
Abstract
Understanding Alzheimer’s disease (AD) dynamics is essential in diagnosis and measuring progression for clinical decision-making; however, clinical instruments are imperfect at classifying true disease stages. This research evaluates sensitivity and determinants of AD stage changes longitudinally using current classifications of “mild,” “moderate,” and “severe” AD, using Mini-Mental State Examination (MMSE), Alzheimer’s Disease Assessment Scale–Cognitive subscale (ADAS-Cog), and the Clinical Dementia Rating–Sum of Boxes (CDR-SB) thresholds. Age and pre-progression rate were significant determinants of AD progression using MMSE alone to stage AD, and pre-progression was found to impact disease progression with CDR-SB. Sensitivity of these instruments for identifying clinical stages of AD to correctly staging a “moderate” level of disease severity for outcomes MMSE, CDR-SB, and ADAS-Cog was 92%, 78%, and 92%, respectively. This research derives longitudinal sensitivity of clinical instruments used to stage AD useful for clinical decision-making. The MMSE and ADAS-Cog provided adequate sensitivity to classify AD stages.
Introduction
Alzheimer’s disease (AD), a major public health problem, affects over 5 million elder individuals and is among the leading causes of US mortality. 1 Due to the nature and duration of the disease, it is costly to patients, caregivers, and the health-care system. Caregivers often encounter higher levels of emotional stress, and their health, employment, and financial security are negatively impacted. While the elderly patients continue to live longer, without curative treatment, prevalence is expected to double by 2050. Clinically, understanding the timing of AD progression and prediction of AD stage duration, especially the mild stage, would help tailor treatment plans that parallel the progression, thus improving disease management. 2 -4
Although methods for predicting progression rates have been studied, 2,5 disease onset and progression is difficult to quantify through studying AD natural history alone, as AD is a complex disease with complex pathogenesis comprised of social, environmental, and genetic factors. One challenge is monitoring change using clinical outcomes. Identifying and validating neuropsychological measures to predict changes in AD severity is important in linking the underlying disease process to observed clinical symptoms, monitoring response to potential therapies, and assessing potential predictability of biomarkers, all requiring sophisticated longitudinal statistical models, in which few studies have utilized. Discrete-time Markov chains have been used to understand the natural history of AD 6 along with other longitudinal techniques, 7 but research thus far does not account exhaustively for unequal duration between visits or lapses between actual stage changes. Baseline risk factors associated with long-term outcomes have been studied, 8 but just how risk factors impact the actual dynamics of the process have not been elucidated.
Clinically, AD is often staged as “mild,” “moderate,”or “severe” using thresholds of well-validated and reliable neuropsychological scales such as the Mini-Mental State Examination (MMSE), 9 Alzheimer’s Disease Assessment Scale-cognitive Subscale (ADAS-Cog), 10 and/or Clinical Dementia Rating–Sum of Boxes (CDR-SB), 11 among others. Imaging biomarkers indicating existing levels of severe cognitive impairments alongside a positive amyloid positron emission tomography scan 12,13 and/or other biomarkers such as cerebrospinal fluid amyloid Beta and tau, 14 -16 each potentially costly and burdensome, are used for AD diagnosis, giving confidence that the diagnosis of dementia is caused by Alzheimer’s pathology. Alzheimer’s disease staging, however, is a separate process, of which there is no easily obtainable neuropsychological-based “gold standard” instruments; thus, examining cut-point sensitivities is challenging. Nevertheless, though subject to misclassification, these instruments remain the primary assessments used to classify AD severity. Studies have examined MMSE sensitivity and specificity of predicting AD onset or progression 17 -20 using receiver operating characteristic curves and growth mixture models, among others. Although these studies assess misclassification post-analysis, they lack statistical model development to allow for misclassification of severity.
Operative use of the CDR-SB to stage Alzheimer’s dementia has been established and cross-validated to classify dementia severity into 6 groupings, ranging from “normal” (CDR-SB: 0) to “severe dementia” (CDR-SB: 16.0-18.0). 21 -23 This cross-validation was not used in determining change in disease over time. The ADAS-Cog, an end point used in AD clinical trials, has been widely used to assess progression by examining change from baseline to measure improvement 24 but has not been used to stage AD severity. 25 Benge and others, 26 through item response theory analysis methods, found that scores 14 and 64 of the raw score provided information on lower and higher levels of cognitive dysfunction.
Few studies have examined sensitivity of MMSE and others for staging AD without a “gold standard.” Luo et al 27 studied the sensitivity of baseline MMSE, ADAS-Cog, CDR-SB, and CDR using binomial regression framework. To the best of our knowledge, sensitivity of tertiary disease stages based on cognitive or functional instruments has not been studied in a longitudinal setting.
For research pertaining to monitoring AD and patient responses in clinical studies, cognitive measures will continue to provide useful assessments of AD progression. 28 Clear staging criteria using accepted instruments will improve comparability. Sensitivity of AD severity changes should be considered due to the continuous nature of the AD process. The purpose of this study is to apply a recently developed continuous-time Markov chain (CTMC) model estimation technique to estimate the probability of misclassification of AD severity and the determinants (eg, sex, age, years of education, pre-progression rate [PPR]) of AD stage changes over time using current instruments (MMSE, ADAS-Cog, and CDR-SB). Namely, this research aims to analyze the progression of AD stage changes using 3 different instruments and measure the sensitivity of each in the absence of a “gold standard.”
Methods
This research has been conducted according to the World Medical Association Declaration of Helsinki. Approval of this study has been provided by Baylor College of Medicine–Alzheimer’s Disease and Memory Disorders Center (IRB# H-9095).
Study Population
A prospective cohort of patients with probable AD 29 from the Baylor Alzheimer’s Disease and Memory Disorders Center collected from January 1990 to September 2011 were examined. Patients were self-referred or referred to the center and evaluated using history and physical examinations, laboratory testing, neuropsychological instruments, and imaging 30 after providing written informed consent, which also included consent by the patient(s) or a legally authorized representative for patient information and images to be published. Patient sociodemographic information such as age, sex and years of education, medical history, and estimates of symptom duration 31 was collected at baseline. Further details of the study design and outcome diagnosis have been described elsewhere. 30
Disease Severity
Patients underwent neuropsychological testing at baseline and annually or on an as-needed basis for medication management. The MMSE (scored 0-30) focuses on memory, attention, and language and aids in identifying dementia progression and severity; lower scores indicate more severe dementia. The ADAS-Cog (scored 0-70) targets cognitive impairment in patients with AD; higher scores indicate worse cognitive impairment. The CDR-SB (scored 0-18) measures global performance; higher scores indicate higher levels of global impairment. These 3 measures of cognitive outcome and global impairment can be used to classify AD severity into mild, moderate, and severe stages. Standard cutoff points of MMSE were used to classify AD severity into mild (MMSE ≥ 20), moderate (10 ≤ MMSE ≤ 19), and severe (MMSE ≤ 9). 32 We applied staging presented by O’Bryant et al 21 to CDR-SB (mild: 0-9.0, moderate: 9.5-15.5, severe: 16.0-18.0) and by Benge et al 26 to ADAS-Cog (mild: 0-14, moderate: 15-63, severe: 64-70).
Pre-Progression Rate
Pre-progression rate, a baseline enrollment measure indicating decline from symptom onset to first clinic visit, is defined as the average decline of MMSE per year before the first physician visit and is calculated as (30 − baseline MMSE)/estimated symptom duration in years. 31 It has been proven to be predictive of cognitive performance over time2 and used to classify patients as slow, intermediate, and rapid progressors.
Inclusion Criteria
Patients with probable AD with complete information on baseline covariates, a baseline pre-progression index, and at least 1 follow-up visit post-baseline (ie, at least one possible transition) were included in this study. Interobservation time was calculated as the duration between 2 consecutive observations.
Data Analysis
Baseline characteristics were compared using χ2 tests for categorical variables and analysis of variance for continuous variables across severity levels for each outcome. For longitudinal modeling, true disease severity (mild, moderate, severe) of each individual is modeled as a 3-state CTMC with a transition rate matrix of unknown parameters

This method also assumes that the covariates impact the dynamics of the transition, not on any specific hazard. The duration in i follows an exponential distribution with mean

For estimating misclassification probabilities, although an individual’s true severity or observed severity may transition from mild to severe over a period of time, we assumed that an individual who is truly in a mild severity state would not be misclassified as severe and that severe would not be misclassified at mild. As the statistical model was based on commonly used and studied staging assessments used to classify disease severity, it is unlikely that these scores would have such large errors. An explicit representation of the misclassification matrix can be found in the study by Benoit et al. 33 Misclassification is assumed independent of the disease process and due to the staging; however, in this model, there is an indirect adjustment of misclassification posed in the presence of explanatory variables. All statistical analyses and customized estimation procedures were written and conducted using SAS version 9.3 (SAS Institute Inc, Cary, North Carolina).
Results
Among 1106 patients with probable AD evaluated from January 1990 to September 2011, 1091 had complete baseline characteristics. Baseline characteristics included age, gender, years of education, cumulative months of exposure to antidementia drugs, follow-up time, total number of visits, and PPR (Table 1) as well as the MMSE, CDR-SB, and ADAS-Cog baseline scores and disease severity along with a complete case description (Tables 2 and 3). At baseline, patients were on average 73 years old (43-93), had 14 years of education (0-29), and predominantly female (67%). The number of visits ranged from 2 to 12 with a median of 3. After exclusion and inclusion criteria were applied, longitudinal analysis included the following sample sizes for each outcome: ADAS-Cog (n = 847), MMSE (n = 972), and CDR-SB (n = 982).
Baseline Characteristics of the ADMDC Probable AD Cohort, Houston, Texas, 1990 to 2011 (N = 1091).

Abbreviations: AD, Alzheimer’s disease; ADMDC, Alzheimer’s Disease and Memory Disorders Center; SD, standard deviation.
a Pre-progression rate at enrollment = (30 − baseline Mini-Mental State Examination)/estimated duration of symptoms in years.
Baseline Cognitive and Functional Measures and Their Severity Distributions Among the ADMDC Probable AD Cohort, Houston, Texas, 1990 to 2011 (N = 1091).

Abbreviations: AD, Alzheimer’s disease; ADAS-Cog, Alzheimer’s Disease Assessment Scale–Cognitive; ADMDC, Alzheimer’s Disease and Memory Disorders Center; CDR-SB, Clinical Dementia Rating Scale–Sum of Boxes; MMSE: Mini-Mental State Examination; SD, standard deviation.
Complete Case Distribution of Baseline Cognitive and Functional Measures and Their Severity Among the ADMDC Probable AD Cohort, Houston, Texas, 1990 to 2011 (N = 871).

Abbreviations: AD, Alzheimer’s disease; ADAS-Cog, Alzheimer’s Disease Assessment Scale–Cognitive; ADMDC, Alzheimer’s Disease and Memory Disorders Center; CDR-SB, Clinical Dementia Rating Scale–Sum of Boxes; MMSE: Mini-Mental State Examination; SD, standard deviation.
Baseline MMSE, CDR-SB, and ADAS-Cog mean (standard deviation) score was 19.8 (6.6), 6.5 (4.1), and 23.6 (12.5), respectively (Table 2). Increased baseline PPR was associated with baseline severity for all outcome measures as was education level (Table 4). Baseline AD severity varied by gender for all outcome measures. Age was associated with baseline severity for CDR-SB (P = .0256).
Distribution of Baseline Covariates Among AD Stages of Severity Defined Using Cognitive and Functional Instruments Among the ADMDC Probable AD Cohort, Houston, Texas, 1990 to 2011 (N = 1091).

Abbreviations: AD, Alzheimer’s disease; ADAS-Cog, Alzheimer’s Disease Assessment Scale–Cognitive; ADMDC, Alzheimer’s Disease and Memory Disorders Center; CDR-SB, Clinical Dementia Rating Scale–Sum of Boxes; MMSE: Mini-Mental State Examination; SD, standard deviation.
Sensitivity of Cognitive and Functional Measures in Staging AD
Overall, sensitivity to correctly staging a moderate level of disease severity for outcomes MMSE, CDR-SB, and ADAS-Cog was 92%, 78%, and 92%, respectively (Table 5). Moderately staged patients when classified by ADAS-Cog and/or MMSE were ≥2 times more likely to be incorrectly staged as mild rather than severe. Incorrectly classifying moderate stage to mild or severe was estimated as about equally likely (11%) using the CDR-SB.
Misclassification Probabilities as “Mild” or “Severe” for Disease Severity Staged by Cognitive and Functional Measures Among the ADMDC Probable AD Cohort, Houston, Texas, 1990 to 2011.
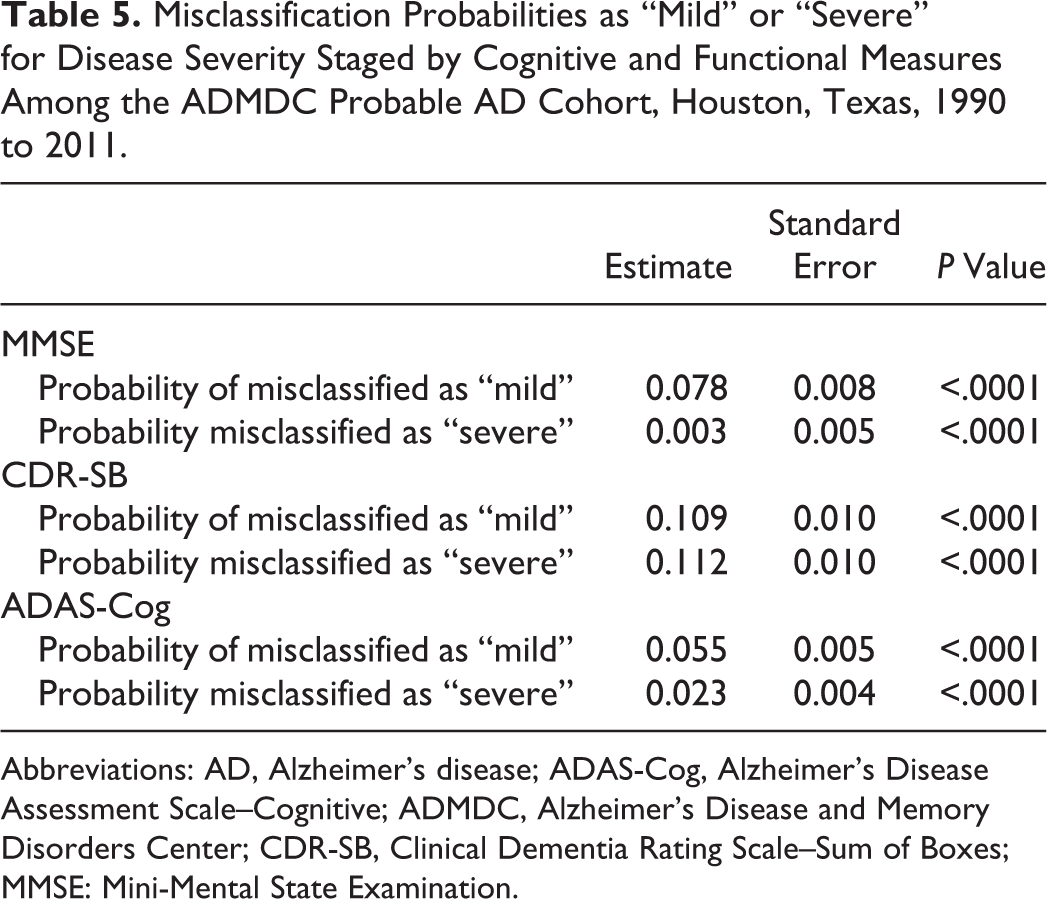
Abbreviations: AD, Alzheimer’s disease; ADAS-Cog, Alzheimer’s Disease Assessment Scale–Cognitive; ADMDC, Alzheimer’s Disease and Memory Disorders Center; CDR-SB, Clinical Dementia Rating Scale–Sum of Boxes; MMSE: Mini-Mental State Examination.
Disease Progression
Mini-Mental State Examination
From the results in Table 6, the intensity of transitioning from mild to moderate severity is
Transition Intensities and Determinants of AD Stage Changes Using Functional and Cognitive Instruments Among the ADMDC Probable AD Cohort, Houston, Texas, 1990 to 2011.

Abbreviations: AD, Alzheimer’s disease; ADAS-Cog, Alzheimer’s Disease Assessment Scale–Cognitive; ADMDC, Alzheimer’s Disease and Memory Disorders Center; CDR-SB, Clinical Dementia Rating Scale–Sum of Boxes; CI, confidence interval; MMSE: Mini-Mental State Examination.
a Note that
Clinical Dementia Rating–Sum of Boxes
Using the same interpretation as above, when modeling disease stage changes based on CDR-SB, the intensity of transitioning from mild to moderate severity is
Alzheimer’s Disease Assessment Scale–Cognitive subscale
The base transition intensity of moving from the mild to moderate stage of severity is 0.24 (95% CI: 0.03-1.80) based on the ADAS-Cog model, and the intensity associated with movement from moderate to severe is 0.01 (95% CI: 0.00-0.07). At the time of disease stage change, a patient with moderate moves to severe with a probability of .83. On average, patients with an enrollment PPR of 1 point per year higher have their mean time to stage change decreased by a multiplicative factor of 1/1.08.
Patient PPR at enrollment had a statistically significant multiplicative impact on the rate of movement of AD stage changes classified using MMSE and CDR-SB, and age had a slight multiplicative reduction in progression when disease status was classified using MMSE.
Discussion
The purpose of this article was 2-fold: to examine the validity of neuropsychological assessments (MMSE, CDR-SB, and ADAS-Cog) used to stage AD disease severity and to characterize the dynamic characteristics of AD progression over time to aid in clinical staging of AD.
Our results indicate that MMSE best classifies moderate stage of severity, with 7% misclassified as mild. This could suggest that misclassification rates may rely on the neuropsychological measures. The MMSE has been criticized by some as being insensitive in distinguishing mild cognitive impairment (sensitivity/specificity reported <80% depending on criteria). 21 However, diagnostic screening studies typically use cross-sectional data to compute sensitivity and specificity and also report crude estimates. 27 At most, an adjusted categorical model might be used. This study takes advantage of clinical longitudinal measurements of observed AD staging and baseline characteristics, examining the interplay of severity over time, determinants of these dynamic changes, and diagnostic accuracy of disease staging through the CTMC model.
The CDR-SB was estimated to misclassify ∼20% of those that could be staged as moderate, which is higher than what might be expected for clinical utility, given the frequency in which the CDR-SB is used and reported reliability. 34 As this tool is used in both staging and diagnosis, this finding supports the literature that CDR-SB may be better served at distinguishing normal from dementia as a diagnostic tool as opposed to later staging of AD. For comprehensiveness, as we did think this number was higher than expected, we investigated the crude proportion of individuals who would have bordered the moderately severe threshold to explore the potential sensitivity prior to estimation. Using a 2-point error, 21% of observations fell within up to 2 units milder and none up to 2 units more severe. Considering 21% being possibly misclassified from moderate to mild or severe, the estimated 22% misclassification is reasonable.
With this rich cohort, we assessed thresholds of 3 neuropsychological instruments of cognitive and functional measures collected in the clinic. Although the MMSE has customarily been used to stage AD clinically, thresholds for classifications vary. Guidelines on CDR-SB and ADAS-Cog for classifying cognitive and AD disease severity, while believed to be sensitive to change, have not been supported by the literature. Not only does this research provide a comparison of sensitivity of staging disease but aims to corroborate diagnostic thresholds used to help clinicians identify, monitor, and treat patients at different levels of severity as well as to aid in patient selection in clinical trial enrollment for treatment development using routinely collected measures beyond the MMSE.
Age significantly impacted disease progression when MMSE was used to classify disease stages but not when severity was defined using CDR-SB. Furthermore, increased enrollment PPR was found to increase the rate of transition of disease when using MMSE and CDR-SB to stage AD severity but not when using ADAS-Cog. Our results also showed that years of education was associated with severity of AD at baseline in an unadjusted analysis; however, education level was not found to be a determinant of the disease process when analyzing the data longitudinally and with other covariates such as PPR. Similar findings have been reported and discussed previously when assessing education attainment related to AD progression 35 and cognitive decline 36 and support a passive cognitive reserve hypothesis described in the literature 37 that while education attainment delays onset of cognitive decline (due to higher cognitive performance), education does not slow the progression of AD as it relates to cognitive decline. Understanding how education indicates cognitive reserve will help clinicians to tailor treatment for the elderly patients and help researchers fine-tune progression models for clinical trial design and AD research.
The clinical utility of the progression results of this study is the estimation of a particular patient’s mean duration in stages of severity. In other words, given a particular patient, we can determine the expected duration of stay in the mild stage prior to transitioning into the moderate stage given an individuals’ PPR, age at onset (or first clinical visit), and so on. For example, for a 73-year-old female with an enrollment PPR of 3.5 MMSE points of worsening per year and 16 years of education, the average length of stay in mild stage of severity is estimated to be 3.1 years based on the MMSE. That same patient, if diagnosed using the CDR-SB or ADAS-Cog, would be expected to transition to the moderate stage after 3.1 and 2.9 years, respectively. Since the indications for antidementia drugs vary by disease stage, and since the need for nonpharmacologic and respite care varies by stage, these estimates are important for treatment and other care planning.
For purposes of application of our model, while the model allows estimability from mild to severe and severe to moderate states of disease, there were either 0 or not enough transitions of this nature in the data set; thus, the transition rate is near 0.
One might argue that the utilization of all 3 scores simultaneously would be optimal to study our research question and to make better clinical decisions. First, collection of clinical data varies in practice across clinicians as well as research projects. Second, this research allows us to understand how each staging criteria could be utilized prior to use in a multidimensional manner. Still, either extension of this method to model all 3 scores simultaneously or utilization of multiple measurements into a composite score could provide more information upon which to assess sensitivity of staging and finding determinants of the process itself. As the methods used in this article were recently developed and not part of standard statistical practices, future research is needed to incorporate these data in a multidimensional space.
This study has several limitations. First, it is a cohort of patients with probable AD and therefore difficult to compare cognitive functions to those who did not have the disease. Second, until 1995, the ADAS-Cog was not routinely conducted; thus, not all patients in the cohort were administered the ADAS-Cog. Further, analyses were limited to the measures collected in this cohort, which included the best known and most often used cognitive impairment screening tool. We acknowledge that other well-validated, reliable measures are used to screen and identify possible mild cognitive impairment and probable dementia (eg, the Montreal Cognitive Assessment, 38 Telephone Interview for Cognitive Status, 39 among others) 40 A future study using our analytical methods in a large cohort with other outcome measures may be useful. Our results are based on the model adopted. There is no other model of a similar nature to use to study the goodness-of-fit when the data are potentially misclassified or incomplete.
From the methodological perspective, we have laid the groundwork for a unique approach at analyzing AD progression/regression useful in clinical decision-making. Methodologically, this is the first research of which we are aware that incorporates longitudinal data to estimate diagnostic accuracy (ie, sensitivity) of cognitive disease severity using an exact analytical form approach. By modeling the natural history of AD, the relationship between true stage changes and baseline covariates was evaluated. We examined transition intensities of AD stage change assuming unobservable underlying disease stages and estimated sensitivities of classifications of moderately diseased patients using established neuropsychological instruments as observed outcomes, which could lead to an improved determination of disease severity cutoff points.
Results of this study have important clinical and research-related ADAS-Cog implications in the AD population. Identifying stages of AD severity will allow researchers to measure disease progression and obtain more information regarding the sensitivity and specificity of neuropsychological measures. The models may be useful in evaluating pharmaceutical and behavioral intervention studies that aim to prevent onset or slow progression of AD. The ability to model the severity of AD is necessary in designing treatment plans which better manage the disease, therefore delaying the progression of disease and enhancing quality of life. Based on the estimates of misclassification, MMSE and ADAS-Cog are appropriate instruments to classify the moderate stage of disease.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.