
Abstract
Background:
To examine the relationships between cognitive dysfunction status and quality of life.
Methods:
Secondary analysis of a nationwide population-based survey (≥65 years) in Taiwan. The 5-dimension EuroQoL questionnaire (EQ-5D) was completed by 10 013 participants.
Results:
Participants with mild cognitive impairment (MCI; odds ratio = 4.88), very mild dementia (VMD; 7.96), or dementia (32.85) were more likely than those with normal cognition to report self-care problems. Participants with MCI (3.86), VMD (9.26), or dementia (31.61) were more likely to have usual-activity problems, and those with MCI (3.04), VMD (3.82), or dementia (9.23) were more likely to have mobility problems. Participants with MCI (2.10 and 2.14), VMD (2.77 and 2.18), or dementia (3.04 and 3.02) were more likely to report pain/discomfort and anxiety/depression.
Conclusion:
Dementia was negatively associated with EQ-5D, especially self-care, usual activities, and mobility. Mild cognitive impairment or VMD was also negatively associated, with VMD more negatively associated. Developing interventions for patients with specific cognitive dysfunctions is critical.
Keywords
Introduction
Dementia has become a major health issue for societies worldwide. 1 Older people with dementia have to contend with cognitive deficits, behavioral disturbances, and increasing dependence for help with daily living activities, all of which negatively impact their quality of life. 2,3 As in many other developed nations, the number of persons with dementia in Taiwan has increased dramatically of late, placing a substantial burden on families nationwide. Indeed, the prevalence rates of all-cause dementia and mild cognitive impairment (MCI) in a population-based, cross-sectional survey in Taiwan were 8.04% and 18.76%, respectively. 4 Since dementia cannot be cured, recent research on dementia has focused on preventing and improving quality of life for persons with dementia and their family caregivers. 5,6 Measuring quality of life may help to understand the progression of dementia, allowing comparison at different stages of the disease. 7
Self-reported health-related quality of life (HRQoL) has been a traditional supplemental indicator of disease and treatment outcomes such as mortality, as well as an objective clinical indicator of the effects of disease and interventions. 8,9 Health-related quality of life data are extensively used in evaluating the economics (ie, cost-effectiveness analyses) of interventions for persons with dementia and their caregivers. 10,11 Regarding disease effects, several HRQoL domains are negatively affected by specific cognitive deficits such as inattention, dysexecutive function, and processing speed. 12 Similarly, HRQoL or Alzheimer’s disease-related quality-of-life dimensions have been affected by cognitive impairment in patients with neurological disease, 12 dementia, 13,14 or MCI. 15,16 These results indicate a negative association between HRQoL and cognitive impairment. In contrast, a review of studies published through October 2007 found no significant association between cognitive impairment and HRQoL in patients with dementia. 17 An 18-month follow-up study showed no significant associations between changes in HRQoL and the progression of Alzheimer’s disease. 18 This inconsistency may be the result of using different measures, statistical methods, and/or sample inclusion criteria. Additionally, most studies used convenience rather than randomly selected samples, 17 limiting the generalizability of the results.
Few studies to date have compared HRQoL among older persons with normal cognition, MCI, very mild dementia (VMD), and dementia. Specifically, the extent of association between each diagnosed cognitive dysfunction and HRQoL has not yet been examined within a large, randomly selected sample. The ability to differentiate HRQoL among older persons with normal cognitive function, MCI, VMD, and dementia can help governments deal with the increasing numbers of older persons with these cognitive dysfunctions by providing a dysfunction-specific basis for planning and developing national dementia programs for social/health services and resources. Therefore, the purpose of this study was to investigate the relationships between cognitive-dysfunction status and HRQoL in a national, randomly selected sample of older persons in Taiwan. We hypothesized that older persons in Taiwan with MCI, VMD, or dementia would experience worse HRQoL than those with normal cognition and that, of the 3 groups, older persons with dementia would report the lowest HRQoL. The relationships of HRQoL with sociodemographics, health conditions, and lifestyle habits also were explored.
Methods
Design and Participants
For this secondary analysis, we used data from a subsample of older Taiwanese persons with normal cognition, MCI, VMD, or dementia in a nationwide population-based cross-sectional study.
4
The original project was designed to assess the prevalence of MCI and dementia in a nationally representative sample (N = 10 432) of persons
Diagnosis of Dementia
Dementia was diagnosed by the core clinical criteria recommended by the National Institute on Aging-Alzheimer’s Association (NIA-AA). 19 The clinical history of cognitive status was determined by evaluating participants and knowledgeable informants (primary family caregivers who cared for the patient at least 10 hours weekly). Cognitive status was objectively assessed using the Clinical Dementia Rating Scale (CDR) and the Taiwanese Mental State Evaluation (TMSE, normal scores are >24 in literate elderly people and >13 in illiterate elderly people). 20 Functional status was assessed using the Activities of Daily Living (ADL) Scale and Instrumental ADL (IADL) Scale. Participants with a CDR score >1 were categorized into the dementia group. Participants with a CDR score of 0.5 and abnormal TMSE score were categorized into the VMD group. Individuals with VMD had a mild decline in daily functions and impairment in at least 2 cognitive domains following the NIA-AA criteria. Participants with a CDR score of 0.5 and impairment in at least 1 cognitive domain but no evidence of impairment in social or occupational functioning as assessed by the ADL and IADL scales were assigned to the MCI group. Participants with none of the above conditions were assigned to the normal-cognition group. More details are in the original studies. 4,21
Measurements
Functional status was assessed by the ADL scale for self-care activities in eating, transferring, grooming, toileting, bathing, walking, climbing stairs, and dressing, along with bowel and bladder control. Activities of Daily Living scores are calculated by summing all individual item scores, with a maximum score of 20 representing full independence. 4
Health-related quality of life was measured using the 5-dimension EuroQoL questionnaire (EQ-5D), a standardized instrument for measuring generic health status. 22 The EQ-5D has 2 self-report sections: a self-classifier and a visual analogue scale (VAS). The self-classifier assesses the dimensions of mobility, self-care, usual activity, pain/discomfort, and anxiety/depression at 3 levels: no problems, some problems, and extreme problems. These are combined to create 243 possible health states, which can then be translated into a summary index by applying time trade-off techniques using Taiwan’s general population. 23 Health state values range from the lowest score of −0.674 (most extreme problems across all 5 dimensions) to a full health score of 1 (no problems in any dimension). The VAS is a 20 cm, vertical scale. Respondents use the VAS to classify and rate their health status on the day of the survey from 0 (worst imaginable health state) to 100 (best imaginable health state). Reliability and validity of the EQ-5D Taiwan version have been established. 24,25
Procedures
The original study was approved by the ethics committee at the National Taiwan University Hospital. 4 Data were collected in face-to-face interviews conducted by trained home care nurses during door-to-door home visits after obtaining written informed consent from all participants or their proxies. Participants were interviewed in accordance with an operation manual defining all questionnaire variables. Home care nurses received a 2-day training course conducted by neurologists and clinical psychologists; this course was then followed by a 2-day internship at a medical center. The quality and reliability of the collected data were ensured by supervisors who checked for inconsistencies and auditing.
Statistical Analysis
For this article, we extracted the following variables as covariates from the original data set: age, gender, marital status (married = 1), living with family (yes = 1), illiterate (yes = 1), current or former smoker (yes = 1), current alcohol drinker (yes = 1), tea drinker (yes = 1), vegetarian (yes = 1), rare exercise (yes = 1), good sleep quality (yes = 1), social activity (no or rare social activities = 1) and comorbidities, including hypertension, diabetes, lung disease, liver disease, history of stroke and/or peptic ulcer. 26,27 Participants’ characteristics were compared across 3 cognitive-dysfunction groups (ie, MCI, VMD, and dementia) using χ2 tests for categorical variables and F tests (or Welch tests, when the homogeneity of the variance test was rejected) for continuous variables. Fisher least significant difference was used in post-hoc analysis for comparisons across groups.
Associations between EQ-5D health status (self-classifier, VAS, and summary index) and cognitive-dysfunction groups were explored by binary logistic regression analyses (for binary variables) and generalized linear models (for continuous variables). Binary variables (with problems = 1, no problems = 0) were generated to identify any health problems in each EQ-5D. All covariates were included in the models. Statistical analyses were performed using SPSS for Windows 22 (SPSS Inc, Chicago, Illinois), with P < .05 considered significant.
Results
Patient Characteristics
The sociodemographic characteristics, health conditions, and lifestyle habits of each cognitive dysfunction group are shown in Table 1. In this sample, 70.26% of participants (n = 7035) had normal cognition, 20.46% (n = 2049) had MCI, 3.66% (n = 366) had VMD, and 5.62% (n = 563) had dementia. The normal cognition group had a significantly lower proportion of participants who were older, female, and illiterate and a greater proportion who were married and living with their family than participants in the other cognitive dysfunction groups (ie, MCI, VMD, and dementia, separately) with post hoc test. As for health condition, the dementia group had a significantly higher proportion of participants having hypertension, diabetes, lung disease, and/or stroke than the normal cognition group. In terms of lifestyle habits, significantly lower proportions of participants in the dementia group than in the other groups reported being current or former smokers, current alcohol or tea drinkers, or sleeping well. A significantly higher proportion of participants in the dementia group also reported exercising rarely and engaging rarely or not at all in social activities.
Relationships of Cognitive Function With Sociodemographic Characteristics, Health Conditions, and Lifestyle Habits.
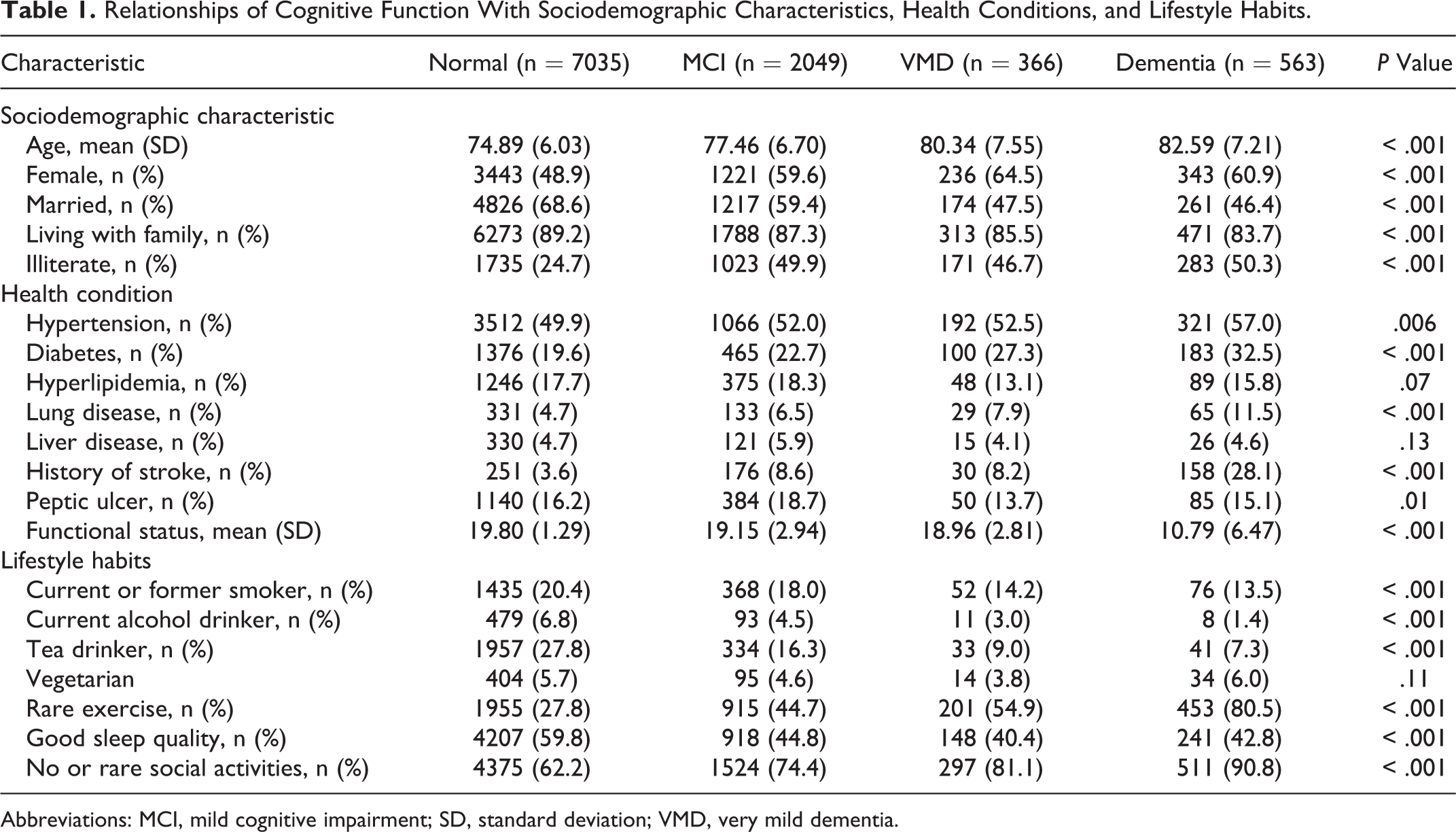
Abbreviations: MCI, mild cognitive impairment; SD, standard deviation; VMD, very mild dementia.
Health-Related Quality of Life Comparison
Comparisons of HRQoL (EQ-5D scores) by cognitive function group are shown in Table 2. The proportion of participants reporting problems increased as cognitive impairment increased, with similar patterns in each EQ-5D across cognitive function subgroups. A significantly higher proportion of patients with dementia reported problems across all dimensions (mobility = 85.9%, self-care = 84.4%, usual activities = 92.1%, pain/discomfort = 71.1%, anxiety/depression = 53.9%). Regarding health status, the mean VAS score for patients with dementia (mean = 49.4) was significantly lower than that for patients with normal cognition, MCI, or VMD (mean differences = −27.70; 95% confidence interval [CI] = −29.39 to −26.01, −18.40; 95% CI = −20.20 to −16.60, and −15.49, 95% CI = −17.91 to −13.07, respectively, all with P < .001). The proportion of participants who rated their current health state at >90 was 27.7% for patients with normal cognition, 11.1% for patients with MCI, 5.2% for patients with VMD, and 4.4% for patients with dementia. A similar trend was observed for summary index scores. The mean index score for patients with dementia (mean = −0.05) was significantly lower than that for patients with normal cognition, MCI or VMD (mean differences = −0.87; 95% CI = −0.90 to −0.85, −0.63; 95% CI = −0.66 to −0.60], and −0.50, 95% CI = −0.54 to −0.46, respectively, all with P < .001).
Proportion (Distribution) of Participants Reporting Problems and Health Status in Different HRQoL Dimensions and Scores by Group.
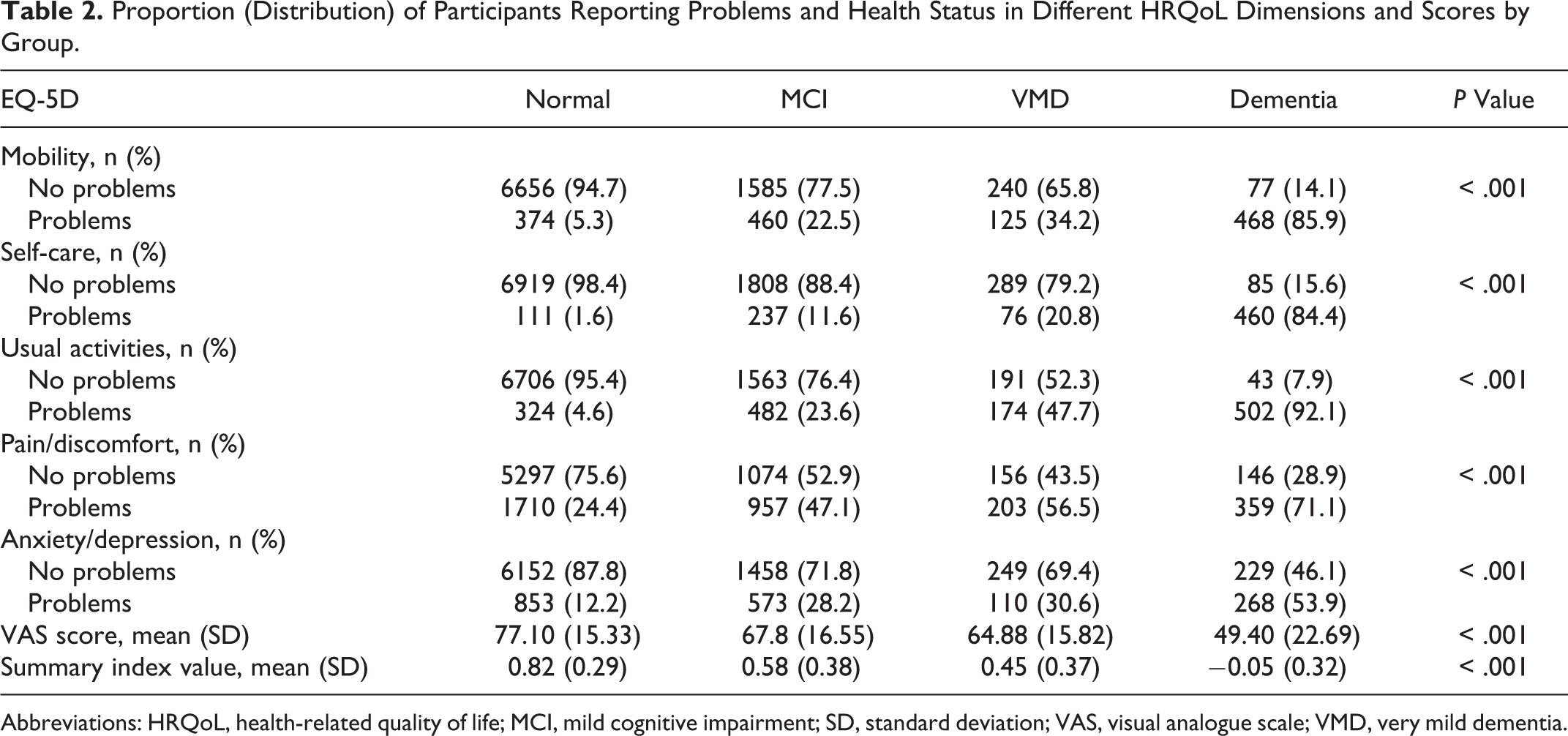
Abbreviations: HRQoL, health-related quality of life; MCI, mild cognitive impairment; SD, standard deviation; VAS, visual analogue scale; VMD, very mild dementia.
Predictors of HRQoL
The associations between cognitive status and HRQoL, after controlling for sociodemographics, health condition, and lifestyle habits, are shown in Table 3. In terms of EQ-5D, participants in the 3 cognitive dysfunction groups were more likely to experience problems with mobility, self-care, usual activities, pain/discomfort, and anxiety/depression than those with normal cognition, as shown by their coefficient b values. Those in the MCI, VMD, and dementia groups had positive b values (MCI: 1.11; standard error [SE] = 0.09 in mobility, 1.59; SE = 0.15 in self-care, 1.35; SE = 0.09 in usual activities, 0.75; SE = 0.06 in pain/discomfort, and 0.76; SE = 0.07 in anxiety/depression; VMD: 1.34; SE = 0.14 in mobility, 2.07; SE = 0.20 in self-care, 2.23; SE = 0.13 in usual activities, 1.02; SE = 0.12 in pain/discomfort, and 0.78; SE = 0.13 in anxiety/depression; and dementia: 2.22; SE = 0.17 in mobility, 3.49; SE = 0.20 in self-care, 3.45; SE = 0.20 in usual activities, 1.11; SE = 0.14 in pain/discomfort, and 1.11; SE = 0.14 in anxiety/depression), all with P < .001, suggesting that participants in these groups were more likely to experience problems than those in the normal cognition group. The likelihood of experiencing problems tended to grow with increasing cognitive dysfunction.
Binary Logistic Regression Analyses/Generalized Linear Models for Factors Associated With Different EQ-5Ds and Health Status Scores.
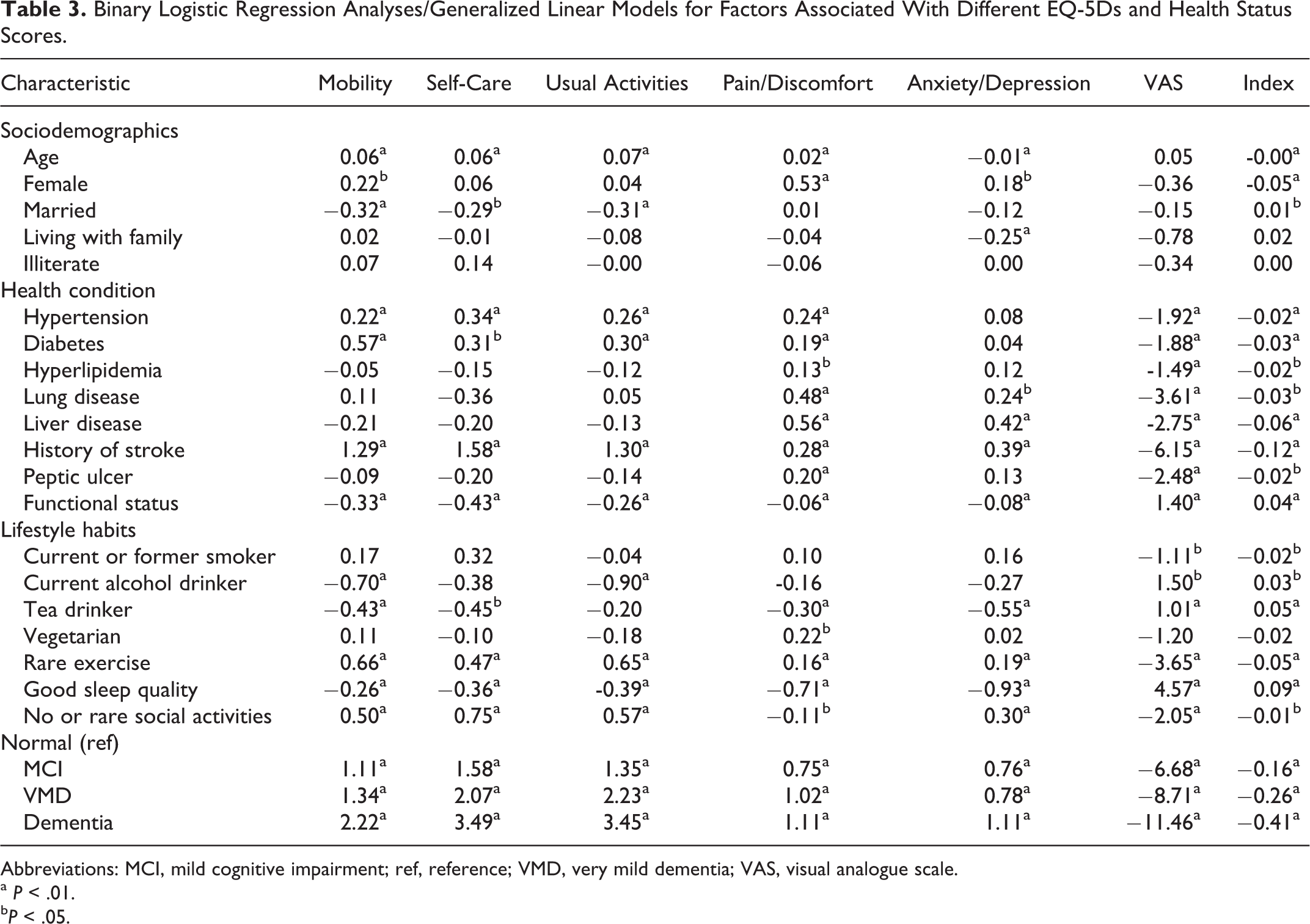
Abbreviations: MCI, mild cognitive impairment; ref, reference; VMD, very mild dementia; VAS, visual analogue scale.
a P < .01.
b P < .05.
Similar results were found for health state scores that is VAS and summary index scores. Participants with MCI (b = −6.68; SE = 0.42 for VAS score and −0.16; SE = 0.01 for index score with P < .001), VMD (b = −8.71; SE = 0.89 for VAS score and −0.26; SE = 0.02 for index score with P < .001) and dementia (b = −11.46; SE = 1.07 for VAS score and −0.41; SE = 0.02 for index score with P < .001) were more likely to report lower VAS and index scores than those in the normal cognition group. These scores tended to decline with increasing cognitive dysfunction, which itself was negatively associated with overall HRQoL.
Regarding health condition, participants with chronic diseases had lower health status scores and reported problems with pain/discomfort. Specifically, participants with hypertension, diabetes, or stroke reported problems in mobility, self-care, and usual activities, whereas those with lung disease, liver disease, or stroke reported problems with anxiety/depression. Functional status was significantly and positively associated with HRQoL, which tended to deteriorate with decreasing levels of functional status. In terms of lifestyle habits, smoking was negatively associated with health status scores. Drinking tea was associated with higher health status scores, and tea drinkers tended to report no problems in mobility, self-care, pain/discomfort, or anxiety/depression. Notably, drinking alcohol was positively, significantly associated with health status scores, and alcohol drinkers tended to report no problems with mobility or usual activities. Regular exercise, good sleep quality, and regular social activities were positively associated with HRQoL.
Discussion
Our study is the first to explore associations between HRQoL and MCI, VMD, and dementia in a nationwide representative sample of older Taiwanese persons. We found that lower cognitive function was associated with higher proportions of patients reporting health problems and lower health state scores (ie, mean VAS and index scores). These results are compatible with those of previous studies on 85-year-old Swedish people, 16 elderly Russian patients with depression and dementia, 28 and older Americans with dementia in long-term care. 29
Our results support that a diagnosis of dementia is strongly associated with all dimensions of HRQoL, consistent with prior studies. 13,14 The proportions of patients with dementia that reported problems in self-care, usual activities, or mobility were especially high. Indeed, older persons with dementia were 32.85 times (95% CI = 22.24-48.53) more likely to have problems in self-care, 31.61 times (95% CI = 21.56-46.36) more likely to have problems in usual activities, and 9.23 times (95% CI = 6.59-12.94) more likely to have problems in mobility, but only 3.04 times (95% CI = 2.34-3.97) more likely to have problems in pain/discomfort and 3.02 times (95% CI = 2.31-3.96) more likely to have problems in anxiety/depression than those without cognitive impairment (estimated odds ratio = exp [b], where b = 3.49 in self-care, 3.45 in usual activities, 2.22 in mobility, 1.11 in pain/discomfort, and 1.11 in anxiety/depression). Our results differ from those of a prior study suggesting that older Chinese persons with cognitive dysfunction were more likely to have problems in pain/discomfort and anxiety/depression. 27 This variance may be due to differing methods of classifying cognitive function; for our sample, dementia was diagnosed using core clinical criteria recommended by the NIA-AA, 19 whereas the prior study used a 10-item screening tool. 27
Our results are consistent with a report that patients with dementia have a higher risk for deterioration in the ability to perform ADL. 30 Furthermore, dependency (or patients’ inability to perform ADL) was shown to be the main predictor of HRQoL among patients with dementia, 18,31 and patients who perform physical activities have been shown to experience a better quality of life. 32 Interference in usual activities and a decline in overall functioning are core clinical criteria for dementia and are used to chart its course and as prognostic markers, in that they contribute significantly to caregiver burden and the likelihood of patients’ institutionalization. 33,34
We also found that belonging to the MCI and VMD groups was negatively associated with HRQoL, yet this association was not as strong as membership in the dementia group. Moreover, post-hoc analysis showed that belonging to the VMD group was more negatively associated with HRQoL than belonging to the MCI group. More participants with VMD reported problems in mobility (34.2% and 22.5%, 95% CI = 0.08-0.15, P < .001), self-care (20.8% and 11.6%, 95% CI = 0.07-0.12, P < .001), usual activities (47.7% and 23.6%, 95% CI = 0.21-0.27, P < .001), and pain/discomfort (56.5% and 47.1%, 95% CI = 0.04-0.14, P < .001), and also had lower mean VAS (64.88 and 67.8, 95% CI = −4.83 to−1.00], P < .01) and index scores (0.45 and 0.58, 95% CI = [−0.17 to −0.08], P < .001). Participants with VMD were also 1.63 times (95% CI = 1.15-2.31, P < .01) more likely to have problems in self-care, 2.40 times (95% CI = 1.85-3.11, P < .001) more likely to have problems in usual activities, and 1.31 times (95% CI = 1.04-1.67, P = .03) more likely to have problems in pain/discomfort than those with MCI. These differences may stem from VMD being diagnosed if cognitive decline interfered with community affairs, at-home hobbies or personal care, whereas patients with MCI showed no evidence of impairment in social or occupational functioning. 4
A greater understanding of the association of sociodemographic factors, individual health conditions, and lifestyle habits with HRQoL may be useful in guiding policies and developing tailored interventions to improve quality of life for older people. We found it noteworthy that the presence of chronic diseases was associated with decreased health state scores and more reported problems with pain/discomfort. In terms of lifestyle habits, tea or alcohol consumption, exercise, sleep quality, and social activities were significantly, positively associated with all EQ-5D and health state scores.
Our findings have several implications. First, the association between dementia and all HRQoL dimensions, particularly self-care, usual activities, and mobility, emphasizes the importance of implementing community-based support services for older people with dementia and their families. More governmental or nongovernmental resources should be provided and innovative strategies developed, not only to facilitate self-care for patients with dementia in terms of usual activities and mobility, but also to detect and limit their problems in pain/discomfort and anxiety/depression. Interventions tailored to individuals with dementia have improved their abilities; 35 –37 for example, exercise interventions significantly improved mobility/functional limitations or physical functioning, 35 occupational therapy interventions positively affected ADL, 36 and cognitive-behavioral therapy-based interventions managed behavior and mood. 37 Care and support should also be provided to patients with MCI and VMD, since all dimensions of their HRQoL are also affected. Patients with VMD are especially in need of enhanced support in terms of their self-care, usual activities, and detecting/reducing pain and discomfort. Our results show that individuals with VMD were more likely than those with MCI to have problems in self-care, usual activities, and pain/discomfort. Thus, a differential diagnosis between MCI and VMD is of the utmost importance in the early stages of developing interventions. Patients with either MCI or VMD would benefit from routine assessment, early detection of and interventions for difficulties in self-care and usual activities, as well as symptomatic treatment for pain/discomfort, but these interventions are especially important for those with VMD. Also, intervention effects can be indicated by improvement in HRQoL dimensions such as self-care ability, usual activities, and pain/discomfort relief, especially for individuals with VMD. Other interventions suggested for patients with dementia include early-stage support groups, 38 musical interventions, 39 and communication-education programs for nurses caring for this population, 40 yet only a limited number of studies have focused on interventions to improve these patients’ quality of life. Further research is therefore recommended. Moreover, our study provides evidence for the validity of the EQ-5D at different stages of dementia. Thus, EQ-5D index scores can be used to evaluate interventions for clinical and economic effectiveness. 41
This study had limitations. First, the cross-sectional design without longitudinal follow-ups was unable to explore changes in HRQoL over time or confirm causal relationships. The cognitive function of all participants was assessed primarily by clinical history, Mini-Mental State Examination, and CDR, without a detailed psychiatric evaluation to exclude other major disorders that may be misdiagnosed as dementia. This limitation may have been negated, however, by consulting a panel of 4 neurologists and 1 clinical psychologist specializing in the diagnosis and care of people with dementia for each difficult case.
In conclusion, this nationwide epidemiological study indicates that cognitive dysfunction is associated with diminished HRQoL. Our findings indicate that dementia is strongly associated with negative overall HRQoL, especially in self-care, usual activities, and mobility among community-dwelling older Taiwanese persons. Being diagnosed with MCI or VMD was also negatively associated with overall HRQoL, with VMD being more negatively associated than MCI in terms of self-care, usual activities, and pain/discomfort. Thus, patients with VMD require more specialized care and support.
Footnotes
Acknowledgments
The authors would like to express their gratitude to the Taiwan Alzheimer’s Disease Association (TADA) for its invaluable contribution to this study, in that we used a database which was conducted and supported in part by the TADA, under commission of the Ministry of Health and Welfare of Taiwan (DOH100-TD-M113-100001). The views expressed throughout this study are exclusively those of the authors and do not represent the views or opinions of the Ministry of Health and Welfare, Taiwan.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chang Gung Medical Foundation (BMRP297 and CMRPD1E0162) and Healthy Aging Research Center, Chang Gung University, Taiwan (EMRPD1H0361 and EMRPD1H0551).