
Abstract
Introduction:
This study tried to find out type of lobar features found in patients with progressive supranuclear palsy (PSP) and whether they differ from those of frontotemporal dementia (FTD) as both of these are tauopathies.
Methods:
We studied lobar functions of 45 patients with PSP.
Results:
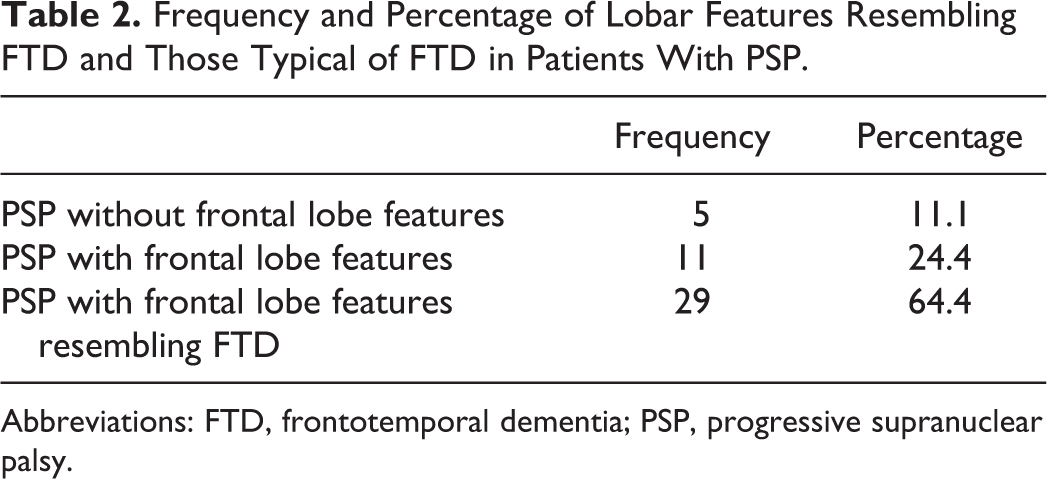
Five (11.1%) patients had no lobar feature; 11 (24.4%) had PSP-like features like apathy, frontal release signs, impaired motor Luria written sequences, and fist-edge-palm test; and 29 (64.4%) patients had FTD-like lobar features like disinhibition, poor naming, and word finding difficulty. Among features resembling FTD, behavioural variant type occurred in 31.1%, primary progressive aphasia type occurred in 58.6%, 3.4% patients had semantic dementia type features, and 6.9% were unclassified.
Conclusions:
Hence, patients with PSP with lobar features may fall in the middle of PSP-FTD spectrum with frontal lobe features typical of PSP (PSP-frontal like) and those with frontal lobe features resembling FTD (PSP-FTD complex) in between.
Keywords
Introduction
Progressive supranuclear palsy (PSP) is a neurodegenerative disorder characterized by supranuclear ophthalmoplegia, postural instability, and a Parkinsonian syndrome. 1 -6 Lobar features like apathy, frontal release signs, impaired motor Luria written sequences, and impaired fist-edge-palm test can occur in patients with PSP. 1,7 -10 Some features involving lobar dysfunction like disinhibition, word finding difficulty, and difficulty in naming objects are characteristic of frontotemporal dementia (FTD). 11 -13 The aim of this study was to find out the exact type of lobar features found in patients with PSP and whether they differ in any way from those typical of frontotemporal dementia, as both of these are tauopathies.
Methods
We studied patients with PSP presenting to the Department of Neurology of the institute from August 2010 to August 2017 and included indoor and outdoor patients of PSP fulfilling the inclusion criteria adapted from possible and probable National Institute of Neurological Disorders and Stroke/Society for progressive supranuclear palsy (NINDS/SPSP) criteria. These were gradually progressive disorder with onset age of more than 40 years with either vertical supranuclear palsy or slowing of vertical saccades and postural instability with falls within a year of disease onset. 1 Supportive features included akinesia or rigidity, abnormal neck posture, early dysphagia and dysarthria, early onset of cognitive impairment including two or more of the following: apathy, impairment in abstract thought, decreased verbal fluency, utilization or imitation behavior, or frontal release signs. Supportive magnetic resonance imaging (MRI) features included midbrain tegmental atrophy leading to “morning glory” and “humming bird” signs.
Exclusion criteria included a recent history of encephalitis, alien limb syndrome, cortical sensory deficits, hallucinations or delusions unrelated to dopaminergic therapy, cortical dementia of Alzheimer type, prominent, early cerebellar symptoms, unexplained dysautonomia, neuroradiological evidence of relevant structural abnormality, and those not giving consent for the study. Since a very high number of patients had lobar atrophy along with all the other features of PSP, hence, we included these patients also in the study.
Research tools included information related to history of present and past illness, physical examination, investigations, and MRI head. We took history of present and past illness, performed physical examination, and did a 3T-MRI and blood tests (blood counts, liver, renal and thyroid function tests, and vitamin B12 and folic acid levels).
We studied the clinical features of patients, especially with regard to the frontal lobe functions. Those having any of the lobar features characteristic of PSP like apathy, frontal release signs, impaired motor Luria written sequences, or impaired fist-edge-palm test were classified as PSP with lobar features and those having any of the features similar to those found in FTD like disinhibition, word finding difficulty, or difficulty in naming objects were classified as PSP with lobar features like FTD and those having no lobar features were classified as PSP without lobar features.
Among PSP with lobar features like FTD, we also analyzed data to see how many patients had features similar to behavioural variant of FTD like disinhibition, how many had features similar to primary progressive aphasia like word finding difficulty and how many had features similar to semantic dementia like difficulty in naming objects.
We used tests of cognition like Addenbrooke’s Cognitive Examination-R, Frontal Assessment Battery, Frontal Behavioural Inventory (FBI), and Frontotemporal Dementia Rating Scale (FRS) in order to assess the frontal lobe features of these patients. 14 -17 We assessed memory using Mini-Mental State Examination as well as interview-based assessment of memory 18 and looked for the visuospatial/visuoconstructional functions using bedside tests. 19 Both the authors assessed the impairment in lobar functioning, including the senior professor. The study includes an informed consent by the study participants or their relatives and an approval by the institutional ethical committee.
Statistics
The authors calculated mean, median, mode, standard deviation for different demographic parameters and found out the frequency and percentage for clinical characteristics. SPSS version 20 analyzed the data.
Results
Of 45 patients of PSP, there were 25 (55.6%) males and 20 (44.4%) females. The mean age of patients was 64.16 ± 8.788 years and maximum number of patients 19 (42.2%) were in the age category of more than or equal to 60 years and less than 70 years. None of the patients had a positive history of similar illness in the family (Figure 1).
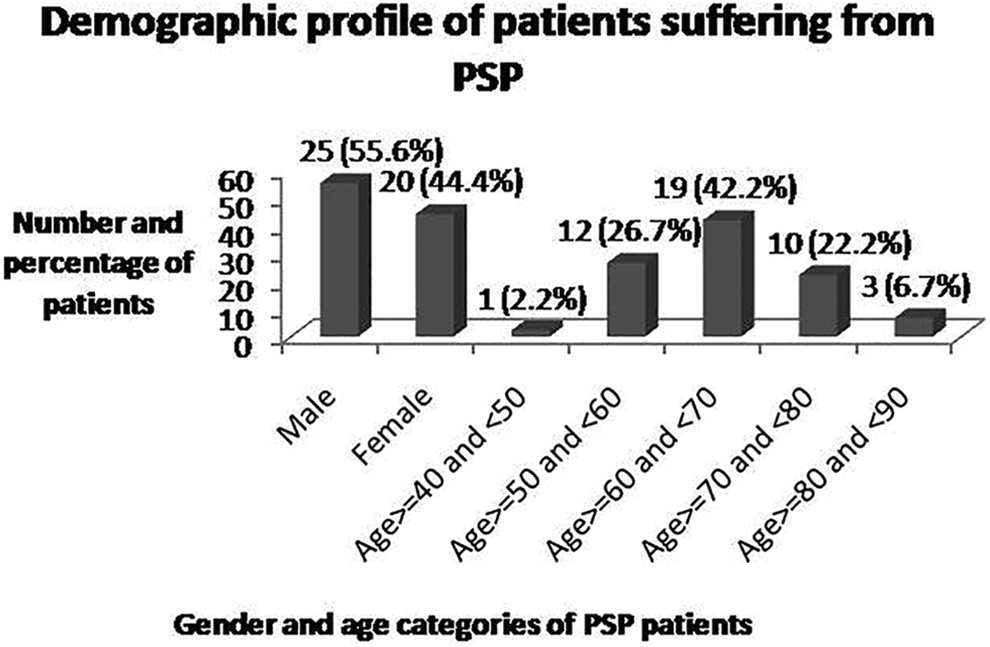
Demographic features of patients suffering from PSP. PSP indicates progressive supranuclear palsy.
Table 1 shows evaluation of different lobar functions, especially frontal lobe features and their results, along with different MRI features in these patients.
Frequency and Percentage of Different Lobar Functions and MRI Features in Patients With PSP.

Abbreviations: MRI, magnetic resonance imaging; PSP, progressive supranuclear palsy.
Table 2 depicts the frequency of patients with PSP who had no lobar features, of those who had lobar features normally seen in PSP like apathy, frontal release signs, impaired motor Luria written sequences, and fist-edge-palm test and of those who had lobar features normally seen in FTD like disinhibition, poor naming, and word finding difficulty.
Frequency and Percentage of Lobar Features Resembling FTD and Those Typical of FTD in Patients With PSP.
Abbreviations: FTD, frontotemporal dementia; PSP, progressive supranuclear palsy.
Table 3 shows the frequency of those who had features resembling the behavioural variant, of those who had features resembling the primary progressive aphasia type and of those who had features resembling the semantic dementia type; among patients who had lobar features normally described in FTD.
Frequency and Percentage of Patients With PSP Resembling Different Variants of FTD.

Abbreviations: FTD, frontotemporal dementia; PSP, progressive supranuclear palsy.
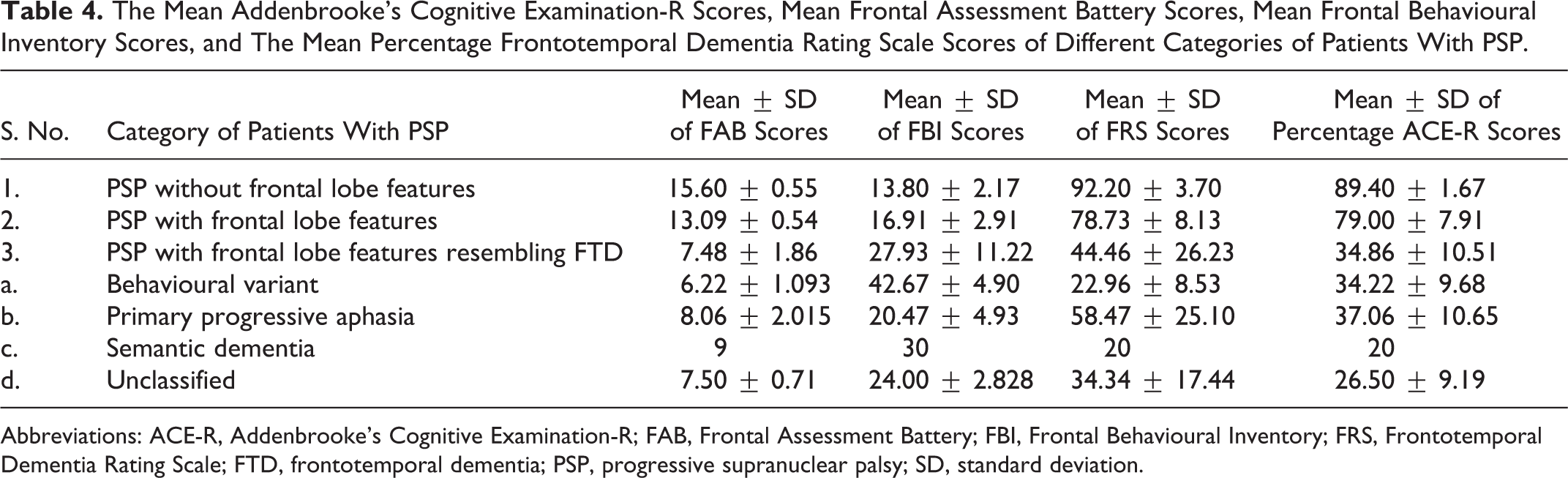
Table 4 has the results of tests of cognition like Addenbrooke’s Cognitive Examination-R (ACE-R), Frontal Assessment Battery (FAB), FBI, and FRS.
The Mean Addenbrooke’s Cognitive Examination-R Scores, Mean Frontal Assessment Battery Scores, Mean Frontal Behavioural Inventory Scores, and The Mean Percentage Frontotemporal Dementia Rating Scale Scores of Different Categories of Patients With PSP.
Abbreviations: ACE-R, Addenbrooke’s Cognitive Examination-R; FAB, Frontal Assessment Battery; FBI, Frontal Behavioural Inventory; FRS, Frontotemporal Dementia Rating Scale; FTD, frontotemporal dementia; PSP, progressive supranuclear palsy; SD, standard deviation.
Table 5 depicts the frequency of various categories of patients with PSP having different MRI features.
Frequency of Various Categories of Patients With PSP Having Different MRI Features.

Abbreviations: FTD, frontotemporal dementia; MRI, magnetic resonance imaging; PSP, progressive supranuclear palsy.
Discussion
The mean age of patients in our study was similar to that found in the previous studies. 2,4,20 Males were more frequent in our study in comparison to females as has been the case in previous studies. 2 Progressive supranuclear palsy is known to have cardinal features primarily meant for differentiating it from Parkinson’s disease. However, deflection from these cardinal clinical features is also known in some cases of PSP. 21 Recently, some additional features have been found to have association with PSP and accordingly PSP is designated with that association. One such association is the presence of some frontal lobe features, designated as PSP-F. Various frontal lobe features found in patients with PSP in this study included behavioural abnormality in the form of irritability and depressed mood, disinhibition, apathy, frontal release signs including palmer grasp reflex, glabellar tap, palmomental test, rooting reflex and snout reflex, impaired fist-palm-hand test, and impaired Luria written sequences test. Previous studies have shown depression and irritability in patients of PSP. 20,22 Patients with PSP may have apathy 8,22 and frontal release signs like grasping. 20
The parietal lobe features studied included impaired constructional ability. The temporal lobe features included impaired recent memory as well as remote memory. Previous studies have shown mild to moderate memory loss in patients with PSP. 20,22 These patients may have episodic memory deficits. 7
The miscellaneous features studied included word finding difficulty, dysarthria, dysphagia, blepharospasm, and dystonia. Progressive supranuclear palsy patients can have dysphagia. 2 Blepharospasm is a known feature of PSP. 3
The diagnostic criteria for PSP include frontal lobe features like apathy and frontal release signs. 1 Progressive supranuclear palsy patients may have executive dysfunction manifested as impaired fist-edge-palm test and motor Luria written sequences test. 10 But in our study, very few patients had frontal lobe features which are normally seen in PSP and many patients had lobar features of the type normally seen in FTD like disinhibition, poor naming, and word finding difficulty. Among these patients, who had lobar features resembling FTD, features resembling primary progressive aphasia were the most frequent ones and those resembling semantic dementia were the most infrequent. The present study revealed primary progressive aphasia kind of presentation to be more frequent than behavioural onset in patients with PSP with frontal lobe features, similar to a previous study. 23
On the application of FAB, we found that the mean scores of patients of PSP without frontal lobe features were much above the cutoff score of 12, those of patients of PSP with frontal lobe features were just above the cutoff score and those of PSP with frontal lobe features resembling FTD were much lower than the cutoff score, proving thereby that patients with PSP with frontal lobe features resembling FTD had the worst frontal lobe functioning. The mean FBI scores of the patients with frontal lobe features resembling FTD were well above 30 indicating severe behavioural involvement. The average FRS scores of the patients with PSP with frontal lobe features resembling FTD signified moderate impairment while the scores of those in the other 2 categories showed only mild impairment with patients with PSP without frontal lobe features being the least affected of all. The average ACE-R scores of patients with PSP without frontal lobe features were much above the category of dementia (cutoff 82) and those of patients with PSP with frontal lobe features resembling FTD were much below the category of dementia. However, the scores of patients with PSP with frontal lobe features were near the borderline. Hence, these patients may be somewhere in between the other 2 categories.
We did not, however, find a significant difference between the MRI features like lobar atrophy in between different groups of patients, though, frontal atrophy was most frequent in patients with PSP with frontal lobe features resembling FTD (Table 5).
Since, several patients of PSP with frontal lobe features also had memory loss and other features of dementia including abnormalities in other lobar functions (apart from frontal lobe functions) and their frontal lobe features were similar to those seen in FTD, hence we hypothesized that patients with PSP with lobar features may fall in middle of PSP-FTD spectrum with PSP without lobar features at one end and FTD at the other, with frontal lobe features resembling PSP, which may be termed as PSP-frontal like and frontal lobe features resembling FTD, which may be called PSP-FTD complex in between (Figure 2).

Proposed PSP-FTD spectrum types. FTD indicates frontotemporal dementia; PSP, progressive supranuclear palsy.
The latest diagnostic criteria for the diagnosis of PSP have included loss of grammar and/or telegraphic speech or writing as well as the presence of disinhibition as types of PSP and some recent studies show these features in patients with PSP. 24 -29 We, however, propose that since the group of patients who are having lobar features resembling FTD may fall in either PSP or in FTD, both of which are tauopathies, we may group them as a separate entity with a name PSP-FTD complex being adopted, and those who are having frontal lobe features much like those seen in PSP may be termed as PSP-frontal like. This would help in differentiating the subgroup of patients who are not so much impaired (PSP-frontal like) in comparison to severely impaired people (PSP-FTD type) and may be helpful in delineating different treatment approaches toward different categories of patients. It is a matter of further research to see whether one subtype evolves into the other with time and whether different categories of genetic mutations are responsible for differences in different subtypes. 30
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.