
Abstract
Background:
The creative use of reminiscent music and natural movements were reported to have positive effects on the well-being of older adults with cognitive impairment.
Objectives:
To explore the effects of the intuitive movement reembodiment (IMR) program on the quality of life (QoL) of older adults with dementia.
Methods:
Data collected from 22 participants were analyzed: group 1 (mild dementia), group 2 (moderate dementia), group 3 (advanced dementia). All study groups participated in 10 weekly sessions. Self-reported QoL ratings were gathered through using the World Health Organisation (WHO)-5 questionnaire, alongside qualitative evidence recorded through onsite observation.
Results:
Statistically significant improvement in QoL was demonstrated after session 6. The qualitative analysis showed that the IMR sessions provided a sense of humor, imagination, and intuition that motivated the participants to dance and interact with joy.
Conclusion:
These preliminary positive findings need to be replicated in a larger randomized controlled trial.
Introduction
Familiarity with the reminiscent music unlocks implicit memories and other remaining cognitive capacities in people with dementia. 1 –3 Natural gestures stimulated by the reminiscent music displays the instinct of moving in people with dementia. 4 This pilot study presents an original creative dance program−intuitive movement reembodiment (IMR), which uses reminiscent music and natural gestures of people with dementia to design a series of dance exercises. In an IMR routine, the participants were taught a combination of gesture-like movements collected from them during the singing session as they responded to the music intuitively. After the demonstration and practice sessions, they were guided to perform the composed routine independently following the musical cues that were rearranged based on the same music repertoire. Constructed in the form of community dance activity, the IMR program aims to promote better quality of life (QoL) for people with dementia by providing memory stimulation, mood moderation, and social interaction.
Research using music and movement has been proven to be effective in improving the QoL of older people with cognitive impairment and dementia. 5 –11 In some of them, the use of intuition, creativity, and improvisation has been explored extensively and has produced positive outcomes. 8,11 In this study, the musical component of the IMR program was constructed using repetition and the Rhythmics concept of the Dalcroze Eurhythmics theory. 12,13 In music, duplicate elements and structured patterns contribute to the development of memory as transitional objects in brain. 14 During an IMR session, consistent repetitive patterns of melody and rhythm foster the effectiveness in improving the passivity of people with dementia in receiving information. Additionally, the time–energy–space concepts of the Rhythmics concept were engaged to stimulate the participants’ spontaneous physical responses by enhancing their concentration in listening to music and thinking. 12,13 Created by composer and music educator Émile Jacques-Dalcroze (1865-1950), the Eurhythmics method has been practiced as a form of music therapy through which the action of perceiving music depends on aural sensations completed by muscular sensation. Through moving to the music spontaneously, the act of listening is a form of thinking embodying the mind–body connection.
People with Alzheimer disease still possess preserved implicit memories despite their significant explicit memory loss. 15,16 The repetitive reembodiment of natural gestures can potentially stimulate underlying implicit memory by reactivating their bodies with familiar sensory experience. 17 Through repetition, a feeling of familiarity and habit can be developed unconsciously and effortlessly by activating the preserved implicit memory. In fact, exposure to familiar stimuli can spontaneously trigger appropriate functional activities, and effectively improve the functional ability in daily tasks of people with dementia. 15,16
Apart from the application of repetition, the movement creating process of the IMR routines uses the effort qualities concept of the Laban movement analysis theory created by Rudolf von Laban (1879-1958). 18,19 Laban movement analysis is a systematic approach for observing, describing, and analyzing changes in human movement. Ultimately, such a creative process of movement exploration creates specific mental simulations that motivate the participants to move spontaneously with joy.
This pilot study aimed to explore: the effects of the IMR program on the QoL of older adults with dementia, and the feasibility of conducting a larger study.
Hypothesis: The creative use of reminiscent music and natural gestures can improve the QoL of older adults with dementia and increase their joy.
Method
Research Approach
This pilot study used mixed methods to collect and analyze data. The QoL results were sought through a quantitative approach and elaborated by the qualitative data. The research framework encompasses an interdisciplinary methodology inclusive of arts, social, and health sciences, with the aim of promoting a holistic wellness of people living with dementia. Inclusion and exclusion criteria for this study were as follows:
Inclusion criteria
(1) Age 60 to 95 years, (2) physically able to take part in singing and dancing activities, (3) diagnosis of dementia by a trained health professional, (4) English as their first language.
Exclusion criteria
(1) Severe hearing impairment, (2) clinically significant depression, (3) agitation preventing attentive attendance for the required session duration, (4) paresis due to stroke impairing mobility.
Participants
A total of 26 New Zealand older adults were recruited for the study. There were 9 men and 17 women; mean age 77.6 (11.8 SD), range: 63 to 95 years ( See Table 1). The great majority were European and only 1 participant was of Māori ethnicity. The participants were either outpatients of the Gibson Day Unit (GDU) (Dunedin Public Hospital) or residents of the Enliven St Andrews Care Home (Dunedin). All underwent clinical assessment by a psychiatrist to establish a diagnosis of dementia prior to referral to the day unit or to transition to long-term care.
Study Participants.a

aTotal N = 22.
Based on the information provided by the institutions, the participants were categorized into 3 groups: group 1 (mild dementia), group 2 (moderate dementia), group 3 (advanced dementia). Ultimately, the quantitative analysis measured data from 22 participants (7 males and 15 females) who attended no fewer than 6 sessions. Unanticipated absences occurred and have caused missing data due to the following reasons: (1) discharge from the GDU, (2) unfit physical conditions, (3) lack of interest, (4) other commitments.
In addition, 4 staff members (1 nurse specialist and 3 clinical specialists) from the GDU and 3 (2 activity coordinators and 1 volunteer) from the Enliven St Andrews Care Home participated in the informal interview and have contributed valuable information to the qualitative data.
Procedure
An ethical approval (reference number H17/153) under category A (health research with intervention or observational approach) was granted by the human ethics committee of the University of Otago, alongside a Māori Consultation provided by the Ngāi Tahu research consultation committee.
The practice conducted at the Gibson Day Unit (Dunedin Public Hospital) was granted with a Locality Authorization (project ID 01425) by Health Research South. The participants selection was made based on the recommendation offered by the management of the GDU and Enliven St Andrews Care Home, who made sure that the participants’ physical and psychological conditions allowed them to take part in the study safely. The participants’ interest in music and dance was not a selecting criterion in the recruiting process.
Sampling
This is in essence a convenience sample. The participants were approached by the staff members and provided with an information sheet and consent form. The consent form was signed only if the participants fully understood and accepted the research procedures and conditions. If they were unable to perform the consent procedure, a family member who is a designated welfare guardian would fulfill the task on their behalf. Also, the staff members were approached with the same information sheet and consent for their involvement in the information interviews. Anonymity was granted for all participants although their real names were used during the intervention session. The staff members at the Gibson Day Unit and Enliven St Andrews Care Home agreed to be addressed by their real first names.
Intuitive Movement Reembodiment Sessions
Ten weekly IMR sessions were conducted from March to May 2018. They were offered in the early afternoon (11-12 o’clock). Each week, the same music repertoire, movement concepts, and improvisation themes were employed for all study groups.
An IMR session was divided into 2 parts: I. Piano playing and singing (5-10 minutes)
This session warmed the participants up and built a rapport between the facilitator and participants. Clapping was incorporated to foster their sense of musicality. The participants’ nonverbal body language was recorded and utilized as the raw material for the dance session. II. Dancing (30-40 minutes)
This session comprised 6 individual routines. Independent practice was attempted after the movement demonstration and 2 practices with music. The participants were seated most of the time.
Intuitive Movement Reembodiment Program Description
The IMR program consists of 6 routines: I. Movement patterning
This exercise is a combination of 2 respective movements structured in the A-B-A-B format.
Music: Preferably 4/4 time signature Moderate and consistent tempo Significant distinctive patterns of A and B Significant contrasting rhythms of A and B (such as melodic vs march, waltz vs march) Significant contrasting dynamics of A and B (softer vs stronger) Recommended songs: You are My Sunshine, Yellow Submarine, The Road to the Isles, Side by Side, Hey Jude II. Synchronize-with-the-Music (Pitch) (See Table 2)
Variations in Pitch and Synchronous Movements.
The participants are taught a gesture or movement that can be reperformed with synchronous alternatives.
Music: 3/4 or 4/4 time signature Variations in tempo and dynamics are significantly emphasized. Recommended songs: Edelweiss, Amazing Grace, Cruising Down the River, Waltzing Matilda III. Synchronize-with-the-Music (Tempo and Dynamics) (See Table 3)
Variations in Tempo and Synchronous Movements.

The participants are taught a gesture or movement that can be reperformed with synchronous alternatives. IV. Move-and-pause (See Table 4)
Variations in Move and Pause.

The participants perform a particular movement repetitively such as marching, and pause as indicated by the musical cue “rest.”
Music:
4/4 time signature in march rhythm
Accentuated on the first count
Recommended songs: The Camptown Faces, Yellow Submarine, Loch Lomond, John Brown’s Body, Red River Valley, Supercalifragilisticexpialidocious
Note:
Participants may “march” in the chair and clap if they encounter physical difficulties in standing and walking.
Percussion instruments and props such as pom-poms can be incorporated.
V. Contrasting Movement
When the music pauses, the participants perform the contrasting movement that is either opposite or reverse to the demonstrated one.
Music:
Any time signature and rhythm
Pause the music for 4 counts every 2 bars
Recommended songs: Chorus from the tunes Yellow Submarine, Waltzing Matilda, Let It Be
VI. Themed improvisation
This exercise is a free improvisation structured around a given theme. During the “story telling” preparatory session, the facilitator may pick up any instant movement of the participants any time. The participants may explore the movements as far as their physical conditions allow.
Music:
Any time signature
Variations in tempo
Variations in rhythmic
Variations in dynamics
Note: Preferably themes associated with the participants’ lived experiences such as “baking cake,” “laundry washing,” “basketball dance,” “bubbles and rocks,” and “tress and wind.” Expressive props such as scarf can be incorporated.
Data Gathering
At baseline and following each IMR session, the participants’ self-reported Well-Being scores (QoL) was collected using the WHO (5) Well-Being Index Questionnaire. A recent review by Topp et al in 2015 demonstrates that the WHO-5 has high clinimetric validity and can be used as an outcome measure balancing the wanted and unwanted effects of treatments. The WHO-5 is a short questionnaire consisting of 5 simple and noninvasive questions, which tap into the subjective well-being of the participants. In the questionnaire, the participants were required to indicate how they have been feeling over the last 2 weeks according to 5 statements: I have felt cheerful and in good spirits. I have felt calm and relaxed. I have felt active and vigorous. I woke up feeling fresh and rested. My daily life has been filled with things that interest me.
The score of each statement ranges from 0 to 5. The raw score is multiplied by 4 to obtain a percentage score ranging from 0 to 100, with 100% the highest score of QoL.
Also, participant observation and informal interview were used to collect qualitative data. The participants’ verbal and nonverbal responses were recorded without undertaking audio or video recording. The staff members of the GDU and Enliven St Andrews Care Home were interviewed informally during and out of the sessions. The qualitative data were collected in the written form as field notes and cross-checked with the staff members regularly.
Data Analysis
All participants’ self-reported QoL ratings collected throughout 10 weeks were analyzed using the paired t test, dependent sample t test ( See Table 5). A combined graph was also produced for further comparison among 3 groups.
Statistical Analysis.a

a z for 95% CI = 1.96; declare P larger than α = 0.05 is not significant.
bBaseline to Session 6: t = −17.087 Pr(T > t) = .001.
cBaseline to Session 10: t = −0.9644 Pr(T > t) = 0.0936.
The qualitative data were analyzed through thematic analysis. To systematically analyze the participants’ responses in individual sessions, the field notes were interpreted and sorted into 3 themes: memory recollection, social interaction, and enjoyment. Indications of the themes recorded weekly were marked in a table.
Results
The quantitative analysis used data collected from 22 participants (of 26) who completed no less than 6 IMR sessions. The participants’ mean Well-Being scores increased from 73 at baseline to 81 at the end of the intervention (session 10). The 95% confidence interval for this difference (4.6, −12.6) was wide, largely driven by the small sample size. However, when testing for differences between baseline and scores following session 6, the mean difference was statistically significant (t = 17.1; P = .001). See Table 5 for detailed statistical analysis.
Qualitative Analysis
As shown in Table 6, in group 1 and 2, numerous positive responses in the form of Memory Recollection, Enjoyment, and Social Interaction were observed consistently throughout the 10 weeks. Throughout the session, especially during the themed improvisation routine, the participants in group 1 shared many personal stories stimulated by the music, movement, and the given concept. Discussion about past memories were initiated and elaborated, for instance: “I used to make nappies for the babies in the 70’s” (participant #3, mid-70s)—after the song Hey Jude; “I did house chores for the whole family” (participant #1, early 60s)—after the “laundry washing” dance. On several occasions, the participants in group 2 sang some other songs and danced in a circle, presumably as they used to do in the past. Actions of memory recollections were observed almost every week: “my friend used to work in a freezing cold butchery” (participant #12, mid-70s)—after Move-and-Pause; “I used to play piano when I was young” (participant #13, late 60s)—after the singing session. However, most of the time they hesitated to extend the conversation associated with the recalled memory and ended it shortly. Nevertheless, responses associated with memory recollection were rarely observed in group 3.
Thematic Analysis.
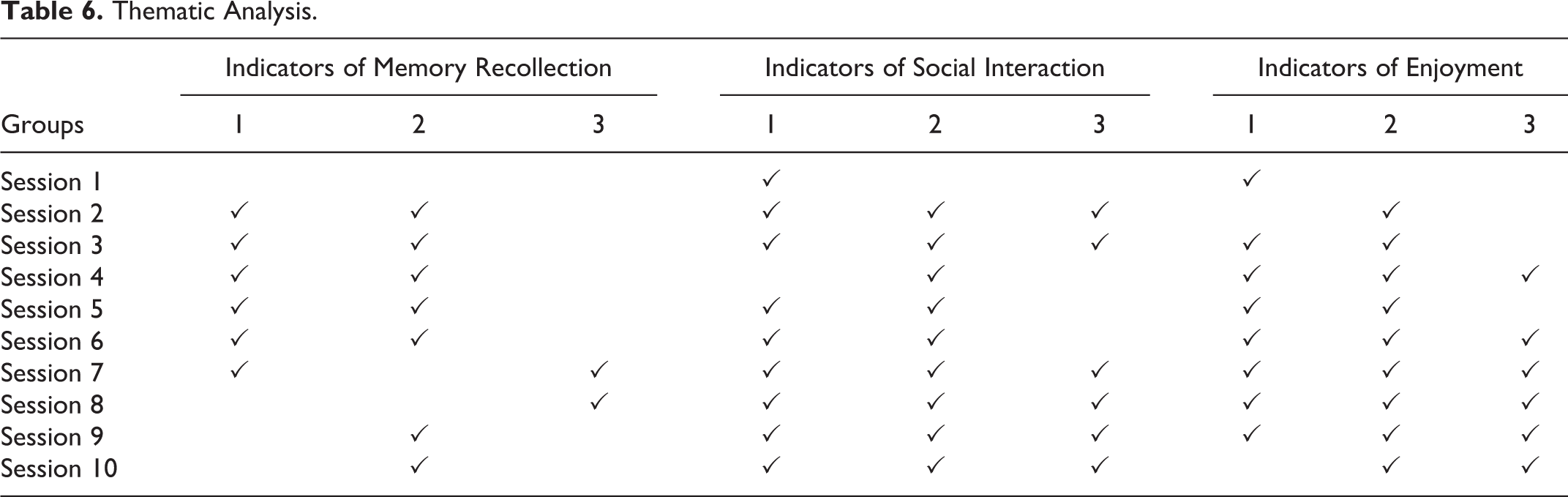
In addition, the participants regularly offered positive feedback regarding their enjoyment in the IMR session: “I felt it [Move-and-Pause] stimulated my brain!” (-participant #3, mid-70s); “I have never done this (Synchronize-with-the-Music) before, I must show him [husband] today!” (participant #2, early 70s). Consequently, such spontaneous responses often translated to further social interaction including movement mirroring, joke making, and sharing of stories accompanied with smiles and laughter. Interestingly, the participants in group 2 demonstrated a great sense of humor as observed on numerous occasions of social interaction: #12 (mid-70s) and participant #14 (late 60s) messed with each other’s laundry because “they were not good at washing clothes”; participant #13 (late 60s) blew back at the facilitator vigorously in response to the imaginary “strong wind” while Participant #12 (mid-70s) trembled like a shaking tree.
During the data collecting period, the speech impairment and physical passivity of group 3 made it technically difficult to capture and understand the participants’ verbal and nonverbal expressions. Such a complicated situation inevitably hindered efficient recordings and interpretations of the participants’ responses, as displayed by the inconsistent data in group 3.
Discussion
In this pilot study, improvement in QoL was observed after 6 IMR sessions. However, by the tenth session, this effect was no longer significant. The largely distinctive scoring patterns of 3 respective groups reflect that, the participants’ QoL was primarily determined by individuals’ health and social conditions, which in turn decisively influenced the effects of the IMR sessions. 20,21
According to the thematic analysis, numerous positive responses were associated with humorous expressions and playfulness. 1 For instance, participant #14 (late 60s, group 2) often created funnier versions of the given movement and poses; participant #20 (late 80s, group 3) who lacked interest in moving, actively engaged in the Move-and-Pause routine when she was allowed to pose “awkwardly.” Birt et al (2017) explain that “in dementia humor may be a way of approaching and dealing with the inevitable losses which accompany changing status and roles.” 2 Based on the observation outcomes, the participants displayed more affinity toward the session when given more freedom and space to generate fun and laughter.
All study groups portrayed a significant degree of imagination through performing movement improvisation. 17,18 In the “bubble & rock” dance (themed improvisation) where an imaginary rock was passed around in the circle, some participants enjoyed embodying the “heavy and hard” features of a rock. Participant #3 (mid-70s, group 1) liked this imagery concept and practiced it at home: “I played the ‘bubble and rock’ with my grandchildren and they loved that!” Senior activity co-ordinator at the Enliven St Andrews Care Home, Mary complimented the use of the imagery element: “They [the Group 3 members] really enjoyed passing the rock!” In line with this finding, Boyle suggests that pragmatic and creative forms of agency shall be provided to people with dementia, especially those in an advanced stage who are still able to express their perceptions, feelings, and desires in habituated, embodied, or emotional forms−“People with dementia may still demonstrate imaginative agency.” 22 By engaging familiar stories and movement themes, the use of creative movement can effectively stimulate the imaginative capacity of people with dementia, which then can be expressed through their natural body language. 22,23
Intuition—the key element of the IMR program—was evidently effective as a sense of aliveness was frequently observed in most participants during and after the session. 4,17 In session 3, participant #3 (mid-70s, group 1) said, “I felt it [the exercise] stimulated my brain!”; participant #2 (early 70s) agreed and added, “It’s the concentration that exercised our brains!” These comments suggest that Intuition was able to enhance the participants’ spontaneity in moving leading to enjoyment. 17,23 Kontos elaborates that “the key to the seemingly inexplicable coherent and spontaneous expressions of musicality that emerge from the depths of dementia is to be found in the body’s own primordial potential and sociocultural significance that sustain selfhood at pre-reflective level.” 23 The intuition-led approach, which allowed the participants to move spontaneously as called upon by their instinctive musicality, effectively increased their ability in engaging their mind and expressing their emotions.
The group context of the IMR session also fostered the participants’ social interaction with peers and staff. 5,11 The interactions in verbal and nonverbal form generated meaningful communication and friendship among them. Discussions extended from the recalled memories, the spontaneous “social dancing” and the use of animated facial expressions when responding to peers were among the interactive activities observed. Senior activity co-ordinator at the Enliven St Andrews Care Home, Mary recalled, “Although most of them [in group 3] cannot perform the movements very well, I still could see that they interacted with each other a lot and enjoyed the session very much…You can see that from the spark in their eyes.” For those whose physicality has been severely compromised by the disease, interacting with other participants even through the tiniest gestures could serve as a source of agency and empowerment. 9,24
Information obtained from informal interviews with staff and participants, on the other hand, highlighted the reasons for the decline in interest of participants in groups 1 and 2, which showed a decrease in fewer indicators of positive responses (and the concurrent lower QoL) in the last 4 sessions. Firstly, the continuous practice of the dance routines became repetitive and predictable and therefore the participants of groups 1 and 2 lost the feeling of excitement they had had in the beginning. Secondly, the group 2 members felt overwhelmed by the number of challenges presented and did not enjoy being continuously “mentally threatened.”
Limitations
Due to the study’s nature as a leisure-based community activity, no control group was enrolled. Also, an inconsistency in the collected data was inevitable due to the difficulty in maintaining regular attendance of individual participants in the sessions.
Future Research Directions
Both the statistical results and the qualitative findings suggest that an alternative arrangement, for instance a 3-week interval between 5 continuous sessions, is more advisable for outpatients having mild-to-moderate dementia. Weekly outpatients at the GDU, who still enjoyed a normal community life, were inclined to perceive the IMR program as a leisure activity rather than an essential intervention. 25 On the other hand, continuous weekly intervention is recommended for the long-term hospitalized residents with advanced dementia who lack constant contact with family and community. 24 The setbacks mentioned in the Discussion section indicated that new creative elements need to be constantly introduced in order to maintain the participants’ interest. Easier and more relaxing exercises should be implemented between the set IMR routines in order to allow them to enjoy the whole session more comfortably. These preliminary positive results should be supported by a larger randomized controlled trial.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.