
Abstract
Objectives:
To examine the mediating effects of depression and anxiety in the relationship between self-efficacy and quality of life among people with mild cognitive impairment (MCI) or mild dementia.
Method:
A total of 196 patients diagnosed with MCI or dementia due to Alzheimer disease completed structured measures of self-efficacy, quality of life, and depressive and anxiety symptoms. We examined direct and mediated effects by fitting structural equation models to data.
Results:
Our analyses supported that the effects of self-efficacy on quality of life may be partially mediated by depression and anxiety. Both anxiety and depression had significant mediating effects, with depression showing a stronger effect.
Conclusion:
These results suggest that increased self-efficacy may have a positive effect on quality of life in people with MCI or dementia—partly by reducing depression and anxiety. These findings may have important practical implications for tailoring therapeutic interventions.
Introduction
Older people have an increased risk of mild cognitive impairment (MCI) that may lead to dementia. The key criteria that distinguish MCI from dementia are preserved independence in functional abilities and lack of impairment in social or occupational functioning—although people with MCI may be less efficient and make more errors in activities of daily living than before. 1 Notably, MCI does not always lead to dementia, although it is associated with increased risk. 2 Research also suggests that compared to people with normal cognitive function, those with MCI and dementia carry an increased risk of developing depression. In one study, at the 4-year follow-up, depression was reported by 38% of people with MCI and 43% with dementia, compared to 20% of people with normal cognition. 3 Anxiety is also more common among individuals with MCI or dementia, with estimated anxiety symptom prevalence rates of 8% to 71% in this population. 4 -6 Both anxiety and depression have substantial impacts on outcome, as they decrease the ability to live independently and lead to a reduced quality of life. 7 -9 To date, there is no medical cure that slows or stops the progression of MCI or dementia. 10 Thus, there is increased interest in psychotherapeutic interventions that target depressive and anxiety symptoms and assist in coping with cognitive impairment.
Meta-analyses of psychotherapy studies targeting depression and anxiety have demonstrated statistically significant improvements in people with MCI and dementia. 8,11 Likewise, randomized controlled psychosocial studies have reported statistically significant reductions in depressive symptoms 12 -14 and anxiety symptoms 15 among people with dementia, as well as positive effects on mood and memory performance in those with MCI. 16 However, most studies to date have focused on the disabilities and cognitive impairments in individuals with MCI and dementia. Little is known about how people with dementia cope with the disease, which is an important aspect because inability to adjust to the illness may lead to negative outcomes, such as resistance to engaging in new treatments, noncompliance, and activity withdrawal. 17
Self-efficacy, defined as people’s beliefs regarding their capacity to exert control over situations affecting their lives, 18 might be a useful concept when studying those who must adjust their lives due to illness. 19 Individuals with stronger self-efficacy are reportedly more likely to engage in effective problem-solving, to maintain their adjustments, and to focus on opportunities. 18 For example, for individuals with chronic pain and cancer, increased self-efficacy is related to a greater capacity to effectively manage these conditions. 20,21 Hence, self-efficacy may be important for handling severe symptoms and chronic conditions. Notably, self-efficacy is not a fixed trait and can be modified through psychosocial interventions. 18
Self-efficacy is suggested to be related to quality of life. 22 Investigations of patients with chronic and severe disorders, such as spinal cord injury, show that patients with significantly lower self-efficacy also report lower quality of life, compared to those with high self-efficacy. 23 Studies of people with bipolar disorder also indicate that higher self-efficacy levels are associated with higher health-related quality of life. 24 Few studies have examined this relationship in people with dementia. However, in a systematic review with a narrative synthesis of family caregivers of people with dementia, self-efficacy was significantly associated with health-related quality of life—showing a mean effect size of 0.21, indicating small-to-medium effects. 25
Research has also demonstrated that self-efficacy is related to depressive symptoms. However, to our knowledge, few studies have examined the relationship between self-efficacy and depression in people with dementia. One study of older participants without dementia revealed that low self-efficacy beliefs were related to overemphasizing task difficulty and effort investment when facing a difficult task. 26 In turn, this led to low initiative and low interest, which are constructs closely linked to depression. In a large study of adults in the United States, greater self-efficacy at baseline significantly predicted less serious depressive symptoms, while severe depressive symptoms at baseline predicted poorer self-efficacy at follow-up. 27 A negative relationship between self-efficacy and depression is also found in the field of caregiving for family members with dementia, in that caregivers with higher self-efficacy are less likely to report depressive symptoms. 28 -30 Anxiety is also suggested to be related to self-efficacy. For example, in a sample of people with cancer, maintaining a sense of self-efficacy reportedly decreased depression and anxiety and thus improved individuals’ perception of a situation. 31 Moreover, in a sample of healthy adolescents, low levels of self-efficacy were related to high levels of trait anxiety/neuroticism, as well as anxiety and depressive symptoms. 32
It also appears that emotional states, such as depression and anxiety, are related to quality of life and self-efficacy. Analysis of a sample of people with dementia indicated that the relationship between loss of autonomy and quality of life was mediated by mood, supporting that depression is an important determinant of quality of life in dementia. 33 Accordingly, other research findings indicate that depression is an important aspect of quality of life, because it’s related to psychological well-being, negative self-perception, and unmet needs. 34 Studies of chronic and severe illnesses also suggest a relationship between depressive and anxiety symptoms, quality of life, and self-efficacy. For example, Robinson-Smith et al 35 propose that self-efficacy increases quality of life and decreases depressive symptoms in older patients with stroke. Another study reported that self-efficacy and depression were significant predictors of quality of life in a sample of patients receiving hemodialysis. 36 Among patients with cancer, depression, anxiety, and self-efficacy have also been found to play major roles in determining perceived quality of life. 37
Both theory and a growing body of evidence support that high self-efficacy is associated with low negative affect (eg, depression and anxiety), high positive affect, and increased quality of life, while low self-efficacy is associated with depression and anxiety, as well as decreased quality of life. 22,23,32 To our knowledge, no studies have directly examined the possibility that depression and anxiety play a mediating role in the relationship between self-efficacy and quality of life among people with MCI or dementia due to Alzheimer disease. In the current study, we aimed to address this gap in the literature.
Methods
Design and Setting
In the present study, we analyzed baseline data of people with MCI and dementia due to Alzheimer disease, who were enrolled in the Norwegian CORDIAL study (ClinicalTrials.gov Identifier: NCT02013518): a randomized, controlled study exploring whether cognitive–behavioral therapy (CBT) is beneficial for depressive symptoms in this population. 38 The participants were recruited from 5 memory and old-age psychiatry clinics in Norway between January 2013 and June 2017.
Participants and Procedure
Participants fulfilled the following eligibility criteria: met the Winblad criteria for MCI 39 due to Alzheimer disease, or met the criteria for dementia in Alzheimer disease according to International Statistical Classification of Diseases, Tenth Edition, or the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) 40 ; living at home; had weekly contact with a caregiver (spouse, friend, sibling, or adult child); and gave informed consent to participate. Exclusion criteria were severe psychiatric or somatic illness that could hinder study adherence, ongoing psychotherapy, and living outside home (eg, in a nursing home). Participants who already received ongoing medication at stable doses were not excluded, due to ethical and practical considerations.
All participants underwent a comprehensive assessment that included advanced cognitive testing following a standard protocol, 41 and magnetic resonance imaging (MRI) scans of the brain with either visual inspection 42 or volumetric hippocampus measurement using Neuroquant software. 43 The MR findings were integrated into the final MCI or dementia diagnosis. Spinal fluid was tested for τ protein and amyloid-β, when appropriate. Diagnoses were discussed in consensus meetings with experienced geriatricians, psychiatrists, a neurologist, and a neuropsychologist. Individuals who completed this comprehensive assessment and met the inclusion criteria were asked to participate via a mailed letter, followed by a phone call. Those who agreed to participate underwent baseline examination, completed by trained health staff.
Measures
Background Variables
We recorded patient age, gender, kinship, work situation, years of schooling, duration of symptoms, and formal help measured with the Resource Utilization in Dementia Questionnaire. 44 The ability to perform activities of daily living was proxy-rated by a close caregiver, using the Instrumental Activities of Daily Living Scale (I-ADL) 45 administered by trained health staff. The I-ADL measures independent everyday activities (eg, cooking, cleaning, and managing finances), with items scored from 1 (independent) to 5 (totally dependent), generating a maximum total score of 31. Cronbach α for the I-ADL reportedly ranges from .78 to .91. 46
Cognitive functioning was assessed using the Norwegian version of the Mini-Mental State Examination (MMSE-NR), 47 administered by trained health staff. The scale comprises 20 items, scored from 0 to 30, with a higher score indicating better cognitive function. The MMSE-NR is commonly used as a screening tool for dementia and covers multiple cognitive domains, such as orientation to time and place, naming of objects, attention, and language. Folstein et al 48 examined the reliability and validity of the MMSE and reported a Cronbach α of .89.
General Self-Efficacy
General perceived efficacy was assessed using the General Self-Efficacy (GSE) 49 Scale as a self-report measure. The GSE is a 10-item self-rated scale including questions that refer to different ways of successfully coping with general matters (eg, “When confronted with a problem, I can usually find several solutions”). Responses were measured on a 4-point scale: not at all true, hardly true, moderately true, and exactly true. Total score ranges from 10 to 42, with higher values indicating higher self-efficacy. In a sample of 23 nations, the estimated Cronbach α values ranged from .76 to .90. 50
Quality of Life
Quality of life was measured using the Norwegian version of the Quality of Life in Alzheimer’s Disease (QOL-AD) scale, 51 administered as a structured interview by a trained health staff member. The QOL-AD is a 13-item questionnaire covering quality of life in different domains, such as living condition, physical health, relationship, and financial condition. Each item was rated on a 4-point scale, yielding a total score ranging from 13 to 52. Systematic examination in samples with dementia has revealed that the QOL-AD showed satisfactory validity and estimated reliability of 0.82. 52
Depression and Anxiety
Anxiety and depression were measured using the Hospital Anxiety and Depression Scale (HADS), 53 completed as a self-reported measure. The HADS anxiety (HADS-A) and depression (HADS-D) subscales each comprise 7 related items, which were rated on a 4-point scale ranging from 0 to 3, yielding a maximum score of 42. A cutoff score of >8 indicates significant anxiety and depressive symptoms. 54 A meta-study by Bjelland et al 54 reported Cronbach α values ranging from .68 to .93 (mean: .83) for HADS-A and from .67 to .90 (mean: .82) for HADS-D.
Depression was also measured using the Montgomery-Åsberg Depression Rating Scale (MADRS), 55 administered by trained health staff in the form of a semistructured interview providing structured probes to ensure item standardization. The MADRS comprises 10 items, covering the 10 most common depressive symptoms reported by patients, including sadness, inner tension, reduced sleep, and suicidal thoughts. Responses were scored on scales ranging from 0 to 6. The MADRS has shown high inter-rater reliability, validity, and sensitivity to change. 55 Fantino and Moore 56 reported a Cronbach α of .84 for MADRS.
Statistical Analyses
Our main analysis focused on the effect of perceived self-efficacy on quality of life, mediated by depression. Mediated effects have traditionally been estimated using ordinary linear regression models and interpreted according to Baron and Kenny, 57 who suggested that 4 criteria should be fulfilled to demonstrate a mediated effect: (1) The causal variable should have a substantial direct effect on outcome; (2) the causal variable should affect the mediating variable; (3) the mediating variable should affect outcome when controlling for the causal variable; and (4) the effect of the causal variable should disappear (complete mediation) or be substantially reduced (partial mediation) when controlling for the mediating variable. Additionally (or alternatively), the causal variable’s indirect effect through the mediating variable can be estimated and tested for statistical significance. Since the sampling distribution shape is unknown in small samples, a bootstrap procedure is usually employed (eg, see Preacher and Hayes 58 ). However, the above-described procedures do not address measurement error in mediator and outcome variables, which is a serious problem in mediation analysis. 59 This issue can be managed by estimating a full structural equation model including all items and latent variables, but this necessarily implies estimation of a large number of model parameters.
Due to our limited sample size, we chose an alternative solution—estimating a single-item latent variable model, and fixing the error variance of the single-item to (1 − reliability) × variance of the item (as examined by, eg, Savalei 60 ). It can be argued that optimal estimates of reliability could preferably be found in large-scale studies or meta-studies. However, since we used Norwegian versions of all measures and all our reliability estimates were in the expected range, we chose to use the Cronbach α values reported in Table 1 as reliability estimates. As a “single item,” we used the observed additive scales of the relevant measures. Fitting structural equation models to data may imply more demanding assumptions than ordinary linear regression—for example, concerning multivariate normality. We examined the distribution of residuals from linear regression models with quality of life dependent on GSE and HADS/MADRS and detected no serious deviations from normality or homogeneity of variance. However, due to the relatively small sample size (n = 196), all conclusions regarding sampling variability were based on nonparametric standard errors and confidence intervals obtained through 2000 bootstrap replications. Statistical analyses were performed using SPSS version 25 and AMOS version 18.
Means, Standard Deviations, Pearson Correlations, and Cronbach αs for All Measures.a

Abbreviations: GSE, general self-efficacy; HADS, Hospital Anxiety and Depression Scale; MADRS, Montgomery-Åsberg Depression Rating Scale; QOL-AD, quality of life in Alzheimer disease.
a n = 196.
b Reliability estimated by Cronbach α.
Ethical Considerations
Written informed consent was obtained from all patients and caregivers. The study followed the ethical principles outlined in the Declaration of Helsinki and was approved by the Regional Committee for Ethics in Medical Research, South-Eastern Norway.
Results
Participant Selection
A total of 1139 people were assessed for eligibility. However, 939 were excluded because they did not meet the inclusion criteria, did not respond, had somatic illness, or other reasons. Thus, 198 participants were initially included. Two participants were excluded from analysis due to incomplete data, such that 196 participants were included in the statistical analysis.
Participant Characteristics
Table 2 summarizes the participants’ baseline characteristics. The sample comprised approximately equal numbers of male and female participants, with a mean age of 70 years. Most participants were married and retired. Over half of all participants had a diagnosis of dementia, and the rest fulfilled the criteria for MCI due to Alzheimer disease. Participants with MCI and dementia significantly differed in mean I-ADL scores (MCI: 11.5; dementia: 13.3; P = .009) and mean MMSE scores (MCI: 25.3; dementia: 24.2; P = .012). However, these groups did not significantly differ on MADRS, HADS, GSE, or QOL-AD, and they had similar hobbies, ages, genders, marital statuses, schooling, formal help, work situations, and symptom durations.
Sample Characteristics of 196 People With MCI and Dementia.

Abbreviations: I-ADL, Instrumental Activities of Daily Living Scale; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; RUD-Lite, Resource Utilization in Dementia Questionnaire.
Most participants received no formal assistance were relatively independent (mean I-ADL score: 12.9) and had a high level of cognitive function (mean MMSE score: 24.1). The high mean scores on QOL-AD and GSE, and low mean scores on MADRS, suggested that the participants were well-functioning individuals with few severe depressive symptoms.
Correlations
Table 1 presents descriptive statistics, bivariate correlations (Pearson r) among all measures used in this study, and the estimated reliability of all measures (Cronbach α). The reliability estimates were within the expected range. Based on the previous report by Bjelland et al 54 showing a mean correlation of 0.56 (range, 0.40-0.74) between HADS-A and HADS-D, correlations between measures of anxiety and depression were within the expected range in the present sample (r = 0.45). With n = 196, correlations above 0.19 will be statistically significant at a rejection level of P < .01. All correlations reported in Table 1 were thereby considered statistically significant. Additionally, results showed a high correlation (r = 0.62, P < .01) between self-reported depression (HADS-D) and depression assessed by the trained health staff (MADRS).
Mediation Analysis
Table 3 presents the summary results from fitting 3 different models, with depression measured by MADRS and HADS-D and anxiety measured by HADS-A. The GSE refers to the observed additive scale measuring generalized self-efficacy, D is a latent variable measured by MADRS or HADS-D, A is a latent variable measured by HADS-A, and Q is a latent variable measured by QOL-AD. GSE → D is an example of a direct effect of GSE on D. GSE → D → Q and GSE → A → Q are indirect effects of GSE on Q, mediated by D and A, respectively. The indirect effects were of primary interest and were found to be substantial and statistically significant for both measures of depression. Figures 1 and 2 present the results of a mediation analysis with depression (measured by MADRS and HADS-D), mediating the effect of GSE on QOL-AD. Although unstandardized variables were used in the analysis, standardized coefficients are presented to simplify interpretation.
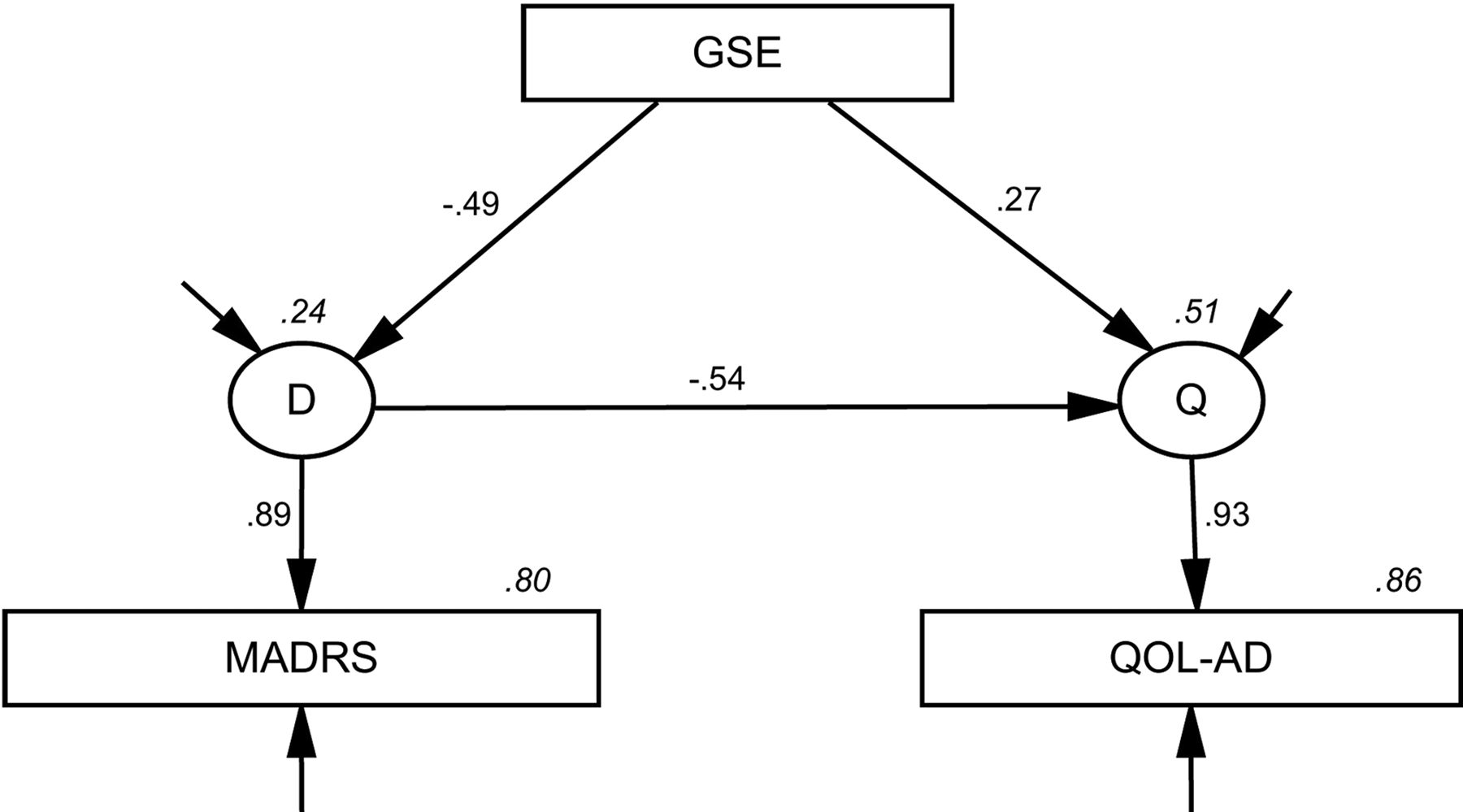
The effect of general self-efficacy on quality of life in Alzheimer’s disease mediated by depression measured by Montgomery-Åsberg Depression Rating Scale. Numbers on arrows are standardized regression coefficients, and italicized numbers indicate the explained variance in latent and observed variables.

The effect of general self-efficacy on quality of life in Alzheimer’s disease mediated by depression measured by Hospital Anxiety and Depression Scale-Depression. Numbers on arrows are standardized regression coefficients, and italicized numbers indicate the explained variance in latent and observed variables.
We fitted the same model with anxiety measured by HADS-A as the mediating variable (Figure 3). The estimated mediating effect of anxiety was substantially lower, but still statistically significant (P < .05). Overall, the results presented in Table 3 and Figures 1 to 3 indicate that our results met the 4 criteria for a partially mediated effect, as suggested by Baron and Kenny. 57

The effect of general self-efficacy on quality of life in Alzheimer’s disease mediated by anxiety measured by Hospital Anxiety and Depression Scale-Anxiety. Numbers on arrows are standardized regression coefficients, and italicized numbers indicate the explained variance in latent and observed variables.
Results From Fitting the Structural Equation Models to Observed Data.a

Abbreviations: CI, confidence interval; GSE, general self-efficacy; HADS, Hospital Anxiety and Depression Scale; MADRS, Montgomery-Åsberg Depression Rating Scale; SE, standard error.
a Standard errors, confidence intervals, and P values estimated by 2000 bootstrap replications.
Discussion
Our main results suggested that the effects of self-efficacy on quality of life may be partially mediated by depression and anxiety. Both depression and anxiety exhibited statistically significant mediating effects, but the effect of depression was stronger than that of anxiety.
The mediating effects of depression and anxiety in the relationship between self-efficacy and quality of life may have important clinical implications. Studies directly targeting depression and anxiety have demonstrated promising results, but our present findings suggest that self-efficacy itself should be an important target of psychotherapy. Studies of interventions for caregivers of people with dementia have examined the potential to alter self-efficacy through psychosocial interventions. Tang and Chan 61 performed a literature review of 14 studies of self-efficacy among caregivers and found that most psychosocial interventions for caregivers yielded small-to-large effects on self-efficacy. For example, self-efficacy significantly improved after an in-home caregiver psychoeducational training program, 62 which is consistent with findings from other studies. 63 -65 Researches have also examined psychosocial interventions that target self-efficacy in patients with dementia. Analysis of a psychoeducational intervention (the Early Diagnosis Dyadic Intervention) for care recipient/caregiver dyads who received early psychosocial intervention revealed no statistically significant changes in self-efficacy. 66 This finding is consistent with the results of other psychosocial interventions for early-stage dementia—including a 12-week health promotion course 67 and a group intervention of cognitive rehabilitation, 68 both of which yielded no improvement in self-efficacy. On the other hand, in a study of people with early-stage dementia, self-efficacy was increased (Cohen d = 0.35) at 3 months in an intervention group who participated in psychoeducational groups, compared to in a group who received treatment as usual. 69
Another important question is how to increase self-efficacy in people with dementia as they experience a continuous and progressive decline in cognitive functioning. Bandura 18 reports that the most influential way to increase self-efficacy is through mastery experience based on prior personal experience. However, this may not be possible for people with dementia, as the disease leads to decreased abilities to perform daily activities that they had no problems with earlier, such as cooking, cleaning, or handling economics. 70 Convincing people with dementia that certain behaviors will lead to a desirable outcome will not necessarily promote behavioral change, unless they are convinced that they can perform the activity in the required situations. For example, a person with dementia may believe that pleasant activities will improve mood (high-outcome expectancy), but may still dismiss this health strategy because they have low expectancy of self-efficacy. 71 Thus, it is highly important that health professionals tailor interventions that comprise realistic activities when attempting to enforce higher self-efficacy expectations.
Self-efficacy might be related to other constructs from positive psychology, such as resilience, hope, optimism, and self-esteem. One study demonstrated that individuals with MCI and mild dementia had lower spiritual well-being, social support, self-esteem, life satisfaction, positive affect, optimism, and hope, as well as higher negative affect scores, compared to a control group of healthy old-age people. 72 Similarly, another study reported that self-efficacy, optimism, and self-esteem were positively associated with living well (quality of life, well-being, and life satisfaction) among people with mild-to-moderate dementia from a community cohort. 73 Accordingly, other cross-sectional studies in people with dementia have revealed that higher self-esteem predicts higher quality of life. 74,75 Moreover, an 8-week self-esteem intervention (comprising music therapy, humor therapy, art therapy, dancing therapy, recreation, and health education) yielded reduced depressive symptoms and improved quality of life, self-esteem, and cognitive function in people with MCI. 76 Notably, analyses reveal overlap among these constructs, demonstrating that a person with high self-efficacy will likely also have high self-esteem and optimism. 73
In the present study, we focused on the effects of self-efficacy on depression and anxiety; however, this relationship may be nonrecursive. As suggested by Bandura, 18 depression will negatively influence confidence in one’s capabilities. Thus, another means of influencing self-efficacy is by altering inner emotional and physical states, indicating that health professionals could also directly target emotional states, such as depression and anxiety. Such a strategy may be supported by CBT, which focuses on increasing the frequency of pleasant experiences and decreasing unpleasant events. 12,77 Intervention studies among people with dementia have demonstrated that mood can be effectively increased through reminiscence therapy—which involves reflection on past activities, events, and experiences. 12,78,79 Interventions could also utilize strategies that simultaneously aim to improve self-efficacy and reduce depressive and anxiety symptoms. Such an approach was investigated in a study of people with dementia, using psychoeducational groups that focused on how to cope with and manage the disease, including associated memory problems (thereby increasing self-efficacy), and increasing pleasant events and enjoyment of hobbies (thereby reducing depression). 69,80 The participants showed gains in self-efficacy at 3 months (Cohen d = 0.35) and 6 months (Cohen d = 0.23) and a reduction of depression at 6 months after the intervention (Cohen d = 0.34).
Limitations, Strengths, and Future Studies
Although our present results contribute to an understanding of the relationship between self-efficacy and quality of life, there are several limitations regarding the conclusions that can be drawn. Causal inference requires control of confounding variables and the temporal ordering of events and is thus challenging when variables are measured at the same time and possible confounding variables are omitted. This seems to be a widespread issue. For example, Frazier et al 81 found that mediation analysis was performed using cross-sectional data in nearly all studies that they surveyed in the field of counseling psychology. It would be useful to perform future studies with a longitudinal design. Additionally, the relationship between depression/anxiety and self-efficacy may be nonrecursive. Consequently, our conclusions are limited to stating that the present data reveal a covariance pattern that is consistent with the interpretation that the effect of generalized self-efficacy is partly mediated by depression.
Questions have been raised regarding the accuracy of self-reported depressive and anxiety symptoms in people with dementia, due to memory and language problems that may cause difficulties in understanding the questions being asked, articulating answers, and recalling mood state. However, the reliability of the scores in our study was strengthened by the high correlation between the depression score on MADRS (completed by health professionals) and on HADS-D (self-reported by the people with MCI/dementia; Table 1, r = 0.62, P < .01).
Another limitation may be the mixed sample of patients with amnestic MCI and dementia. However, there were few baseline differences between the 2 groups. Moreover, in practice, the distinction between MCI and dementia often depends only on the premorbid cognitive level. Consequently, although the sample was heterogeneous, the mixed sample was representative of people with amnestic MCI and mild dementia due to Alzheimer disease in outpatient health-care settings. Nevertheless, validation in new samples will be required to generalize the present findings to patients with severe dementia and with more diverse background characteristics. Lastly, since there may be overlap between self-efficacy, self-esteem, and optimism, future randomized controlled studies with longitudinal designs are needed to examine whether psychosocial interventions can improve these areas in people with MCI and dementia.
Conclusion
To our knowledge, this is the first study to examine a mediation effect of depression and anxiety in the relationship between self-efficacy and quality of life in people with MCI and dementia. Our findings suggest that increased self-efficacy may positively impact quality of life in this group of patients, partly by reducing depression and anxiety. The results of the current study may have important implications, particularly if validated with replication, and in studies with longitudinal designs that permit stronger conclusions regarding the directions of causal effects. The findings support the further development of interventions tailored to increase self-efficacy, and to thereby decrease depression and anxiety and improve quality of life, in people with MCI or dementia.
Supplemental Material
Supplemental Material, Co-author_declaration_Paper3 - Effect of Self-Efficacy on Quality of Life in People With Mild Cognitive Impairment and Mild Dementia: The Mediating Roles of Depression and Anxiety
Supplemental Material, Co-author_declaration_Paper3 for Effect of Self-Efficacy on Quality of Life in People With Mild Cognitive Impairment and Mild Dementia: The Mediating Roles of Depression and Anxiety by Johanne B. Tonga, Dag-Erik Eilertsen, Ingrid K. Ledel Solem, Espen A. Arnevik, Maria S. Korsnes and Ingun D. Ulstein in American Journal of Alzheimer"s Disease & Other Dementias
Supplemental Material
Supplemental Material, ICMJF_Disclosure_Form_for_Conflict_of_Interest_Form - Effect of Self-Efficacy on Quality of Life in People With Mild Cognitive Impairment and Mild Dementia: The Mediating Roles of Depression and Anxiety
Supplemental Material, ICMJF_Disclosure_Form_for_Conflict_of_Interest_Form for Effect of Self-Efficacy on Quality of Life in People With Mild Cognitive Impairment and Mild Dementia: The Mediating Roles of Depression and Anxiety by Johanne B. Tonga, Dag-Erik Eilertsen, Ingrid K. Ledel Solem, Espen A. Arnevik, Maria S. Korsnes and Ingun D. Ulstein in American Journal of Alzheimer"s Disease & Other Dementias
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for the research by The Norwegian Association of Health and Department of Old Age Psychiatry, Oslo University Hospital.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.