
Abstract
The AD7c-NTP is a promising biomarker for AD diagnosis. However, the exact urinary AD7c-NTP concentration to differentiate AD from the mild cognitive impairment (MCI) remains inconclusive. We enrolled 98 and 90 clinical defined AD and MCI patients, respectively, and access their cognition impairment with Neuropsychiatric Inventory (NPI) and Mental State Examination (MMSE) along with their urinary AD7c-NTP. We demonstrated that urinary AD7c-NTP level in sequence from high to low was AD, MCI, and healthy groups (P < .01), and the AD7c-NTP was positively and negatively correlated with the NPI and MMSE scores, respectively. Additionally, AD7c-NTP well-matched NPI subscale scores, including agitation, depression, and apathy (P < .05). Importantly, the optimal cut-off AD7c-NTP level to distinguish the AD and MCI was .94 ng/mL (sensitivity 85.71% & specificity 73.91%). Conclusively, urinary AD7c-NTP could be used for cognition impairment evaluation and differentiated diagnosis of AD and MCI.
Significance Statement
The exact urinary AD7c-NTP concentration to differentiate AD from the mild cognitive impairment (MCI) remains inconclusive. We identified that urinary AD7c-NTP could be used for cognition impairment evaluation and differentiated diagnosis of AD and MCI.
Introduction
The senior population has been rapidly growing across the world. According to the United Nations, there were 703 million persons aged 65 years or over in the world in 2019. 1 It is apparent that the senior population imposes great demands on society and health care systems, one important cause of which is due to cognitive impairment. Mild cognitive impairment (MCI) is the most common cause of cognitive impairment, which accounts for approximately 6.7% to 25.2% of the eld population in advanced countries. 2 Moreover, 10% to 15% of MCI can progress to dementia, mostly in the form of Alzheimer’s disease (AD), especially in elderly patients.3,4 Due to the overlapping clinical features between MCI and AD, the current cognitive screening battery leads to a high misdiagnosis rate. 5 Thus, it is extremely critical for the efforts to find novel screening tools and biomarkers to differentiate between MCI and AD. So far, MRI or fluorodeoxyglucose PET (FDG-PET) are used for improving diagnostic accuracy by proving distinct topographic patterns between MCI and AD. However, the excessive cost and radiation exposure of PET impede their clinical application. Additionally, other biomarkers in the cerebrospinal fluid (CSF), such as Aß1-42 and T-tau are also limited to utility due to their invasive collection methods. Thus, this is desirable to use alternative biomarkers, which feature high sensitivity and specificity for the differentiated diagnosis of MCI and AD.
In 1997, Monte et al 6 isolated a 41-kD protein from an AD brain library. This protein was designated as the Alzheimer-Associated Neural Thread Protein (AD7c-NTP) since it was specifically overexpressed in AD brains. Since the AD7c-NTP is also actively secreted by the neurons to the CSF, the CSF AD7c-NTP was proposed as a biomarker to correlate with the severity of dementia symptoms. 6 Interestingly, in the subsequent study, Ghanbari et al 7 demonstrated that the AD7c-NTP protein was also detectable in the urine and featured a high accuracy for AD diagnosis. Thus, the urinary AD7c-NTP-based assay was developed and used for clinical evaluation of elderly patients at risk for AD.8,9 In recent studies, some research focused on the diagnostic role of urinary AD7c-NTP in MCI.10,11 However, the exact AD7c-NTP concentration to differentiate AD from MCI remains inconclusive.
In the current study, we hypothesized that the urinary AD7c-NTP levels were different between MCI and AD patients. After enrolling clinical defined AD and MCI cases, we tried to find out an optimal cut-off urinary AD7c-NTP concentration, at which MCI and AD could be differentiated from each other. Additionally, we also hypothesized that urinary AD7c-NTP levels could be used to objectively assess the severity of cognition impairment in AD and MCI. We performed the correlation analysis between AD7c-NTP with various neuropsychiatric symptoms (NPS) to understand their potential correlation.
Materials and Methods
The study protocol was approved by the Research and Ethics Committee of Shanghai Jiao Tong University Medical College Affiliated No.9 People’s Hospital.
Participants’ Enrollment
The AD patients were enrolled if they fulfilled the following inclusion criteria: (1) diagnosis of AD according to the criteria of the United States National Institute of Neurology Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA); 12 (2) > 50-year-old; (3) able to understand the contents of the interview; (4) cognitive dysfunction results only from AD, but no other disorders; (5) not on any drugs that may affect cognition. The MCI group was recruited during the study period if they fulfilled the following inclusion criteria: (1) > 50-year-old; (2) diagnosis of MCI according to the Petersen’s MCI criteria; 13 (3) not on any drugs that may affect cognition. All patients or their guardians provided the voluntary provision of written informed consent. Eventually, 98 AD and 90 MCI were enrolled. At the same time, 42 matched healthy participants were also enrolled for control purposes.
Sample Collection
Subjects’ 24 hours urine samples were collected and kept in a refrigerator (4°C) for up to 7 days. After collection, all samples were instantly centrifuged for 30 minute at 5000 rpm in a 50 mL aliquot. The supernatant was then filtered through a .2 µ acetate filter under a vacuum. Then 2 mL filtrate was collected and centrifuged at 5000 rpm for 30 minute. The precipitate was kept and washed twice using TBS (pH 7.0) and stored at 20°C for further testing.
Cognitive Assessment and Neuropsychological Tests
All participants underwent a standardized neuropsychological assessment, which used the mini-mental state examination (MMSE) and Neuropsychiatric Inventory (NPI). 14 The current version of NPI evaluates 12 NPS commonly observed in dementia. The investigator recorded the frequency of symptoms in the domain on a four-point scale from 1 (occasionally; less than once a week) to 4 (very frequently; more than once a day). Additionally, the severity of NPS was rated from 1 (mild) to 3 (severe). Each NPS yields a domain rating of 1-12 by multiplying the severity and frequency scores, which helped to achieve a final general NPI score.
Biological Sample Testing
Urinary AD7c-NTP was assayed using an AD7c-NTP ELISA kit (Biorbyt, Cambridge, UK). A microplate reader at 450 nm wavelength was used to measure the optical density (OD) value and calculated the AD7c-NTP concentration based on the standard curve from recombinant human AD7c-NTP peptides (Biorbyt, Cambridge, UK).
Statistical Analysis
Data were analyzed by SPSS Statistics 21 (IBM®, Endicott, US) while the graphs were generated by GraphPad Prism 8.1 (Graphpad®, San Diego, US). All data were presented as mean ± SD. The normal distribution of data was tested using the Anderson-Darling method. The one-way analysis of variance (ANOVA) testing was used to identify the difference in data among AD, MCI, and healthy groups. The Spearman’s rank correlation measures the strength and direction of association between urinary AD7c-NTP and MMSE, NPI, and NPS. The level of statistical significance was set at P < .05.
Results
Demographic Features of all Participants
The Demographic Features of All Participants.

Neuropsychological Assessment Revealed Varied Cognition Impairment in AD and MCI Patients
The Comparison of Cognitive and Neuropsychological Profiles Among MCI, AD, and Healthy Groups.

*Indicated a significant difference between the AD and MCI group while the # indicated a significant difference between the healthy group and the AD or MCI group.
*and #indicated P < .05; **and ##indicated P < .01.
To further understand the differences in neuropsychiatric disturbances among the 3 groups, we further evaluated 12 NPS listed in the NPI (Table 2). As compared to the healthy group, the AD and MCI demonstrated 7 and 3 significantly disturbed NPS (all P < .05), respectively. Among these NPS, agitation, apathy, and depression all scored the highest value in both AD and MCI groups. Additionally, agitation, apathy, and depression were in more severe status in the AD group than in the MCI group (all P < .01).
Urinary AD7c-NTP Levels Varied Among Different Groups
The levels of AD7c-NTP protein measured in control urine samples were uniformly low (.4 ± .14, Figure 1). Meanwhile, in confirmed cases of AD, the AD7c-NTP level was more broadly distributed, and the mean values were significantly higher than the control (1.23 ± .38, P < .001). The urinary AD7c-NTP of the MCI group was .67 ± .38 ng/mL, which was prominently lower than the AD group (P < .001), but remained higher than the healthy group (P < .001). Comparison of urinary AD7c-NTP levels between AD, MCI, and healthy groups. The AD groups exhibited a significantly higher urinary AD7c-NTP level (1.23 ± .38 ng/mL) than that of the MCI groups (.67 ± .38 ng/mL, P < .01). Meanwhile, the urinary AD7c-NTP levels in the healthy group were low (.4 ± .14).
Urinary AD7c-NTP Levels Demonstrated a Good Correlation with Cognition Impairment
The Correlation Between Urinary AD7c-NTP Level and Neuropsychological Symptoms in MCI and AD Patients.
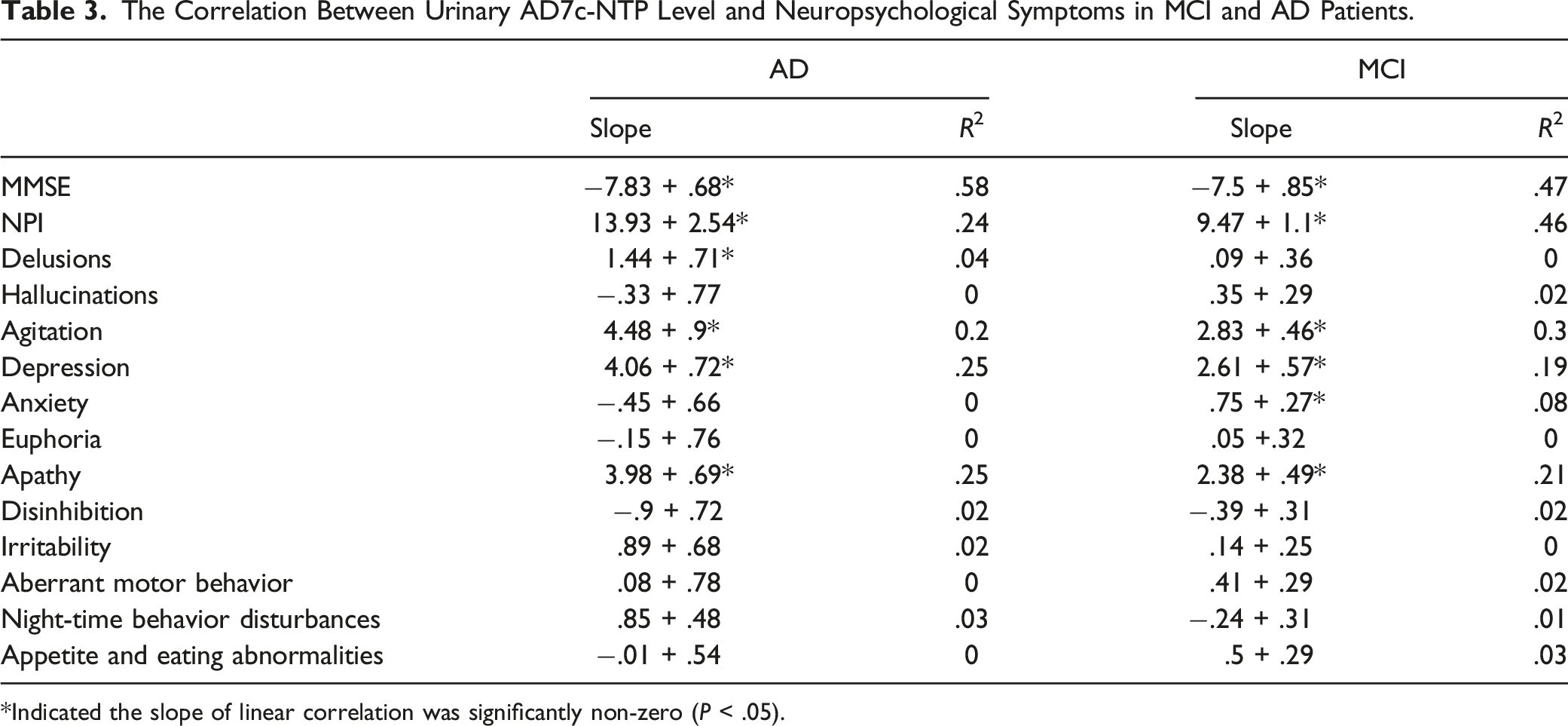
*Indicated the slope of linear correlation was significantly non-zero (P < .05).
Urinary AD7c-NTP Levels Could Distinguish the AD and MCI
To determine the utility of AD7c-NTP for differentiated diagnosis of AD and MCI, we conducted an operating characteristic (ROC) curve analysis and calculated the optimal cut-off value based on the maximum sum of sensitivity and specificity. First, our results showed that the optimal cut-off urinary AD7c-NTP concentration to distinguish the MCI from the healthy group was .62 ng/mL, at which the sensitivity and specificity were 97.62% and 58.7%, respectively (Figure 2A). Meanwhile, using the cut-off concentration at .76 ng/mL, the AD7c-NTP showed a sensitivity of 100% and specificity of 90.82% to differentiate the AD from the healthy individual (Figure 2B). Most importantly, we found that the optimal cut-off value to distinguish the AD and MCI for AD7c-NTP was .94 ng/mL, at which the sensitivity and specificity were 85.71% and 73.91%, respectively (Figure 2C). The ROC curve depicts the sensitivity and specificity (1- sensitivity) of urinary AD7c-NTP for discrimination between (A) MCI and healthy group, (B) AD and healthy group, and (C) AD and MCI group, whose area under the curve (AUC) is .77 (95% CI .7 to .85), .99 (95% CI .97 to .99) and .84 (95% CI .79 to .9), respectively. The data indicated that the optimal cut-off urinary AD7c-NTP concentration to distinguish the MCI-healthy group, AD-healthy group and AD-MCI were .62 ng/mL (sensitivity 97.62% & specificity 58.7%), .76 ng/mL (sensitivity 100% & specificity 90.82%), and .94 ng/mL (sensitivity 85.71% and specificity 73.91%), respectively.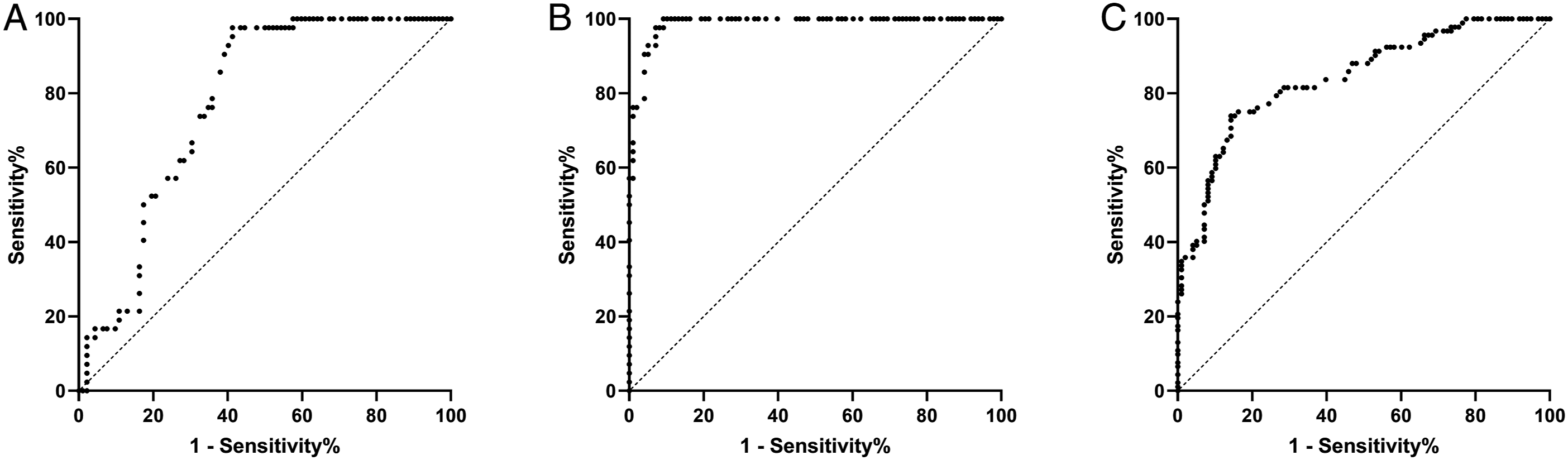
Discussion
AD is a progressive and irreversible neurodegenerative disease, characterized by a progressive loss of learning, memory, orientation, language, comprehension, judgment, and intellectual performance. Meanwhile, the MCI is the stage between the cognitive decline of normal aging and the more serious decline of dementia. Due to high similarities in terms of symptoms, the clinical differentiated diagnosis of AD and MCI remain a challenging evaluation process. In the current study, we compare the urinary AD7c-NTP level patients with either AD or MCI. We identified that urinary AD7c-NTP level in sequence from high to low is AD, MCI, and healthy group. At .95 ng/mL, urinary AD7c-NTP reached its optimal cut-off centration for distinguishing the MCI from AD.
The neuronal thread protein (NTP) is a family of developmental regulation molecules that are expressed in the brain and the neuroectodermal tumor cell lines.15,16 Previous studies demonstrated that the NTP is tightly associated with neuronal proliferation and differentiation.16,17 However, in 1997, Monte et al 6 first identified a novel member of the NTP family (a.k.a. the AD7c-NTP), which was highly expressed in the AD brains. Further studies demonstrated that AD7c-NTP reduced neuron survival in vitro 18 and promote neurodegenerative sprouting and synaptic disconnection in vivo 19 From then on, the role of AD7c-NTP in AD was actively pursued. It is now evident that AD7c-NTP is tightly associated with the pathological process of AD. Standing at a histology level, both AD7c-NTP mRNA and protein accumulate in the neurons in the frontal and temporal lobe in human AD brain samples. 6 Additionally, the AD7c-NTP was actively secreted by the neurons to the CSF, which significantly elevated the CSF AD7c-NTP level in cases of definite AD as compared to the age-matched group.6,20 Interestingly, the concentration of AD7c-NTP was positively correlated with the severity of dementia6,21 and cerebral amyloid-β deposition. 22 Based on this information, novel assays targeting the CSF AD7c-NTP were developed, and the diagnostic sensitivity and specificity were as high as 89.3% and 84.7%, respectively.23,24 However, collecting CSF remains an invasive method and patients must bear severe complications of lumbar puncture. Excitingly, Ghanbari et al 7 identified that AD7c-NTP protein is sufficiently small enough to be excreted into the urine. Moreover, Ghanbari demonstrated that the AD7c-NTP proteins in urine have the same molecular mass as in CSF and cerebral tissue, and test results of both sample sources have similar accuracy. 7 A subsequent study indicated that urinary AD7c-NTP level is higher in the urine of AD patients than in the normal population. 25 Previously, a clinical trial using urinary AD7c-NTP assay also demonstrated high sensitivity (89%) and specificity (90%) for AD diagnosis. 26 Thus, the urinary AD7c-NTP is now known as a non-invasive biomarker for AD diagnosis. In the current study, our data also supported this statement as we demonstrated that urinary AD7c-NTP is significantly elevated in AD patients as compared to the control group. Additionally, AD7C-NTP values identified patients with AD with a sensitivity of 100% and specificity of 90.82% at a cut-off concentration of .76 ng/mL. These values were close to previously reported data.7,27 Thus we believe that urinary AD7C-NTP could be a useful diagnostic tool for clinical usage as it meets the characteristics of the qualified biomarker for AD diagnosis as previously proposed. 13
The MCI is an intermediate stage between cognitive health and dementia,28,29 and up to 15% of MCI can progress to dementia, mostly in the form of Alzheimer’s disease. However, diagnostic criteria for MCI are a very complicated process, which includes concerns regarding a change in cognition, abnormal cognitive function in one or more domains, normal daily activity, and absence of dementia.30,31 Additionally, unlike AD, MCI is thought to be reversible when caused by certain treatable factors. Thus, accurate diagnosis of AD and MCI is of particular importance as they require different interventions. Hence, adding appropriate screening assays becomes a crucial part of the clinical diagnosis and evaluation of patients with MCI. So far, only a handful of studies focused on the correlation between urinary AD7c-NTP and MCI. For example, a previous study showed that the level of urinary AD7c-NTP in MCI patients was higher than in healthy people, 11 suggesting a potential diagnostic feature of AD7c-NTP for MCI. Additionally, Zhang et al 22 also demonstrated a significant difference in urinary AD7c-NTP levels between AD and MCI. However, the exact cut-off value of AD7c-NTP to distinguish AD and MCI remains inconclusive. In the current study, we presented that the urinary AD7c-NTP concentrations were 1.23 ± .38 and .67 ± .38 ng/mL in AD patients and MCI subjects, respectively, which was consistent with the previous study. 22 Additionally, we reported that the optimal cut-off AD7c-NTP concentration to distinguish the AD and MCI was .94 ng/mL, at which the sensitivity and specificity were 85.71% and 73.91%, respectively. To our best knowledge, the current study not only supports the results from previous studies,11,22 but also, for the first time, provided the exact cut-off concentration of urinary AD7c-NTP for differential diagnosis of AD and MCI. Due to the wide overlapping clinical symptoms between AD and MCI, we believe that urinary AD7c-NTP is not only a supplementary tool for AD and MCI diagnosis, but a potentially useful biomarker for differential diagnosis of AD and MCI.
NPS affects nearly all dementia patients over the course of their illness. Not surprisingly, the insidious nature of AD is also associated with a collection of NPS. According to previous studies, 97% of AD patients present at least one NPS, 32 among which apathy, depression, and agitation rank the top 3.33,34 A consensus has emerged that apathy is tightly associated with the severity of cognitive impairment. 35 Meanwhile, agitation is associated with more advanced dementia and adversely impacts cognitive status, functional status, and rate of cognitive decline. 36 These findings were consistent with what we found in the current study, as our data exhibited significantly elevated NPI subscale scores in delusion, hallucination, agitation, depression, euphoria, apathy, and aberrant motor behavior in AD patients. Moreover, we also demonstrated a higher NPI score in agitation, depression, and apathy for the MCI, which also overall matched with a previous study. 37 However the matched NPI scores, only one study so far had used urinary AD7c-NTP to correlate certain NPS. 22 Since accurately and subjectively NPS assessment is important in evaluation, medication and prognosis for AD and MCI, we thus correlated the urinary AD7c-NTP with every single item of NPI. Similar to previous results, 22 we found that urinary AD7c-NTP is well correlated with agitation in AD patients. Additionally, we had also shown that delusion, depression, and apathy were also well correlated with AD7c-NTP. This result indicates that urinary AD7c-NTP levels can reflect the severity of 4 NPI subscale scores and indicate overall cognition impairment status. Interestingly, we detected that, in both AD and MCI groups, urinary AD7c-NTP level was significantly and positively correlated with agitation, depression, and apathy. Literature indicated that the Tau protein deposition in the orbitofrontal and anterior cingulate cortex is closely related to the agitation symptoms in AD. 38 Neuroimaging study demonstrated that the neurological dysfunction in the right temporoparietal and anterior cingulate cortex is responsible for apathy.39,40 Additionally, depression is associated with institutionalization 41 and higher mortality, 42 which is mainly due to the significant reduction in serotonin transporter binding in the prefrontal cortex in AD. 43 This information indicated that urinary AD7c-NTP was able to reflect the potential damages in these anatomic regions and indicate the severity of cognition impairment, which could be useful in evaluating the therapeutic outcome and long-term prognosis for AD and MCI. Additionally, the Tau protein is the major constituent of intraneuronal and glial fibrillar lesions described in the AD. Since the Tau and AD7c-NTP can mutually promote the deposition of each other in neurons,44,45 the urinary AD7c-NTP could potentially be a biomarker to monitor Tau deposition in the brain.
The current study bared the following limitation. First, the sample size was relatively small. Since we were validating a biomarker for AD and MCI differentiated diagnosis, the small sample size could affect the power of the study. Secondly, due to the study design, the urinary AD7c-NTP levels were studied in a cross-sectional pattern rather than in a time-sequential pattern. A longitudinal study is required to verify the diagnostic accuracy of urinary AD7c-NTP and provide more information regarding the prognostic role of AD7c-NTP. Moreover, the kinetics of the AD7c-NTP (from secretion to excretion) and contributing factors remain inconclusive. This missing information may affect how we interpret the AD7c-NTP data from the current study.
In conclusion, we identified that urinary AD7c-NTP level in sequence from high to low is AD, MCI, and healthy group. This indicated that urinary AD7c-NTP could help in the differentiated diagnosis of AD and MCI. Additionally, since the urinary AD7c-NTP level was tightly correlated with severity of the NPS (especially for agitation, depression, and apathy), urinary AD7c-NTP could be used as an assessment method for not only cognition impairment, but also the therapeutic outcome and long-term prognosis in AD and MCI management.
Footnotes
Acknowledgments
We want to express our sincere acknowledgment to all the personnel helping us to complete the current study.
Author Contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by Prof. Ming-Ran Xu. The first draft of the manuscript was written by Prof. Ying Hu, Ming-Ran Xu, and Qing-Qi Wei. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current study is funded by the Scientific Research Program of Huangpu District, Shanghai (HKM201912).
Ethics Approval
The research protocol was approved by the Research and Ethics Committee of Shanghai Jiao Tong University Medical College Affiliated No.9 People’s Hospital (2019-Q-023).
Data Availability
All data are available upon reasonable request.