
Abstract
The present study examined the effects of a telephone-based cognitive behavioral intervention on dementia caregivers’ quality of life (QoL). A total of 273 caregivers were randomly assigned to an intervention or control group. The intervention comprised 12 telephone sessions of individual cognitive behavioral therapy (CBT) over 6 months. At baseline, postintervention, and 6-month follow-up, QoL was assessed with the World Health Organization QoL-BREF, which measures perceived QoL for the domains physical health, psychological health, social relationships, and environment as well as overall QoL and satisfaction with general health. Intention-to-treat analyses using latent change models were performed. At postintervention, intervention group participants reported better overall QoL and satisfaction with general health as well as better physical and psychological health compared to control group participants. Together with existing evidence, the results suggest that the telephone CBT intervention does not only reduce impairments but also fosters improvements in health-related QoL.
Introduction
Across the globe, the primary caregivers for people with dementia are family members. 1 It is well known that family caregivers of people with dementia face a number of challenges that negatively impact their health and well-being. 2 The numerous challenges of caring for a relative with dementia include coping with the behavioral and psychological symptoms of dementia (eg, agitation, aberrant motor behavior, and delusions) and the gradual loss of central qualities of primary relationships (eg, mutual caring and reciprocal exchanges of affection and assistance). 3
Fortunately, research has shown that interventions can effectively improve dementia caregiver outcomes. 4 However, to date most studies have focused only on caregivers’ symptoms, problems, and complaints, and more research on how interventions also affect dimensions of optimal health and human flourishing is critically needed. 5 The World Health Organization (WHO) defines health as “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity” (p 1). 6 Over the past 2 decades, the positive psychology movement has likewise stimulated increased recognition that human flourishing entails more than just the absence of pathology and suffering. 7 Evaluating the full effectiveness of a caregiver intervention should therefore entail assessing not only whether it reduces impairments but also whether it helps participants to thrive. Experts recently identified dementia caregivers’ quality of life (QoL) as an important “positive” outcome for psychosocial intervention research, with the Short-Form Health Survey (SF) scales, EuroQol-5D (EQ-5D), and the WHO Quality of Life instrument (WHOQoL) as the best measures of QoL currently available. 8 In the current study, we therefore assess the effect of a telephone-based cognitive behavioral therapy (CBT) intervention on dementia caregivers’ QoL.
Previous Research on the Effects of Dementia Caregiver Interventions on QoL
In the following, the findings of different types of caregiver interventions on QoL are grouped according to a recent classification that distinguished psychoeducational interventions, occupational therapy interventions, respite care, and cognitive-behavioral therapy (CBT). 4 Due to the heterogeneity of interventions, outcome measures, and settings, we include information about the specific intervention and QoL outcome measures in our review.
Psychoeducational interventions focus on improving participants’ knowledge and coping skills (through, eg, problem-solving techniques or skill-building activities) and providing social support. Evidence suggests that single component psychoeducational interventions that solely focus on one strategy or activity do not appear to improve caregivers’ QoL (social support intervention: EQ-5D 9 ; family meetings intervention: SF-12 10 ; disease management program: EQ-5D 11 ). Evidence for multicomponent psychoeducational interventions that offer participants a range of activities is mixed, with some improving QoL (dementia family care program: WHOQoL-BREF 12 ; coping strategy training: HSQ: mental health domain 13,14 ; individual-based psychoeducational intervention program: SF-36, GHQ-28 15 ; and enhanced counseling and support treatment: self-rated health adapted from Older Americans Resources and Services Multidimensional Assessment Questionnaire 16 ), and some not (education and training intervention: WHOQoL-BREF 17 ; group-based psychoeducational intervention program: SF-36, General Health Questionnaire [GHQ-28] 18 ; and psychosocial counseling and support program: European Quality of Life - Visual Analogue Scale [EQ-VAS] 19,20 ). The REACH study 21 investigated the effects of a multicomponent intervention on a QoL indicator comprising measures of both positive and negative outcomes (depression, self-care, burden, social support and problem behaviors of the care recipient) and also found positive treatment effects.
Occupational therapy interventions aim at maintaining and improving independence and participation in activities of daily living through performing meaningful activities and increasing the ability to handle problematic behaviors as well as the sense of competence. Positive effects on dementia caregivers’ QoL were only found for individual occupational therapy interventions (perceived change index 22 ; Dementia QoL Instrument, GHQ-12 23 ), whereas no benefit was found for a group-based occupational therapy intervention (EQ5-D and GHQ-28). 24
Respite care provides caregivers with a temporary breakthrough community-based (in-home or host family respite) or residential respite care (day care, temporary residential admission, and nighttime care). To our knowledge, evidence from randomized controlled trials (RCTs) comparing the effect of respite care on dementia caregivers’ QoL to that of a control condition is still lacking. 4,25 One quasi-experimental study including patients and family caregivers (not limited to dementia) compared the effects of geriatric day care offering a rehabilitation program, social contacts, and constructive activities to the care recipients and information about the disease to the caregivers to an untreated matched control group (CG). No significant differences in caregivers’ life satisfaction (life satisfaction questionnaire) were found. 26 Two other studies used respite care as the control condition and produced ambiguous results. One quasi-experimental study compared an integrated family support program with geriatric day care and found no significant differences in their impact on caregivers’ general health (GHQ-28). 27 One RCT found that polarity therapy (ie, a type of touch therapy) had superior effects on health-related QoL (SF-36) than respite care. 28 All in all, current evidence regarding the effects of respite care on caregivers’ health and well-being should be treated with caution, as the quality of the evidence has mostly been rated as low, and well-designed trials are needed before any conclusions can be drawn. 4,25
Of the 4 different kinds of caregiver interventions, CBT interventions have been consistently found to be most effective across various outcome measures. 29,30 CBT is particularly suitable for supporting dementia caregivers, as it aims to help participants develop cognitive and behavioral skills for managing their complex and demanding role. Wilz et al 31 provide an overview of research supporting the effectiveness of cognitive behavioral strategies such as changing dysfunctional cognitions (eg, perfectionism in care as a barrier for using professional or informal support) and improving emotion regulation strategies (eg, for coping with predeath grief and other stressful emotions like anger, shame, and anxiety) for improving many aspects of caregivers’ health and well-being. Given that effect sizes in psychosocial intervention research in dementia care are generally small, 32 one study 33 found extraordinarily large-sized effects of CBT on depression and medium-sized effects on increases in engagement in pleasant events as well as on reduction in dysfunctional thoughts at postintervention compared to a control group. A significant medium-sized effect of CBT on depression was maintained until follow-up. 33 Others 34 reported medium-sized effects of CBT on self-perceived health and dysfunctional thoughts.
Research, however, on the effects of CBT interventions on caregivers’ QoL remains scarce, and the few available studies have evaluated interventions that are based only in part on CBT. One study investigated the effects of psychodynamic group therapy (classified as a CBT intervention) 35 which targeted several aspects of the caregiver role (eg, feeling lonely and helpless, family conflicts, changing family dynamics) and encouraged caregivers to explore their emotions (eg, sadness, frustration, anger, guilt) but found no treatment effects on caregivers’ QoL (WHOQoL). 36 Two other studies 13,14 evaluated the effects of a blended intervention that consisted of psychoeducational components (eg, learning about dementia and caregiver stress), discussing problematic behaviors of the care recipient and difficult situations as well as elements of CBT (eg, behavioral management techniques, self-care skills including changing unhelpful thoughts, and promoting acceptance). Compared to a control group, intervention group participants had better health-related QoL (mental health domain of the HSQ) over an 8-month as well as 24-month evaluation period. 13,14 One other study evaluated a CBT group intervention focused on managing dysfunctional thoughts and self-help techniques that yielded significant improvements in mental health (GHQ-12) but no statistically significant treatment effects on QoL (Ruiz & Baca’s QoL Questionnaire). 34
Finally, in previous work, we evaluated the effects of the Tele.TAnDem intervention on caregivers’ QoL. To our knowledge, Tele.TAnDem 31,37 is the first telephone-based CBT-based intervention specifically adapted for family caregivers of people with dementia. Many dementia caregivers have problems participating in face-to-face interventions because they cannot leave the care recipient alone, have physical constraints, or live in rural areas with poor infrastructure. The telephone setting, however, enables caregivers to integrate the intervention sessions into their everyday lives, thereby increasing access and overcoming barriers to participation. 38 Intervention participants receive either seven 60-minute therapeutic sessions delivered over 3 months (short-term intervention) 37 or twelve 50-minute sessions delivered over 6 months (extended intervention). 31 The intervention was extended because participants evaluated the short-term intervention as helpful but the number of sessions as too few and the duration of the intervention as too short. 37 Tele.TAnDem sessions are focused on managing the care recipient’s behavior problems and personality changes, self-care, reducing social isolation, utilizing professional and informal support, reducing stress, regulating emotions, reinforcing positive activities, and accepting role change and loss. Previous studies support the effectiveness of the Tele.TAnDem intervention with regard to a number of outcomes. 31,37,39,40 With respect to QoL specifically, we found that participants of the short-term intervention who were still caring at home 2 years posttreatment reported significantly higher overall QoL and satisfaction with general health and higher scores in the domain environment than those in the control group (WHOQoL-BREF). 41 The effect of the extended intervention on caregivers’ QoL has not yet been evaluated.
Research Objective
To date, caregiver intervention research has primarily focused on how well interventions can reduce participants’ symptoms and complaints. Recognizing that health is more than just the absence of disease, more research on the effects of dementia caregiver interventions on positive outcomes like QoL is needed. Although CBT interventions can be considered as particularly suitable for supporting dementia caregivers and have yielded promising results, little is known about the effects of CBT interventions on dementia caregivers’ QoL. In the current study, we therefore examine the effects of the extended Tele.TAnDem intervention on caregivers’ QoL. Quality of life was included as a secondary outcome measure in the RCT that evaluated the effectiveness of the extended Tele.TAnDem intervention. 42 Data on secondary outcomes like QoL are often not reported or provided only in insufficient detail. 35 In the current study, we focus exclusively on QoL in order to highlight its importance as a positive outcome measure in dementia caregiver intervention research.
Method
Sample and Procedure
The present study is based on data from an RCT evaluating the effectiveness of the Tele.TAnDem intervention compared to usual care. 31,42 In this RCT, the extended Tele.TAnDem intervention was delivered in established care provision structures. Family caregivers were eligible to participate if they were primarily responsible for the home-based care of a person diagnosed with at least low-grade dementia. As an effectiveness study, the study did not include any threshold of baseline scores with regard to any outcome measure as inclusion criteria but included all interested caregivers who felt burdened by the care situation and wished for (more) support. Exclusion criteria were ongoing psychotherapy, severe physical illness, or psychiatric disorder of the caregiver.
A total of 273 caregivers agreed to participate in the study. After the baseline assessment, a random number generator was used to randomly assign participants stratified by gender to either the intervention group (TEL; n = 139) or the control group (CG; n = 134). Caregivers’ QoL was assessed at baseline (T0), postintervention (6 months after baseline, T1), and follow-up (12 months after baseline, T2). Participants were sent the questionnaires by e-mail and asked to complete them at home. In order to reduce the risk of missing data and/or dropout, data were collected through telephone interviews. The aim of the telephone interview was to be able to discuss comprehension difficulties, clarify unanswered questions, and review the questionnaires for completeness. All participants provided written consent and the trial was approved by the ethics commission of the Friedrich Schiller University Jena, Germany.
Intervention
Participants of the CG received written information on dementia and care and were allowed to use any support available to them. TEL participants received twelve 50-minute telephone CBT sessions over 6 months. Fifteen clinical psychologists (93.34% female, age: mean [M] = 31.47, standard deviation [SD] = 4.17) delivered the intervention. Their mean clinical experience was 4.27 (SD = 3.41) years. All therapists attended an 8-hour training and received regular supervision.
The main goal of the intervention was to help caregivers cope with the challenges of caregiving, such as managing behavior problems of the care recipient, managing own stressful emotions, accepting losses and unchangeable situations, and changing dysfunctional thoughts. The intervention manual incorporates CBT strategies such as cognitive restructuring, problem analysis and problem-solving along with emotion regulation strategies, psychoeducation, and strategies aimed at fostering acceptance. A number of the strategies are aimed at improving caregiver’s QoL, namely, discussing how to accept help and increase use of respite services (eg, identifying and addressing barriers) as well as jointly working out the importance of self-care and (re-)activating pleasant activities. Moreover, the activation of psychosocial resources is included in the Tele.TAnDem intervention as a superordinate heuristic. This means that psychosocial resources are not merely addressed in one single module but are instead incorporated into every module in the form of resource-activating questions as well as in the therapeutic stance and relationship (eg, approaching caregivers as “care experts” and appreciating and validating their efforts). The term “psychosocial resources” refers to the intrapersonal and interpersonal resources that caregivers can utilize as means for achieving motivational goals (vs the prevalent use of the term “resources” to refer to support services, sources of information, or financial resources). By activating caregivers’ psychosocial resources, the intervention helps caregivers experience themselves in terms of their strengths and positive aspects, increases their utilization of psychosocial resources, and thereby initiates an upward spiral of mastery experiences and other need-fulfilling perceptions (for more details, see the study by Töpfer and Wilz 40 ). A more detailed description of the intervention has been published elsewhere. 31
Measures
Quality of life was assessed with the German version of the WHOQoL-BREF. 43,44 The measure was modified to assess participants’ QoL over the last 2 weeks. A total of 26 items were used to measure perceived QoL for the domains of physical health (7 items, α = .83, eg, “To what extent did you feel that physical pain prevented you from doing what you needed to do?”), psychological health (6 items, α = .81, eg, “How much did you enjoy life?”), social relationships (3 items, α = .58, eg, “How satisfied were you with your personal relationships?”), and environment (8 items, α = .72, e.g. “How satisfied were you with the conditions of your living place?”). Finally, 2 items were combined into a score of overall QoL and satisfaction with general health (Overall QoL and Health; “How would you rate your quality of life?”, “How satisfied are you with your health?”; α = .52). Scores were transformed into a scale ranging from 0 to 100.
Statistical Analyses
Descriptive analyses were conducted with IBM SPSS Statistics 22. 45 To identify treatment effects, we performed intention-to-treat analyses with latent change models 46 using MPlus Version 7. 47 We used latent change models to test for intervention effects because they (like all latent structural equation models) have the benefit of explicitly accounting for measurement error, can be used to test for measurement invariance, and Full Information Maximum Likelihood estimation is used to deal with missing values.
Separate models were specified for Overall QoL and Health and for each of the 4 QoL domains. In the Overall QoL and Health model, the 2 scale items were used as indicators for the latent variable. For the 4-domain models, items were aggregated into parcels according to item-to-construct balance, and the parcels were used as indicators. 48 As measurement invariance is necessary to conduct and interpret analyses involving longitudinal multigroup data, before analyzing intervention effects, we simultaneously tested measurement invariance levels (ie, configural, weak factorial, and strong factorial) across time and study groups. For our analyses, data had to show at least strong factorial invariance (ie, the loadings and intercepts of indicators were fixed to be equal). Partial invariance (ie, invariance of the majority of indicators with free estimation of the variant parameters) was considered if model fit was not satisfactory. A level of invariance was deemed fulfilled if the Comparative Fit Index (CFI) difference between the more and the less restrictive model was ≤0.01. 49
Figure 1 displays the latent change model. Study group affiliation (CG = 0, TEL = 1) predicted mean latent change compared to baseline (ΔT1-T0; ΔT2-T0). Because participants were randomized stratified by gender, gender was included as a covariate at T0. The unstandardized path coefficient (γ) represents the mean difference between the TEL and the CG. 31,50 The fixed factor method was used for scale setting. Residual covariances were specified between the indicators measured at the different time points (T0, T1, and T2). Thus, for every indicator, 3 residual covariances were estimated freely.
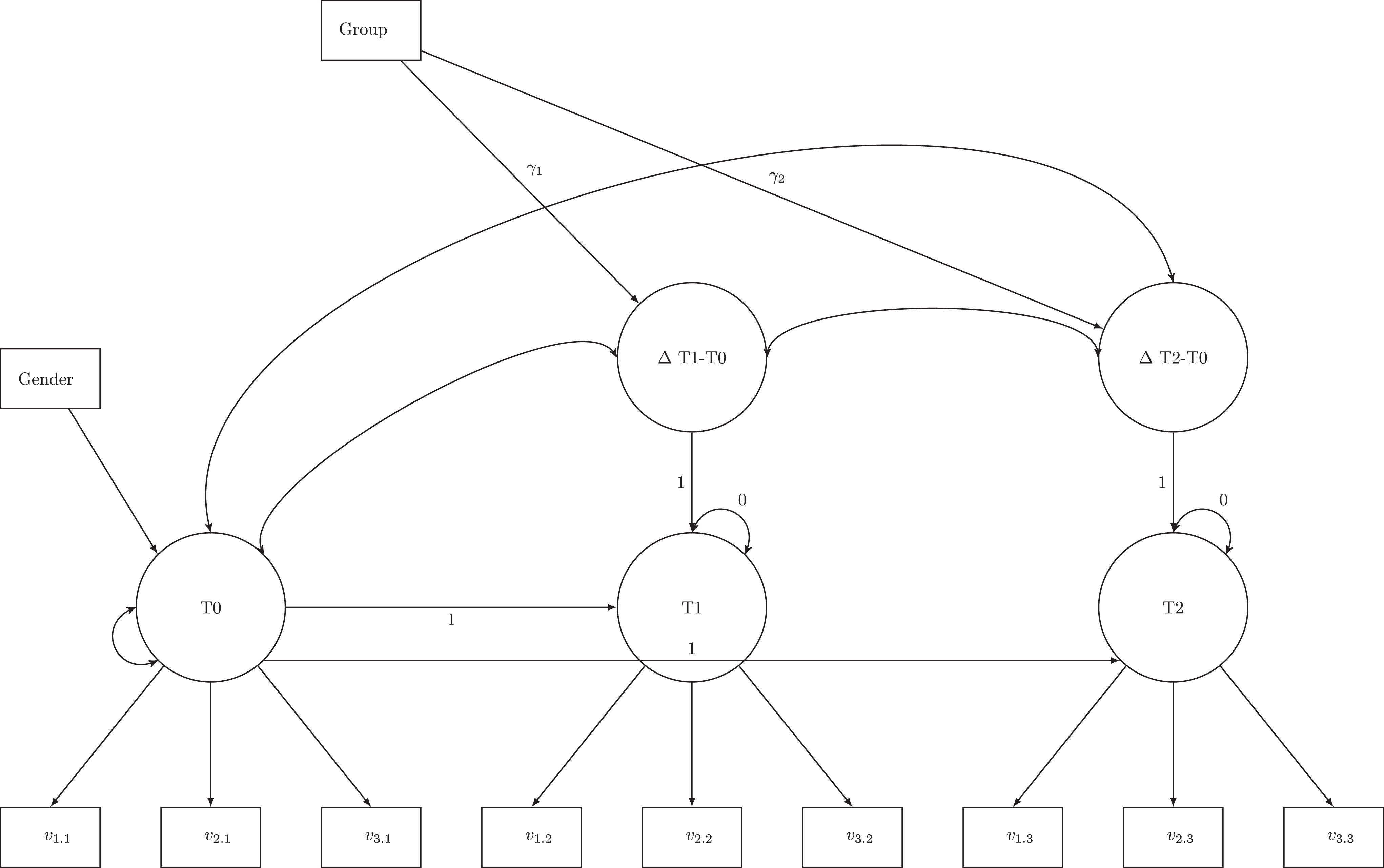
Latent change model. T0 = baseline assessment; T1 = postintervention assessment; T2 = 6-month follow-up assessment. Reprinted from Wilz et al. 31 Copyright (2018) by Oxford University Press. Permission requested.
Model fit was evaluated using 3 goodness-of-fit indices: Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), and Root Mean Square Error of Approximation (RMSEA). Acceptable fit is indicated by a CFI and a TLI ≥0.90 and an RMSEA ≤0.08. Good fit is indicated by a CFI and a TLI ≥0.95, and an RMSEA ≤0.05. 51 We used Cohen's d as a measure of effect size. A Cohen's d of 0.20 indicates a small effect, 0.50 indicates a medium effect, and 0.80 indicates a large effect. 52
Based on previous findings that the subgroup of short-term Tele.TAnDem intervention participants still caring at home had higher QoL 2 years later compared to CG participants, 41 we tested whether QoL depended on care status at T1 and T2 in post hoc analyses. We included care status (i.e., 0 = nursing home placement or bereavement, 1 = still caring at home) and the interactions between care status and study group as additional predictors for change in ΔT1-T0 and ΔT2-T0, respectively, in the latent change models.
To assess the clinical significance of changes in QoL, we calculated the difference in net improvement between the TEL and the CG. First, we calculated the difference between T1 and T0 QoL for each individual caregiver. We then determined whether the caregiver deteriorated or improved based on a 0.5 SD baseline QoL criterion. 21 That is, if the change in QoL was smaller than −0.5 SD, we classified the caregiver as deteriorated. If the change was larger than 0.5 SD, we classified the caregiver as improved. We then subtracted the number of caregivers who had deteriorated from the number of caregivers who had improved to get the net improvement for each group. Finally, we subtracted the net improvement of the CG from that of TEL and calculated the 95% confidence interval (CI) for the difference in net improvement.
Results
Sample Characteristics at Baseline
A detailed description of the sample has been published elsewhere. 31 Caregivers had a mean age of 64.10 years (SD = 11.04, range: 23-91) and were predominantly female (n = 220, 80.6%). Most caregivers were taking care of a spouse (n = 165, 60.4%) or parent with dementia (n = 104, 38.1%). On average, caregivers had been fulfilling caregiving duties for 4.89 years (SD = 3.68, range: 5 months-19 years), and the majority (n = 218, 79.9%) were living with the care recipient. Care recipients had a mean age of 78.76 years (SD = 9.35, range: 44-104 years), and 51.3% (n = 140) were female. Most care recipients had been diagnosed with Alzheimer’s disease (n = 123, 45.2%), and most were in the moderate (n = 105, 38.5%) or severe (n = 101; 37%) stages of dementia. The most frequently used in-home respite care services were in-home patient supervision (n = 84, 30.8%) and in-home care (n = 78, 28.6%); the most frequently used residential respite care services were day care (n = 74, 27.1%) and residential care groups (n = 36, 13.2%).
Compared to a community sample (CS) aged 56 to 65 years, 43 caregivers in the present sample had lower baseline overall QoL and health (M = 48.86, SD = 17.98, range: 0-100, vs M = 63.2, SD = 18.2; t[272] = −13.118, p < .001), physical health (M = 62.42, SD = 18.66, range: 7-100 vs MCS = 72.9, SDCS = 17.4; t[272] = −9.28, p < .001), psychological health (M = 55.48, SD = 17.22, range: 8-100 vs MCS = 72.8, SDCS = 16.0; t[272] = −16.62, p < .001), and social relationships (M = 48.49, SD = 19.38, range: 0-92 vs MCS = 70.0, SDCS = 18.1; t[270] = −18.27, p < .001). In contrast, our sample did not differ from the community sample with regard to environment (M = 69.72, SD = 13.8, range: 25-97 vs MCS = 70.7, SDCS = 14.7; t[272] = −1.17, p = .242).
Importantly, there were no significant differences between the TEL and the CG with regard to sociodemographic characteristics, caregiving characteristics, respite care service use, or baseline QoL. Furthermore, the TEL and CG did not differ with regard to received support (ie, no support, personal support, professional support, or both personal and professional support), satisfaction with received support, or the need for more support (ie, personal, emotional, or professional) at baseline, nor did the groups differ with regard to changes in any of the support variables from baseline to postintervention to follow-up.
Drop Out and Change in Care Status
A total of 36 (18 TEL and 18 CG) caregivers dropped out between T0 and T1, and another 7 caregivers (2 TEL and 5 CG) dropped out between T1 and T2 (overall drop out: 15.8%). Over the course of the one-year study duration, 27 (9.9%; 12 TEL, 14 CG) caregivers opted for nursing home placement and 45 (16.5%; 22 TEL, 23 CG) were bereaved.
Treatment Effects
Table 1 displays the manifest QoL scores by study group at each measurement point. Strong factorial measurement invariance was determined for all domains, and model fits for all predictor models were satisfactory (see Table 2). Regarding overall QoL and health, the TEL had significantly higher scores than the CG at T1 compared to T0 (γ = .386, P = .006, Cohen's d = .340). The effect was not maintained at T2 (γ = .057, p = .714, Cohen d's = .044). Analyses for the 4 domains revealed that the TEL had significantly better physical health than the CG at T1 compared to T0 (γ = .283, p = .006, Cohen's d = .336). The TEL also had a significantly better psychological health than the CG at T1 compared to T0 (γ = .237, p = .041, Cohen d's = .249). Neither effect was maintained at T2 (γ = .019, p = .852, Cohen's d = .023 and γ = .053, p = .675, Cohen's d = .051, respectively). There were no treatment effects regarding social relationships (T1: γ = .075, p= .590, Cohen d's = .065; T2: γ = .252, p = .117, Cohen d's = .190) or environment (T1: γ = .153, p = .178, Cohen's d = .164; T2: γ = .006, p = .962, Cohen's d = .006).
Mean Quality of Life in the Intervention and Control Groups at Baseline, Postintervention, and 6-Month Follow-Up.
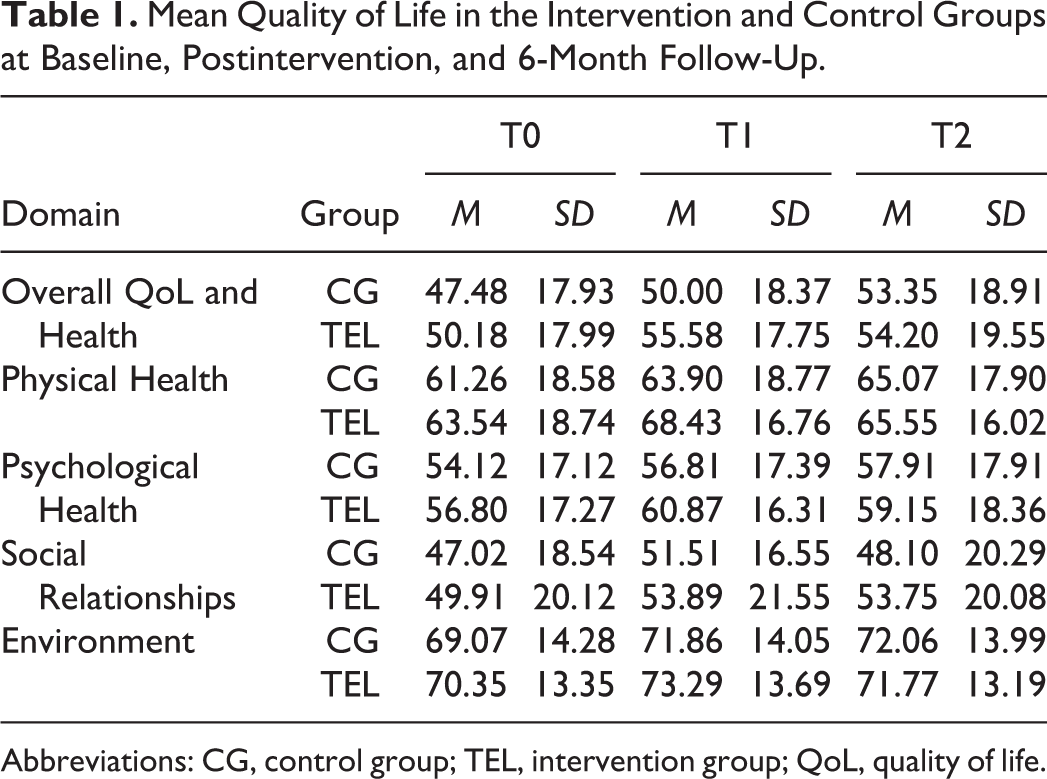
Abbreviations: CG, control group; TEL, intervention group; QoL, quality of life.
Model Fit of the Latent Change Models for Each Quality-of-Life Domain.

Abbreviations: CFI, comparative fit index; CI, confidence interval; QOL, quality of life; RMSEA, root mean square error of approximation; TLI, Tucker-Lewis index.
The post hoc analyses revealed no significant moderation effect of care status at T1 (overall QoL and health: γ = −.447, p = .206, Cohen's d = −0.154; physical health: γ = −.030, p = .918, Cohen's d = −0.012; psychological health: γ = −.082, p = .789, Cohen's d = −0.032; social relationships: γ = .120, p = .734, Cohen's d = 0.041; environment: γ = −.295, p = .336, Cohen's d = −0.117) or T2 (overall QoL and health: γ = −.279, p = .361, Cohen's d = −0.110; physical health: γ = −.278, p = .221, Cohen's d = −0.149; psychological health: γ = −.060, p = .815, Cohen's d = −0.028; social relationships: γ = −.356, p = .262, Cohen's d = −0.136; environment: γ = −259, p= .291, Cohen d 's= −0.128).
Net Improvement
Table 3 displays the net improvement per group and the difference in net improvements between groups for overall Qol and health and each of the 4 QoL domains. Net improvement was higher in the TEL than the CG for overall QoL and health (Δ percentage points = 23.8; 95% CI: 15.6 to 32.0) and the domains physical health (Δ percentage points = 19.1; 95% CI: 11.8 to 26.4) and psychological health (Δ percentage points = 22.4; 95% CI: 14.8 to 30.0). There was no difference in net improvement between groups for the domains social relationships (Δ percentage points = 1.2; 95% CI: −6.4 to 8.8) or environment (Δ percentage points = 4.6; 95% CI: −3.4 to 12.6).
Net Improvement in Quality of Life for Intervention and Control Group Participants.
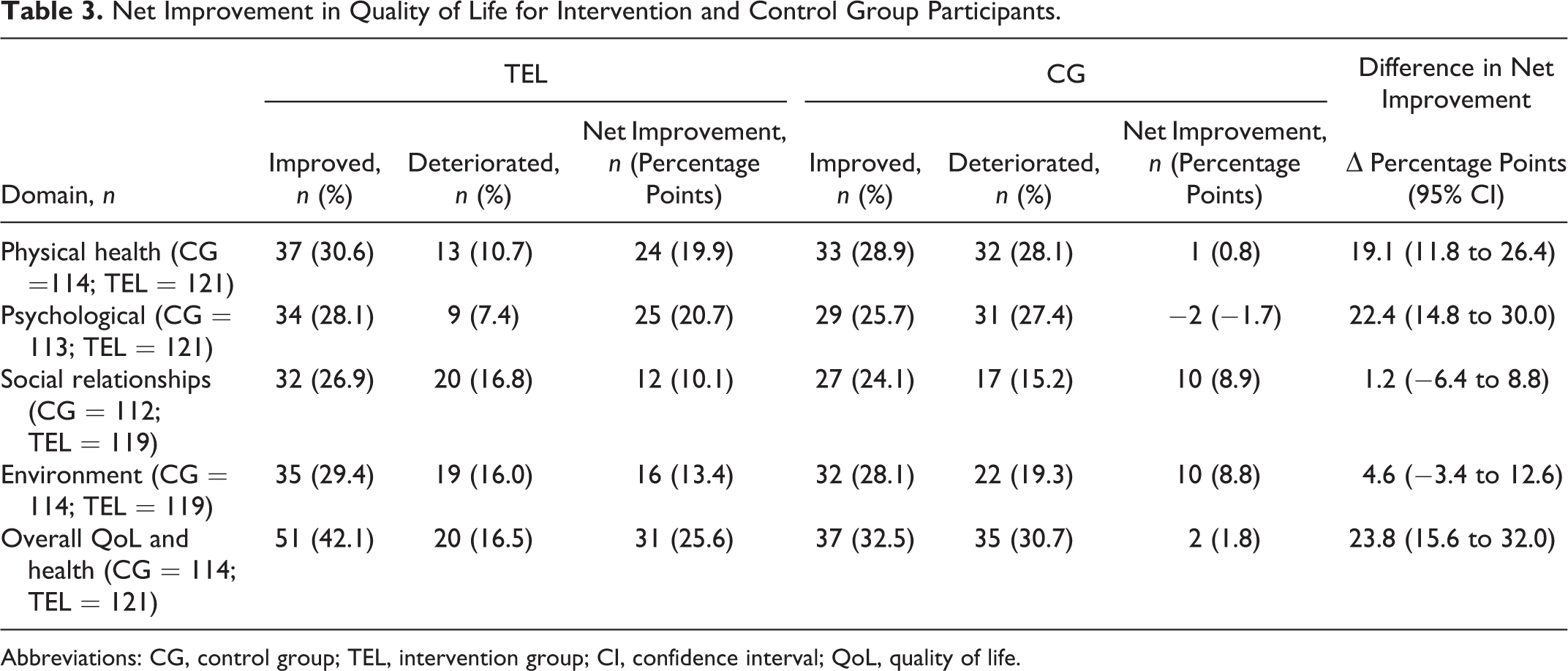
Abbreviations: CG, control group; TEL, intervention group; CI, confidence interval; QoL, quality of life.
Discussion
So far, dementia caregiver intervention research has focused predominantly on caregivers’ impairments and problems. 5 Noting that health and well-being are more, however, than just the absence of disease and suffering, 6,7 there is an urgent need to assess how interventions also affect levels of human flourishing and growth. In response to the call for more research on how interventions can improve caregivers’ positive outcomes, 5 in the current study, we examined the effect of the extended Tele.TAnDem intervention on caregivers’ QoL. Caregivers who enrolled in the current study reported lower baseline overall QoL and health as well as lower baseline physical health, psychological health, and social relationships than a community sample of older adults. These differences corroborate earlier findings on the negative effects of caregiving on QoL and health 2,53,54 and underline the importance of delivering interventions that not only target impairments but also help caregivers to maintain or improve their QoL.
After treatment, participants who received the extended Tele.TAnDem intervention reported higher overall QoL and health as well as higher QoL in the domains physical health and psychological health than CG participants. The net improvement in these 3 QoL domains from baseline to postintervention was also significantly higher in the TEL than in the CG. Previous intervention studies that have also used the WHOQoL-BREF either found no effects on any of the QoL domains 17 or only reported findings for an overall QoL score without differentiating between distinct QoL subscales. 12,36 The small improvements in QoL observed in the present study are similar in magnitude to the improvements observed with other caregiver interventions and with regard to other outcomes. 32 The observed effects are also similar in magnitude to the effects of the extended Tele.TAnDem intervention on other outcomes (eg, symptoms of depression, well-being, and physical health symptoms) 31 and the effect of the short-term intervention on QoL among the subgroup of participants still caring at home 2-years later. 41
Contrary to what one might expect, given the increasingly diffcult caregiving situation, QoL did not decrease in the CG as indicated by mean QoL levels (see Table 1), and net deterioration in the CG was only observed for psychological health (see Table 3). However, a closer look at Table 3 yields that there are more than 2 times (physical health) or 3 times (psychological health) more participants with deteriorated QoL in the CG than in the TEL group. Thus, while changes in mean QoL levels appear to indicate that the intervention effectively improved caregivers’ QoL, clinically significant intraindividual changes in QoL from pre- to posttest rather suggest that the intervention effectively prevented decreases in QoL. In other words, the intervention appears to buffer the negative impact of caregiving on QoL. The potential buffering effect implies that the intervention is likely to have stronger effects on more severely burdened caregivers. Since the study included all interested caregivers regardless of their baseline QoL scores and not just more severely burdened caregivers, the effects reported in the present study can be regarded as conservative.
No treatment effects or differences in net improvement were observed for the QoL domains social relationships or environment. Improving the quality of social relationships depends on the functionality and availability of a social network which might take time to be (re-)established. Therefore, it might not have been possible to observe treatment effects on social relationships within 6 months after intervention completion. Regarding the environment domain, environmental issues (eg, living situation) are not the central targets of psychotherapy. Moreover, in contrast to other QoL domains, there was no indication that intervention participants had low environment QoL at intake. Thus, there might not have been much room for improvement in the environment domain.
None of the treatment effects were sustained at 6-month postintervention (ie, 1 year after baseline). The lack of sustained effects is a common result in caregiver intervention studies. 32 The only other study that evaluated the effects of an explicit CBT intervention on caregivers’ QoL did not include a follow-up assessment. 34 Three other studies found that the positive effects of other kinds of face-to-face interventions on dementia caregivers’ QoL were maintained more than 1 year after baseline. 12,14,16 However, since the telephone setting is more accessible than face-to-face support, our sample might have included more participants with physical constraints, participants who were unable to leave the care recipient, and/or caregivers in rural areas. These are aspects that might have a mostly negative impact on dementia caregivers’ QoL and should therefore be kept in mind when comparing and interpreting the current findings. Nevertheless, the lack of follow-up effects in our study is curious in light of previous findings that the short-term intervention appeared to stimulate improvements in QoL among caregivers still caring at home 2 years later. 41 Further investigations on potential longer term treatment effects (also depending on care status) beyond 6 months after completion of the treatment are currently underway. In order to maintain their health and QoL, it seems likely that caregivers need more continuous support and/or more or other strategies to manage the new challenges that arise as the care recipient’s dementia progresses. Generalizing the acquired strategies to new situations requires profound changes in behavior and cognition that might not be reached in just 12 sessions and a longer intervention may have been more successful. “Booster sessions” have also been discussed as a potentially helpful approach for sustaining long-term intervention effects. 33 Identifying the change mechanisms of interventions would be helpful for designing interventions that stimulate more sustainable, long-term effects.
A number of factors make it challenging to compare our results with previous research in greater detail. The most notable reasons are differences in intervention content, duration, intensity, and setting. One novelty of the current intervention is that it was delivered via telephone, whereas the interventions in all other studies were delivered face-to-face. Another problem is that existing intervention studies have relied on many different, often suboptimal indicators of QoL. 55 For example, among the studies that reported effects on dementia caregivers’ QoL, QoL was measured rather roughly, using for example scales with just 3 items 16 or scales that assess just one domain. 13,14 One other study 12 reported findings for an overall QoL score but did not differentiate findings for distinct QoL subscales. Other studies have used screening instruments for mental disorders (eg, GHQ-12/-28) 34 or measures that comprise both positive and negative outcomes as indicators of QoL. 21 A third problem is that studies on the effects of interventions on caregivers’ QoL seldom report effect sizes. 12 -15 However, as noted earlier, the effect sizes observed in the current study are similar to the effect sizes generally observed in psychosocial intervention research in dementia care. 32
The current study adds to previous evidence regarding the effectiveness of the extended Tele.TAnDem intervention. Previous evaluations found that the extended Tele.TAnDem intervention also led to significant improvements in dementia caregivers’ well-being, depression, physical health symptoms, and coping with the care situation as well as the behavior of the care recipient at postintervention; the treatment effects on well-being and coping were maintained at the 6-month follow-up. 31 The extended intervention also successfully fostered caregivers’ coping with loss and reduced burden of predeath grief 39 as well as successfully increased dementia caregivers’ utilization of their psychosocial resources related to well-being and coping with daily hassles. 40 As typical in dementia caregiver intervention research, 5 previous evaluations have primarily focused on negative outcomes. The current results now allow us to conclude that the intervention can both reduce impairments and foster improvements in health-related QoL.
The results also add to the scarce body of research on the effectiveness of interventions on dementia caregivers’ QoL more generally. So far, improvements in caregivers’ QoL have been observed for participants of an individual occupational therapy intervention, 22,23 a number of multicomponent psychoeducational interventions, 12,15,16 and a blended intervention combining elements of psychoeducation and CBT elements. 13,14 One found that a CBT intervention delivered in a group setting had medium-sized effects on mental health and a small-sized effect, albeit not statistically significant, on QoL (d = .39). 34 Thus, the present study extends the effectiveness of CBT interventions on QoL to the individual telephone-based delivery format and might even raise the question whether individual CBT sessions may be more effective than face-to-face group CBT sessions for improving caregivers’ QoL.
Given that previous research has been characterized by diverse interventions, varied outcome measures, and inconsistent findings, insight into intervention effects on dementia caregivers’ QoL cannot be gained through comparing and contrasting empirical findings alone. Additional theoretical considerations of how an intervention may have stimulated improvements in specific dimensions of QoL are also indispensable. Conceptual models of caregiving distinguish between negative appraisals leading to negative outcomes (eg, distress, negative affect, depression) and positive appraisals leading to positive outcomes (eg, satisfaction, positive affect, gain), most likely through interrelated pathways. 55 In turn, both negative and positive outcomes are associated with health-related QoL. Accordingly, Tele.TAnDem focuses on attenuating negative appraisals and enhancing positive appraisals. Standard CBT strategies such as modifying dysfunctional thoughts (eg, perfectionism in care or guilt as a barrier to using support) and behavioral activation (eg, demonstrating the link between positive activities and mood, creating lists of health-promoting activities, planning activities, and promoting their implementation) are deemed particularly suitable in this regard. Modifying dysfunctional thoughts and behavioral activation were also identified as mechanisms through which CBT exerts its effect on dementia caregivers’ depressive symptomatology in one of the rare studies addressing mediating pathways. 56
With regard to enhancing positive appraisals, one particularity of Tele.TAnDem is that it incorporates resource activation as a superordinate intervention heuristic (for a detailed description, see the study by Töpfer and Wilz 40 ). The focus on dementia caregivers’ strengths and psychosocial resources allows them to experience themselves as functional and competent. Thereby, instead of becoming passive and demoralized, caregivers find themselves in an upward spiral including positive emotions, feelings of self-efficacy, positive reinterpretations of problems, and a proactive use of existing psychosocial resources. Tele.TAnDem has been shown to significantly increase dementia caregivers’ utilization of resources related to well-being and coping with daily hassles as an indicator of successful resource activation. 40 Thus, resource activation may be a promising candidate for sparking a positive appraisal pathway leading to increased health-related QoL.
Coen et al 57 found that “time for self” was one of only 2 QoL factors (alongside “finances”) that distinguished low-burden from high-burden dementia caregivers. In light of these results, one might be tempted to conclude that it would suffice to increase dementia caregivers’ access to respite care services as opposed to conducting CBT in order to improve their QoL. However, evidence suggests that service availability and affordability are not, in fact, major impediments to service use. 58 Thus, merely increasing “time for self” through respite services seems to be insufficient for improving caregivers’ QoL. Rather, interventions also need to target how caregivers subjectively appraise and use their time. Based on our own experience, we believe that interventions that target the psychological aspects of accepting help, recognizing the importance of self-care, and (re-)activating pleasant activities are likely to be most effective for helping dementia caregivers improve their QoL.
Limitations
Based on expert opinion, 8,44 we used the WHOQoL-BREF as a measure of QoL in the current study. A clear advantage of the WHOQoL-BREF is that it assesses a number of domains that allowed us to investigate specific treatment effects and detect differences across domains. However, the internal consistencies for overall QoL and health and the domain social relationships were not satisfactory, potentially indicating substantial measurement error. It should be kept in mind, however, that latent change models are able to separate measurement error from the latent construct of interest. Thus, the results reported here have been adjusted for measurement error. Nevertheless, a reevaluation of the psychometric qualities of the WHOQoL-BREF in caregiver populations seems necessary, especially given that few dementia caregiver studies have reported the internal consistencies of the WHOQoL-BREF subscales.
In this study, we aimed to evaluate the effectiveness of the intervention within existing care provision structures. We therefore prioritized external over internal validity. As such, the study did not include an active control condition, and low baseline QoL was not a requirement for participation. It cannot be ruled out that the current results are not specific to CBT specifically but rather an effect of personal attention more generally. Given that a previous efficacy trial demonstrated the superior effectiveness of the short-term Tele.TAnDem intervention over a relaxation training, 37 we find this alternative explanation unlikely.
Furthermore, we cannot conclude that the telephone CBT intervention was more (cost) effective than a face-to-face CBT intervention. Originally, a third group with a face-to-face CBT intervention was planned. 42 However, soon after starting recruitment, it became evident that only a limited number of caregivers could regularly attend face-to-face sessions, for example, because they lacked access to alternative supervision for the care recipient. We therefore decided to continue the face-to-face condition as a nonrandomized condition (for more details see the study by Wilz et al 31 ). In the present study, we focused only on the 2 randomized groups in keeping with the standards for evaluating the effectiveness of an intervention. A comparison between the nonrandomized face-to-face condition and the telephone condition is currently underway.
Although baseline QoL was generally low in the sample as a whole, some caregivers reported satisfactory or even high QoL at baseline. Thus, there might not have been much room for improvement following treatment for a portion of the sample, resulting in a loss of statistical power to detect change. 59
The observed increases in QoL (and some other outcome measures) 31 in the CG require explanation, although the percentages of CG participants with clinically significant increases in QoL in our study (24.1%-32.5%, see Table 3) are within the range observed in previous studies including an evaluation of a CBT group intervention 34 (10%-28.6%) and an evaluation of the REACH intervention 21 (white or caucasian caregivers: 25.6%-41.9%). Potentially, the data collection procedure (ie, telephone interviews) may have affected participants’ QoL ratings. When participants voiced their concerns and feelings, interviewers made an effort to keep the focus on the assessment, but it would have been unethical not to respond empathetically. The experience of speaking with an emphathetic listener during the telephone interviews might have improved participants’ mood and thereby positively affected how they rated their QoL, thus disguising true decreases in QoL in the CG group and hence true differences between the TEL and CG. It is therefore possible that a different data collection procedure would have revealed larger treatment effects.
Conclusion and Outlook
Including positive outcomes such as QoL in dementia caregiver intervention research can provide a more complete picture of how interventions affect caregivers’ health and well-being as well as provide important insights about how interventions can help caregivers flourish in the face of adversity. The present study provides evidence that a telephone-based CBT intervention can improve dementia caregivers’ health-related QoL. Suggestions for future research include identifying the mechanisms through which dementia caregiver interventions increase QoL (eg, through increasing dementia caregiver’s utilization of psychosocial resources) and addressing how intervention effects can be sustained.
Footnotes
Authors’ Note
Acknowledgments
The authors wish to thank Sabine Jansen and Bianca Broda from the German Alzheimer’s Association for their contribution to the study organization and participant recruitment. The authors thank Graduate Psychologists Kathi Albrecht and Tanja Kalytta along with Anna Machmer, MSc, Christina Reiter, MSc, Denise Schinköthe, MSc, and Lisette Weise, MSc, for their contribution to study organization and data collection. The authors thank Graduate Psychologists Beate Czerwon, Lydia Franke, Katharina Grams, Ruth Haferkamp, Friederike Huget, Marie Jüngst, Franka Möllmann-Hofman, Silvana Polotzek, Tamara Thurn, Michael Wenz, Katharina Wurm, and Johanna Zimmer for delivering the intervention. The authors thank all family caregivers who participated in the study. The authors kindly acknowledge Dr Catherine E. Bowen for editing the manuscript and for providing helpful feedback.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Federal Ministry of Health (Grant IIA5-2512FSB555).