
Abstract
Objectives:
Assessments of unawareness in Alzheimer’s disease mainly focus on the objects (the “what”) of unawareness. A recent person-centered approach proposes to also assess the processes (the “how”). The present study combines 2 approaches to understand this heterogeneity in assessments of unawareness.
Method:
We recruited 46 participants from 8 nursing homes. They underwent a semi-structured interview and were assessed using a prediction–performance paradigm. Spearman correlations were calculated, and generalized additive models were established.
Results:
The 2 approaches are associated through cognitive deficits, confrontation with difficulties and identity changes. Objects (the what), mechanisms, and modes of expression (the how) explain at least 29.6% of the variance of unawareness.
Conclusions:
Unawareness is more than simply being unaware of something; it is a synergy between the objects and processes of arousal and expression. Moreover, unawareness extends beyond the disease to include the self. Considering the entire person seems to be necessary.
Introduction
Assessments of unawareness in Alzheimer’s disease (AD) can be divided into 3 approaches: an explicit system of reference, an implicit system of reference, and qualitative or person-centered methods. 1 The first 2 approaches are the most commonly used in AD and have recently been used in combination to provide a broader understanding of unawareness. 2,3 Whereas an explicit system of reference refers to comparisons with a social or cognitive norm, an implicit system of reference refers to a professional assessment of unawareness. 1 However, unawareness in AD is still assessed through objects (i.e., the “what”) of deficits such as memory impairments, and the understanding of unawareness is removed from the daily lived experiences of people with AD. In contrast, a grounded approach provides the possibility of understanding the unawareness of people with AD through their discourses by considering the objects of unawareness and mechanisms and modes of expression (i.e., the “how”). 4,5 Based on this approach, a recent assessment tool for unawareness that includes these two processes of awareness has been developed and validated. 1 To further develop this approach, the similarities and differences between these 2 perspectives on unawareness (i.e., a comparison focusing on objects and a subjective perspective including the mechanisms and modes of expression) must be understood. We propose a combination of an assessment with an explicit system of reference (i.e., a prediction–performance paradigm) and a new subjective assessment. Given the heterogeneity of assessments of unawareness in AD, the present study aims to understand how such assessments rate the objects and/or processes of this phenomenon.
A Focus on the Objects of Unawareness in AD
Studies assessing unawareness in AD have mainly focused on objects, which are presented as the first aspect to consider in the phenomenon of “understanding patients’ conditions and clinical variables.” 6 Marková et al. (2005) specified that the objects of unawareness can be a deficit from the disease (e.g., memory, functional abilities) or an aspect of daily life or the person (e.g., activities of daily life, relationships). This variety of objects studied in unawareness derives from their heterogeneity. 7 Indeed, studies on unawareness have shown a distinction between unawareness of a memory deficit and unawareness of other cognitive functions 8 or psychological symptoms such as depression. 9 The heterogeneity of objects also influences assessments of unawareness. For example, Hannesdottir and Morris (2007) 10 observed that memory and executive functions were affected differently in assessments of unawareness.
To provide valuable and important information about these aspects of unawareness, various assessment tools have been developed 11,12 ; these tools consider discrepancies between performance and predictions or discrepancies between informant and patient ratings (i.e., assessments with an explicit system of reference) and clinician ratings (i.e., assessments with an implicit system of reference). 1 Through these assessments, we can understand that people with AD are more or less unaware of something. This unawareness refers to many objects ranging from the most studied item—memory 13 —to more pragmatic items such as financial abilities. 14 However, when researchers choose a method of assessment for unawareness, they focus only on part of it. 6 To obtain a broader perspective on unawareness, researchers have combined different assessments mainly through explicit systems of reference. 15 -17
Recently, studies on unawareness have included the implicit system of reference and neurological indicators (e.g., magnetic resonance imaging 2,3 ) or reviewing people’s lived experiences. 1,5,18 However, the perspective of people with AD seems to be insufficiently explored in the understanding of unawareness. To address this challenge, from a phenomenological perspective, qualitative and person-centered approaches have been proposed to analyze the subjective experiences of people with AD.
A New Perspective to Understand the Awareness of Disease: Personal Experience
Subjective experiences in many domains of daily life can contribute to the understanding of the unawareness in people with AD. 18 In one study, Emery Trindade et al (2018) used an assessment with an explicit system of reference (i.e., the Assessment Scale of Psychosocial Impact of the Diagnosis of Dementia) combined with a qualitative analysis. The authors observed that certain people with AD can provide stable information about their lived experiences with the disease. Although this original combination associated 2 distinct approaches to unawareness and provided a person-centered approach, the conclusions still focused on the objects of unawareness (e.g., people with AD are aware/unaware of cognitive deficits, health conditions, social functioning, relationships, and changes in activities of daily living). From a phenomenological perspective of reviewing people’s lived experiences beyond objects, some researchers have proposed modeling AD individuals’ unawareness of disease. 4,5 Based on discourses about daily life with the disease, Billiet et al. (2009, 2010) obtained valuable information and built a comprehensive model of unawareness that extended beyond objects. This model is composed of 3 distinct domains: objects (e.g., the disease, the relations), mechanisms (e.g., observation of the environment, confrontation with difficulties), and modes of expression (e.g., to deny, to be bewildered). The first domain refers to the classical “what” of unawareness, while the last 2 refer to the “how” of unawareness (how unawareness arises and how it is expressed). These domains represent unawareness based on discourses with people with AD. According to this model, a new assessment of unawareness consisting of these 3 domains and based on the subjective experiences of people with AD and their associated perspectives is proposed. 1
In summary, there are 2 main perspectives on the assessment of unawareness in AD. The first involves assessments through a system of reference (implicit or explicit), which have demonstrated success and provided valuable information to understand the objects of unawareness (the “what”). The second perspective involves a renewed interest in the lived experiences of people with AD to understand their unawareness of disease (including the “how”). To our knowledge, these 2 perspectives have not yet been explored together. Our objective is to propose an original combination of these assessments (i.e., a person-centered approach and an assessment with an explicit system of reference). We aim to provide information about unawareness in AD by adopting a broad perspective from the “what” to the “how.” To do so, we propose 3 hypotheses. First, the “what” (i.e., the objects assessed by the person-centered approach) will be associated with the unawareness of deficit score from the assessment with an explicit system of reference. Second, the “what” items and the “how” items referring to cognition (e.g., memory deficit, confrontation with difficulties) from the person-centered approach will be more associated with the unawareness of deficits from the assessment with an explicit system of reference. Finally, we hypothesize that the synergy of items from the “what” and “how” of the person-centered approach can predict the unawareness of deficit score from the assessment with an explicit system of reference.
Method
Participants
This observational study was conducted in 8 institutions in North France. Each participant provided written informed consent. The University of Lille ethics committee granted ethical approval. To be included, participants had to have been diagnosed with AD by an experienced neurologist or geriatrician based on the National Institute on Aging-Alzheimer’s Association clinical criteria, 19 to be native French speakers or able to speak French with the investigator, and to have no history of traumatic brain injury, psychiatric illness, or cerebrovascular disease.
The sample consisted of 46 participants (mean [M age] = 84.5 years, SD = 7.27; M MMSE = 18.15, SD = 4.39). This sample included 40 women (aged 72-100 years, M = 84.98 years, SD = 6.69; Mini-Mental State Examination [MMSE] from 9 to 26, M = 17.68, SD = 4.33) and 6 men (aged 71-92 years, M = 81.33 years, SD = 10.61; MMSE from 18 to 28, M = 21.33, SD = 3.67). Each participant participated in 1 individual interview for the subjective measure and 1 paradigm prediction performance.
Measures
Awareness of Self and Disease Assessment: Unawareness from discourses
The Awareness of Self and Disease Assessment (ASDA) involved a semi-structured interview conducted by a trained investigator that followed themes such as mood, emotions, well-being (physical and psychological), daily life, self-perception (body, personality), family, friends, relationship changes, cognitive functions, memory loss, elderly experiences, disease, and expectations for the future. 1 It assessed 3 aspects: objects, mechanisms, and modes of expression. Objects are the basis of changes and new information perceived by people with AD (e.g., the environment, emotions, the body, communication, autonomy, identity changes, loss of cognitive abilities, and the disease). Mechanisms are the processes of unawareness (e.g., observation of the environment, perception of the expressions of others, comparison between the past and the present, metacognition, and confrontation with difficulties). Modes of expression are how people with AD express their unawareness of the disease and/or the self (e.g., denial, bewilderment, attribution, description, judgment, recognition of the need for help, the use of coping strategies, and confirmation of the disease). The items for mechanisms and modes of expression are rated on a 6-point Likert scale ranging from “minimally present” to “extremely present” (1: “minimally present,” 2: “slightly present,” 3: “mildly present,” 4: “moderately present,” 5: “strongly present,” and 6: “extremely present”). The object items are rated on a 6-point Likert scale ranging from “strong unawareness” to “strong awareness” (1: “strong unawareness,” 2: “mild unawareness,” 3: “slight unawareness,” 4: “slight awareness,” 5: “mild awareness,” and 6: “strong awareness”). A lower rating is associated with high impairment of awareness. Every item could not be detected during the interviews. When this was the case, the item was noted as “not assessed.” For statistical analyses, the mean of the 22 items can be calculated, but in practice, the ASDA provides “a profile” of unawareness rather than a score.
Multidimensional Isomorphic Simple Awareness : Unawareness from a prediction–performance paradigm
The Multidimensional Isomorphic Simple Awareness (MISAWARENESS) procedure is based on a self-assessment followed by a real performance test through tasks to assess unawareness of deficits in AD. 8,20 Each task derives from the Dementia Rating Scale. The tasks refer to cognitive functions labeled attention, initiation, construction, conceptualization, and memory. In detail, the investigator communicates the task and asks a person with AD to predict his or her performance. Four cases are possible: (1) right prediction, failure to perform; (2) right prediction, successful performance; (3) wrong prediction, successful performance; (4) wrong prediction, failure to perform. Two scores are calculated: the real score corresponding to the number of correct answers and the level of deficit of the actual performance and the prediction score. From these results, an anosognosia score is calculated for each cognitive function separately, which is the difference between the real score and predicted score. An anosognosia total score is also calculated considering cognitive functions as a whole.
Procedure and statistical analysis
All statistical analyses were performed with R (version 3.5.2) and the packages “MissMDA” and “FactoMineR” to offset the missing values. Preliminary analysis (i.e., Shapiro–Wilk tests) was conducted to verify statistical assumptions of normality. Given the small sample size (N = 46), normality of the distribution was not detected; thus Spearman correlations were used to establish correlations between the ASDA and MISAWARENESS with the package “SpearmanCI” to include information about confidence intervals (CIs). Generalized additive models with the package “mgcv” were used to observe the influence of ASDA on MISAWARENESS.
Results
Preliminary Results: Influence of Cognitive Deficit on Unawareness
For the cognitive information, the MMSE score correlated significantly with the total score of unawareness assessed by MISAWARENESS (r = −.313, P = .034, 95% CI [−.593, −.031]), the subscale “Initiation” (r = −.340, P = .021, 95% CI [−.602, −.077]) and the subscale “Construction” (r = −.368, P = .012, 95% CI [−.679, −.056]) (Table 1). The MMSE score was not correlated with the domains of unawareness assessed by ASDA (Table 1). Contrary to MISAWARENESS, the unawareness observed through ASDA was not influenced by the impairment of cognition assessed by the MMSE.
Summary of General Data: Correlations Between the Domains of Each Scale.a

Abbreviations: ASDA, Awareness of Self and Disease Assessment; MMSE, Mini-Mental State Examination; MISA, MISAWARENESS; r, Spearman correlations.
a Values in square brackets refer to the 95% confidence interval for each correlation.
b P < .05.
c P < .01.
Comparison of the Domains of the Two Approaches Assessing Unawareness
In this part, we aim to determine the correlations between the objects representing the unawareness score from MISAWARENESS and the objects, mechanisms, and modes of expression from ASDA.
A first observation is the significant associations between the total score of unawareness obtained by MISAWARENESS and the domains of “objects” (r = −.470, P = .000, 95% CI [−.732, −.206]), “mechanisms” (r = −.480, P = .000, 95% CI [−.752, −.206]), and “modes of expression” (r = −.423, P = .003, 95% CI [−.683, −.162]) obtained by the ASDA (Table 1). A higher unawareness score for people with AD in the prediction–performance assessment corresponded to a higher unawareness score for objects of the ASDA and less appropriate use of the mechanisms and modes of expression as assessed by the ASDA. Contrary to our hypothesis, the strongest correlation was found between the total MISAWARENESS score and the domain “mechanisms,” whereas the total MISAWARENESS score had the lowest correlation with the domain “objects.”
Deficits in the use of the “mechanisms” of awareness assessed by the ASDA were correlated with the subscale of MISAWARENESS: unawareness of “initiation” (r = −.402, P < .005, 95% CI [−.688, −.116]) and “memory” (r = −.347, P = .017, 95% CI [−.621, −.073]; Table 1). Deficits in the use of the “modes of expression” of awareness assessed by the ASDA were correlated with the subscales of MISAWARENESS: unawareness of “initiation” (r = −.331, P = .024, 95% CI [−.604, −.058]) and “memory” (r = −.334, P = .023, 95% CI [−.632, −.034]; Table 1). The unawareness of “objects” assessed by the ASDA was significantly correlated only with the unawareness of the “memory” subscale (r = −.476, P = .001, 95% CI [−.755, −.200]; Table 1). We can observe that the unawareness obtained through the “mechanisms,” “objects,” and “modes of expression” assessed by the ASDA was mainly correlated with the unawareness obtained through the “initiation” and “memory’ subscales assessed by MISAWARENESS.
Correlations Between the “what” and “how” of Unawareness From the 2 Perspectives
Fifteen of the 22 items of the ASDA were significantly correlated with the total unawareness score of MISAWARENESS (r from −.309 to −.545; Table 2). These 15 items refer to 2 mechanisms (M4: metacognition and M5: confrontation with difficulties); 6 objects (O1: environment, O3: body, O4: communication, O6: identity changes, O8: memory, and O9: disease); 7 modes of expression (E2: bewilderment, E3: attribution, E4: description, E5: judgment, E6: recognize the need for help, E7: use coping strategies, and E8: confirmation of the disease).
Data Summary of Correlations With Significant Subscales of MISAWARENESS.a
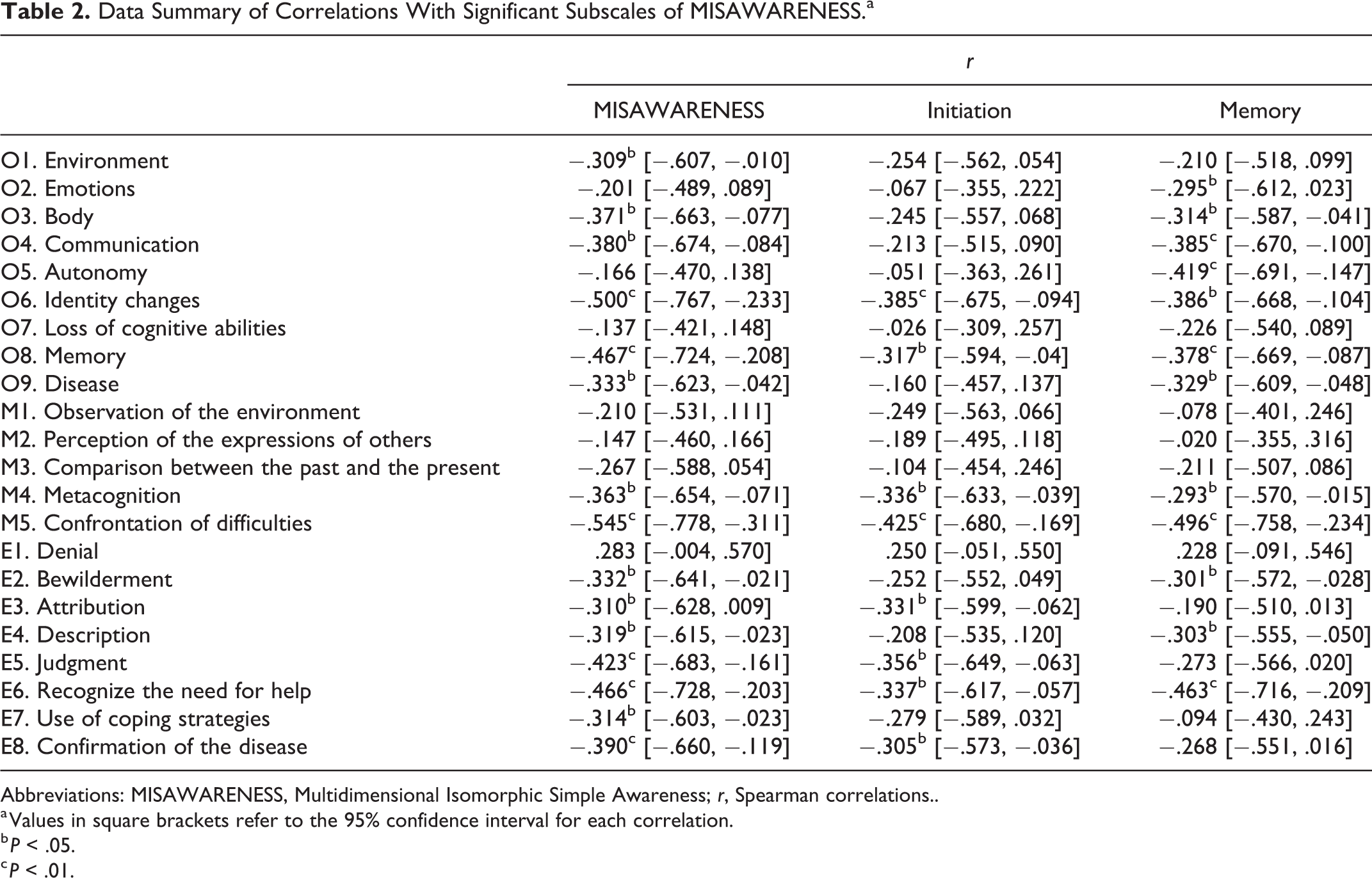
Abbreviations: MISAWARENESS, Multidimensional Isomorphic Simple Awareness; r, Spearman correlations..
a Values in square brackets refer to the 95% confidence interval for each correlation.
b P < .05.
c P < .01.
For the objects (the “what”), for people with AD, greater unawareness of their cognitive difficulties as assessed by MISAWARENESS corresponded to greater unawareness of the environment, their bodies, their difficulties in communication and memory, their identity changes, and their disease.
For the mechanisms and modes of expression (the “how”), greater unawareness of people with AD according to MISAWARENESS corresponded to less appropriate use of metacognition, confrontation with difficulties, bewilderment, attribution, self-description, judgment, recognition of help, coping strategies, and confirmation of the disease. Thus, our hypothesis is partially confirmed. Indeed, with the exception of denial, the 2 other items of the ASDA (i.e., confrontation with difficulties [M5] and recognizing the need for help [E6]) were closer to the conceptual perspective of MISAWARENESS and had significant correlations with it.
The “initiation” and “memory” subscales of MISAWARENESS showed recurrent significant correlations with some items of the ASDA. There were 8 significant correlations between the subscale “initiation” and the items of the ASDA (r from −.305 to −.425). These 8 items referred to 2 mechanisms (M4: metacognition and M5: confrontation with difficulties), 2 objects (O6: identity changes and O8: memory), and 4 modes of expression (E3: attribution, E5: judgment, E6: recognize the need for help, and E8: confirmation of the disease). There were 12 significant correlations between the subscale “memory” and the items of ASDA (r from −.293 to −.496). These 12 items referred to 2 mechanisms (M4: metacognition and M5: confrontation with difficulties); 7 objects (O2: emotions, O3: body, O4: communication, O5: autonomy, O6: identity changes, O8: memory, and O9: disease); 3 modes of expression (E2: bewilderment, E4: self-description, and E6: recognize the need for help).
We also observed the recurrence of associations (i.e., correlation with the total score, “initiation” and “memory”) for 5 items of ASDA. These 5 items referred to 2 mechanisms (M4: metacognition and M5: confrontation with difficulties), 2 objects (O6: identity changes and O8: memory), and 1 mode of expression (E6: recognize the need for help). Except for the item “identity changes” (O6), these correlations between ASDA items and the total score and the MISAWARENESS subscales followed the conceptualization (i.e., a prediction–performance paradigm) and the objects (i.e., cognitive functions). These observations confirmed our second hypothesis. However, the exceptions of the strong correlations (r = −.500, P = .000, 95% CI [−.767, −.233]; r = −.385, P = .008, 95% CI [−.675, −.094]; r = −.386, P = .008, 95% CI [−.668, −.104]) between the MISAWARENESS total score, the initiation subscale, the memory subscale, and the item “identity changes” support the hypothesis of a larger process associated with the awareness of disease.
In these results, we can observe correlations between the objects and mechanisms and modes of expression from 2 different perspectives of unawareness. These correlations also indicate the scope of unawareness with regard to its many objects. To extend our understanding of unawareness, we applied 2 generalized additive models between the 2 assessments.
Implication of the “How” on the “What” of Unawareness
We observed that the “what” (i.e., the objects) is correlated with the “how” (i.e., the mechanisms and modes of expression) of unawareness. To go further, we examined how they are explained in relation to each other through 2 generalized additive models. The first model was composed of the domains of ASDA as predictive variables, and the second model was composed of the 5 most significant items of ASDA as predictive variables.
In the first model, we considered the domains of ASDA (i.e., the objects, mechanisms, and modes of expression) as predictors of the total score of unawareness obtained by MISAWARENESS. In this model, the 3 domains explained 29.6% (P = .000) of the variance of unawareness obtained by MISAWARENESS (Table 3). The mechanisms and modes of expression (the “how”; P = .219 and P = .331, respectively) had a greater influence than the objects (the “what”), but this observation by domain is not significant (Table 3). For this model, the synergy of the domains of the ASDA seems to be more influential than each domain alone.
Details of the Effects Identified by the Generalized Additive Models.

Abbreviations: F, F test value; MISAWARENESS, Multidimensional Isomorphic Simple Awareness; r 2, r 2 adjusted by the generalized additive models.
In the second model, we considered the 5 most significant items of ASDA (i.e., M4: metacognition, M5: confrontation with difficulties, O6: identity changes, O8: memory, and E6: recognize the need for help) as predictors of the total score of unawareness obtained by MISAWARENESS. This model (i.e., the 5 items) explained 41.2% (P = .000) of the variance of unawareness obtained by MISAWARENESS (Table 3). The mechanism (i.e., confrontation with difficulties) and the mode of expression (i.e., recognize the need for help; P = .140 and P = .154, respectively) had a greater influence than the objects “identity changes (O6)” and “memory (O8)”; P = .591 and P = .582, respectively; Table 3). Again, this observation by item is not significant. For this model, the association of the items of ASDA had a greater influence than each item.
Discussion
The literature on unawareness in AD provides valuable information about the assessments of objects of unawareness. Recently, studies have shown the possibility for people with AD to talk about their experience of the disease and to use these discourses (i.e., themes or how they express themselves) to assess the level of unawareness. The originality of this person-centered approach is its extension from objects to mechanisms and modes of expression of unawareness. In the current study, we propose an original combination of assessments (i.e., a prediction–performance paradigm and a person-centered approach) to understand the heterogeneity of unawareness from the “what” (i.e., the objects) to the “how” (i.e., the mechanisms and modes of expression).
We expected that the “what” (i.e., the objects assessed by the person-centered approach) would be more associated with the unawareness of deficit score from the assessment with an explicit system of reference. Contrary to this hypothesis, we observed that the mechanisms and modes of expression of ASDA (i.e., the “how”) were more associated with MISAWARENESS than the domain of “objects” (i.e., the “what”). With or without significant results, the more unaware people with AD were according to MISAWARENESS, the more unaware they were of objects in the ASDA, and the less they used mechanisms and modes of expression according to the ASDA. These associations were particularly evident for “initiation” and “memory” in MISAWARENESS. These subscales of MISAWARENESS were previously observed as the most relevant for heterogeneity. 8 However, our results are original because, contrary to the literature, processes (i.e., mechanisms and modes of expression) were more correlated than objects, which were previously observed to be largely correlated between approaches. 2,3,15 -17 Thus, we suggest that the assessments that have been developed thus far should consider and score more than the objects of unawareness (i.e., “being unaware of something”). In the case of MISAWARENESS, the assessment seems to score the mechanism of the comparison of one’s own cognitive deficit at 1 time. Each type of assessment captures a specific mechanism and/or mode of expression according to the conceptualization (e.g., confrontation to difficulties for the prediction–performance paradigm, comparison between the past and the present for the comparison between people with AD and caregivers’ discourse, and denial or bewilderment for the clinician ratings). The use of only one type of assessment would explicitly capture some objects and implicitly capture part of the processes of unawareness. Our study provides proof of the entanglement of objects and processes in unawareness and, consequently, the need to consider them as explicitly as objects.
In the second part, we hypothesized that the correlations between the domains of each approach were based on specific items. We postulated that the “what” items and the “how” items from the person-centered approach, referring to the conceptual perspective of the other assessment (e.g., memory deficit, confrontation with difficulties) would be more associated with the unawareness of deficit from the assessment with an explicit system of reference. We obtained these relevant associations for 5 items of ASDA. They mainly concern cognitive deficits or refer to the conceptual perspective of MISAWARENESS. 20 These observations also support the first results and interpretations of the associations. Nevertheless, a specific association was original: the association with identity changes in ASDA. This item, an object of unawareness, is not in the conceptualization of MISAWARENESS but presented the most significant association with the total score of unawareness. When people with AD were unaware according to MISAWARENESS, they were unaware of their identity changes according to the ASDA. From this observation, we can propose different assumptions. First, we propose an interrelationship between the awareness of disease and the awareness of self. In the awareness of self, people are able to represent themselves and their identity characteristics from an “objective view.” 21 This process is associated with autobiographical memory, and how people build their stories. 22 In identity building, people integrate and reject some events and characteristics. This movement has been observed in people with AD with an alternation between integration and rejection of AD as a new part of the self. 23 If people with AD reject AD and its deficits, they do not regard the disease as a change in their identity and fail to elaborate it or express it and become aware of the present self (i.e., an elderly person with a chronic disease). This hypothesis of an overlap between the awareness of disease and the awareness of the self should be explored through self-statement exercises. 24 From a more pragmatic perspective, the second assumption is that this association between cognition and identity changes may be the result of the specific context of the semi-structured interview in an institution for elderly individuals. Indeed, the environment and the ability to talk and reflect on cognitive functions, aging, and psychological and physical well-being may influence the content of AD individuals’ answers to questions about self-description. This influence is emphasized in the biopsychosocial approach to awareness: Cognitive functions influence psychological strategies, which are influenced by the social context. 25 This global approach to unawareness in AD supports the need to consider the entire person in the assessment of unawareness.
Our study could provide more information if we had considered other individual characteristics and their influence on unawareness. Because our sample was mainly composed of women (n = 40) and only a few men (n = 6), we could not examine the influence of gender on unawareness, 26 especially with regard to identity changes. Concerning the clinical profiles, we had only the MMSE score and had no information about personality traits or depression or their influence on unawareness. 27 Personality traits may be associated with the person-centered assessment and may strengthen the specificities of each type of assessment.
Finally, we hypothesized that the synergy of the “what” and “how” of the person-centered approach may be associated with the unawareness of deficit score from the assessment with an explicit system of reference. In 2 different models on the effect of the ASDA on MISAWARENESS, we observed that the synergies of domains and items were more relevant than the consideration of only 1 domain or 1 item. When people with AD were unaware according to MISAWARENESS, unawareness was influenced by mechanisms, modes of expression, and objects from the ASDA. These associations between MISAWARENESS, objects, mechanisms, and modes of expression of ASDA highlight the importance of considering more than the objects of unawareness. This observation of mutual associations of the “what” and the “how” of unawareness compliments the results obtained in studies of unawareness focusing on the “what.” Moreover, with regard to the items, we observed for a second time that unawareness results from a synergy of the “what” and “how.” Combining 2 different approaches to unawareness allows us to understand that it is a broad phenomenon composed of objects and processes (i.e., mechanisms and modes of expression). Although these results must be replicated with other assessments of unawareness in AD to verify the hypotheses, in future studies and in practice, we must consider unawareness as a combination of objects and processes of arousal and expression.
To more closely consider individual unawareness, it seems necessary to think of “profiles of unawareness” that include different bases and types of development and expression. In clinical practice, these individual profiles allow for the adaptation of care and the life project with the disease. This new understanding of unawareness needs to be completed with a third type of unawareness assessment that includes the caregiver (e.g., the Anosognosia Questionnaire-Dementia 28,29 or the Patient Competency Rating Scale 30,31 ). The inclusion of a caregiver will provide new information about individual unawareness with regard to the influence of and on relatives. Moreover, a triple perspective (i.e., a prediction–performance paradigm, a person-centered approach and a scoring of discrepancies between ratings of the people with AD and the informant ratings) will follow the French social policy aims for elaboration of the “life project” 32 through the collaborative work of 3 stakeholders (i.e., people with AD, relatives, and formal caregivers).
In conclusion, the combination of 2 perspectives facilitated an understanding of a wider perspective on unawareness in people with AD, its basis, and how it arises and is expressed. This threefold perspective hypothesizes the association of unawareness of disease with larger concepts such as identity. In the future, research and practice should consider people with AD in their entirety.
Footnotes
Authors’ Note
Significance Statements – Unawareness in Alzheimer’s Disease (AD) is the product of a synergy between the objects and processes of arousal and expression. – Unawareness in AD extends beyond the disease and cognitive deficits to include the self and identity changes.
Acknowledgments
LABEX (excellence laboratory, program investment for the future), DISTALZ (Development of Innovative Strategies for a Transdisciplinary Approach to Alzheimer’s disease) and the regional council of Hauts-de-France supported this work.
Author Contributions
All authors substantially contributed to the design of the work (AM, MEH, and PA). All authors drafted (AM) or revised (MEH and PA) the work. All authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.