-analysis on the risk of dementia with shift work exposure. The solid vertical line represents the summary effect estimates. The dotted lines are pseudo 95%CIs.
Subgroup Analysis of Risk of Dementia with Shift Work Exposure
Pooled Risk Estimation of Dementia with Shift Work Exposure, by Sub-Group.
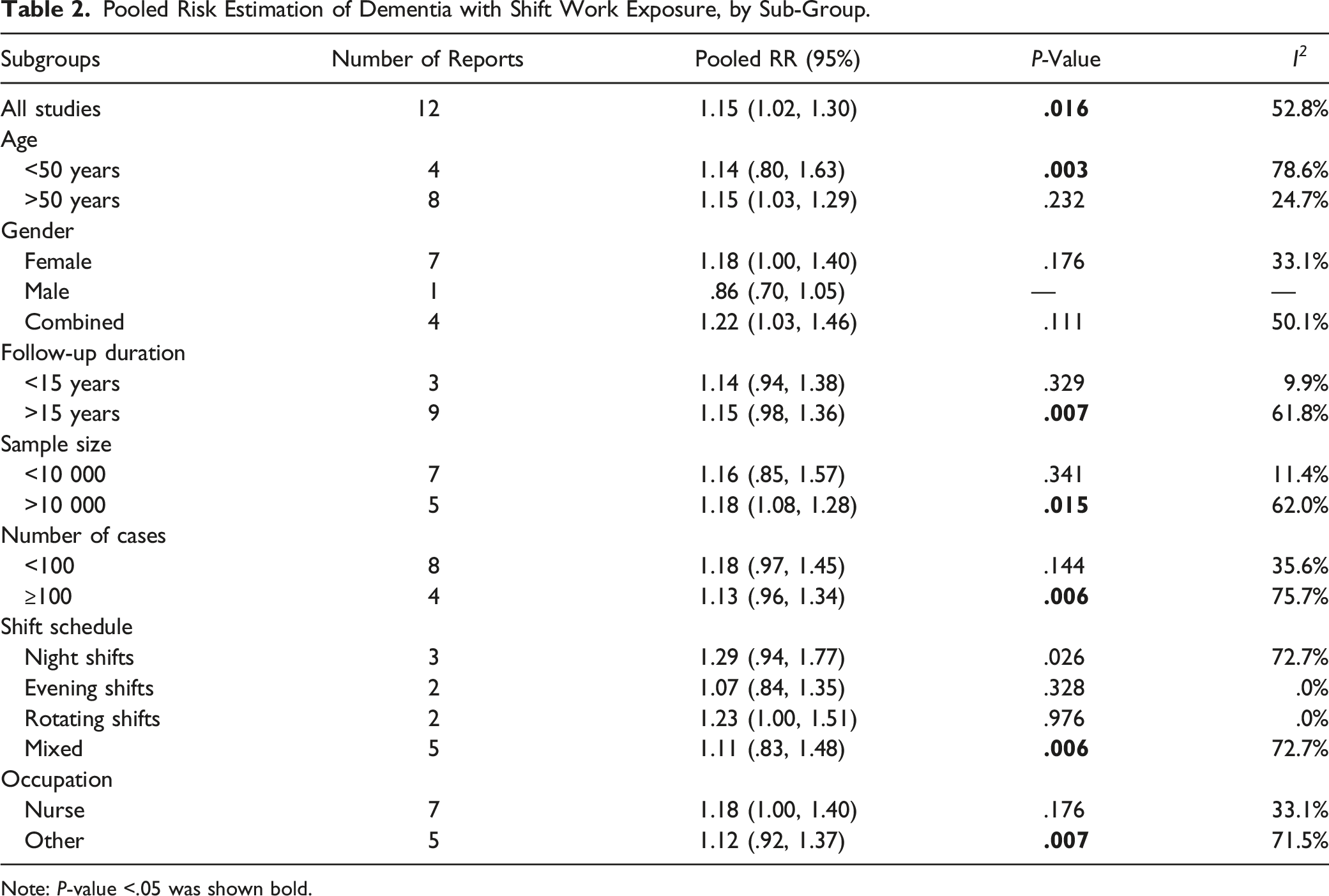
Note: P-value <.05 was shown bold.
No significant variation was shown in the risk of dementia between the 2 age-dependent subgroups. Notably, the reports on population-based shift workers displayed the significantly increased pooled risk, characterized with subgroups harboring larger size, more dementia cases and longer follow-up duration (all P < .0%). Also, the mixed schedule addressed a remarked increase of pooled risk. It was shown that occupational nurses harbored a significant yet slight increase in the risk of dementia compared to non-nurses, largely due to its relatively small size. Of note, all significantly influenced subgroups addressed considerably high heterogeneity, which could well explain the overall 52.8% heterogeneity in the present analysis.
Only Jorgensen et al stratified shift work schedules into 3 subtypes: Evenings, nights, and rotation. They also compared RRs between cross-sectional data and longitudinally continuous data to determine if the risk of dementia increased with a cumulative effect. Interestingly, it was shown that continuous evening shifts exhibited a decreased risk of dementia compared to temporary evening shift work or other schedules. 29 Moreover, a changing shift schedule presented a relatively low risk of dementia. Therefore, these findings indicate that temporary and mild impairment due to shift work might be modified and even reversed by compensatory good rest. However, continuous night shifts exhibited a significantly high risk of dementia compared to temporary night shifts or other schedules.29,31 Taken together, long-term cumulative exhaustion due to an affected circadian rhythm could not be reserved anymore, instead exaggerating the impairment. Another notable issue is that the subgroup analysis of shift schedules was conducted merely on occupational nurses. As the majority of elderly patients are vulnerable in the early hours, stressful shifts might also contribute to an increased risk of dementia for continuous night shift nurses.
Discussion
The present review comprised 80 567 participants with 3707 diagnosed dementia cases. Overall, the pooled analysis of all included studies supports the idea that shift work is associated with an increased risk of dementia (RR = 1.15, 95%CI = 1.02-1.30, P = .016). Such a mild increase in pooled 15% RRs had consistent significance in the majority of the subgroups, including in the population with a long follow-up, large sample size, and many dementia cases. One attributable reason for this is that these cohorts harbored a much larger sample size and more dementia cases. An increased risk was also shown in occupational nurses. The significance in these subgroups partially reflects the cumulative chronicity of dementia. However, some controversial results compelled us to explore the potential mechanism underlying shift work and cognitive impairments that might promote the occurrence of dementia. Thus, we conducted a systematic narrative review between shift work and cognitive impairment. A search flow diagram for risk of cognitive impairment with shift work was shown in Supplementary Figure S3. According to our findings, the 4 analyzed publications indicated that shift work significantly impairs cognitive function with a dose-dependent effect.24,25,42,43 Moreover, an exponentially sharp trajectory could be seen when the shift work endured over 10 years. 24 However, a reverse or restoration of cognitive decline has also been found with long-term removal from shift work exposure for more than 5 years,24,42 indicating that impairment from shift work exposure is age-dependently cumulative and could also be modified due to the long-term scenario. In another 3 publications, no significant association was shown between long-term shift work exposure and declined cognition.15,27,28 Based on these contradictory publications, it is still inconclusive in terms of whether long shift work negatively impacts psychoneurological function from a chronic perspective.
Our meta-analysis has several strengths. This is the first meta-analysis to systematically analyze the association between the risk of dementia and shift work exposure. Moreover, all included studies had high NOS scores. All diagnosed dementia cases were identified based on the ICD system from nationwide databases.
Several caveats must be noted. First, as there is no well-accepted definition of shift work, 44 vague definitions of shift work were used. Varied schedules and/or regimens of shift work, varied intensity, and varied spans between shifts might produce a heterogenous impact on the results. Second, dementia is a clinical syndrome with a wide spectrum and heterogeneous diseases. We conducted the present meta-analysis based on the ICD root criteria without sub-stratification. As the top 2 common dementias, 45 vascular dementia (VaD) was shown to be closely correlated to numerous cerebrovascular pathologies, including atherosclerosis, large vascular diseases, and microvascular diseases, 46 all of which could be promoted with shift work exposure based on previous meta-analyses.11,47-50 Therefore, an interaction effect between shift work, vascular risk, and neurological risk should be intensively estimated. Third, shift work definitely disturbs sleep, which indirectly decreases temporary cognition. 4 However, unlike long-term occupational sleep loss, 28 some types of shift work might be working 3 shifts, followed by 3 days off.51,52 The temporary cognitive impairment related to short-term sleep disturbance could be restored or refreshed by compensatory sleep, vacation, or a long rest. 28 These findings indicate that temporary sleep disturbed by shift work is modifiable. It has also been documented that more than 5 years without shift work could reverse declined chronic cognition due to previous shift work.24,25,42 Therefore, optimal original data should indicate the continuity of shift work exposure. Fourth, the majority of dementia cases occur in the elderly,53,54 however, normal aging per se accelerates cognitive decline and degeneration55,56 and is accompanied by poor sleep,57,58 the present meta-analysis could not separately adjust the aging-dependent interactive effects within. In another cohort study, using mortality from dementia as the outcome addressed a much higher risk of dementia with shift work exposure. 40 Therefore, more interactive studies between dementia and aging due to shift work are required. Fifth, considerably high heterogeneity was shown. Sixth, numerous potential confounders, including the age at which a shift worker first engaged, individual’s genetic diversity, and the adaptability of the circadian clock in response to shift work, 59 et,al. could not be analyzed due to data unavailability.
In conclusion, experienced shift workers had a mildly increased risk of dementia in later life based on the present meta-analysis. Given the increase in shift work in the industrialization world and the heavy care and economic burden of dementia, more awareness is required about shift worker health promotion. More cohort studies with a larger size, longer follow-up, better definitions, and optimal schedule data are required for more convincing findings.
Supplemental Material
Supplemental Material - Does Long-Term Shift Work Increase the Risk of Dementia? A Systematic Review and Meta-Analysis
Supplemental Material for Does Long-Term Shift Work Increase the Risk of Dementia? A Systematic Review and Meta-Analysis by Yang Hai, Ying Xue, and Yu-hong Wang in American Journal of Alzheimer's Disease & Other Dementias®
Supplemental Material
Supplemental Material - Does Long-Term Shift Work Increase the Risk of Dementia? A Systematic Review and Meta-Analysis
Supplemental Material for Does Long-Term Shift Work Increase the Risk of Dementia? A Systematic Review and Meta-Analysis by Yang Hai, Ying Xue, and Yu-hong Wang in American Journal of Alzheimer's Disease & Other Dementias®
Footnotes
Acknowledgments
We thank Dr. Zun-song Hu for the long-term supports on data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.